
Enhanced Skin Delivery of Therapeutic Peptides Using Spicule-Based Topical Delivery Systems


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Preparation and Characterization of Sponge Spicules
2.3. Preparation and Characterization of Liposomal Systems
2.4. Skin Penetration Study In Vitro
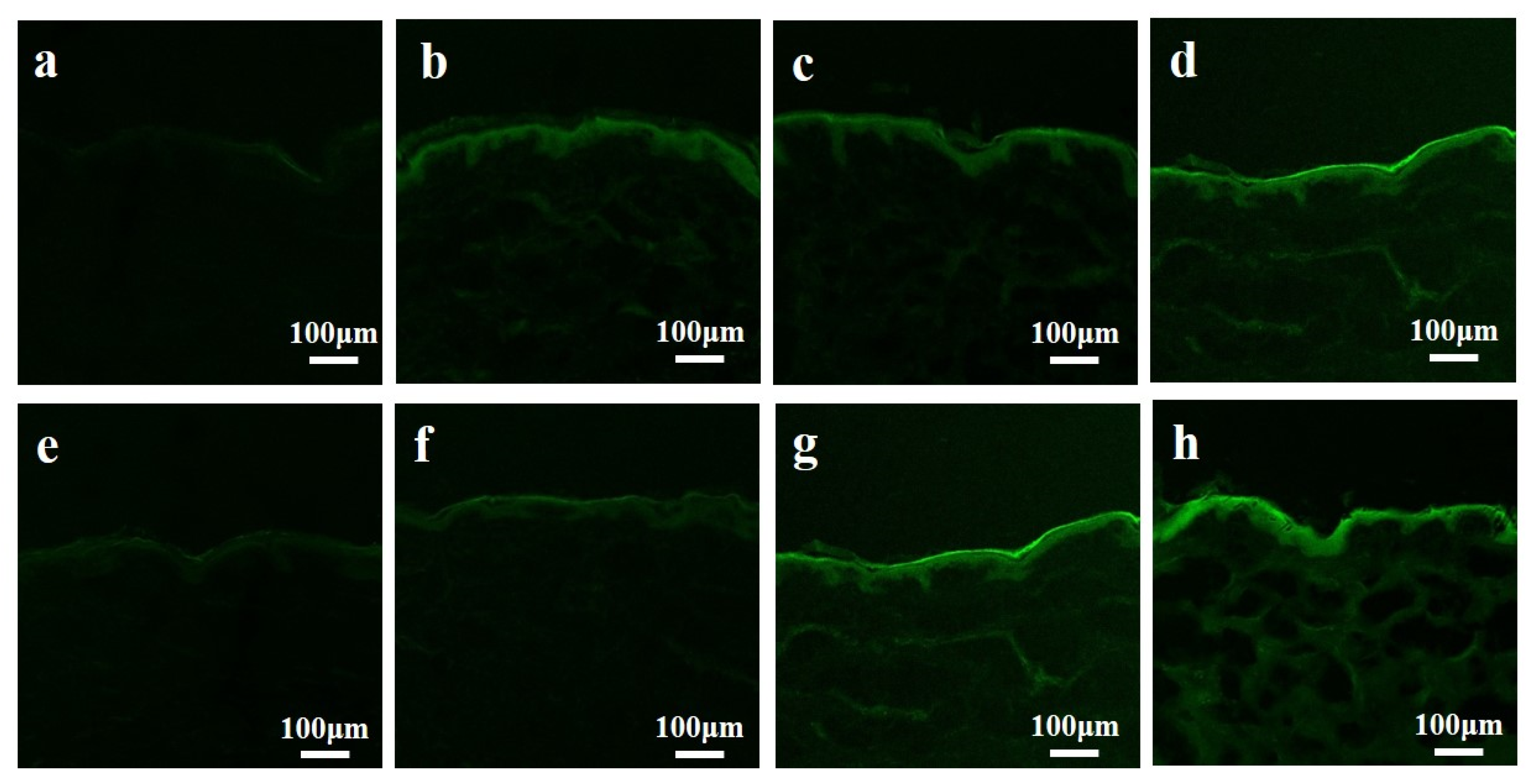
2.5. Confocal Microscopy Study
2.6. Development of Diabetic Animal Models and Psoriatic Animal Models
2.7. Treatment of Diabetes In Vivo
2.8. Treatment of Psoriasis In Vivo
2.9. Statistical Analysis
3. Results
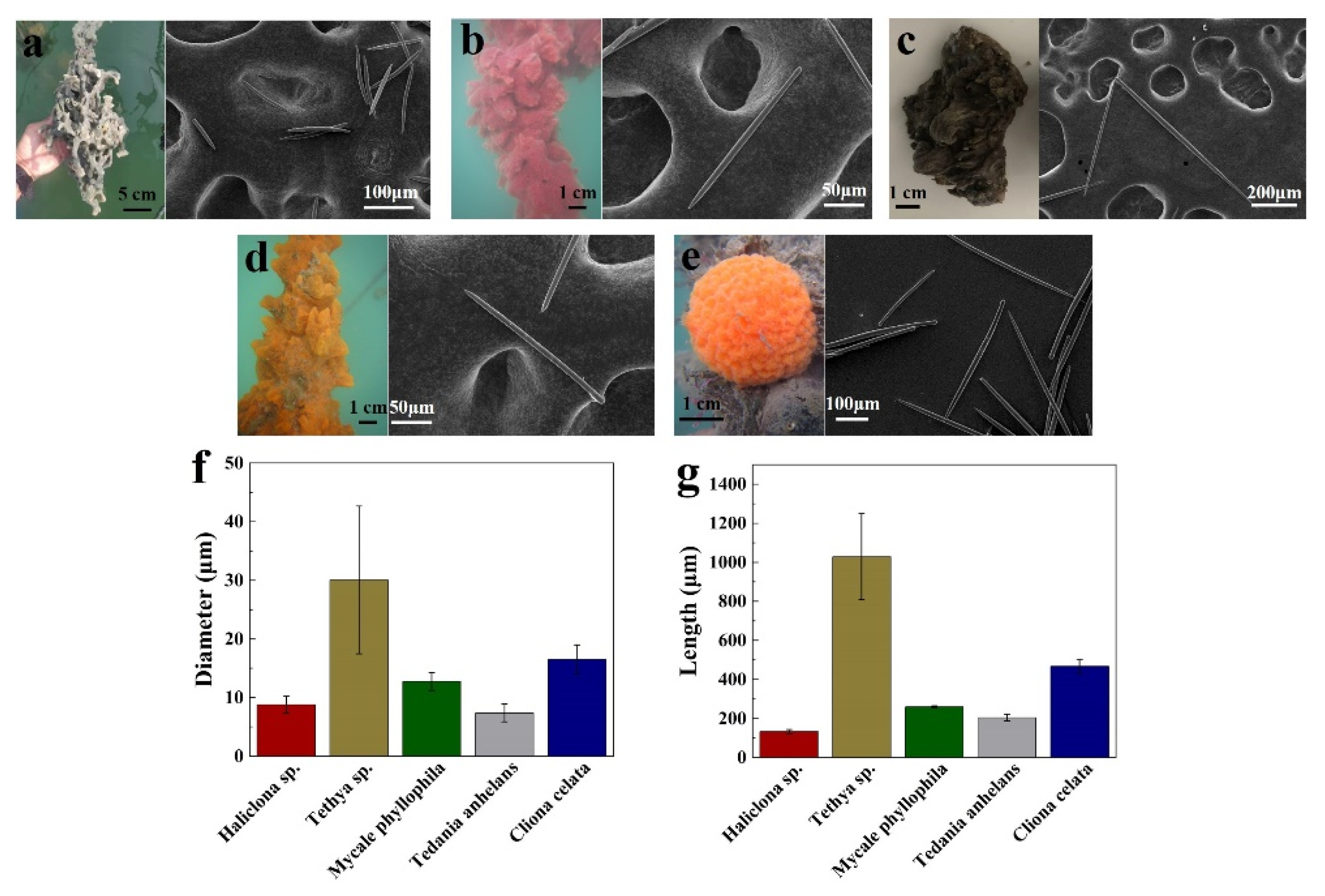
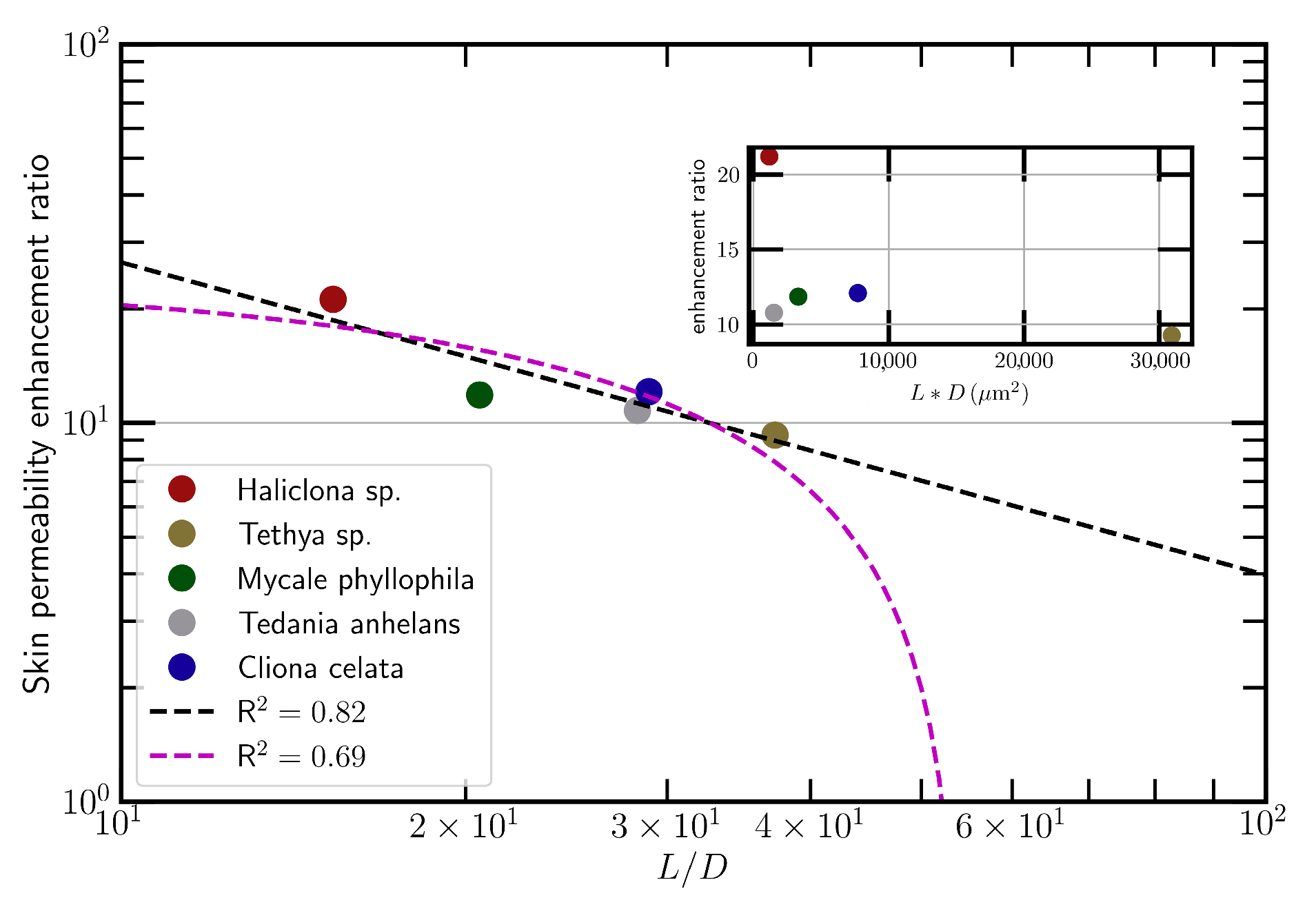
3.1. Increased Skin Permeability by Topical Application of Spicules
3.2. Enhanced Transdermal Delivery of Insulin In Vitro
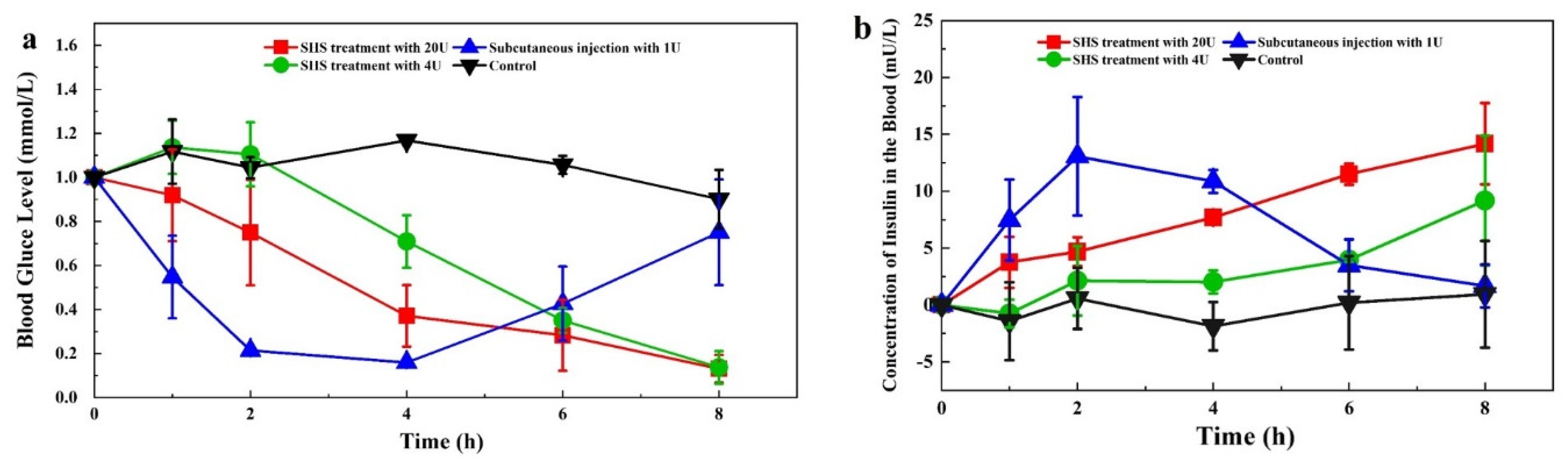
3.3. Transdermal Delivery of Insulin In Vivo
3.4. Enhanced Dermal Delivery of CysA In Vitro
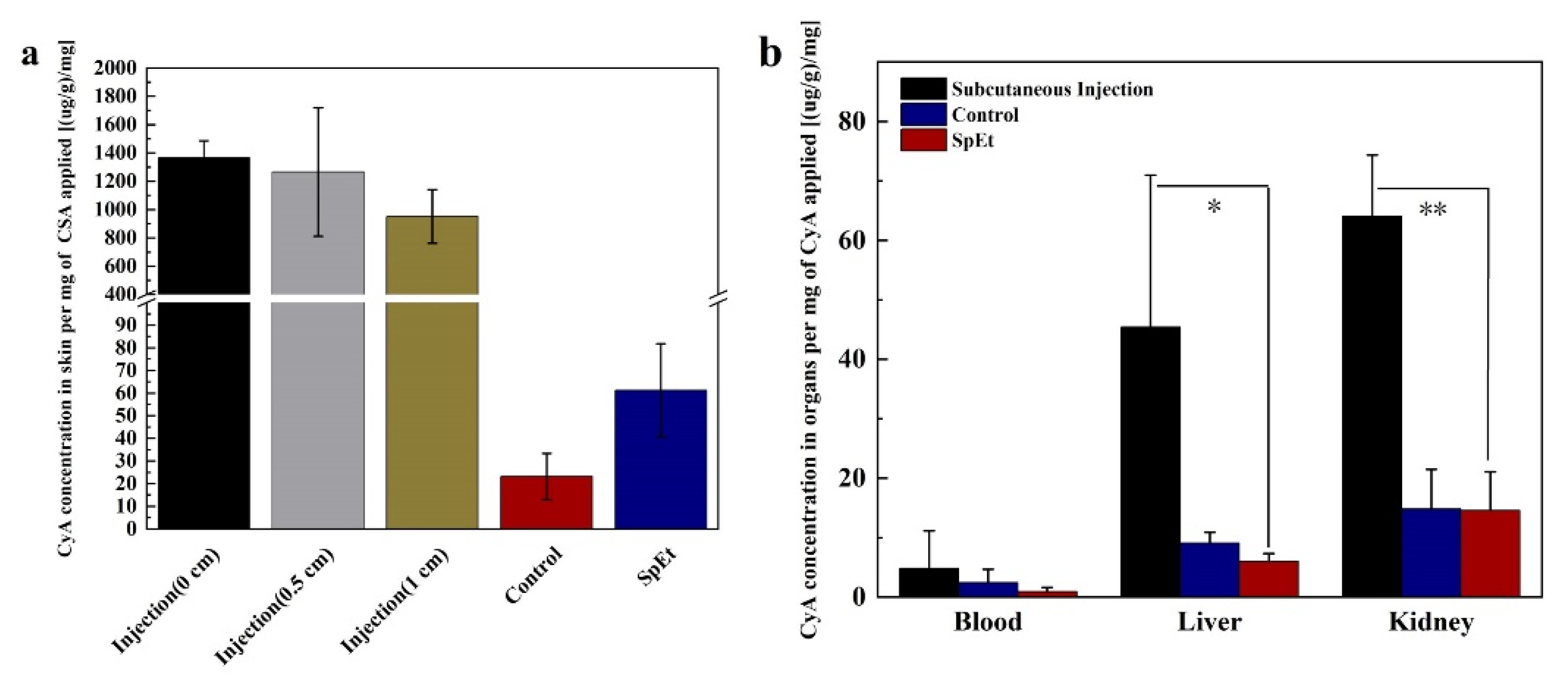
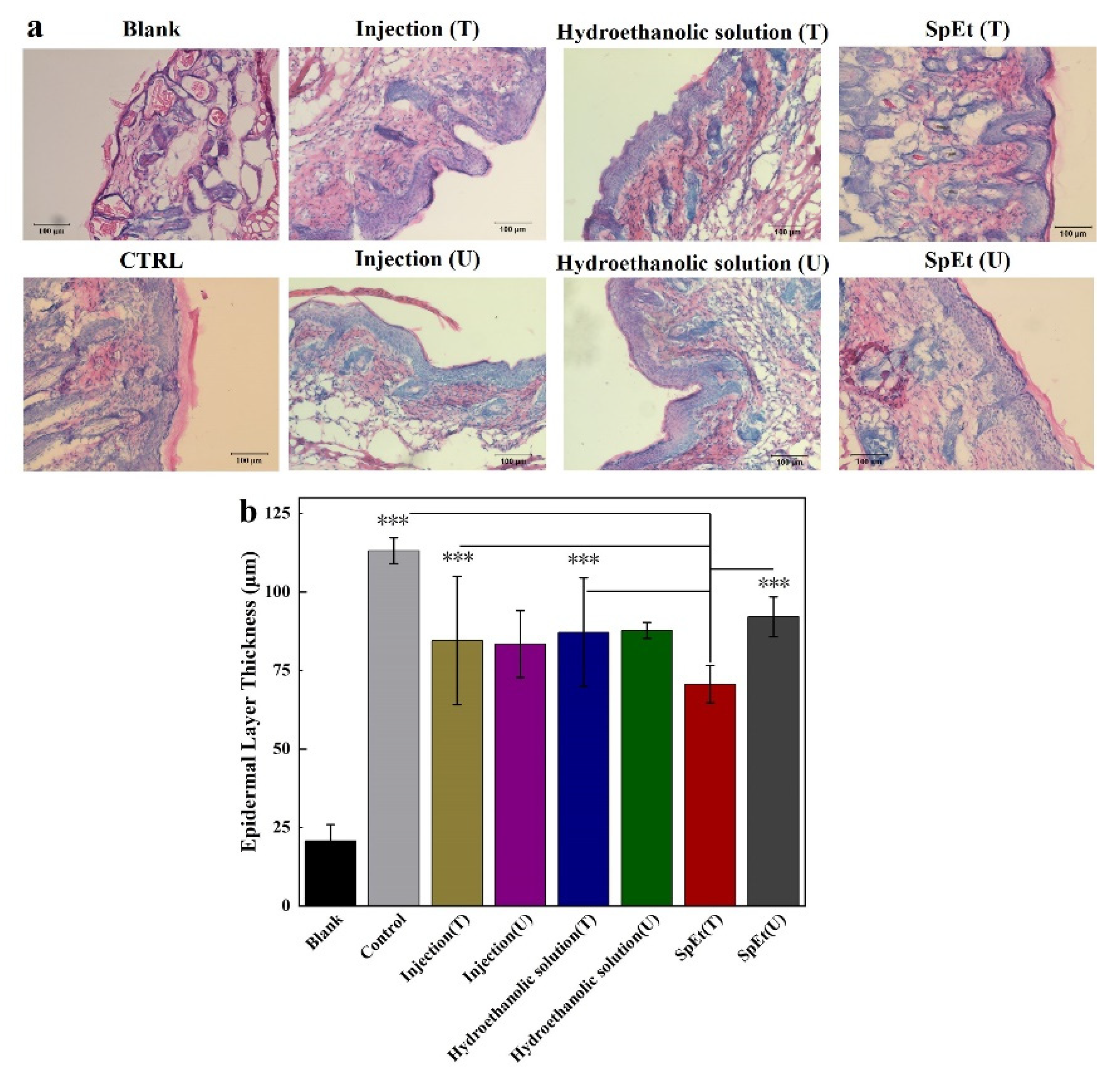
3.5. Dermal Delivery of CysA In Vivo
4. Discussion
5. Conclusions
6. Patent
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lax, R.; Meenan, C. Challenges for Therapeutic Peptides Part 1: On the Inside, Looking Out. Innov. Pharm. Technol. 2012, 42, 54–56. [Google Scholar]
- Grieco, P.; Gomez-Monterrey, I. Natural and synthetic peptides in the cardiovascular diseases: An update on diagnostic and therapeutic potentials. Arch. Biochem. Biophys. 2019, 662, 15–32. [Google Scholar] [CrossRef]
- Liu, W.; Tang, H.; Li, L.; Wang, X.; Yu, Z.; Li, J. Peptide-based therapeutic cancer vaccine: Current trends in clinical application. Cell Prolif. 2021, 54, e13025. [Google Scholar] [CrossRef] [PubMed]
- Marqus, S.; Pirogova, E.; Piva, T.J. Evaluation of the use of therapeutic peptides for cancer treatment. J. Biomed. Sci. 2017, 24, 21. [Google Scholar] [CrossRef] [Green Version]
- Cooper, B.M.; Iegre, J.; DH, O.D.; Ölwegård Halvarsson, M.; Spring, D.R. Peptides as a platform for targeted therapeutics for cancer: Peptide–drug conjugates (PDCs). Chem. Soc. Rev. 2021, 50, 1480–1494. [Google Scholar] [CrossRef] [PubMed]
- Kaspar, A.A.; Reichert, J.M. Future directions for peptide therapeutics development. Drug Discov. Today 2013, 18, 807–817. [Google Scholar] [CrossRef]
- Das, D.; Jaiswal, M.; Khan, F.N.; Ahamad, S.; Kumar, S. PlantPepDB: A manually curated plant peptide database. Sci. Rep. 2020, 10, 2194. [Google Scholar] [CrossRef] [Green Version]
- Fosgerau, K.; Hoffmann, T. Peptide therapeutics: Current status and future directions. Drug Discov. Today 2015, 20, 122–128. [Google Scholar] [CrossRef] [Green Version]
- Torchilin, V.P.; Lukyanov, A.N. Peptide and protein drug delivery to and into tumors: Challenges and solutions. Drug Discov. Today 2003, 8, 259–266. [Google Scholar] [CrossRef]
- Di, L. Strategic Approaches to Optimizing Peptide ADME Properties. AAPS J. 2015, 17, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Eckert, R. Road to clinical efficacy: Challenges and novel strategies for antimicrobial peptide development. Future Microbiol. 2011, 6, 635–651. [Google Scholar] [CrossRef]
- Otvos, L.; Wade, J.D. Current challenges in peptide-based drug discovery. Front. Chem. 2014, 2, 62. [Google Scholar] [CrossRef]
- Pardeshi, N.N.; Qi, W.; Dahl, K.; Caplan, L.; Carpenter, J.F. Microparticles and Nanoparticles Delivered in Intravenous Saline and in an Intravenous Solution of a Therapeutic Antibody Product. J. Pharm. Sci. 2017, 106, 511–520. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.H.; Po, A. Peptide and protein drugs: II. Non-parenteral routes of delivery. Int. J. Pharm. 1991, 75, 117–130. [Google Scholar] [CrossRef]
- Brown, M.B.; Martin, G.P.; Jones, S.A.; Akomeah, F.K. Dermal and transdermal drug delivery systems: Current and future prospects. Drug Deliv. 2006, 13, 175–187. [Google Scholar] [CrossRef] [Green Version]
- Prausnitz, M.R.; Mitragotri, S.; Langer, R. Current status and future potential of transdermal drug delivery. Nat. Rev. Drug Discov. 2004, 3, 115. [Google Scholar] [CrossRef]
- Bos, J.D.; Meinardi, M. The 500 Dalton rule for the skin penetration of chemical compounds and drugs. Exp. Dermatol. 2000, 9, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Thysman, S.; Hanchard, C.; Préat, V. Human calcitonin delivery in rats by iontophoresis. J. Pharm. Pharmacol. 1994, 46, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Vemulapalli, V.; Bai, Y.; Kalluri, H.; Herwadkar, A.; Kim, H.; Davis, S.P.; Friden, P.M.; Banga, A.K. In vivo iontophoretic delivery of salmon calcitonin across microporated skin. J. Pharm. Sci. 2012, 101, 2861–2869. [Google Scholar] [CrossRef] [PubMed]
- Raiman, J.; Koljonen, M.; Huikko, K.; Kostiainen, R.; Hirvonen, J. Delivery and stability of LHRH and Nafarelin in human skin: The effect of constant/pulsed iontophoresis. Eur. J. Pharm. Sci. 2004, 21, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, Y.B.; Naik, A.; Guy, R.H.; Vuaridel, E.; Kalia, Y.N. Transdermal iontophoretic delivery of vapreotide acetate across porcine skin in vitro. Pharm. Res. 2005, 22, 1305–1312. [Google Scholar] [CrossRef] [PubMed]
- Lau, D.T.; Sharkey, J.W.; Petryk, L.; Mancuso, F.A.; Yu, Z.; Tse, F.L. Effect of current magnitude and drug concentration on iontophoretic delivery of octreotide acetate (Sandostatin) in the rabbit. Pharm. Res. 1994, 11, 1742–1746. [Google Scholar] [CrossRef] [PubMed]
- Sen, A.; Daly, M.E.; Hui, S.W. Transdermal insulin delivery using lipid enhanced electroporation. Biochim. Biophys. Acta 2002, 1564, 5–8. [Google Scholar] [CrossRef] [Green Version]
- Rs, A.; Ml, A.; Ks, A.; Cb, B.; Vl, C.; Whb, D.; Ynk, A. Targeted cutaneous delivery of etanercept using Er:YAG fractional laser ablation—ScienceDirect. Int. J. Pharm. 2020, 580, 119234. [Google Scholar]
- Sen, A.; Zhao, Y.L.; Hui, S.W. Saturated anionic phospholipids enhance transdermal transport by electroporation. Biophys. J. 2002, 83, 2064–2073. [Google Scholar] [CrossRef] [Green Version]
- Sen, A.; Zhao, Y.; Zhang, L.; Hui, S.W. Enhanced transdermal transport by electroporation using anionic lipids. J. Control. Release 2002, 82, 399–405. [Google Scholar] [CrossRef]
- Cormier, M.; Johnson, B.; Ameri, M.; Nyam, K.; Libiran, L.; Zhang, D.D.; Daddona, P. Transdermal delivery of desmopressin using a coated microneedle array patch system. J. Control. Release 2004, 97, 503–511. [Google Scholar] [CrossRef]
- Ito, Y.; Yoshimitsu, J.; Shiroyama, K.; Sugioka, N.; Takada, K. Self-dissolving microneedles for the percutaneous absorption of EPO in mice. J. Drug Target. 2006, 14, 255–261. [Google Scholar] [CrossRef]
- Mohammed, Y.H.; Yamada, M.; Lin, L.L.; Grice, J.E.; Roberts, M.S.; Raphael, A.P.; Benson, H.A.; Prow, T.W. Microneedle enhanced delivery of cosmeceutically relevant peptides in human skin. PLoS ONE 2014, 9, e101956. [Google Scholar] [CrossRef]
- Karande, P.; Jain, A.; Mitragotri, S. Discovery of transdermal penetration enhancers by high-throughput screening. Nat. Biotechnol. 2004, 22, 192–197. [Google Scholar] [CrossRef]
- Karande, P.; Jain, A.; Mitragotri, S. Insights into synergistic interactions in binary mixtures of chemical permeation enhancers for transdermal drug delivery. J. Control. Release 2006, 115, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Benigni, M.; Pescina, S.; Grimaudo, M.A.; Padula, C.; Santi, P.; Nicoli, S. Development of microemulsions of suitable viscosity for cyclosporine skin delivery. Int. J. Pharm. 2018, 545, 197–205. [Google Scholar] [CrossRef]
- Karande, P.; Mitragotri, S. High throughput screening of transdermal formulations. Pharm. Res. 2002, 19, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Foldvari, M.; Baca-Estrada, M.E.; He, Z.; Hu, J.; Attah-Poku, S.; King, M. Dermal and transdermal delivery of protein pharmaceuticals: Lipid-based delivery systems for interferon alpha. Biotechnol. Appl. Biochem. 1999, 30, 129–137. [Google Scholar]
- Silva, M.I.; Barbosa, A.I.; Costa Lima, S.A.; Costa, P.; Torres, T.; Reis, S. Freeze-Dried Softisan® 649-Based Lipid Nanoparticles for Enhanced Skin Delivery of Cyclosporine A. Nanomaterials 2020, 10, 986. [Google Scholar] [CrossRef]
- Zhang, S.; Ou, H.; Liu, C.; Zhang, Y.; Mitragotri, S.; Wang, D.; Chen, M. Skin Delivery of Hydrophilic Biomacromolecules Using Marine Sponge Spicules. Mol. Pharm. 2017, 14, 3188–3200. [Google Scholar] [CrossRef]
- Zhang, C.; Zhang, K.; Zhang, J.L.; Ou, H.; Duan, J.; Zhang, S.; Wang, D.; Mitragotri, S.; Chen, M. Skin delivery of hyaluronic acid by the combined use of sponge spicules and flexible liposomes. Biomater. Sci. 2019, 7, 1299–1310. [Google Scholar] [CrossRef]
- Liang, X.J.; Zhang, J.L.; Ou, H.L.; Chen, J.; Mitragotri, S.; Chen, M. Skin Delivery of siRNA Using Sponge Spicules in Combination with Cationic Flexible Liposomes. Mol. Ther. Nucleic Acids 2020, 20, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Bendas, E.R.; Tadros, M.I. Enhanced transdermal delivery of salbutamol sulfate via ethosomes. Aaps Pharmscitech 2007, 8, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Ita, K.B.; Du, P.J.; Lane, M.E.; Hadgraft, J.; Du, P.J. Dermal delivery of selected hydrophilic drugs from elastic liposomes: Effect of phospholipid formulation and surfactants. J. Pharm. Pharmacol. 2010, 59, 1215–1222. [Google Scholar] [CrossRef]
- Liu, H.; Li, S.; Wang, Y.; Yao, H.; Yan, Z. Effect of vehicles and enhancers on the topical delivery of cyclosporin A. Int. J. Pharm. 2006, 311, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Mahato, R.I.; Narang, A.S.; Thoma, L.; Miller, D.D. Emerging trends in oral delivery of peptide and protein drugs. Crit. Rev. Ther. Drug Carr. Syst. 2003, 20, 153. [Google Scholar] [CrossRef]
- Singh, N.; Kalluri, H.; Herwadkar, A.; Badkar, A.; Banga, A.K. Transcending the skin barrier to deliver peptides and proteins using active technologies. Crit. Rev. Ther. Drug Carr. Syst. 2012, 29, 265–298. [Google Scholar] [CrossRef]
- Mayer, J.P.; Zhang, F.; Dimarchi, R.D. Insulin structure and function. Pept. Sci. 2007, 88, 687–713. [Google Scholar] [CrossRef]
- Brange, J.; Owens, D.R.; Kang, S.; Volund, A. Monomeric Insulins and Their Experimental and Clinical Implications. Diabetes Care 1990, 13, 923–954. [Google Scholar] [CrossRef] [PubMed]
- Lallemand, F.; Felt-Baeyens, O.; Besseghir, K.; Behar-Cohen, F.; Gurny, R. Cyclosporine A delivery to the eye: A pharmaceutical challenge. Eur. J. Pharm. Biopharm. 2003, 56, 307–318. [Google Scholar] [CrossRef]
- Liddicoat, A.M.; Lavelle, E.C. Modulation of innate immunity by Cyclosporine A. Biochem. Pharmacol. 2019, 163, 472–480. [Google Scholar] [CrossRef]
- Chen, M.; Kumar, S.; Anselmo, A.C.; Gupta, V.; Slee, D.H.; Muraski, J.A.; Mitragotri, S. Topical delivery of Cyclosporine A into the skin using SPACE-peptide. J. Control. Release 2015, 199, 190–197. [Google Scholar] [CrossRef]
- Lopes, L.B.; Collett, J.H.; Bentley, M. Topical delivery of cyclosporin A: An in vitro study using monoolein as a penetration enhancer. Eur. J. Pharm. Biopharm. 2005, 60, 25–30. [Google Scholar] [CrossRef]
- Duncan, J.I.; Payne, S.; Winfield, A.J.; Ormerod, A.D.; Thomson, A.W. Enhanced percutaneous absorption of a novel topical cyclosporin A formulation and assessment of its immunosuppressive activity. Br. J. Dermatol. 2010, 123, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Flynn, G.L.; Amidon, G.L. Percutaneous absorption and dermal delivery of cyclosporin A. J. Pharm. Sci. 2010, 84, 581–583. [Google Scholar] [CrossRef] [PubMed]
- Rothbard, J.B.; Garlington, S.; Lin, Q.; Kirschberg, T.; Kreider, E.; McGrane, P.L.; Wender, P.A.; Khavari, P.A. Conjugation of arginine oligomers to cyclosporin A facilitates topical delivery and inhibition of inflammation. Nat. Med. 2000, 6, 1253–1257. [Google Scholar] [CrossRef] [PubMed]
- Der Fits, L.V.; Mourits, S.; Voerman, J.S.A.; Kant, M.; Boon, L.; Laman, J.D.; Cornelissen, F.; Mus, A.; Florencia, E.; Prens, E.P. Imiquimod-Induced Psoriasis-Like Skin Inflammation in Mice Is Mediated via the IL-23/IL-17 Axis. J. Immunol. 2009, 182, 5836–5845. [Google Scholar] [CrossRef] [PubMed]
- Terhorst, D.; Chelbi, R.; Wohn, C.; Malosse, C.; Tamoutounour, S.; Jorquera, A.; Bajenoff, M.; Dalod, M.; Malissen, B.; Henri, S. Dynamics and Transcriptomics of Skin Dendritic Cells and Macrophages in an Imiquimod-Induced, Biphasic Mouse Model of Psoriasis. J. Immunol. 2015, 195, 4953–4961. [Google Scholar] [CrossRef] [PubMed] [Green Version]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, C.; Duan, J.; Huang, Y.; Chen, M. Enhanced Skin Delivery of Therapeutic Peptides Using Spicule-Based Topical Delivery Systems. Pharmaceutics 2021, 13, 2119. https://doi.org/10.3390/pharmaceutics13122119
Zhang C, Duan J, Huang Y, Chen M. Enhanced Skin Delivery of Therapeutic Peptides Using Spicule-Based Topical Delivery Systems. Pharmaceutics. 2021; 13(12):2119. https://doi.org/10.3390/pharmaceutics13122119
Chicago/Turabian StyleZhang, Chi, Jiwen Duan, Yongxiang Huang, and Ming Chen. 2021. "Enhanced Skin Delivery of Therapeutic Peptides Using Spicule-Based Topical Delivery Systems" Pharmaceutics 13, no. 12: 2119. https://doi.org/10.3390/pharmaceutics13122119