
Bronchodilator Delivery via High-Flow Nasal Cannula: A Randomized Controlled Trial to Compare the Effects of Gas Flows


Abstract
:1. Introduction
2. Materials and Methods
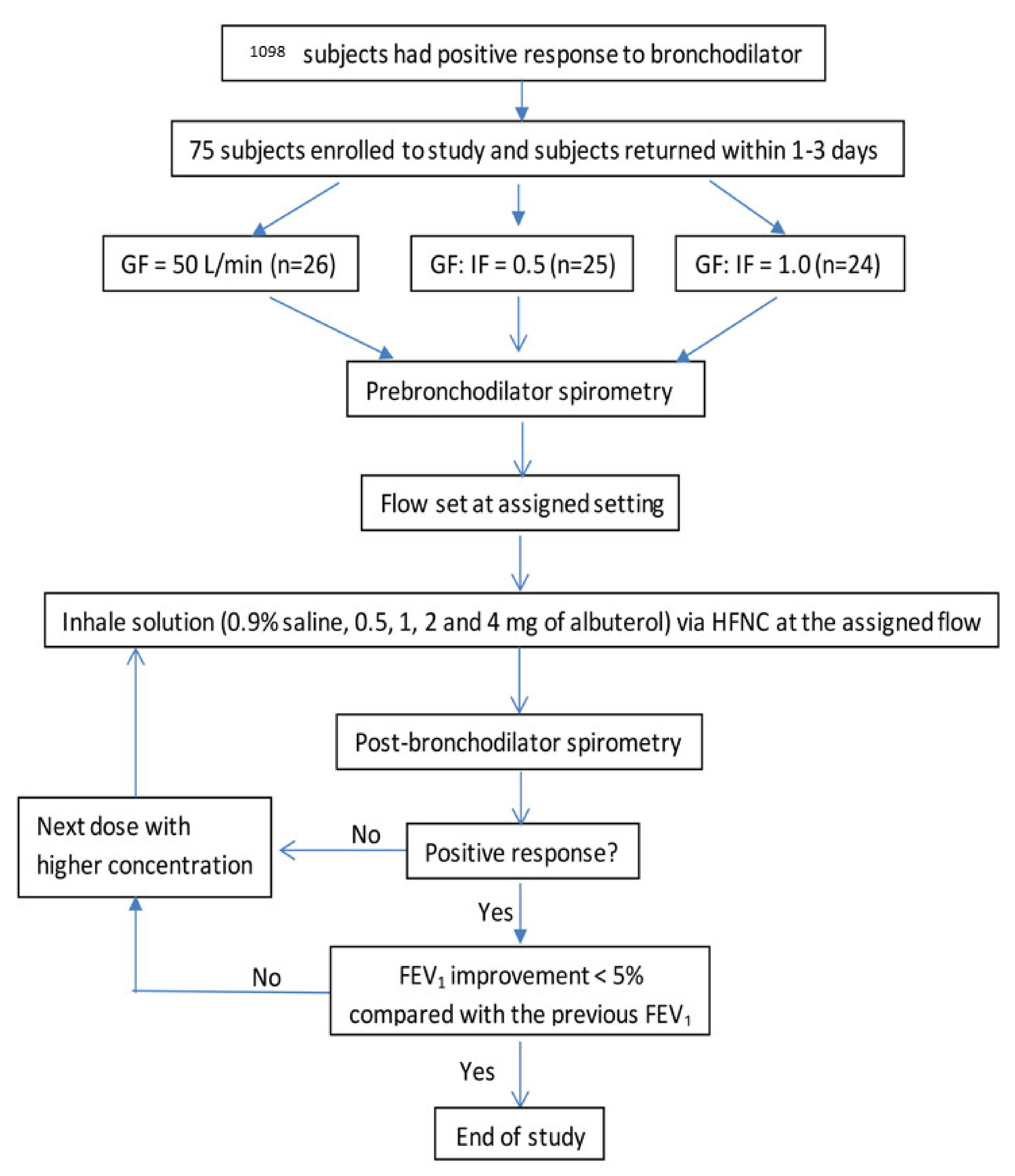
2.1. Study Population
2.2. Study Procedures
2.3. Outcomes
2.4. Sample Size Calculation
2.5. Data Collection
2.6. Statistical Analysis
3. Results
3.1. Bronchodilation Responses after Inhaling Salbutamol via HFNC
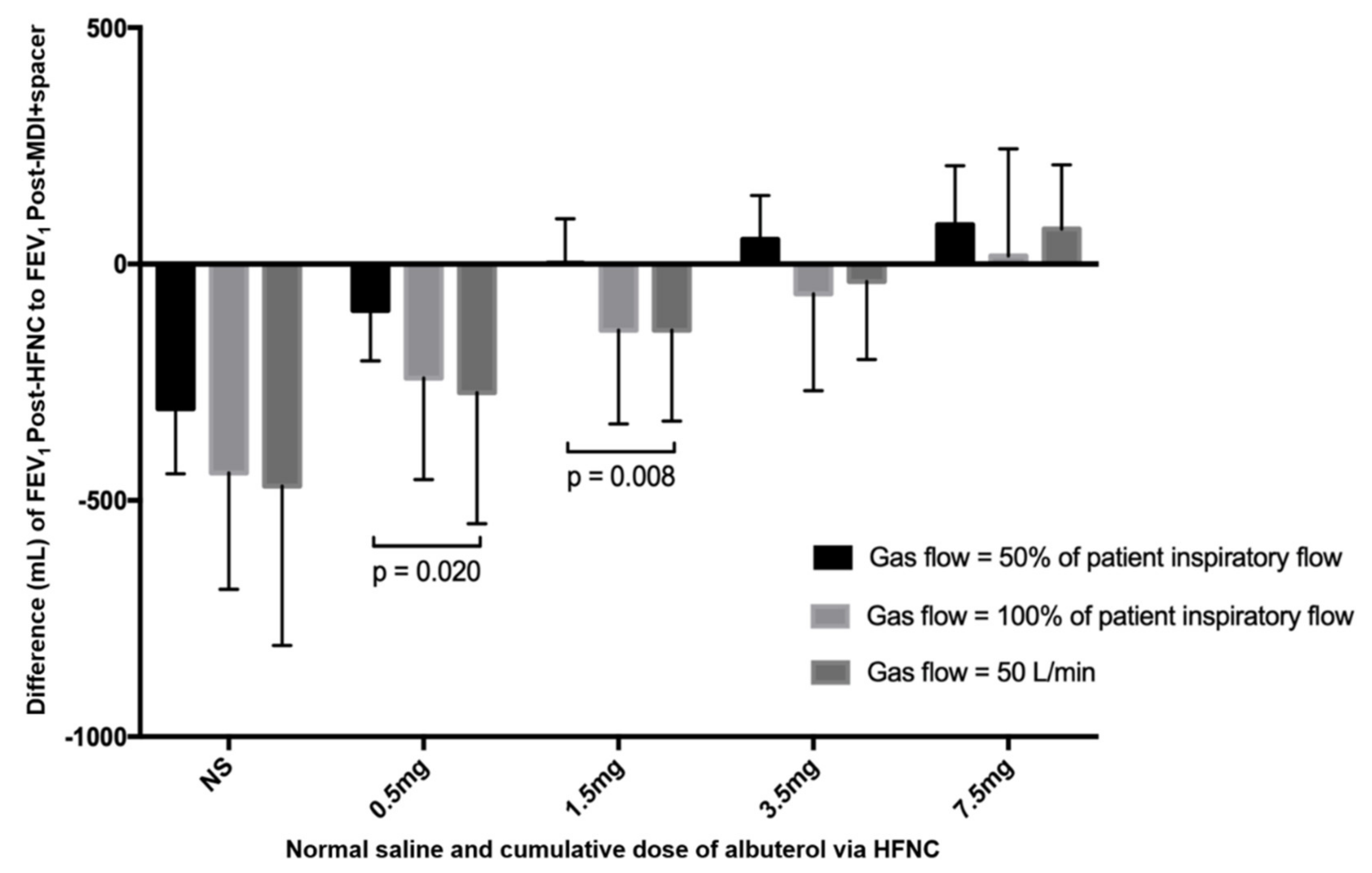
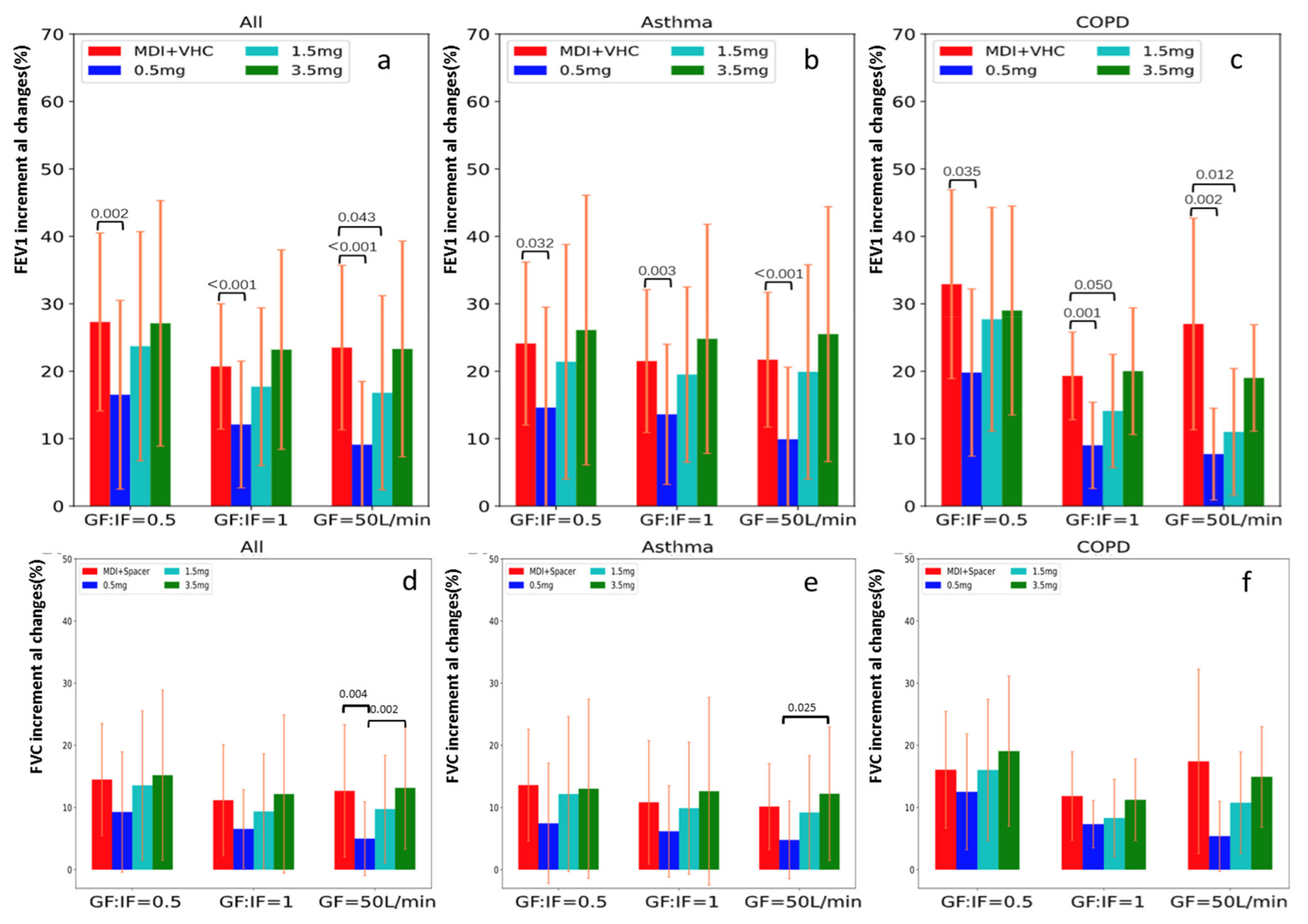
3.2. FEV1 and FVC Changes after Inhaling Salbutamol via MDI + VHC and via HFNC at Different Doses
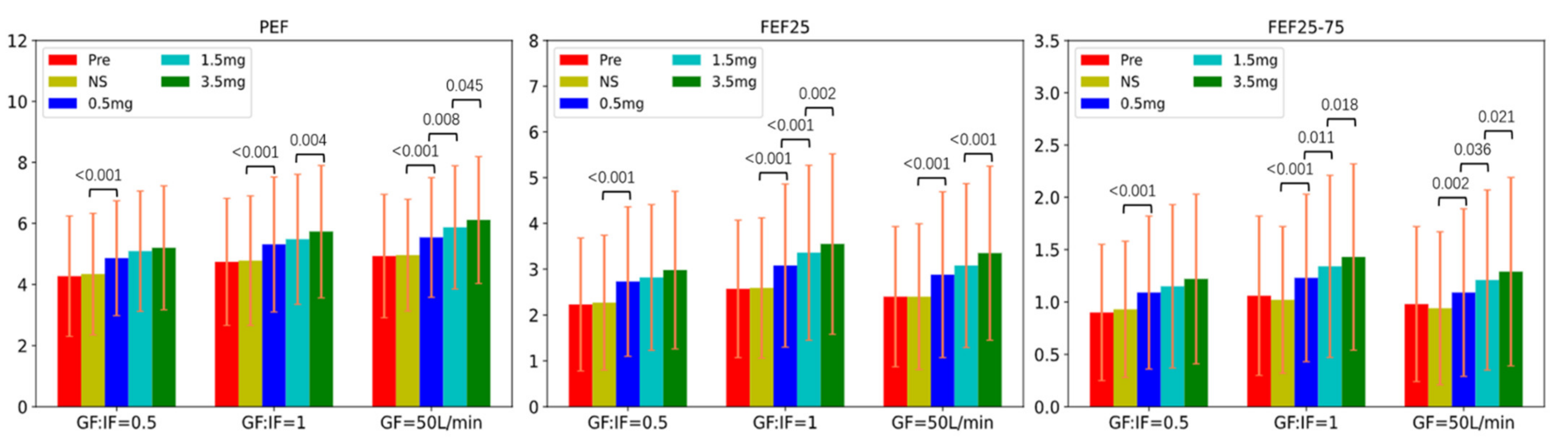
3.3. Other Spirometry Results of Inhaling Salbutamol at Different Doses
3.4. The Differences between Asthma and COPD Subjects at the Three HFNC Flows
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rochwerg, B.; Granton, D.; Wang, D.X.; Helviz, Y.; Einav, S.; Frat, J.P.; Mekontso-Dessap, A.; Schreiber, A.; Azoulay, E.; Mercat, A.; et al. High flow nasal cannula compared with conventional oxygen therapy for acute hypoxemic respiratory failure: A systematic review and meta-analysis. Intensive Care Med. 2019, 45, 563–572. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Jing, G.Q.; Scott, J.B. Year in review 2019: High-flow nasal cannula (HFNC) oxygen therapy for adult patients. Respir. Care 2020, 65, 545–557. [Google Scholar] [CrossRef]
- Rochwerg, B.; Einav, S.; Chaudhuri, D.; Mancebo, J.; Mauri, T.; Helviz, Y.; Goligher, E.C.; Jaber, S.; Ricard, J.-D.; Rittayamai, N.; et al. The role for high flow nasal cannula as a respiratory support strategy in adults: A clinical practice guideline. Intensive Care Med. 2020, 46, 2226–2237. [Google Scholar] [CrossRef] [PubMed]
- Helviz, Y.; Einav, S. A Systematic Review of the High-flow Nasal Cannula for Adult Patients. Crit. Care 2018, 22, 71. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Tu, M.; Yang, L.; Jing, G.; Fink, J.B.; Burtin, C.; de Andrade, A.D.; Gong, L.; Xie, L.; Ehrmann, S. Worldwide Clinical Practice of High-Flow Nasal Cannula and Concomitant Aerosol Therapy in the Adult ICU Setting. Respir. Care 2021, 66, 1416–1424. [Google Scholar] [CrossRef] [PubMed]
- Li, X.Y.; Tang, X.; Wang, R.; Yuan, X.; Zhao, Y.; Wang, L.; Li, H.-C.; Chu, H.-W.; Li, J.; Mao, W.-P.; et al. High-flow nasal cannula for chronic obstructive pulmonary disease with acute compen-sated hypercapnic respiratory failure: A randomized, controlled trial. Int. J. Chron. Obstruct. Pulmon. Dis. 2020, 15, 3051–3061. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Du, Y.; Ma, Z. High-flow nasal cannula oxygen versus conventional oxygen for hypercapnic chronic ob-structive pulmonary disease: A meta-analysis of randomized controlled trials. Clin. Respir. J. 2020, 15, 437–444. [Google Scholar] [CrossRef]
- Geng, W.; Batu, W.; You, S.; Tong, Z.; He, H. High-Flow Nasal Cannula: A Promising Oxygen Therapy for Patients with Severe Bronchial Asthma Complicated with Respiratory Failure. Can. Respir. J. 2020, 2020, 2301712. [Google Scholar] [CrossRef] [Green Version]
- Raeisi, S.; Fakharian, A.; Ghorbani, F.; Jamaati, H.R.; Mirenayat, M.S. Value and Safety of High Flow Oxygenation in the Treatment of Inpatient Asthma: A Randomized, Double-blind, Pilot Study. Iran. J. Allergy Asthma Immunol. 2020, 18, 615–623. [Google Scholar] [CrossRef]
- Jing, G.Q.; Li, J.; Hao, D. Comparison of high flow nasal cannula with noninvasive ventilation in chronic obstructive pulmonary disease patients with hypercapnia in preventing post extubation respiratory failure: A pilot randomized con-trolled trial. Res. Nurs. Health 2019, 42, 217–225. [Google Scholar] [CrossRef]
- Nagata, K.; Kikuchi, T.; Horie, T. Domiciliary high-flow nasal cannula oxygen therapy for patients with stable hy-percapnic chronic obstructive pulmonary disease. A multicenter randomized crossover trial. Ann. Am. Thorac. Soc. 2018, 15, 432–439. [Google Scholar] [CrossRef]
- Bennett, G.; Joyce, M.; Fernández, E.F.; MacLoughlin, R. Comparison of aerosol delivery across combinations of drug delivery interfaces with and without concurrent high-flow nasal therapy. Intensive Care Med. Exp. 2019, 7, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Fink, J.B.; MacLoughlin, R.; Dhand, R. A narrative review on trans-nasal pulmonary aerosol delivery. Crit. Care 2020, 24, 506. [Google Scholar] [CrossRef] [PubMed]
- Alalwan, M.A.; Fink, J.B.; Ari, A. In Vitro evaluation of aerosol drug delivery with and without high flow nasal cannula in children. Pediatr. Pulmonol. 2019, 54, 1968–1973. [Google Scholar] [CrossRef] [PubMed]
- Szychowiak, P.; Gensburger, S.; Bocar, T.; Landel, C.; Philippe, M.; Le Pennec, D.; Cabrera, M.; Mordier, L.; Vecellio, L.; Reminiac, F.; et al. Pressurized Metered Dose Inhaler Aerosol Delivery Within Nasal High-Flow Circuits: A Bench Study. J. Aerosol Med. Pulm. Drug Deliv. 2021, 34. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Gong, L.; Fink, J.B. The Ratio of Nasal Cannula Gas Flow to Patient Inspiratory Flow on Trans-nasal Pulmonary Aerosol Delivery for Adults: An in Vitro Study. Pharmaceutics 2019, 11, 225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Réminiac, F.; Vecellio, L.; Heuzé-Vourc’H, N.; Petitcollin, A.; Respaud, R.; Cabrera, M.; Le Pennec, D.; Diot, P.; Ehrmann, S. Aerosol Therapy in Adults Receiving High Flow Nasal Cannula Oxygen Therapy. J. Aerosol Med. Pulm. Drug Deliv. 2016, 29, 134–141. [Google Scholar] [CrossRef]
- Dailey, P.A.; Harwood, R.; Walsh, K.; Fink, J.B.; Thayer, T.; Gagnon, G.; Ari, A. Aerosol Delivery Through Adult High Flow Nasal Cannula With Heliox and Oxygen. Respir. Care 2017, 62, 1186–1192. [Google Scholar] [CrossRef]
- Li, J.; Zhao, M.; Hadeer, M.; Luo, J.; Fink, J.B. Dose Response to Transnasal Pulmonary Administration of Bronchodilator Aerosols via Nasal High-Flow Therapy in Adults with Stable Chronic Obstructive Pulmonary Disease and Asthma. Respiration 2019, 98, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Bräunlich, J.; Wirtz, H. Oral Versus Nasal High-Flow Bronchodilator Inhalation in Chronic Obstructive Pulmonary DiseaseNotation of prior abstract notification: Parts of the results were presented at ATS congress in 2017 as a thematic poster presentation. J. Aerosol Med. Pulm. Drug Deliv. 2018, 31, 248–254. [Google Scholar] [CrossRef]
- Reminiac, F.; Vecellio, L.; Bodet-Contentin, L.; Gissot, V.; Le Pennec, D.; Gandonnière, C.S.; Cabrera, M.; Dequin, P.-F.; Plantier, L.; Ehrmann, S. Nasal high-flow bronchodilator nebulization: A randomized cross-over study. Ann. Intensive Care 2018, 8, 128. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Gurnani, P.K.; Roberts, K.M.; Fink, J.B.; Vines, D. The Clinical Impact of Flow Titration on Epoprostenol Delivery via High Flow Nasal Cannula for ICU Patients with Pulmonary Hypertension or Right Ventricular Dysfunction: A Retrospective Cohort Comparison Study. J. Clin. Med. 2020, 9, 464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Harnois, L.J.; Markos, B. Epoprostenol delivered via high flow nasal cannula for ICU subjects with severe hy-poxemia comorbid with pulmonary hypertension or right heart dysfunction. Pharmaceutics 2019, 11, 281. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Luo, J.; Chen, Y. Effects of flow rate on trans-nasal pulmonary aerosol delivery of bronchodilators via high-flow nasal cannula for COPD and asthma patients: Protocol for a randomized controlled trial. BMJ Open 2019, 9, e028584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; Van Der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Wu, W.; Fink, J.B. In Vitro comparison between inspiration synchronized and continuous vibrating mesh nebulizer during trans-nasal aerosol delivery. Intensive Care Med. Exp. 2020, 8, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef] [PubMed]
- Fishwick, D.; Bradshaw, L.; Macdonald, C. Cumulative and single dose design to assess the bronchodilator effects of beta2-agonists in individuals with asthma. Am. J. Respir. Crit. Care Med. 2001, 163, 474–477. [Google Scholar] [CrossRef]
- Corda, L.; La Piana, G.; Bertella, E.; Taranto-Montemurro, L.; Pini, L.; Tantucci, C. Dose-response curve to salbutamol during acute and chronic treatment with formoterol in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2011, 6, 399–405. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Wu, W.; Fink, J.B. In Vitro comparison of unit dose versus infusion pump administration of albuterol via high-flow nasal cannula in toddlers. Pediatr. Pulmonol. 2020, 55, 322–329. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Information | GF:IF = 0.5 (n = 25) | GF:IF = 1.0 (n = 24) | GF = 50 L/min (n = 26) | p |
|---|---|---|---|---|
| Age, years | 51.2 ± 13.4 | 51.9 ± 16.6 | 51.1 ± 14.0 | 0.978 |
| Male, % | 16 (64%) | 14 (58%) | 18 (69%) | 0.725 |
| Asthma, % | 16 (64%) | 16 (67%) | 17 (65%) | 0.981 |
| COPD, % | 9 (36%) | 8 (33%) | 9 (35%) | |
| Height, cm | 164.3 ± 6.8 | 166.2 ± 7.4 | 164.4 ± 7.7 | 0.587 |
| Weight, Kg | 71.7 ± 11.3 | 72.2 ± 12.8 | 68.7 ± 11.0 | 0.510 |
| BMI, Kg/m2 | 26.5 ± 3.5 | 26.0 ± 3.3 | 25.4 ± 3.6 | 0.523 |
| Vt, mL | 766.4 ± 146.0 | 740.0 ± 190.3 | 800.2 ± 215.7 | 0.519 |
| Peak inspiratory flow during tidal breathing, L/min | 37.4 ± 7.8 | 34.5 ± 6.9 | 38.2 ± 6.0 | 0.137 |
| HFNC flow settings, L/min | 18.7 ± 3.9 | 34.5 ± 6.9 | 50 | <0.001 |
| Smoker, % | 11 (44%) | 11 (46%) | 11 (42%) | 0.969 |
| Number of Patients (%) | Cumulative Dose | GF: IF = 0.5 (n = 25) | GF: IF = 1.0 (n = 24) | GF = 50 L/min (n = 26) | p | |
|---|---|---|---|---|---|---|
| Criteria for bronchodilation responses | FEV1 increased by 200 mL and 12% | Saline | 1 (4%) | 0 | 1 (4%) | NA |
| 0.5 mg | 11 (44%) | 6 (25%) | 7 (27%) | 0.286 | ||
| 1.5 mg | 16 (64%) | 14 (58%) | 11 (42%) | 0.271 | ||
| 3.5 mg | 17 (68%) | 18 (75%) | 18 (69%) | 0.848 | ||
| FEV1 via HFNC ≥ FEV1 post MDI + Spacer | Saline | 1 (4%) | 0 | 0 | NA | |
| 0.5 mg | 4 (16%) | 3 (13%) | 4 (15%) | 0.934 | ||
| 1.5 mg | 16 (64%) | 7 (29%) | 7 (27%) | 0.011 | ||
| 3.5 mg | 22 (88%) | 11 (46%) | 14 (54%) | 0.005 | ||
| Met either of the two criteria of FEV1 | 0.5 mg | 13 (52%) | 8 (33%) | 10 (39%) | 0.388 | |
| 1.5 mg | 19 (76%) | 17 (71%) | 14 (54%) | 0.213 | ||
| 3.5 mg | 23 (92%) | 20 (83%) | 21 (81%) | 0.497 | ||
| Met both criteria of FEV1 | 0.5 mg | 2 (8%) | 1 (4%) | 1 (4%) | NA | |
| 1.5 mg | 13 (52%) | 4 (17%) | 4 (15%) | 0.013 | ||
| 3.5 mg | 16 (64%) | 9 (38%) | 11 (42%) | 0.366 | ||
| FVC increased by 200 mL and 12% | 0.5 mg | 8 (32%) | 5 (20%) | 5 (19%) | 0.513 | |
| 1.5 mg | 13 (52%) | 8 (33%) | 10 (39%) | 0.388 | ||
| 3.5 mg | 13 (52%) | 10 (42%) | 15 (58%) | 0.520 | ||
| Inhalation Device | FEV1 Changes | GF:IF = 0.5 (n = 25) | GF:IF = 1.0 (n = 24) | GF = 50 L/min (n = 26) | p |
|---|---|---|---|---|---|
| FEV1 (L) salbutamol (400 mcg) via MDI + VHC | Pre | 1.65 ± 0.79 | 1.98 ± 0.80 | 1.91 ± 0.80 | 0.321 a |
| Pre FEV1 in predicted (%) | 56.5 ± 23.8 | 66.2 ± 18.1 | 64.0 ± 18.9 | 0.221 a | |
| Post | 2.03 ± 0.83 | 2.34 ± 0.86 | 2.30 ± 0.87 | 0.577 a | |
| Increase | 0.375 ± 0.125 | 0.365 ± 0.110 | 0.389 ± 0.135 | 0.577 a | |
| Increase (%) | 27.3 ± 13.2 | 20.7 ± 9.3 | 23.5 ± 12.2 | 0.429 a | |
| FEV1 (L) with saline and salbutamol via VMN + HFNC | Pre | 1.72 ± 0.84 | 1.91 ± 0.79 | 1.87 ± 0.80 | 0.691 a |
| Pre FEV1 in predicted (%) | 58.5 ± 24.7 | 64.0 ± 19.0 | 63.2 ± 19.7 | 0.613 a | |
| Saline | 1.74 ± 0.87 | 1.90 ± 0.77 | 1.83 ± 0.81 | 0.060 b | |
| 0.5 mg | 1.95 ± 0.86 | 2.10 ± 0.80 | 2.02 ± 0.81 | 0.194 b | |
| 1.5 mg | 2.05 ± 0.86 | 2.20 ± 0.81 | 2.16 ± 0.84 | 0.804 b | |
| 3.5 mg | 2.09 ± 0.87 | 2.28 ± 0.80 | 2.26 ± 0.84 | 0.968 b | |
| 7.5 mg c | 2.20 ± 0.93 | 2.21 ± 0.95 | 2.35 ± 0.89 | 0.567 b | |
| FEV1 increment (ml) with saline and salbutamol via VMN + HFNC | Saline | 23 ± 87 | −5 ± 65 | −47 ± 139 | 0.060 b |
| 0.5 mg | 228 ± 146 | 197 ± 148 | 152 ± 147 | 0.194 b | |
| 1.5 mg | 321 ± 161 | 298 ± 191 | 284 ± 240 | 0.804 b | |
| 3.5 mg | 373 ± 171 | 375 ± 215 | 387 ± 264 | 0.968 b | |
| FEV1 increment (%) with saline and salbutamol via VMN + HFNC | Saline | 0.7 ± 7.5 | 0 ± 5.0 | −3.0 ± 8.5 | 0.140 b |
| 0.5 mg | 16.5 ± 14.0 | 12.1 ± 9.4 | 9.1 ± 9.4 | 0.087 b | |
| 1.5 mg | 23.7 ± 17.0 | 17.7 ± 11.7 | 16.8 ± 14.4 | 0.283 b | |
| 3.5 mg | 27.1 ± 18.2 | 23.2 ± 14.8 | 23.3 ± 16.0 | 0.831 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Chen, Y.; Ehrmann, S.; Wu, J.; Xie, L.; Fink, J.B. Bronchodilator Delivery via High-Flow Nasal Cannula: A Randomized Controlled Trial to Compare the Effects of Gas Flows. Pharmaceutics 2021, 13, 1655. https://doi.org/10.3390/pharmaceutics13101655
Li J, Chen Y, Ehrmann S, Wu J, Xie L, Fink JB. Bronchodilator Delivery via High-Flow Nasal Cannula: A Randomized Controlled Trial to Compare the Effects of Gas Flows. Pharmaceutics. 2021; 13(10):1655. https://doi.org/10.3390/pharmaceutics13101655
Chicago/Turabian StyleLi, Jie, Yibing Chen, Stephan Ehrmann, Jie Wu, Lixin Xie, and James B Fink. 2021. "Bronchodilator Delivery via High-Flow Nasal Cannula: A Randomized Controlled Trial to Compare the Effects of Gas Flows" Pharmaceutics 13, no. 10: 1655. https://doi.org/10.3390/pharmaceutics13101655