
Targeting of Inhaled Therapeutics to the Small Airways: Nanoleucine Carrier Formulations


Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.1.1. Manufacture of Ciclesonide Powder for Inhalation (CPI)
2.1.2. Capsule Filling of CPI
2.2. Methods
2.2.1. Primary Particle Size Distribution
2.2.2. Tapped Density
2.2.3. X-ray Powder Diffraction (XRPD)
2.2.4. Dynamic Vapor Sorption (DVS)
2.2.5. Ciclesonide Determination by RP-HPLC with UV Detection
2.2.6. Assay and Blend Uniformity
2.2.7. Emitted Dose
2.2.8. Aerodynamic Particle Size Distribution (APSD)
2.2.9. Mass Median Impaction Parameter (MMIP) and Stage Groupings
2.2.10. Total Lung Dose
3. Results
3.1. Nanoleucine Carrier Particles
3.2. Physicochemical Properties of Ciclesonide Powder for Inhalation
3.3. CPI Particle Size Distribution
3.4. Drug Content and Blend Uniformity
3.5. Crystallinity
3.6. Aerosol Performance of Ciclesonide Powder for Inhalation
3.7. Total Lung Dose of CPI in Idealized Anatomical Throat Models
4. Discussion
4.1. Comparison of CPI to Marketed ICS Formulations
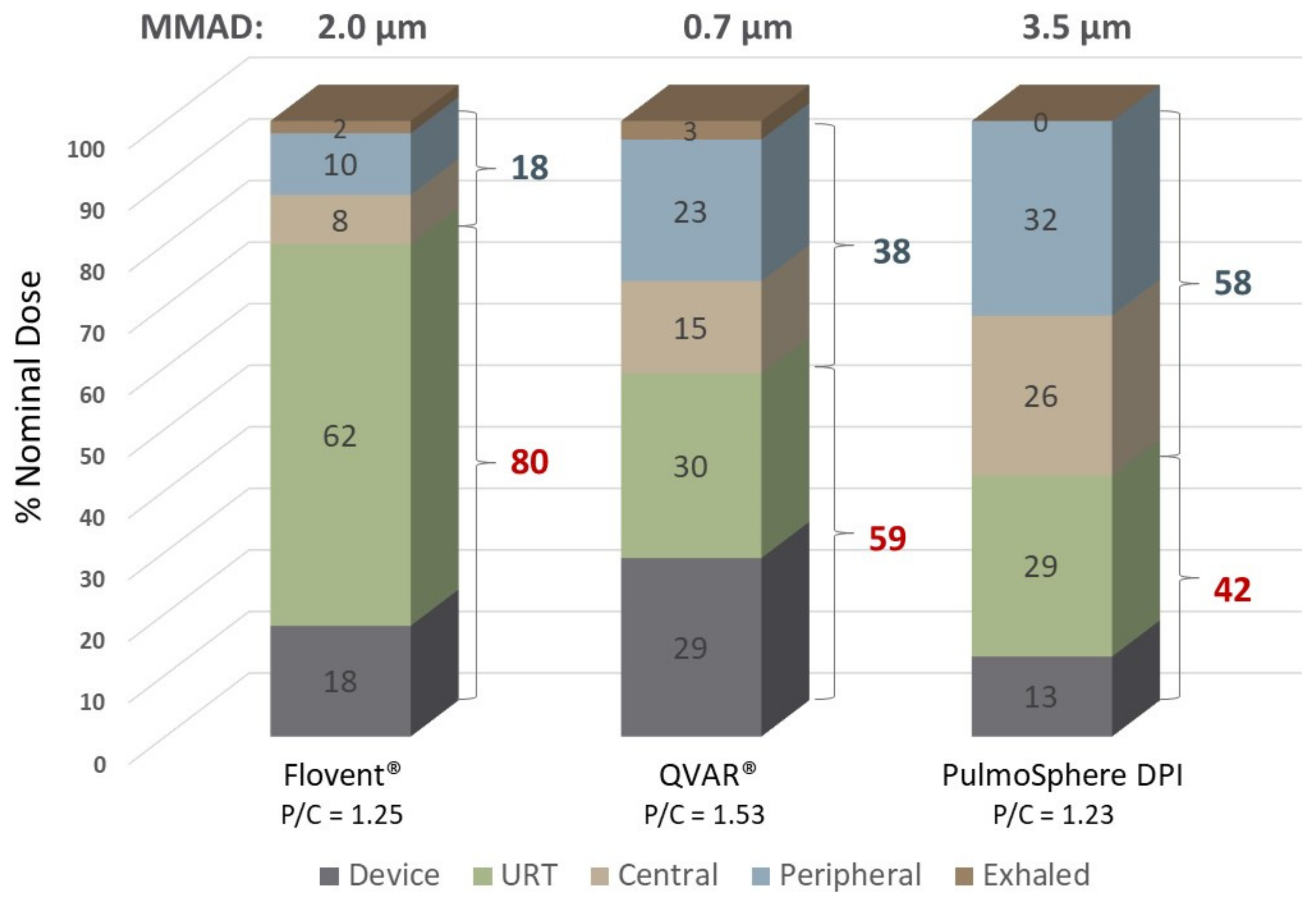
4.2. Regional Deposition in the Respiratory Tract
4.3. Small Airways Delivery
4.4. Minimum Flow Rate
5. Conclusions
- Adhesive mixtures comprising extrafine ciclesonide crystals and crystalline nanoleucine carrier particles achieve TLD values that are 93% and 87% of the ED in adult and child anatomical throat models, respectively.
- The TLD measured in the throat models was independent of flow rate and relative humidity.
- In an NGI, deposition of CPI in the “large particle fraction” comprising the induction port, stage 1 and stage 2 was just 2.3% of the emitted dose. In the “airways fraction” comprising stages 3 through stage 5, deposition was 78.1%. In the “very fine fraction” comprising stages 6 to MOC, deposition was 19.6%.
- Lung targeting, expressed as the ratio of the TLD/URT deposition was significantly greater than current marketed ICS therapeutics.
- The nanoleucine carrier technology represents an alternative to traditional lactose blends and solution pMDIs, with improved ability to target drug to the large and small airways in the lungs, while minimizing extrathoracic and alveolar delivery.
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AOS® DPI | Axial oscillating sphere dry powder inhaler |
| APSD | Aerodynamic particle size distribution |
| CIC | Ciclesonide |
| COPD | Chronic obstructive pulmonary disease |
| CPI | Ciclesonide powder for inhalation |
| CT | Computed tomography |
| Diameter of the airspace | |
| Da | Median aerodynamic diameter for primary particles |
| Aerodynamic diameter | |
| Impaction parameter | |
| Geometric diameter | |
| Particle diameter | |
| dm/dt | Change in mass per unit time |
| DSPC | Distearoylphosphatidylcholine |
| DUSA | Dose unit sampling apparatus |
| DVS | Dynamic vapor sorption |
| ED | Emitted dose |
| FPF<5 μm | Fine particle fraction less than 5 μm |
| Acceleration due to gravity | |
| ICS | Inhaled corticosteroid |
| ICT | Idealized child throat |
| IP | Induction port |
| LEU | Leucine |
| LB | Lactose blend |
| LRT | Lower respiratory tract |
| MIP | Maximum inspiratory pressure |
| MMAD | Mass median aerodynamic diameter |
| MMIP | Mass median impaction parameter |
| MOC | Micro orifice collector |
| ND | Nominal dose |
| NP | Nanoparticles |
| PFOB | Perfluorooctyl bromide, Perflubron USP |
| RH | Relative humidity |
| RP-HPLC | Reverse phase-High performance liquid chromatography |
| SPH | Spheronized particles |
| Stk | Stokes Number |
| TLD | Total lung dose |
| URT | Upper respiratory tract |
| USP | United States Pharmacopeia |
| UV | Ultraviolet |
| X10 | Diameter for which 10% of the particles have a smaller size |
| X50 | Diameter for which 50% of the particles have a smaller size |
| X90 | Diameter for which 90% of the particles have a smaller size |
| XRPD | X-ray powder diffraction |
| Particle density | |
| Tapped density | |
| Dynamic viscosity | |
| Linear velocity | |
| Terminal settling velocity |
References
- Darquenne, C. Deposition mechanisms. J. Aerosol Med. Pulm. Drug Deliv. 2020, 33, 181–185. [Google Scholar] [CrossRef]
- Newman, S.; Hirst, P.; Pitcairn, G.; Clark, A. Understanding regional lung deposition data in gamma scintigraphy. Respir. Drug Deliv. VI. 1998, 1, 9–15. [Google Scholar]
- Carr, T.F.; Altisheh, R.; Zitt, M. Small airways disease and severe asthma. World Allergy Organ. J. 2017, 10, 20. [Google Scholar] [CrossRef] [Green Version]
- Usmani, O.S. Treating the small airways. Respiration 2012, 84, 441–453. [Google Scholar] [CrossRef]
- Keen, C.; Olin, A.-C.; Wennergren, G.; Gustafsson, P. Small airway function, exhaled NO and airway hyper-responsiveness in paediatric asthma. Respir. Med. 2011, 105, 1476–1484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamid, Q.; Song, Y.; Kotsimbos, T.C.; Minshall, E.; Bai, T.R.; Hegele, R.; Hogg, J.C. Inflammation of small airways in asthma. J. Allergy Clin. Immunol. 1997, 100, 44–51. [Google Scholar] [CrossRef]
- Lavorini, F.; Pedersen, S.; Usmani, O.S.; Aerosol Drug Management Improvement Team (ADMIT). Dilemmas, confusion, and misconceptions related to small airways directed therapy. Chest 2017, 151, 1345–1355. [Google Scholar] [CrossRef] [PubMed]
- Weers, J.G.; Son, Y.-J.; Glusker, M.; Haynes, A.; Huang, D.; Kadrichu, N.; Le, J.; Li, X.; Malcolmson, R.; Miller, D.P.; et al. Idealhalers versus realhalers: Is it possible to bypass deposition in the upper respiratory tract? J. Aerosol Med. Pulm. Drug Deliv. 2019, 32, 55–69. [Google Scholar] [CrossRef]
- Stahlhofen, W.; Rudolf, G.; James, A. Intercomparison of experimental regional aerosol deposition data. J. Aerosol Med. 1989, 2, 285–308. [Google Scholar] [CrossRef]
- Borgström, L.; Olsson, B.; Thorsson, L. Degree of throat deposition can explain the variability in lung deposition of inhaled drugs. J. Aerosol Med. 2006, 19, 473–483. [Google Scholar] [CrossRef]
- Stapleton, K.W.; Guentsch, E.; Hoskinson, M.K.; Finlay, W.H. On the suitability of the κ−ε turbulence model for aerosol depo-sition in the mouth and throat: A comparison with experiments. J. Aerosol Sci. 2000, 31, 739–749. [Google Scholar] [CrossRef]
- Grgic, B.; Finlay, W.; Heenan, A. Regional aerosol deposition and flow measurements in an idealized mouth and throat. J. Aerosol Sci. 2004, 35, 21–32. [Google Scholar] [CrossRef]
- Golshahi, L.; Noga, M.; Finlay, W. Deposition of inhaled micrometer-sized particles in oropharyngeal airway replicas of children at constant flow rates. J. Aerosol Sci. 2012, 49, 21–31. [Google Scholar] [CrossRef]
- Golshahi, L.; Finlay, W.H. An idealized child throat that mimics average pediatric oropharyngeal deposition. Aerosol Sci. Technol. 2012, 46, i–iv. [Google Scholar] [CrossRef]
- Olsson, B.; Borgström, L.; Lundbäck, H.; Svensson, M. Validation of a general in vitro approach for prediction of total lung deposition in healthy adults for pharmaceutical inhalation products. J. Aerosol Med. Pulm. Drug Deliv. 2013, 26, 355–369. [Google Scholar] [CrossRef] [PubMed]
- Delvadia, R.R.; Longest, P.W.; Byron, P.R. In vitro tests for aerosol deposition. I: Scaling a physical model of the upper airways to predict drug deposition variation in normal humans. J. Aerosol Med. Pulm. Drug Deliv. 2012, 25, 32–40. [Google Scholar] [CrossRef]
- Wei, X.; Hindle, M.; Kaviratna, A.; Huynh, B.K.; Delvadia, R.R.; Sandell, D.; Byron, P.R. In vitro tests for aerosol deposition. VI: Realistic testing with different mouth–throat models and in vitro–in vivo correlations for a dry powder inhaler, metered dose inhaler, and soft mist inhaler. J. Aerosol Med. Pulm. Drug Deliv. 2018, 31, 358–371. [Google Scholar] [CrossRef] [PubMed]
- Tavernini, S.; Church, T.K.; Lewis, D.A.; Noga, M.; Martin, A.R.; Finlay, W.H. Deposition of micrometer-sized aerosol particles in neonatal nasal airway replicas. Aerosol Sci. Technol. 2018, 52, 407–419. [Google Scholar] [CrossRef] [Green Version]
- Delvadia, R.; Hindle, M.; Longest, P.W.; Byron, P.R. In vitro tests for aerosol deposition II: IVIVCs for different dry powder inhalers in normal adults. J. Aerosol Med. Pulm. Drug Deliv. 2013, 26, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Delvadia, R.R.; Longest, P.W.; Hindle, M.; Byron, P.R. In vitro tests for aerosol deposition. III: Effect of inhaler insertion angle on aerosol deposition. J. Aerosol Med. Pulm. Drug Deliv. 2013, 26, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Ruzycki, C.A.; Golshahi, L.; Vehring, R.; Finlay, W.H. Comparison of in vitro deposition of pharmaceutical aerosols in an idealized child throat with in vivo deposition in the upper respiratory tract of children. Pharm. Res. 2014, 31, 1525–1535. [Google Scholar] [CrossRef]
- Weers, J.G.; Clark, A.R.; Rao, N.; Ung, K.; Haynes, A.; Khindri, S.K.; Perry, S.A.; Machineni, S.; Colthorpe, P. In vitro–in vivo correlations observed with indacaterol-based formulations delivered with the Breezhaler®. J. Aerosol Med. Pulm. Drug Deliv. 2015, 28, 268–280. [Google Scholar] [CrossRef]
- Haynes, A.; Geller, D.; Weers, J.; Ament, B.; Pavkov, R.; Malcolmson, R.; Debonnett, L.; Mastoridis, P.; Yadao, A.; Heuerding, S. Inhalation of tobramycin using simulated cystic fibrosis patient profiles. Pediatr. Pulmonol. 2016, 51, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Gilbertson, K.; Finlay, W.H. In vivo–in vitro comparison of deposition in three mouth–throat models with Qvar® and Turbuhaler® inhalers. J. Aerosol Med. 2007, 20, 227–235. [Google Scholar] [CrossRef] [Green Version]
- Kaviratna, A.; Tian, G.; Liu, X.; Delvadia, R.; Lee, S.; Guo, C. Evaluation of bio-relevant mouth-throat models for characterization of metered dose inhalers. AAPS PharmSciTech 2019, 20, 130. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Sun, J.; Cheng, Y.-S. Comparison of deposition in the USP and physical mouth–throat models with solid and liquid particles. J. Aerosol Med. Pulm. Drug Deliv. 2011, 24, 277–284. [Google Scholar] [CrossRef]
- Newman, S.P.; Chan, H.-K. In vitro-in vivo correlations (IVIVCs) of deposition for drugs given by oral inhalation. Adv. Drug Deliv. Rev. 2020, 167, 135–147. [Google Scholar] [CrossRef]
- Usmani, O.S.; Biddiscombe, M.F.; Barnes, P.J. Regional lung deposition and bronchodilator response as a function of β2-agonist particle size. Am. J. Respir. Crit. Care Med. 2005, 172, 1497–1504. [Google Scholar] [CrossRef]
- Hoppentocht, M.; Hagedoorn, P.; Frijlink, H.W.; de Boer, A. Technological and practical challenges of dry powder inhalers and formulations. Adv. Drug Deliv. Rev. 2014, 75, 18–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ung, K.T.; Rao, N.; Weers, J.G.; Huang, D.; Chan, H.-K. Design of spray dried insulin microparticles to bypass deposition in the extrathoracic region and maximize total lung dose. Int. J. Pharm. 2016, 511, 1070–1079. [Google Scholar] [CrossRef]
- Chew, N.Y.K.; Chan, H.-K. Use of solid corrugated particles to enhance powder aerosol performance. Pharm. Res. 2001, 18, 1570–1577. [Google Scholar] [CrossRef]
- Vehring, R. Pharmaceutical particle engineering via spray drying. Pharm. Res. 2008, 25, 999–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weers, J.G.; Miller, D.P. Formulation design of dry powders for inhalation. J. Pharm. Sci. 2015, 104, 3259–3288. [Google Scholar] [CrossRef]
- Trevino, L.A.; Dellamary, L.A.; Tarara, T.E.; Weers, J.G.; Ranney, H.M. Continuous Fluorochemical Microdispersions for the Delivery of Lipophilic Pharmaceutical Agents. U.S. Patent 5,667,809, 16 September 1997. [Google Scholar]
- Ostwald, W.Z. Blocking of Ostwald ripening allowing long-term stabilization. Phys. Chem. 1901, 37, 385. [Google Scholar]
- Lifshitz, I.M.; Slezov, V. The kinetics of precipitation from supersaturated solid solution. J. Phys. Chem. Solids 1961, 19, 35. [Google Scholar] [CrossRef]
- Hartman, M.; Tarara, T.E.; Teung, P.; Weers, J.G. Respirable Agglomerates of Porous Particles. U.S. Patent 9,744,178, 29 August 2017. [Google Scholar]
- Weers, J.G.; Tarara, T.; Teung, P.; Walsh, K.; Rao, N.; Le, J.; Haynes, A.; Huang, D.; Miller, D.P. Solving the particle adhesion paradox: Respirable agglomerates of micronized drugs and porous (microcarrier) particles. Proc. Respir. Drug Deliv. Eur. 2015, 1, 177–185. [Google Scholar]
- Vehring, R.; Lechuga-Ballesteros, D.; Joshi, V.; Noga, B.; Dwivedi, S.K. Cosuspensions of microcrystals and engineered microparticles for uniform and efficient delivery of respiratory therapeutics from pressurized metered dose inhalers. Langmuir 2012, 28, 15015–15023. [Google Scholar] [CrossRef] [PubMed]
- Weers, J.; Lyons, S.; Tarara, T.; Miller, D.P.; Molloy, L.; Weers, A.; Saavedra, K.; Heller, D.; Curtis, R. The AOS™ DPI: A cap-sule-based dry powder inhaler with four distinct dispersion elements. Proc. Respir. Drug Deliv. 2020, 2020, 459–462. [Google Scholar]
- Weers, J.; Rao, N.; Kadrichu, N. Is aerodynamic diameter a good metric for understanding regional deposition? Proc. Respir. Drug Deliv. Eur. 2019, 2019, 59–66. [Google Scholar]
- Weers, J. Regional deposition of particles within the respiratory tract should be linked to impaction parameter, not aerodynamic size. J. Aerosol Med. Pulm. Drug Deliv. 2018, 31, 116–118. [Google Scholar] [CrossRef]
- Dolovich, M.B.; Mitchell, J.D.; Roberts, D.L. Re: “Harmonizing the nomenclature for therapeutic aerosol particle size: A pro-posal” by Hillyer et al. (J. Aerosol Med. Pulm. Drug Deliv. 2018 [31 (2): 111–113]; DOI: 10.1089/jamp.2017.1396). J. Aerosol Med. Pulm. Drug Deliv. 2018, 31, 266–268. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.R.; Moore, C.P.; Finlay, W.H. Models of deposition, pharmacokinetics, and intersubject variability in respiratory drug delivery. Expert Opin. Drug Deliv. 2018, 15, 1175–1188. [Google Scholar] [CrossRef] [PubMed]
- Dunber, C.A.; Hickey, A.J.; Holzner, P. Dispersion and characterization of pharmaceutical dry powder aerosols. KONA Powder Part. J. 1998, 16, 7–45. [Google Scholar] [CrossRef] [Green Version]
- Leung, S.; Tang, P.; Zhou, Q.T.; Tong, Z.; Leung, C.; Decharaksa, J.; Yang, R.; Chan, H.-K. De-agglomeration effect of the US pharmacopeia and alberta throats on carrier-based powders in commercial inhalation products. AAPS J. 2015, 17, 1407–1416. [Google Scholar] [CrossRef]
- Feth, M.P.; Volz, J.; Hess, U.; Sturm, E.; Hummel, R.-P. Physicochemical, crystallographic, thermal, and spectroscopic behavior of crystalline and X-ray amorphous ciclesonide. J. Pharm. Sci. 2008, 97, 3765–3780. [Google Scholar] [CrossRef] [PubMed]
- Ordoubadi, M.; Gregson, F.K.; Wang, H.; Nicholas, M.; Gracin, S.; Lechuga-Ballesteros, D.; Reid, J.P.; Finlay, W.H.; Vehring, R. On the particle formation of leucine in spray drying of inhalable microparticles. Int. J. Pharm. 2021, 592, 120102. [Google Scholar] [CrossRef] [PubMed]
- Weers, J.; Tarara, T. The PulmoSphere™ platform for pulmonary drug delivery. Ther. Deliv. 2014, 5, 277–295. [Google Scholar] [CrossRef] [PubMed]
- Weers, J.G.; Miller, D.P.; Tarara, T.E. Spray-dried PulmoSphere™ formulations for inhalation comprising crystalline drug particles. AAPS PharmSciTech 2019, 20, 103. [Google Scholar] [CrossRef] [PubMed]
- Clark, A. The role of inspiratory pressures in determining the flow rates though dry powder inhalers: A review. Curr. Pharm. Des. 2015, 21, 3974–3983. [Google Scholar] [CrossRef]
- Pedersen, S. How to use a rotahaler. Arch. Dis. Child. 1986, 61, 11–14. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, S.; Hansen, O.R.; Fugelsang., G. Influence of inspiratory flow rate upon the effect of a Turbuhaler. Arch. Dis. Child. 1990, 65, 308–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bentur, L.; Mansour, Y.; Hamzani, Y.; Beck, R.; Elias, N.; Amirav, I. Measurement of inspiratory flow in children with acute asthma. Pediatr. Pulmonol. 2004, 38, 304–307. [Google Scholar] [CrossRef]
- Clark, A.R.; Weers, J.G.; Dhand, R. The confusing world of dry powder inhalers: It is all about inspiratory pressures, not inspiratory flow rates. J. Aerosol Med. Pulm. Drug Deliv. 2020, 33, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Koning, J.; van der Mark, T.; Coenegracht, P.; Tromp, T.; Frijlink, H. Effect of an external resistance to airflow on the inspiratory flow curve. Int. J. Pharm. 2002, 234, 257–266. [Google Scholar] [CrossRef]
- Tiddens, H.; Geller, D.; Challoner, P.; Speirs, R.; Kesser, K.; Overbeek, S.; Humble, D.; Shrewsbury, S.; Standaert, T. Effect of dry powder inhaler resistance on the inspiratory flow rates and volumes of cystic fibrosis patients of six years and older. J. Aerosol Med. 2006, 19, 456–465. [Google Scholar] [CrossRef]
- Azouz, W.; Chetcuti, P.; Hosker, H.S.; Saralaya, D.; Stephenson, J.; Chrystyn, H. The inhalation characteristics of patients when they use different dry powder inhalers. J. Aerosol Med. Pulm. Drug Deliv. 2015, 28, 35–42. [Google Scholar] [CrossRef] [Green Version]
- Sahay, S.; Holy, R.; Lyons, S.; Parsley, E.; Maurer, M.; Weers, J. Impact of human behavior on inspiratory flow profiles in patients with pulmonary arterial hypertension using AOS™ dry powder inhaler device. Pulm. Circ. 2021, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Weers, J.G.; Clark, A.R. The impact of inspiratory flow rate on drug delivery to the lungs with dry powder inhalers. Pharm. Res. 2017, 34, 507–528. [Google Scholar] [CrossRef]
- Boraey, M.; Hoe, S.; Sharif, H.; Miller, D.P.; Lechuga-Ballesteros, D.; Vehring, R. Improvement of the dispersibility of spray-dried budesonide powders using leucine in an ethanol–water cosolvent system. Powder Technol. 2013, 236, 171–178. [Google Scholar] [CrossRef]
- Lechuga-Ballesteros, D.; Charan, C.; Stults, C.L.; Stevenson, C.L.; Miller, D.P.; Vehring, R.; Tep, V.; Kuo, M. Trileucine improves aerosol performance and stability of spray-dried powders for inhalation. J. Pharm. Sci. 2008, 97, 287–302. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, H.; Vehring, R. Leucine enhances the dispersibility of trehalose-containing spray-dried powders on exposure to a high-humidity environment. Int. J. Pharm. 2021, 601, 120561. [Google Scholar] [CrossRef]
- Cui, Y.; Zhang, X.; Wang, W.; Huang, Z.; Zhao, Z.; Wang, G.; Cai, S.; Jing, H.; Huang, Y.; Pan, X.; et al. Moisture-resistant co-spray-dried netilmicin with l-leucine as dry powder inhalation for the treatment of respiratory infections. Pharmaceutics 2018, 10, 252. [Google Scholar] [CrossRef] [Green Version]
- Feng, A.; Boraey, M.; Gwin, M.; Finlay, P.; Kuehl, P.; Vehring, R. Mechanistic models facilitate efficient development of leucine containing microparticles for pulmonary drug delivery. Int. J. Pharm. 2011, 409, 156–163. [Google Scholar] [CrossRef]
- Li, L.; Leung, S.; Gengenbach, T.; Yu, J.; Gao, G.F.; Tang, P.; Zhou, Q.T.; Chan, H.-K. Investigation of L-leucine in reducing the moisture-induced deterioration of spray-dried salbutamol sulfate power for inhalation. Int. J. Pharm. 2017, 530, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Sun, S.; Parumasivan, T.; Denman, J.A.; Gengenbach, T.; Tang, P.; Mao, S.; Chan, H.-K. L-leucine as an excipient against moisture on in vitro aerosolization performances of highly hygroscopic spray-dried powders. Eur. J. Pharm. Biopharm. 2016, 102, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Shetty, N.; Park, H.; Zemlyanov, D.; Mangal, S.; Bhujbal, S.; Zhou, Q.T. Influence of excipients on physical and aerosolization stability of spray dried high-dose powder formulations for inhalation. Int. J. Pharm. 2018, 544, 222–234. [Google Scholar] [CrossRef]
- Sibum, I.; Hagedoorn, P.; Kluitman, M.P.G.; Kloezen, M.; Frijlink, H.W.; Grasmeijer, F. Dispersibility and storage stability optimization of high dose isoniazid dry powder inhalation formulations with L-leucine or trileucine. Pharmaceutics 2019, 12, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, S.; Salmon, A.; Nave, R.; Drollmann, A. High lung deposition of 99mTc-labeled ciclesonide administered via HFA-MDI to patients with asthma. Respir. Med. 2006, 100, 375–384. [Google Scholar] [CrossRef] [Green Version]
- Leach, C.L.; Kuehl, P.J.; Chand, R.; McDonald, J.D. Respiratory tract deposition of HFA–beclomethasone and HFA–fluticasone in asthmatic patients. J. Aerosol Med. Pulm. Drug Deliv. 2016, 29, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Mariotti, F.; Sergio, F.; Acerbi, D.; Meyer, T.; Herpich, C. Lung deposition of the extra fine dry powder fixed combination beclomethasone dipropionate plus formoterol fumarate via the NEXT DPI® in healthy subjects, asthmatic, and COPD patients. Eur. Respir. J. 2011, 38, 830. [Google Scholar]
- Pitcairn, G.; Reader, S.; Pavia, D.; Newman, S. Deposition of corticosteroid aerosol in the human lung by Respimat® Soft Mist™ inhaler compared to deposition by metered dose inhaler or by Turbuhaler® dry powder inhaler. J. Aerosol Med. 2005, 18, 264–272. [Google Scholar] [CrossRef]
- Leach, C.; Davidson, P.; Boudreau, R. Improved airway targeting with the CFC-free HFA–beclomethasone metered-dose inhaler compared with CFC–beclomethasone. Eur. Respir. J. 1998, 12, 1346–1353. [Google Scholar] [CrossRef] [PubMed]
- Duddu, S.P.; Sisk, S.A.; Walter, Y.H.; Tarara, T.E.; Trimble, K.R.; Clark, A.R.; Eldon, M.A.; Elton, R.C.; Pickford, M.; Hirst, P.H.; et al. Improved lung delivery from a passive dry powder inhaler using an engineered PulmoSphere® powder. Pharm. Res. 2002, 19, 689–695. [Google Scholar] [CrossRef]
- Buttini, F.; Brambilla, G.; Copelli, D.; Sisti, V.; Balducci, A.G.; Bettini, R.; Pasquali, I. Effect of flow rate on in vitro aerodynamic performance of NEXThaler® in comparison with Diskus® and Turbohaler® dry powder inhalers. J. Aerosol Med. Pulm. Drug Deliv. 2016, 29, 167–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laube, B.L.; Janssens, H.M.; de Jongh, F.H.C.; Devadason, S.G.; Dhand, R.; Diot, P.; Everard, M.L.; Horvath, I.; Navalesi, P.; Voshaar, T.; et al. What the pulmonary specialist should know about the new inhalation therapies. Eur. Respir. J. 2011, 37, 1308–1417. [Google Scholar] [CrossRef] [Green Version]
- Haidl, P.; Heindl, S.; Siemon, K.; Bernacka, M.; Cloes, R.M. Inhalation device requirements for patients’ inhalation maneuvers. Respir. Med. 2016, 118, 65–75. [Google Scholar] [CrossRef] [Green Version]
- Mahler, D.A. Peak inspiratory flow rate as a criterion for dry powder inhaler use in chronic obstructive pulmonary disease. Ann. Am. Thorac. Soc. 2017, 14, 1103–1107. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metric | Method | Mean ± SD |
|---|---|---|
| Ciclesonide assay (μg/mg) | RP-HPLC | 9.6 ± 0.1 |
| Geometric size (μm) | Laser diffraction | 0.79 ± 0.01 |
| (μm) | Laser diffraction | 1.70 ± 0.02 |
| (μm) | Laser diffraction | 3.16 ± 0.05 |
| Tapped density (g/cm3) | Tapped density | 0.047 ± 0.001 |
| (nm) | Calculated | 370 |
| Water content (% w/w) | DVS | < 0.3 (90% RH) |
| ICS physical form | XRPD | Crystalline |
| Leucine physical form | XRPD | Crystalline |
| Metric | Method | Mean ± SD |
|---|---|---|
| Emitted dose (% ND) a | DUSA / RP-HPLC | 94.0 ± 0.7 |
| Fine particle fraction < 5 μm (% ED) b | NGI / RP-HPLC | 96.8 |
| Fine particle fraction S4-F (% ED) b | NGI / RP-HPLC | 94.5 |
| Mass median aerodynamic diameter (μm) b | NGI / RP-HPLC | 1.66 |
| Geometric standard deviation b | NGI / RP-HPLC | 1.57 |
| Mass median impaction parameter (μm2 Lmin-1) b | NGI / RP-HPLC | 115.8 |
| Total lung dose (% ED) a | Alberta idealized throat AIT / RP-HPLC | 93.0 |
| Total lung dose (% ED) a | Idealized child throat ICT / RP-HPLC | 86.5 |
| Q index (%) a | ICT / RP-HPLC | −3.9 |
| TLD 75% RH / TLD 40% RH b | ICT / RP-HPLC | 0.99 |
| Aerosol Metric | Mean | Asmanex Twisthaler (%ED) | Flovent Diskus (%ED) | Alvesco pMDI (%ED) | QVAR pMDI (%ED) | Foster Nexthaler (%ED) | CPI AOS (%ED) |
|---|---|---|---|---|---|---|---|
| Stage Grouping (T-S2) | > 1176 | 81.7 | 79.6 | 28.6 | 24.0 | 35.0 | 2.3 |
| Stage Grouping (S3-S5) | 56–1176 | 16.6 | 18.3 | 19.2 | 22.5 | 33.3 | 78.1 |
| Stage Grouping (S4-S5) | 56–467 | 10.9 | 9.0 | 19.2 | 21.5 | 26.5 | 74.9 |
| Stage Grouping (S6-F) | < 56 | 2.7 | 1.2 | 52.2 | 53.5 | 31.8 | 19.6 |
| Stage Grouping (S7-F) | < 21 | 1.7 | 0.1 | 26.7 | 29.5 | 18.6 | 4.4 |
| MMAD (μm) | / | 2.6 | 2.8 | 1.0 | 0.6 | 1.2 | 1.7 |
| MMIP (μm2 L min−1) | / | 394.8 | 704.2 | 29.0 | 30.9 | 61.8 | 115.8 |
| Drug APSD | / | Fine | Fine | Extrafine | Extrafine | Extrafine | Extrafine |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miller, D.P.; Tarara, T.E.; Weers, J.G. Targeting of Inhaled Therapeutics to the Small Airways: Nanoleucine Carrier Formulations. Pharmaceutics 2021, 13, 1855. https://doi.org/10.3390/pharmaceutics13111855
Miller DP, Tarara TE, Weers JG. Targeting of Inhaled Therapeutics to the Small Airways: Nanoleucine Carrier Formulations. Pharmaceutics. 2021; 13(11):1855. https://doi.org/10.3390/pharmaceutics13111855
Chicago/Turabian StyleMiller, Danforth P., Thomas E. Tarara, and Jeffry G. Weers. 2021. "Targeting of Inhaled Therapeutics to the Small Airways: Nanoleucine Carrier Formulations" Pharmaceutics 13, no. 11: 1855. https://doi.org/10.3390/pharmaceutics13111855