
Design of Topical Moxifloxacin Mucoadhesive Nanoemulsion for the Management of Ocular Bacterial Infections

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.1.1. Chemicals and Glassware
2.1.2. Biological Tissues and Samples
2.2. Methods
2.2.1. HPLC
2.2.2. Screening of Oils
2.2.3. Preparation of MOX-NE Formulations
2.2.4. Preparation of MOX-NEM Formulations
2.2.5. Control Formulation
Vigamox® (Alcon Laboratories, Inc., Fort Worth, TX, USA)
Crude Drug Solution (MOX-HCL-S)
2.2.6. Measurement of Droplet Size (DS), Polydispersity Index (PDI), and Zeta Potential (ZP)
2.2.7. Drug Content
2.2.8. pH Measurement
2.2.9. Viscosity Measurement
2.2.10. Stability Studies
2.2.11. Sterilization Process and Stability Assessment
2.2.12. Scanning Transmission Electron Microscopy (STEM)
2.2.13. In Vitro Release Studies
2.2.14. Transcorneal Permeation Studies
2.2.15. Antimicrobial Efficacy
2.2.16. Statistical Analysis
3. Results and Discussion
3.1. Screening of Oils
3.2. Preparation of MOX-NE Formulations
3.3. Physicochemical Characteristics of MOX-NE Formulations
3.4. Addition of Mucoadhesive Agents to the MOX-NE Formulation
3.5. Physicochemical Characteristics of MOX-NEM Formulations
3.6. pH and Viscosity
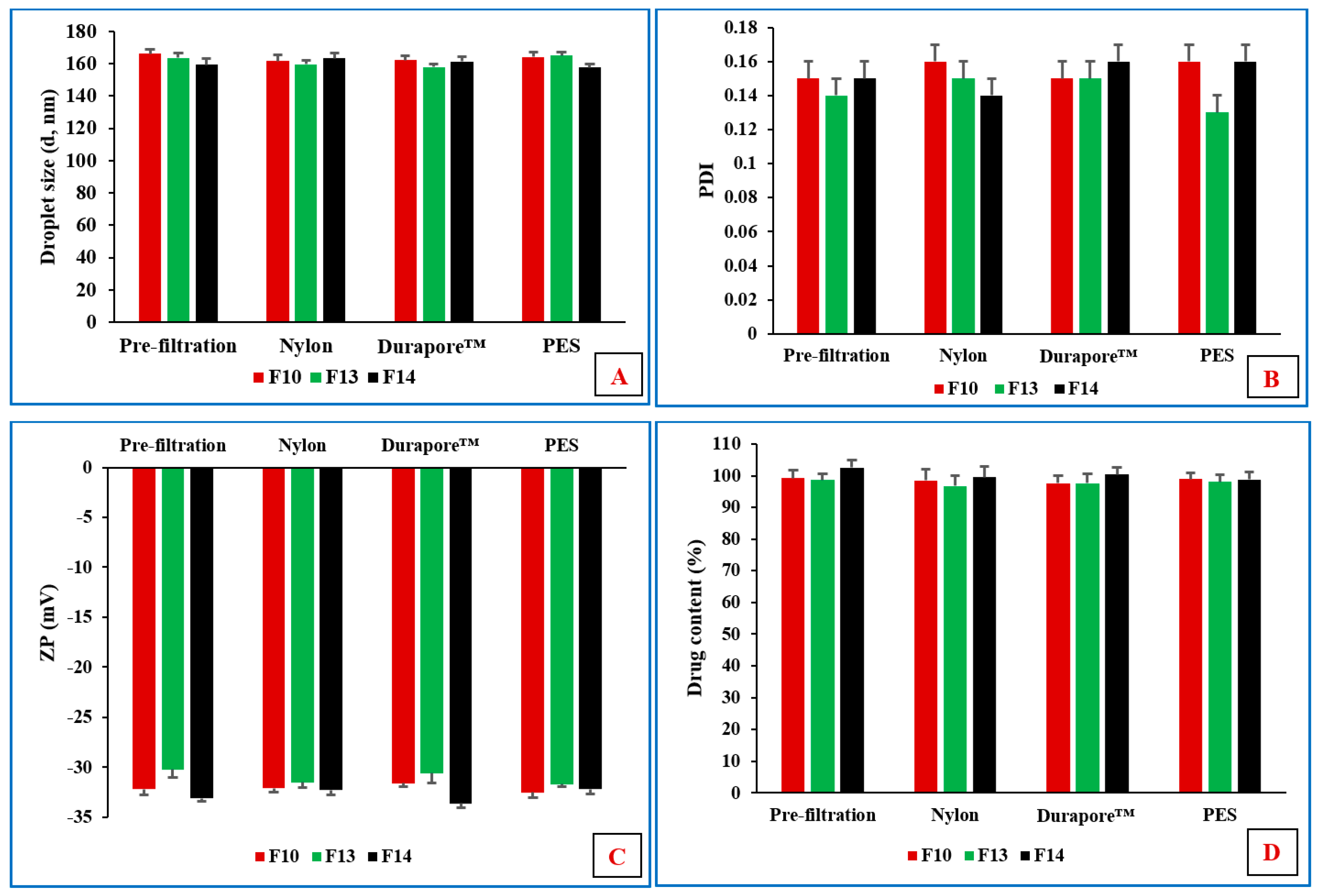
3.7. Sterilization by Filtration
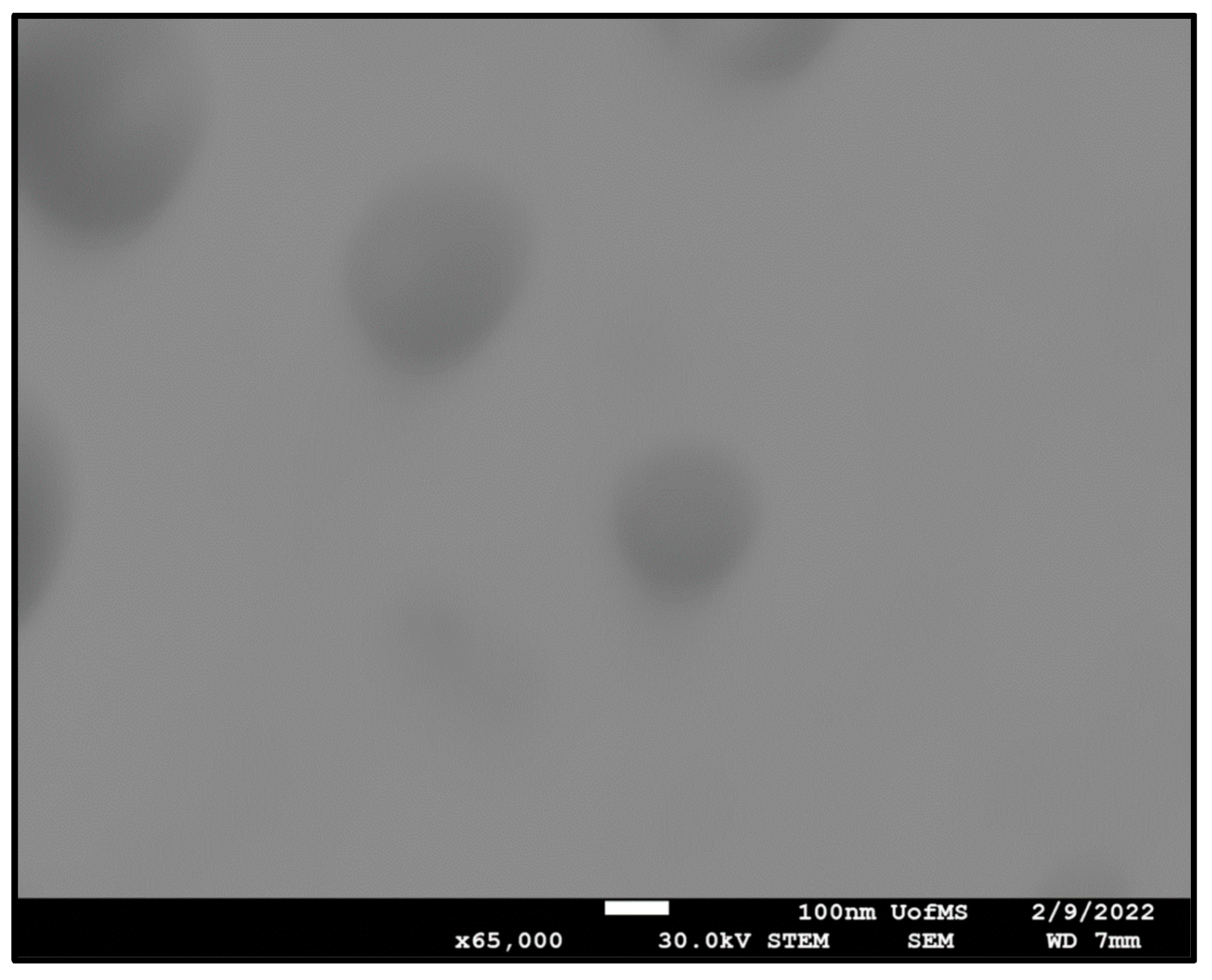
3.8. STEM
3.9. Antibacterial Activity of MOX-NE and MOX-NEM
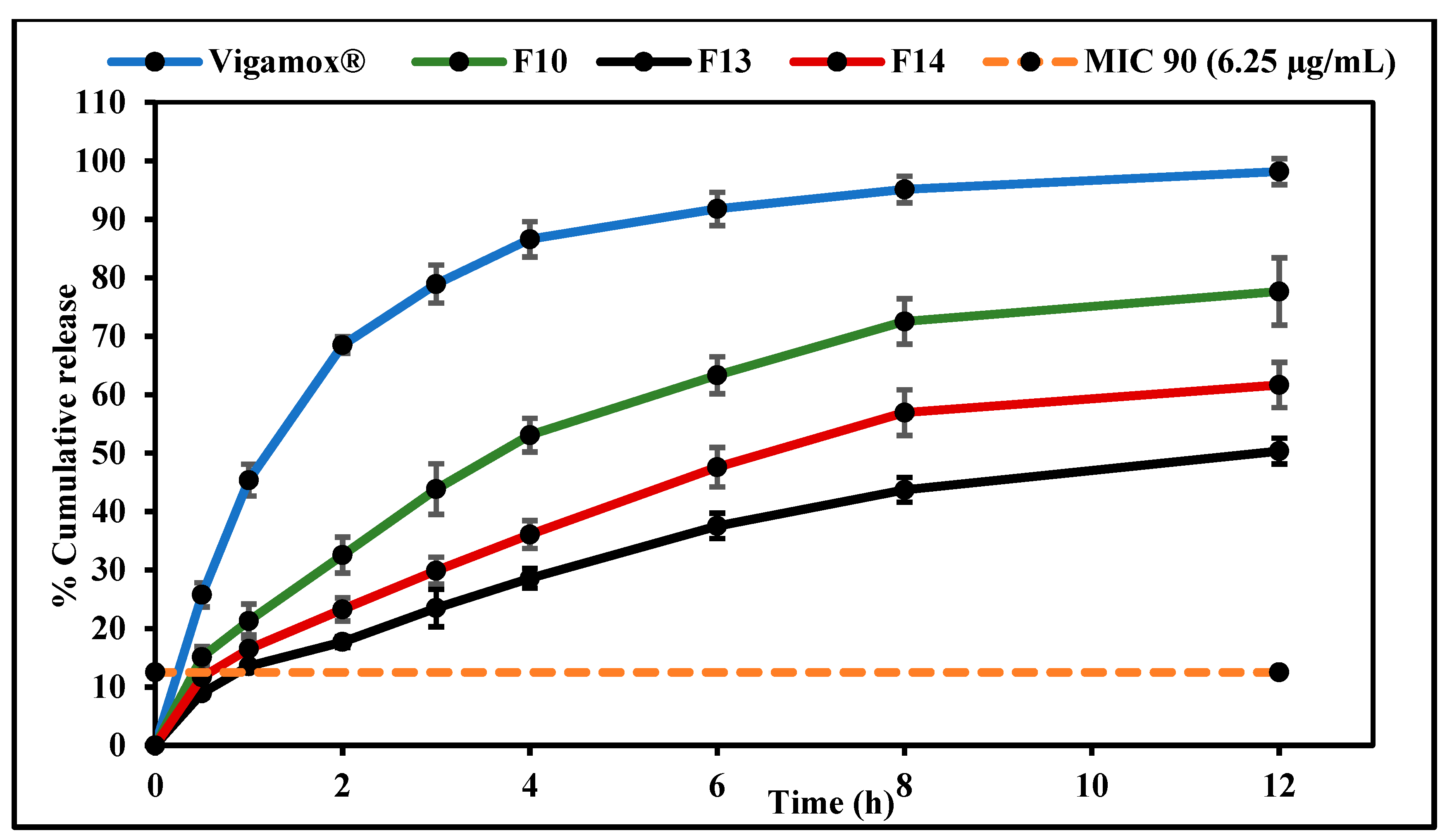
3.10. In Vitro Release Studies
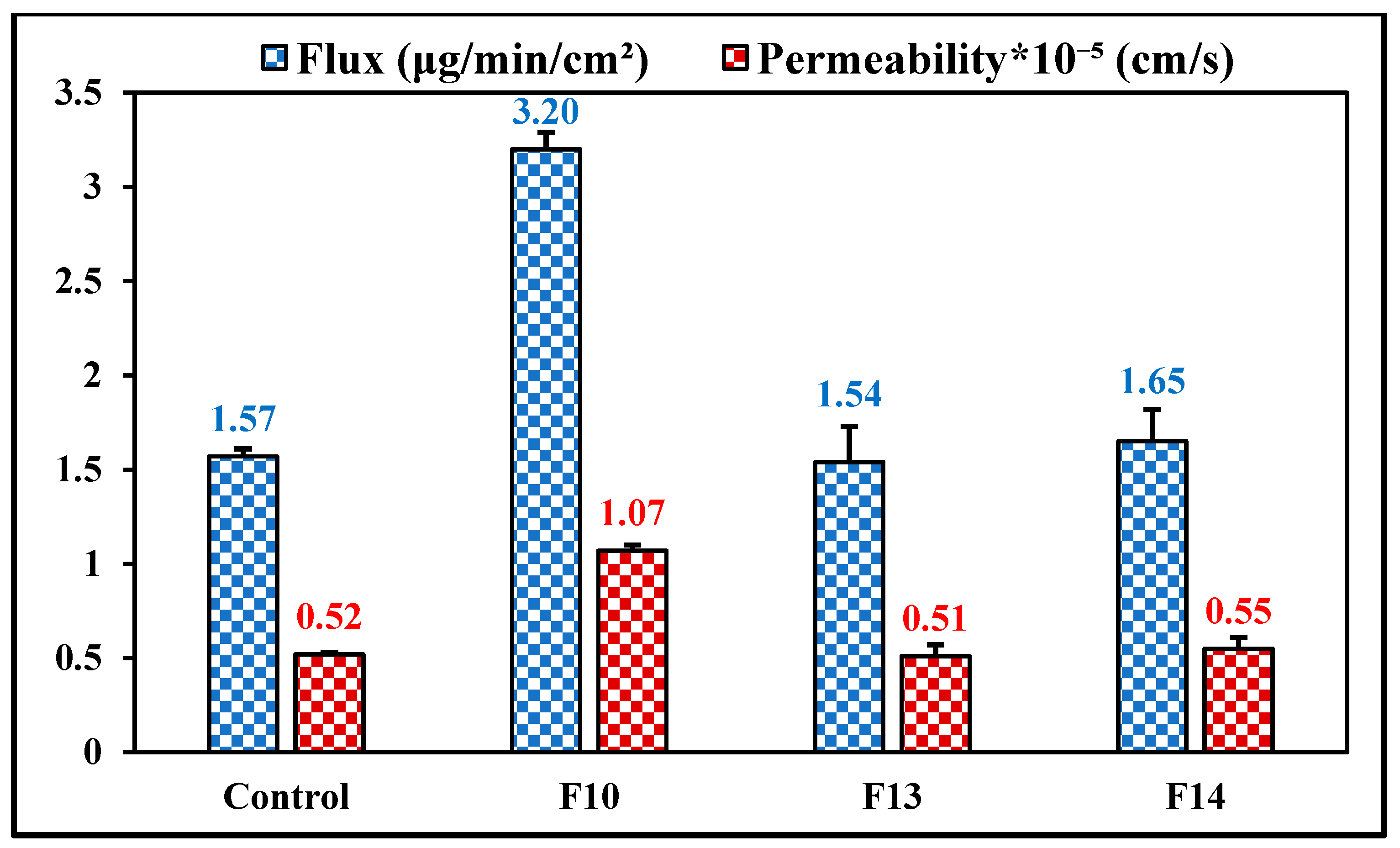
3.11. Ex Vivo Transcorneal Permeation
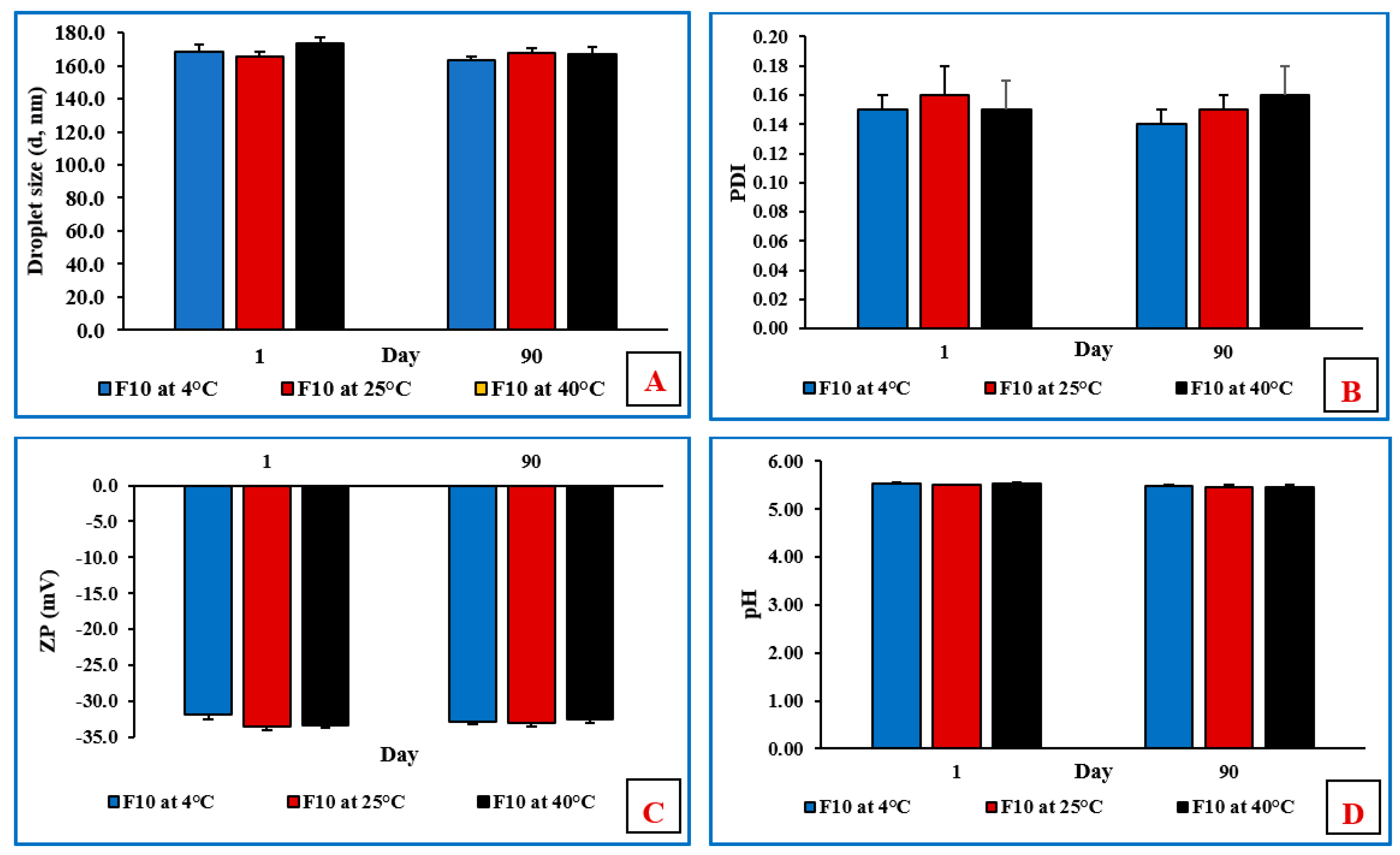
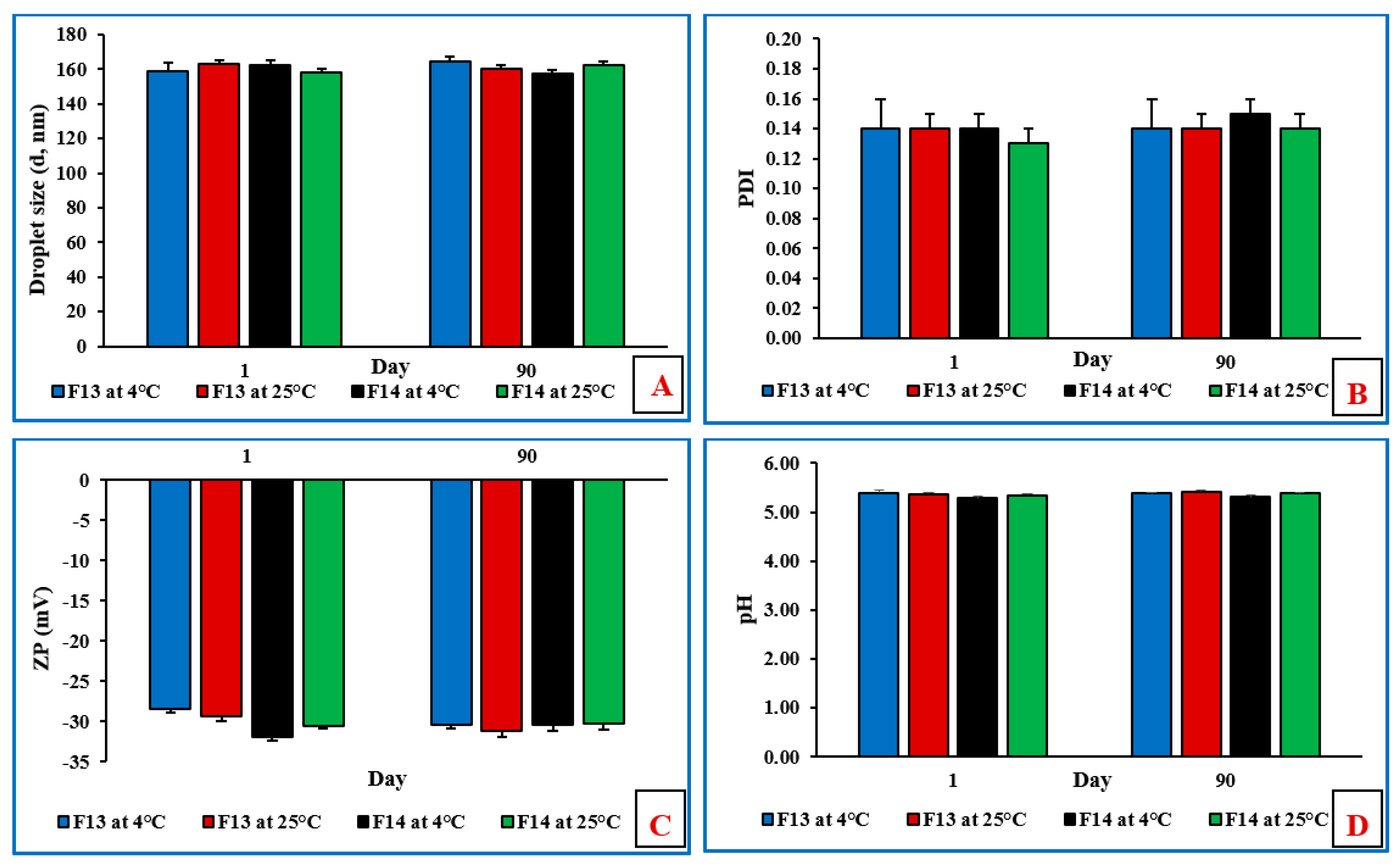
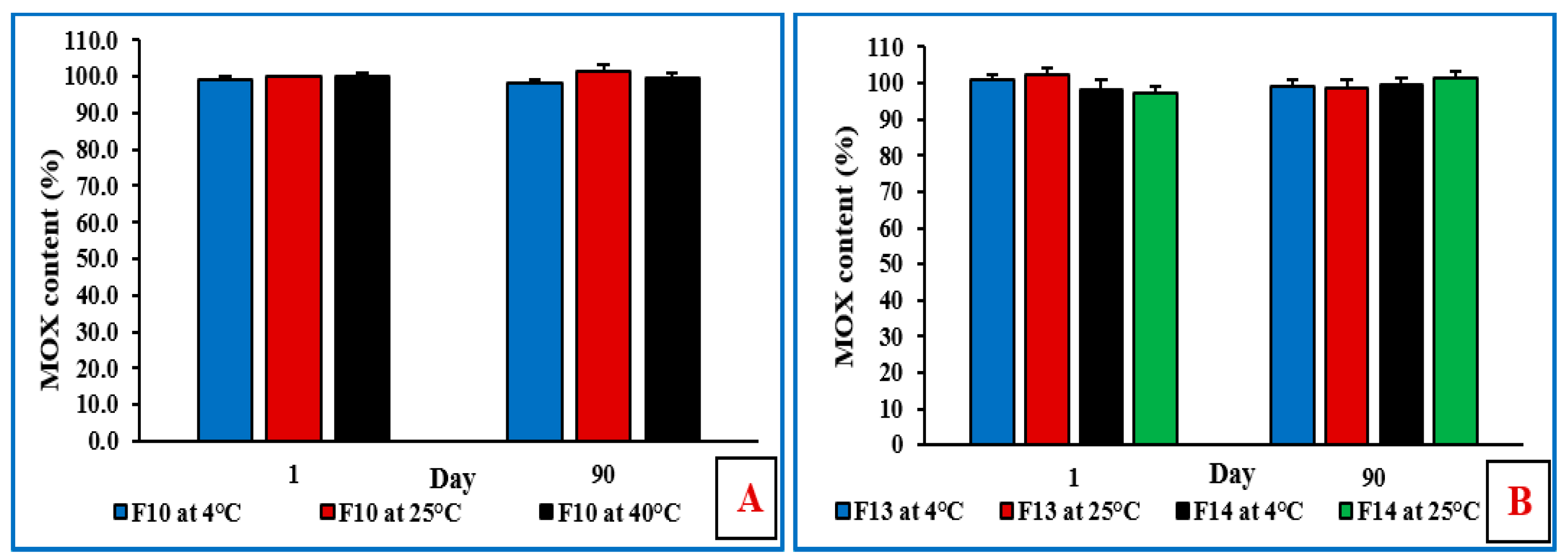
3.12. Stability Studies of NE and Mucoadhesive NE Formulations
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Teweldemedhin, M.; Gebreyesus, H.; Atsbaha, A.H.; Asgedom, S.W.; Saravanan, M. Bacterial Profile of Ocular Infections: A Systematic Review. BMC Ophthalmol. 2017, 17, 212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowalski, R.P.; Dhaliwal, D.K. Ocular Bacterial Infections: Current and Future Treatment Options. Expert Rev. Anti Infect. Ther. 2005, 3, 131–139. [Google Scholar] [CrossRef]
- Ballouz, D.; Maganti, N.; Tuohy, M.; Errickson, J.; Woodward, M.A. Medication Burden for Patients with Bacterial Keratitis. Cornea 2019, 38, 933–937. [Google Scholar] [CrossRef] [PubMed]
- Youssef, A.A.A.; Dudhipala, N.; Majumdar, S. Dual Drug Loaded Lipid Nanocarrier Formulations for Topical Ocular Applications. Int. J. Nanomed. 2022, 17, 2283–2299. [Google Scholar] [CrossRef]
- Ung, L.; Bispo, P.J.M.; Shanbhag, S.S.; Gilmore, M.S.; Chodosh, J. The Persistent Dilemma of Microbial Keratitis: Global Burden, Diagnosis, and Antimicrobial Resistance. Surv. Ophthalmol. 2019, 64, 255–271. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.; Cavuoto, K.M.; Alfonso, E.C. Bacterial Keratitis. In Infections of the Cornea and Conjunctiva; Springer: Berlin/Heidelberg, Germany, 2021; pp. 85–104. [Google Scholar]
- Smith, A.F.; Waycaster, C. Estimate of the Direct and Indirect Annual Cost of Bacterial Conjunctivitis in the United States. BMC Ophthalmol. 2009, 9, 13. [Google Scholar] [CrossRef] [Green Version]
- Lemp, M.A.; Nichols, K.K. Blepharitis in the United States 2009: A Survey-Based Perspective on Prevalence and Treatment. Ocul. Surf. 2009, 7, S1–S14. [Google Scholar] [CrossRef]
- Durand, M.L. Endophthalmitis. Clin. Microbiol. Infect. 2013, 19, 227–234. [Google Scholar] [CrossRef] [Green Version]
- Hooper, D.C. Mechanisms of Quinolone Resistance. Quinolone Antimicrob. Agents 2003, 41–67. [Google Scholar] [CrossRef]
- Kowalski, R.P.; Dhaliwal, D.K.; Karenchak, L.M.; Romanowski, E.G.; Mah, F.S.; Ritterband, D.C.; Gordon, Y.J. Gatifloxacin and Moxifloxacin: An in Vitro Susceptibility Comparison to Levofloxacin, Ciprofloxacin, and Ofloxacin Using Bacterial Keratitis Isolates. Am. J. Ophthalmol. 2003, 136, 500–505. [Google Scholar] [CrossRef]
- Belfort, R.; Gabriel, L.; Martins Bispo, P.J.; Muccioli, C.; Zacharias Serapicos, P.C.; Clark, L.; Bell, B.; Bartell, J.; Stroman, D.W.; Höfling-Lima, A.L. Safety and Efficacy of Moxifloxacin-Dexamethasone Eyedrops as Treatment for Bacterial Ocular Infection Associated with Bacterial Blepharitis. Adv. Ther. 2012, 29, 416–426. [Google Scholar] [CrossRef] [PubMed]
- Pflugfelder, S.C.; Karpecki, P.M.; Perez, V.L. Treatment of Blepharitis: Recent Clinical Trials. Ocul. Surf. 2014, 12, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Arshinoff, S.A.; Modabber, M. Dose and Administration of Intracameral Moxifloxacin for Prophylaxis of Postoperative Endophthalmitis. J. Cataract Refract. Surg. 2016, 42, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Vieira, I.V.; Boianovsky, C.; Saraiva, T.J.; Godoy, R.B.; de Lake, J. Safety and Efficacy of Intracameral Moxifloxacin Injection for Prophylaxis of Endophthalmitis after Phacoemulsification. Arq. Bras. Oftalmol. 2017, 80, 165–167. [Google Scholar] [CrossRef] [PubMed]
- Youssef, A.A.A.; Cai, C.; Dudhipala, N.; Majumdar, S. Design of Topical Ocular Ciprofloxacin Nanoemulsion for the Management of Bacterial Keratitis. Pharmaceuticals 2021, 14, 210. [Google Scholar] [CrossRef] [PubMed]
- Farkouh, A.; Frigo, P.; Czejka, M. Systemic Side Effects of Eye Drops: A Pharmacokinetic Perspective. Clin. Ophthalmol. 2016, 10, 2433–2441. [Google Scholar] [CrossRef] [Green Version]
- Bertino, J.S. Impact of Antibiotic Resistance in the Management of Ocular Infections: The Role of Current and Future Antibiotics. Clin. Ophthalmol. 2009, 3, 507–521. [Google Scholar] [CrossRef] [Green Version]
- Pachigolla, G.; Blomquist, P.; Cavanagh, H.D. Microbial Keratitis Pathogens and Antibiotic Susceptibilities: A 5-Year Review of Cases at an Urban County Hospital in North Texas. Eye Contact Lens 2007, 33, 45–49. [Google Scholar] [CrossRef]
- Jaiswal, M.; Dudhe, R.; Sharma, P.K. Nanoemulsion: An Advanced Mode of Drug Delivery System. 3 Biotech 2015, 5, 123–127. [Google Scholar] [CrossRef] [Green Version]
- Lallemand, F.; Daull, P.; Benita, S.; Buggage, R.; Garrigue, J.-S. Successfully Improving Ocular Drug Delivery Using the Cationic Nanoemulsion, Novasorb. J. Drug Deliv. 2012, 2012, 1–16. [Google Scholar] [CrossRef]
- Singh, M.; Bharadwaj, S.; Lee, K.E.; Kang, S.G. Therapeutic Nanoemulsions in Ophthalmic Drug Administration: Concept in Formulations and Characterization Techniques for Ocular Drug Delivery. J. Control. Release 2020, 328, 895–916. [Google Scholar] [CrossRef] [PubMed]
- Ammar, H.O.; Salama, H.A.; Ghorab, M.; Mahmoud, A.A. Nanoemulsion as a Potential Ophthalmic Delivery System for Dorzolamide Hydrochloride. AAPS PharmSciTech 2009, 10, 808–819. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, C.; Dudhipala, N.; Thakkar, R.; Mehraj, T.; Marathe, S.; Gul, W.; ElSohly, M.A.; Murphy, B.; Majumdar, S. Effect of Surfactant Concentration and Sterilization Process on Intraocular Pressure–Lowering Activity of Δ9-Tetrahydrocannabinol-Valine-Hemisuccinate (NB1111) Nanoemulsions. Drug Deliv. Transl. Res. 2021, 11, 2096–2107. [Google Scholar] [CrossRef]
- Sweeney, C.; Dudhipala, N.; Thakkar, R.; Mehraj, T.; Marathe, S.; Gul, W.; ElSohly, M.A.; Murphy, B.; Majumdar, S. Impact of Mucoadhesive Agent Inclusion on the Intraocular Pressure Lowering Profile of Δ9-Tetrahydrocannabinol-Valine-Hemisuccinate Loaded Nanoemulsions in New Zealand White Rabbits. Int. J. Pharm. 2022, 616, 121564. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, A. The Use of Mucoadhesive Polymers in Ocular Drug Delivery. Adv. Drug Deliv. Rev. 2005, 57, 1595–1639. [Google Scholar] [CrossRef]
- Tundisi, L.L.; Mostaço, G.B.; Carricondo, P.C.; Petri, D.F.S. Hydroxypropyl Methylcellulose: Physicochemical Properties and Ocular Drug Delivery Formulations. Eur. J. Pharm. Sci. 2021, 159, 105736. [Google Scholar] [CrossRef]
- Kurakula, M.; Rao, G.S.N.K. Pharmaceutical Assessment of Polyvinylpyrrolidone (PVP): As Excipient from Conventional to Controlled Delivery Systems with a Spotlight on COVID-19 Inhibition. J. Drug Deliv. Sci. Technol. 2020, 60, 102046. [Google Scholar] [CrossRef] [PubMed]
- Razzaq, S.N.; Khan, I.U.; Mariam, I.; Razzaq, S.S. Stability Indicating HPLC Method for the Simultaneous Determination of Moxifloxacin and Prednisolone in Pharmaceutical Formulations. Chem. Central J. 2012, 6, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balguri, S.P.; Adelli, G.R.; Janga, K.Y.; Bhagav, P.; Majumdar, S. Ocular Disposition of Ciprofloxacin from Topical, PEGylated Nanostructured Lipid Carriers: Effect of Molecular Weight and Density of Poly (Ethylene) Glycol. Int. J. Pharm. 2017, 529, 32–43. [Google Scholar] [CrossRef]
- Dudhipala, N.; Ettireddy, S.; Youssef, A.A.A.; Puchchakayala, G. Cyclodextrin Complexed Lipid Nanoparticles of Irbesartan for Oral Applications: Design, Development, and In Vitro Characterization. Molecules 2021, 26, 7538. [Google Scholar] [CrossRef]
- Thakkar, R.; Komanduri, N.; Dudhipala, N.; Tripathi, S.; Repka, M.A.; Majumdar, S. Development and Optimization of Hot-Melt Extruded Moxifloxacin Hydrochloride Inserts, for Ocular Applications, Using the Design of Experiments. Int. J. Pharm. 2021, 603, 120676. [Google Scholar] [CrossRef] [PubMed]
- Narang, A.S.; Delmarre, D.; Gao, D. Stable Drug Encapsulation in Micelles and Microemulsions. Int. J. Pharm. 2007, 345, 9–25. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Moulik, S.P. Biocompatible Microemulsions and Their Prospective Uses in Drug Delivery. J. Pharm. Sci. 2008, 97, 22–45. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.-C.; Qi, H.-P.; Bai, J.-H.; Huang, L.; Cui, H. Effects of Oleic Acid on the Corneal Permeability of Compounds and Evaluation of Its Ocular Irritation of Rabbit Eyes. Curr. Eye Res. 2014, 39, 1161–1168. [Google Scholar] [CrossRef]
- Sita, V.G.; Vavia, P. Bromocriptine Nanoemulsion-Loaded Transdermal Gel: Optimization Using Factorial Design, In Vitro and In Vivo Evaluation. AAPS PharmSciTech 2020, 21, 80. [Google Scholar] [CrossRef]
- Thakkar, H.P.; Khunt, A.; Dhande, R.D.; Patel, A.A. Formulation and Evaluation of Itraconazole Nanoemulsion for Enhanced Oral Bioavailability. J. Microencapsul. 2015, 32, 559–569. [Google Scholar] [CrossRef]
- Youssef, A.; Dudhipala, N.; Majumdar, S. Ciprofloxacin Loaded Nanostructured Lipid Carriers Incorporated into In-Situ Gels to Improve Management of Bacterial Endophthalmitis. Pharmaceutics 2020, 12, 572. [Google Scholar] [CrossRef]
- Khames, A.; Khaleel, M.A.; El-Badawy, M.F.; El-Nezhawy, A.O.H. Natamycin Solid Lipid Nanoparticles—Sustained Ocular Delivery System of Higher Corneal Penetration against Deep Fungal Keratitis: Preparation and Optimization. Int. J. Nanomed. 2019, 14, 2515–2531. [Google Scholar] [CrossRef] [Green Version]
- Kulkarni, S.A.; Feng, S.-S. Effects of Particle Size and Surface Modification on Cellular Uptake and Biodistribution of Polymeric Nanoparticles for Drug Delivery. Pharm. Res. 2013, 30, 2512–2522. [Google Scholar] [CrossRef]
- Kou, L.; Sun, J.; Zhai, Y.; He, Z. The Endocytosis and Intracellular Fate of Nanomedicines: Implication for Rational Design. Asian J. Pharm. Sci. 2013, 8, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.; Gu, Y.; Cui, H. Moringa Oil/Chitosan Nanoparticles Embedded Gelatin Nanofibers for Food Packaging against Listeria Monocytogenes and Staphylococcus Aureus on Cheese. Food Packag. Shelf Life 2019, 19, 86–93. [Google Scholar] [CrossRef]
- Makwana, S.B.; Patel, V.A.; Parmar, S.J. Development and Characterization of In-Situ Gel for Ophthalmic Formulation Containing Ciprofloxacin Hydrochloride. Results Pharma Sci. 2016, 6, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almáši, M.; Matiašová, A.A.; Šuleková, M.; Beňová, E.; Ševc, J.; Váhovská, L.; Lisnichuk, M.; Girman, V.; Zeleňáková, A.; Hudák, A.; et al. In Vivo Study of Light-Driven Naproxen Release from Gated Mesoporous Silica Drug Delivery System. Sci. Rep. 2021, 11, 20191. [Google Scholar] [CrossRef] [PubMed]
- Sterner, O.; Karageorgaki, C.; Zürcher, M.; Zürcher, S.; Scales, C.W.; Fadli, Z.; Spencer, N.D.; Tosatti, S.G. Reducing Friction in the Eye: A Comparative Study of Lubrication by Surface-Anchored Synthetic and Natural Ocular Mucin Analogues. ACS Appl. Mater. Interfaces 2017, 9, 20150–20160. [Google Scholar] [CrossRef] [Green Version]
- Abelson, M.B.; Udell, I.J.; Weston, J.H. Normal Human Tear PH by Direct Measurement. Arch. Ophthalmol. 1981, 99, 301. [Google Scholar] [CrossRef]
- Uddin, M.S.; Mamun, A.A.; Kabir, M.T.; Setu, J.R.; Zaman, S.; Begum, Y.; Amran, M.S. Quality Control Tests for Ophthalmic Pharmaceuticals: Pharmacopoeial Standards and Specifications. J. Adv. Med. Pharm. Sci. 2017, 14, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Peterson, J.M.; Fixman, M. Viscosity of Polymer Solutions. J. Chem. Phys. 1963, 39, 2516–2523. [Google Scholar] [CrossRef]
- Astley, R.; Miller, F.C.; Mursalin, M.H.; Coburn, P.S.; Callegan, M.C. An Eye on Staphylococcus Aureus Toxins: Roles in Ocular Damage and Inflammation. Toxins 2019, 11, 356. [Google Scholar] [CrossRef] [Green Version]
- Tayel, S.A.; El-Nabarawi, M.A.; Tadros, M.I.; Abd-Elsalam, W.H. Promising Ion-Sensitive in Situ Ocular Nanoemulsion Gels of Terbinafine Hydrochloride: Design, in Vitro Characterization and in Vivo Estimation of the Ocular Irritation and Drug Pharmacokinetics in the Aqueous Humor of Rabbits. Int. J. Pharm. 2013, 443, 293–305. [Google Scholar] [CrossRef]
- Akhter, S.; Anwar, M.; Siddiqui, M.A.; Ahmad, I.; Ahmad, J.; Ahmad, M.Z.; Bhatnagar, A.; Ahmad, F.J. Improving the Topical Ocular Pharmacokinetics of an Immunosuppressant Agent with Mucoadhesive Nanoemulsions: Formulation Development, in-Vitro and in-Vivo Studies. Colloids Surf. B Biointerfaces 2016, 148, 19–29. [Google Scholar] [CrossRef]
- Khare, A.; Grover, K.; Pawar, P.; Singh, I. Mucoadhesive Polymers for Enhancing Retention in Ocular Drug Delivery: A Critical Review. Rev. Adhes. Adhes. 2014, 2, 467–502. [Google Scholar] [CrossRef]
- Agarwal, P.; Rupenthal, I.D. In Vitro and Ex Vivo Corneal Penetration and Absorption Models. Drug Deliv. Transl. Res. 2016, 6, 634–647. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.; Nair, A.B.; Jacob, S.; Patel, R.K.; Shah, H.; Shehata, T.M.; Morsy, M.A. Nanoemulsion Based Vehicle for Effective Ocular Delivery of Moxifloxacin Using Experimental Design and Pharmacokinetic Study in Rabbits. Pharmaceutics 2019, 11, 230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gade, S.; Patel, K.K.; Gupta, C.; Anjum, M.M.; Deepika, D.; Agrawal, A.K.; Singh, S. An Ex Vivo Evaluation of Moxifloxacin Nanostructured Lipid Carrier Enriched In Situ Gel for Transcorneal Permeation on Goat Cornea. J. Pharm. Sci. 2019, 108, 2905–2916. [Google Scholar] [CrossRef]
- Sebastián-Morelló, M.; Calatayud-Pascual, M.A.; Rodilla, V.; Balaguer-Fernández, C.; López-Castellano, A. Ex Vivo Rabbit Cornea Diffusion Studies with a Soluble Insert of Moxifloxacin. Drug Deliv. Transl. Res. 2018, 8, 132–139. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Oil | Solubility | Oil | Solubility |
|---|---|---|---|
| Soybean oil | (−) | Miglyol® 829 | (−) |
| Castor oil | (−) | Labrafac® Lipophile WL 1349 | (−) |
| Oleic acid | (+) | Transcutol® P | (−) |
| Sesame oil | (−) | Isopropyl Myristate, NF | (−) |
| Formulation Composition (% w/v) | ||||||
|---|---|---|---|---|---|---|
| Code * | Oleic Acid | Tween® 80 | HPMC K4M | PVP K29/32 | Milli-Q Water Up to (mL) | Visual Examination |
| F1 | 1.0 | 0.75 | – | – | 10 | Precipitation on day 2 |
| F2 | 1.0 | 2.0 | – | – | 10 | Precipitation on day 2 |
| F3 | 1.0 | 3.0 | – | – | 10 | Precipitation on day 2 |
| F4 | 1.0 | 4.0 | – | – | 10 | Precipitation on day 2 |
| F5 | 2.5 | 0.75 | – | – | 10 | Precipitation on day 4 |
| F6 | 2.5 | 2.0 | – | – | 10 | Precipitation on day 6 |
| F7 | 2.5 | 3.0 | – | – | 10 | Precipitation on day 10 |
| F8 | 2.5 | 4.0 | – | – | 10 | Precipitation on day 17 |
| F9 | 5.0 | 0.75 | – | – | 10 | Cracking on day 4 |
| F10 | 5.0 | 2.0 | – | – | 10 | Stable |
| F11 | 5.0 | 3.0 | – | – | 10 | Stable |
| F12 | 5.0 | 4.0 | – | – | 10 | Stable |
| F13 | 5.0 | 2.0 | 0.4 | – | 10 | Stable |
| F14 | 5.0 | 2.0 | – | 0.4 | 10 | Stable |
| Parameter | F10 | F11 | F12 |
|---|---|---|---|
| Droplet size (d.nm) | 174.1 ± 5.9 | 150.2 ± 2.2 | 124.7 ± 1.5 |
| Polydispersity index | 0.16 ± 0.01 | 0.14 ± 0.01 | 0.15 ± 0.02 |
| Zeta potential (mV) | −33.3 ± 0.3 | −33.4 ± 0.5 | −32.1 ± 1.2 |
| Viscosity (cP) | 5.6 ± 0.5 | 5.6 ± 0.2 | 5.7 ± 0.4 |
| Drug content (%) | 100.8 ± 7.3 | 101.7 ± 0.3 | 99.1 ± 3.8 |
| Parameter | F10 | F13 | F14 |
|---|---|---|---|
| Droplet size (d.nm) | 165.5 ± 3.2 | 163.4 ± 2.0 | 157.8 ± 2.6 |
| Polydispersity index | 0.16 ± 0.02 | 0.14 ± 0.02 | 0.15 ± 0.01 |
| Zeta potential (mV) | −33.5 ± 1.5 | −31.3 ± 0.6 | −30.5 ± 0.4 |
| Drug content (%) | 99.0 ± 1.2 | 101.0 ± 1.3 | 98.3 ± 2.5 |
| pH | 5.5 ± 0.1 | 5.4 ± 0.0 | 5.4 ± 0.1 |
| Viscosity (cP) | 5.6 ± 0.5 | 26.5 ± 0.9 | 27.9 ± 0.3 |
| Code | Day | Storage at 4 ± 2 °C | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| DS (d, nm) | PDI | ZP (mV) | pH | Drug Content (%) | |||||||
| Sterilization Stage | |||||||||||
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | ||
| F10 | 0 | 168.3 ± 4.2 | 162.9 ± 4.8 | 0.16 ± 0.01 | 0.16 ± 0.01 | −32.5 ± 0.5 | −33.5 ± 0.6 | 5.4 ± 0.1 | 5.3 ± 0.1 | 98.3 ± 2.3 | 101.3 ± 4.3 |
| 30 | 163.9 ± 3.2 | 167.5 ± 4.0 | 0.16 ± 0.02 | 0.15 ± 0.02 | −31.8 ± 1.1 | −33.2 ± 0.4 | 5.4 ± 0.1 | 5.4 ± 0.1 | 101.5 ± 3.8 | 98.2 ± 4.3 | |
| F13 | 0 | 160.2 ± 3.0 | 166.2 ± 2.4 | 0.17 ± 0.01 | 0.16 ± 0.01 | −33.0 ± 0.7 | −34.4 ± 0.6 | 5.3 ± 0.1 | 5.4 ± 0.1 | 98.5 ± 4.7 | 99.1 ± 2.5 |
| 30 | 165.3 ± 2.3 | 161.4 ± 3.8 | 0.16 ± 0.01 | 0.16 ± 0.03 | −32.5 ± 0.3 | −34.1 ± 0.2 | 5.4 ± 0.1 | 5.4 ± 0.1 | 102.3 ± 2.6 | 98.7 ± 2.5 | |
| F14 | 0 | 172.1 ± 2.8 | 163.0 ± 3.7 | 0.17 ± 0.02 | 0.15 ± 0.02 | −33.4 ± 0.6 | −31.8 ± 1.0 | 5.5 ± 0.1 | 5.3 ± 0.1 | 99.1 ± 3.0 | 103.5 ± 3.5 |
| 30 | 164.7 ± 2.9 | 167.5 ± 4.2 | 0.16 ± 0.01 | 0.17 ± 0.01 | −31.7 ± 0.5 | −33.1 ± 1.3 | 5.3 ± 0.1 | 5.4 ± 0.1 | 97.5 ± 3.5 | 98.2 ± 3.0 | |
| Code | Day | Storage at 25 ± 2 °C | |||||||||
| F10 | 0 | 164.7 ± 1.5 | 169.9 ± 2.5 | 0.17 ± 0.01 | 0.16 ± 0.03 | −33.5 ± 1.3 | −33.5 ± 2.0 | 5.5 ± 0.1 | 5.4 ± 0.1 | 96.5 ± 4.7 | 98.8 ± 2.8 |
| 30 | 160.5 ± 4.6 | 167.1 ± 2.0 | 0.17 ± 0.01 | 0.16 ± 0.01 | −31.5 ± 0.3 | −31.1 ± 1.2 | 5.4 ± 0.1 | 5.4 ± 0.1 | 98.5 ± 2.5 | 100.5 ± 1.3 | |
| F13 | 0 | 166.2 ± 2.4 | 170.2 ± 5.4 | 0.16 ± 0.02 | 0.17 ± 0.01 | −32.4 ± 0.5 | −31.5 ± 0.7 | 5.5 ± 0.1 | 5.4 ± 0.1 | 102.0 ± 3.5 | 99.2 ± 2.5 |
| 30 | 162.5 ± 3.4 | 166.6 ± 4.2 | 0.16 ± 0.02 | 0.15 ± 0.02 | −34.7 ± 1.5 | −32.0 ± 1.0 | 5.5 ± 0.1 | 5.3 ± 0.1 | 97.6 ± 3.4 | 99.0 ± 4.7 | |
| F14 | 0 | 162.0 ± 2.7 | 168.8 ± 2.4 | 0.17 ± 0.01 | 0.15 ± 0.01 | −34.4 ± 0.5 | −32.7 ± 0.5 | 5.3 ± 0.1 | 5.5 ± 0.1 | 99.0 ± 1.9 | 98.5 ± 3.1 |
| 30 | 167.4 ± 4.9 | 165.4 ± 5.0 | 0.17 ± 0.01 | 0.15 ± 0.02 | −32.5 ± 0.7 | −33.3 ± 0.4 | 5.4 ± 0.1 | 5.4 ± 0.1 | 103.1 ± 2.7 | 98.9 ± 3.3 | |
| Formulation | MIC 90 (µg/mL) against MRSA |
|---|---|
| F10 | 6.25 |
| Placebo F10 | NA |
| F13 | 6.25 |
| Placebo F13 | NA |
| F14 | 6.25 |
| Placebo F14 | NA |
| Vigamox® | 6.25 |
| MOX-HCL-S | 6.25 |
| Equation | Q0 − Q = kt | ln Q = kt | Q0 − Q = kt1/2 | log (Q0 − Q) = n log t + log k | |
|---|---|---|---|---|---|
| Model | Zero-Order | First-Order | Higuchi | Korsmeyer–Peppas | |
| R2 | R2 | R2 | R2 | n | |
| F10 | 0.8388 | 0.9520 | 0.9786 | 0.9991 | 0.7 |
| F13 | 0.9112 | 0.9594 | 0.9906 | 0.9967 | 0.6 |
| F14 | 0.8924 | 0.9532 | 0.9885 | 0.9990 | 0.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Youssef, A.A.A.; Thakkar, R.; Senapati, S.; Joshi, P.H.; Dudhipala, N.; Majumdar, S. Design of Topical Moxifloxacin Mucoadhesive Nanoemulsion for the Management of Ocular Bacterial Infections. Pharmaceutics 2022, 14, 1246. https://doi.org/10.3390/pharmaceutics14061246
Youssef AAA, Thakkar R, Senapati S, Joshi PH, Dudhipala N, Majumdar S. Design of Topical Moxifloxacin Mucoadhesive Nanoemulsion for the Management of Ocular Bacterial Infections. Pharmaceutics. 2022; 14(6):1246. https://doi.org/10.3390/pharmaceutics14061246
Chicago/Turabian StyleYoussef, Ahmed Adel Ali, Ruchi Thakkar, Samir Senapati, Poorva H. Joshi, Narendar Dudhipala, and Soumyajit Majumdar. 2022. "Design of Topical Moxifloxacin Mucoadhesive Nanoemulsion for the Management of Ocular Bacterial Infections" Pharmaceutics 14, no. 6: 1246. https://doi.org/10.3390/pharmaceutics14061246