
Physiologic Effects of Instilled and Aerosolized Surfactant Using a Breath-Synchronized Nebulizer on Surfactant-Deficient Rabbits †


Abstract
:1. Introduction
2. Methods
2.1. Surgical Preparation/Instrumentation
2.2. Induction of Surfactant-Deficiency and Lung Injury
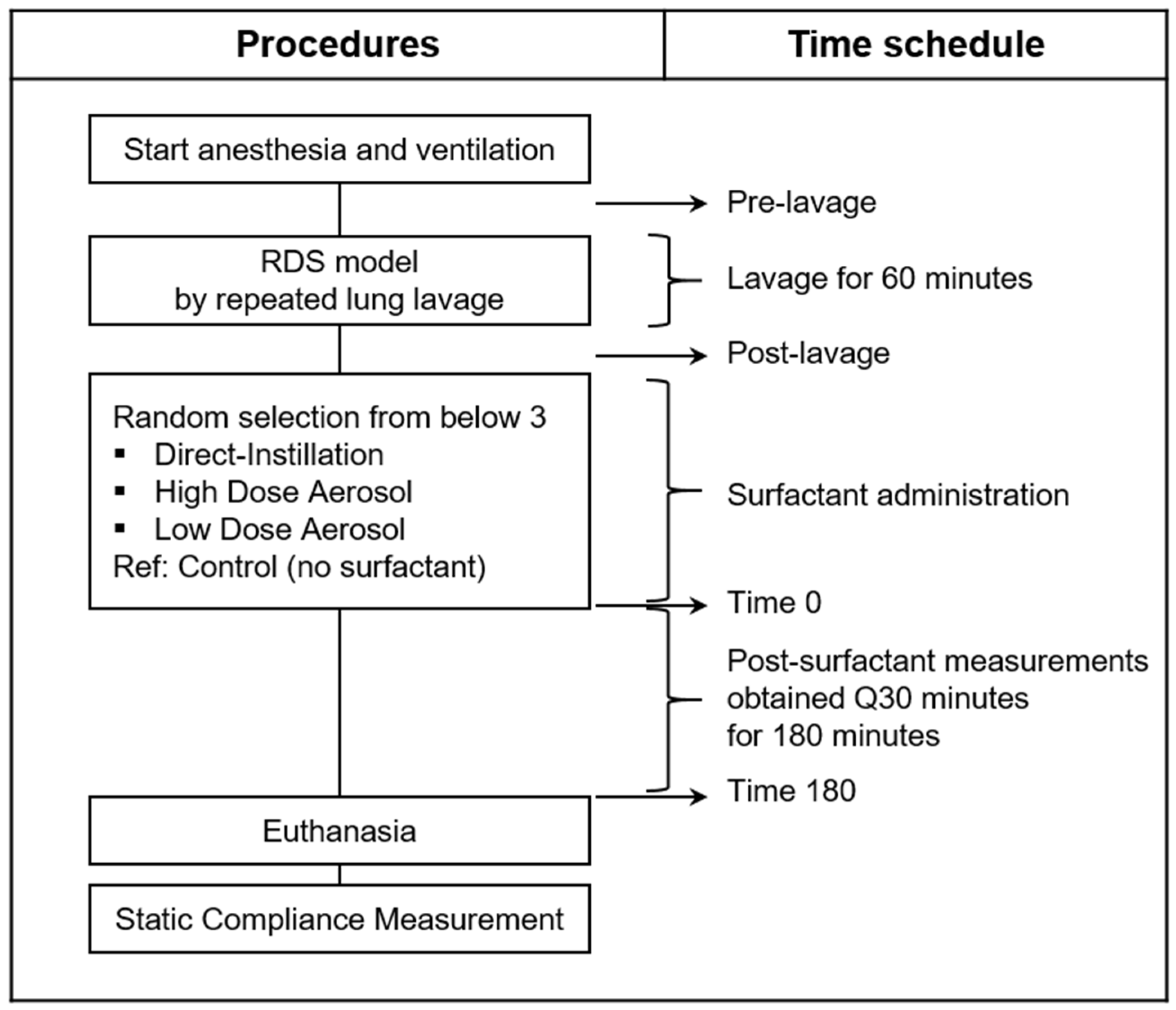
2.3. Experimental Protocol
2.4. Intratracheal Liquid Surfactant Administration (Direct-Instillation)
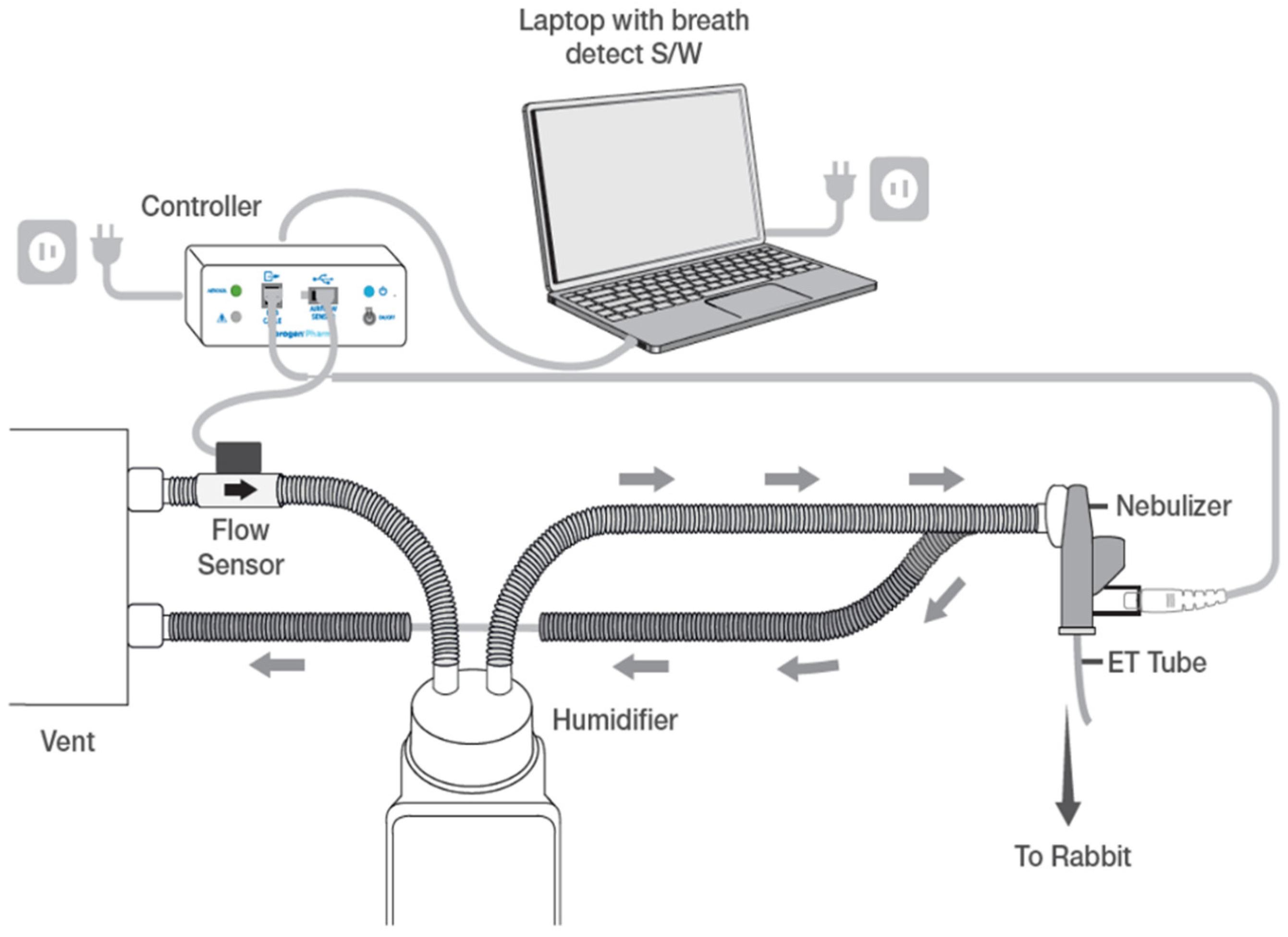
2.5. Breath-Synchronized Aerosolized Surfactant (High and Low Dose Aerosol)
2.6. Peridosing Events
2.7. Physiologic Measurements
2.8. Statistical Analysis
3. Results
3.1. Animal Descriptions
3.2. Peridosing Events
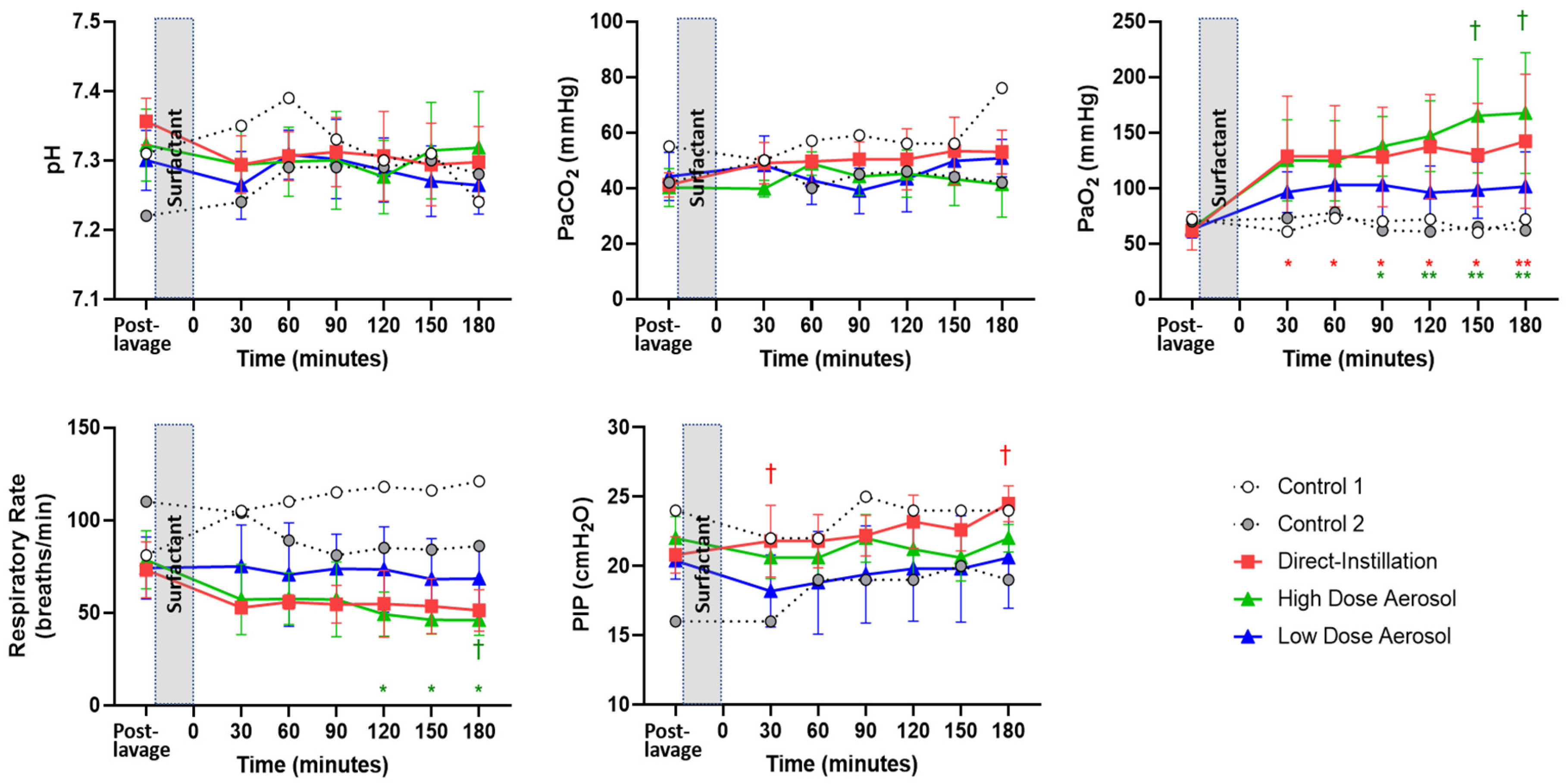
3.3. Hemodynamics, Gas exchange and Ventilation Parameters
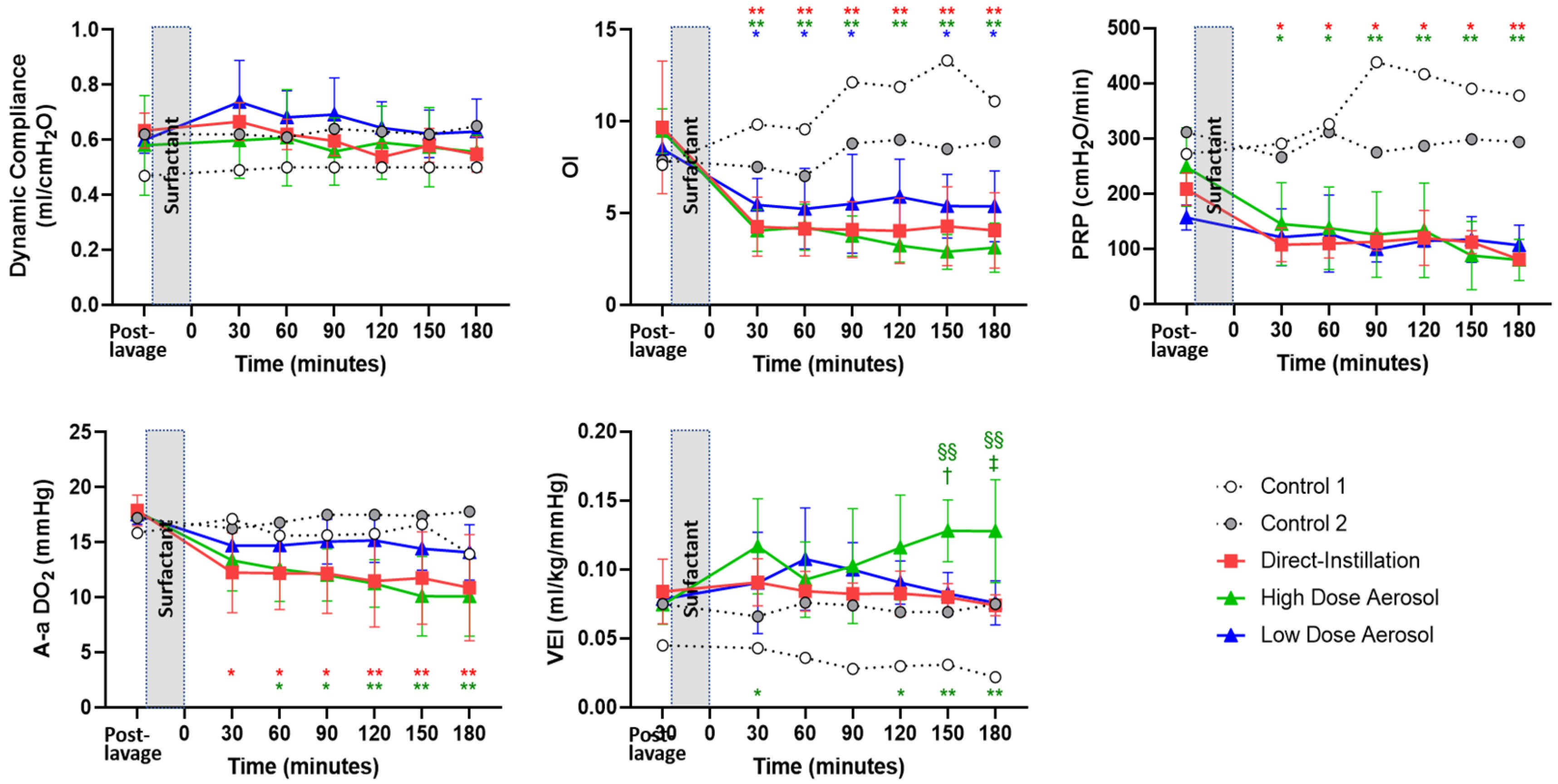
3.4. Indices of Disease Severity
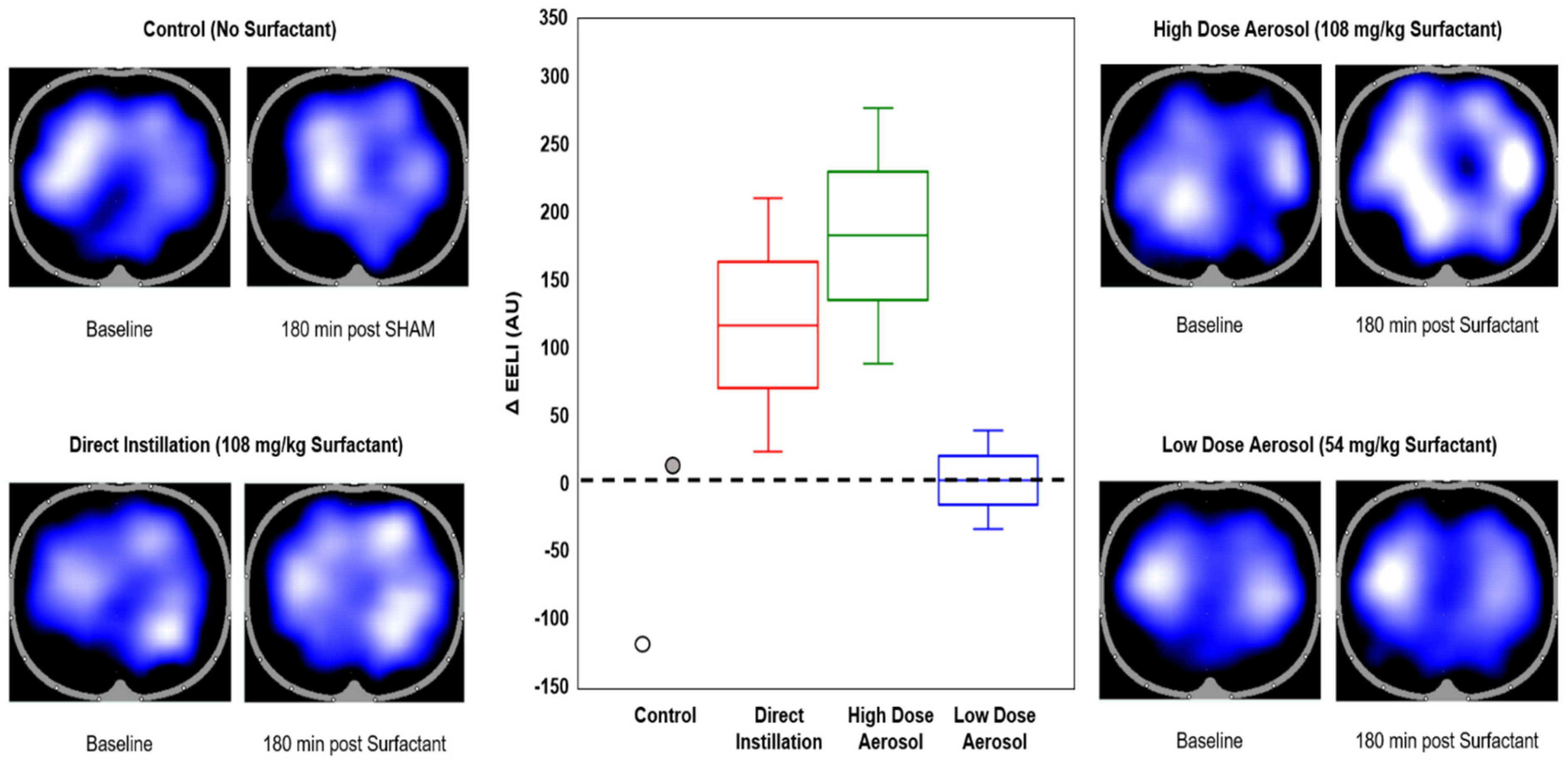
3.5. Electrical Impedance Tomography
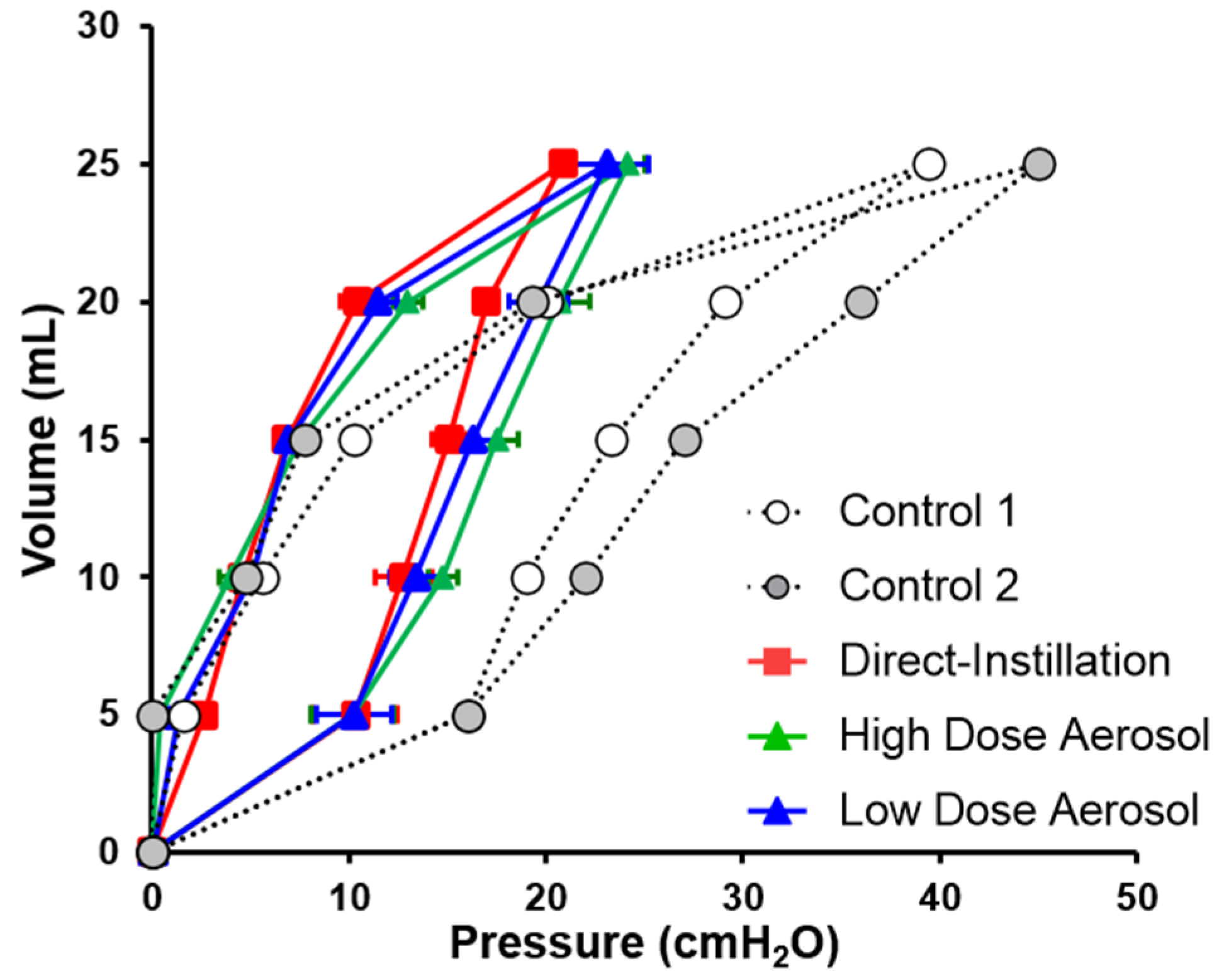
3.6. Lung Mechanics
4. Discussion
4.1. Limitations
4.2. Clinical Implications for the Proposed Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Walsh, B.K.; Daigle, B.; DiBlasi, R.M.; Restrepo, R.D.; American Association for Respiratory, C. AARC Clinical Practice Guideline. Surfactant replacement therapy: 2013. Respir. Care 2013, 58, 367–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bancalari, E.; Jain, D. Bronchopulmonary Dysplasia: 50 Years after the Original Description. Neonatology 2019, 115, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Nouraeyan, N.; Lambrinakos-Raymond, A.; Leone, M.; Sant’Anna, G. Surfactant administration in neonates: A review of delivery methods. Can. J. Respir. 2014, 50, 91–95. [Google Scholar]
- Horbar, J.D.; Wright, E.C.; Onstad, L. Decreasing mortality associated with the introduction of surfactant therapy: An observational study of neonates weighing 601 to 1300 grams at birth. The Members of the National Institute of Child Health and Human Development Neonatal Research Network. Pediatrics 1993, 92, 191–196. [Google Scholar] [PubMed]
- Goldsmith, L.S.; Greenspan, J.S.; Rubenstein, S.D.; Wolfson, M.R.; Shaffer, T.H. Immediate improvement in lung volume after exogenous surfactant: Alveolar recruitment versus increased distention. J. Pediatr. 1991, 119, 424–428. [Google Scholar] [CrossRef]
- Nilsson, R.; Grossmann, G.; Robertson, B. Lung surfactant and the pathogenesis of neonatal bronchiolar lesions induced by artificial ventilation. Pediatr. Res. 1978, 12, 249–255. [Google Scholar] [CrossRef] [Green Version]
- Hillman, N.H.; Moss, T.J.; Kallapur, S.G.; Bachurski, C.; Pillow, J.J.; Polglase, G.R.; Nitsos, I.; Kramer, B.W.; Jobe, A.H. Brief, large tidal volume ventilation initiates lung injury and a systemic response in fetal sheep. Am. J. Respir. Crit. Care Med. 2007, 176, 575–581. [Google Scholar] [CrossRef] [Green Version]
- Bjorklund, L.J.; Ingimarsson, J.; Curstedt, T.; John, J.; Robertson, B.; Werner, O.; Vilstrup, C.T. Manual ventilation with a few large breaths at birth compromises the therapeutic effect of subsequent surfactant replacement in immature lambs. Pediatr. Res. 1997, 42, 348–355. [Google Scholar] [CrossRef] [Green Version]
- Hentschel, R.; Brune, T.; Franke, N.; Harms, E.; Jorch, G. Sequential changes in compliance and resistance after bolus administration or slow infusion of surfactant in preterm infants. Intensive Care Med. 2002, 28, 622–628. [Google Scholar] [CrossRef]
- Miedema, M.; de Jongh, F.H.; Frerichs, I.; van Veenendaal, M.B.; van Kaam, A.H. Changes in lung volume and ventilation during surfactant treatment in ventilated preterm infants. Am. J. Respir. Crit. Care Med. 2011, 184, 100–105. [Google Scholar] [CrossRef] [Green Version]
- Jorch, G.; Rabe, H.; Garbe, M.; Michel, E.; Gortner, L. Acute and protracted effects of intratracheal surfactant application on internal carotid blood flow velocity, blood pressure and carbondioxide tension in very low birth weight infants. Eur. J. Pediatr. 1989, 148, 770–773. [Google Scholar] [CrossRef]
- van Bel, F.; de Winter, P.J.; Wijnands, H.B.; van de Bor, M.; Egberts, J. Cerebral and aortic blood flow velocity patterns in preterm infants receiving prophylactic surfactant treatment. Acta Paediatr. 1992, 81, 504–510. [Google Scholar] [CrossRef]
- Fernandez-Ruanova, M.B.; Alvarez, F.J.; Gastiasoro, E.; Arnaiz, A.; Robertson, B.; Curstedt, T.; Valls-i-Soler, A. Comparison of rapid bolus instillation with simplified slow administration of surfactant in lung lavaged rats. Pediatr. Pulmonol. 1998, 26, 129–134. [Google Scholar] [CrossRef]
- Segerer, H.; van Gelder, W.; Angenent, F.W.; van Woerkens, L.J.; Curstedt, T.; Obladen, M.; Lachmann, B. Pulmonary distribution and efficacy of exogenous surfactant in lung-lavaged rabbits are influenced by the instillation technique. Pediatr. Res. 1993, 34, 490–494. [Google Scholar] [CrossRef] [Green Version]
- Ueda, T.; Ikegami, M.; Rider, E.D.; Jobe, A.H. Distribution of surfactant and ventilation in surfactant-treated preterm lambs. J. Appl. Physiol. 1994, 76, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Dijk, P.H.; Heikamp, A.; Piers, D.A.; Weller, E.; Bambang Oetomo, S. Surfactant nebulisation: Safety, efficiency and influence on surface lowering properties and biochemical composition. Intensive Care Med. 1997, 23, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Syedain, Z.H.; Naqwi, A.A.; Dolovich, M.; Somani, A. In Vitro Evaluation of a Device for Intra-Pulmonary Aerosol Generation and Delivery. Aerosol. Sci. Technol. 2015, 49, 747–752. [Google Scholar] [CrossRef] [Green Version]
- Dijk, P.H.; Heikamp, A.; Bambang Oetomo, S. Surfactant nebulisation: Lung function, surfactant distribution and pulmonary blood flow distribution in lung lavaged rabbits. Intensive Care Med. 1997, 23, 1070–1076. [Google Scholar] [CrossRef] [PubMed]
- Dijk, P.H.; Heikamp, A.; Bambang Oetomo, S. Surfactant nebulisation prevents the adverse effects of surfactant therapy on blood pressure and cerebral blood flow in rabbits with severe respiratory failure. Intensive Care Med. 1997, 23, 1077–1081. [Google Scholar] [CrossRef] [PubMed]
- Brasher, M.; Raffay, T.M.; Cunningham, M.D.; Abu Jawdeh, E.G. Aerosolized Surfactant for Preterm Infants with Respiratory Distress Syndrome. Children 2021, 8, 493. [Google Scholar] [CrossRef]
- Jorch, G.; Hartl, H.; Roth, B.; Kribs, A.; Gortner, L.; Schaible, T.; Hennecke, K.H.; Poets, C. Surfactant aerosol treatment of respiratory distress syndrome in spontaneously breathing premature infants. Pediatr. Pulmonol. 1997, 24, 222–224. [Google Scholar] [CrossRef]
- Fok, T.F.; al-Essa, M.; Dolovich, M.; Rasid, F.; Kirpalani, H. Nebulisation of surfactants in an animal model of neonatal respiratory distress. Arch. Dis. Child. Fetal. Neonatal. Ed. 1998, 78, F3–F9. [Google Scholar] [CrossRef] [PubMed]
- DiBlasi, R.M.; Kearney, C.N.; Hotz, J.C.; Salyer, J.W.; Poli, J.A.; Crotwell, D.N.; Hartmann, S.M. Physiologic Effects of 3 Different Neonatal Volume-Targeted Ventilation Modes in Surfactant-Deficient Juvenile Rabbits. Respir. Care 2019, 64, 361–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baydur, A.; Behrakis, P.K.; Zin, W.A.; Jaeger, M.; Milic-Emili, J. A simple method for assessing the validity of the esophageal balloon technique. Am. Rev. Respir. Dis. 1982, 126, 788–791. [Google Scholar] [CrossRef]
- Cogo, P.E.; Facco, M.; Simonato, M.; Verlato, G.; Rondina, C.; Baritussio, A.; Toffolo, G.M.; Carnielli, V.P. Dosing of porcine surfactant: Effect on kinetics and gas exchange in respiratory distress syndrome. Pediatrics 2009, 124, e950–e957. [Google Scholar] [CrossRef] [PubMed]
- Kopincova, J.; Mikolka, P.; Kolomaznik, M.; Kosutova, P.; Calkovska, A.; Mokra, D. Selective inhibition of NF-kappaB and surfactant therapy in experimental meconium-induced lung injury. Physiol. Res. 2017, 66, S227–S236. [Google Scholar] [CrossRef] [PubMed]
- Notter, R.H.; Egan, E.A.; Kwong, M.S.; Holm, B.A.; Shapiro, D.L. Lung surfactant replacement in premature lambs with extracted lipids from bovine lung lavage: Effects of dose, dispersion technique, and gestational age. Pediatr. Res. 1985, 19, 569–577. [Google Scholar] [CrossRef] [Green Version]
- Katalan, S.; Falach, R.; Rosner, A.; Goldvaser, M.; Brosh-Nissimov, T.; Dvir, A.; Mizrachi, A.; Goren, O.; Cohen, B.; Gal, Y.; et al. A novel swine model of ricin-induced acute respiratory distress syndrome. Dis. Model. Mech. 2017, 10, 173–183. [Google Scholar] [CrossRef] [Green Version]
- Ringer, C.N.; Engberg, R.J.; Carlin, K.E.; Smallwood, C.D.; DiBlasi, R.M. Physiologic Effects of Nasal Aspiration and Nasopharyngeal Suctioning on Infants With Viral Bronchiolitis. Respir. Care 2020, 65, 984–993. [Google Scholar] [CrossRef]
- Hinz, J.; Hahn, G.; Neumann, P.; Sydow, M.; Mohrenweiser, P.; Hellige, G.; Burchardi, H. End-expiratory lung impedance change enables bedside monitoring of end-expiratory lung volume change. Intensive Care Med. 2003, 29, 37–43. [Google Scholar] [CrossRef]
- van Genderingen, H.R.; van Vught, A.J.; Jansen, J.R. Estimation of regional lung volume changes by electrical impedance pressures tomography during a pressure-volume maneuver. Intensive Care Med. 2003, 29, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Riedel, T.; Kyburz, M.; Latzin, P.; Thamrin, C.; Frey, U. Regional and overall ventilation inhomogeneities in preterm and term-born infants. Intensive Care Med. 2009, 35, 144–151. [Google Scholar] [CrossRef] [Green Version]
- Wheeler, K.I.; Davis, P.G.; Kamlin, C.O.; Morley, C.J. Assist control volume guarantee ventilation during surfactant administration. Arch. Dis. Child. Fetal. Neonatal. Ed. 2009, 94, F336–F338. [Google Scholar] [CrossRef]
- Lewis, J.F.; McCaig, L. Aerosolized versus instilled exogenous surfactant in a nonuniform pattern of lung injury. Am. Rev. Respir. Dis. 1993, 148, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Popow, C.; Simbruner, G. Comparison between dynamic lung compliance and static compliance of the respiratory system in sick newborn infants. Wien. Klin. Wochenschr. 1988, 100, 153–157. [Google Scholar] [PubMed]
- DiBlasi, R.M.; Kajimoto, M.; Poli, J.A.; Deutsch, G.; Pfeiffer, J.; Zimmerman, J.; Crotwell, D.N.; Malone, P.; Fink, J.B.; Ringer, C.; et al. Breath-Synchronized Nebulized Surfactant in a Porcine Model of Acute Respiratory Distress Syndrome. Crit. Care Explor. 2021, 3, e0338. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (n = 2) | Direct-Instillation (n = 5) | High Dose Aerosol (n = 5) | Low Dose Aerosol (n = 5) | p Value | |
|---|---|---|---|---|---|
| BW (kg) | 1.25, 1.55 | 1.57 ± 0.17 | 1.54 ± 0.24 | 1.47 ± 0.20 | 0.75 |
| PaCO2 (mmHg) | 55, 42 | 41 ± 4 | 40 ± 7 | 44 ± 8 | 0.64 |
| PaO2 (mmHg) | 72, 70 | 62 ± 17 | 64 ± 7 | 63 ± 8 | 0.95 |
| Compliance (ml/cmH2O) | 0.47, 0.62 | 0.63 ± 0.06 | 0.58 ± 0.18 | 0.60 ± 0.05 | 0.76 |
| OI | 7.64, 7.88 | 9.68 ± 3.61 | 9.48 ± 1.21 | 8.51 ± 0.90 | 0.69 |
| VEI (mL/kg/mmHg) | 0.05, 0.08 | 0.08 ± 0.02 | 0.07 ± 0.01 | 0.08 ± 0.01 | 0.66 |
| A-aDO2 (mmHg) | 15.9, 17.2 | 17.9 ± 1.4 | 17.8 ± 0.6 | 17.5 ± 0.9 | 0.84 |
| Lavages (n) | 10, 9 | 10 ± 2 | 10 ± 2 | 9 ± 3 | 0.92 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
DiBlasi, R.M.; Micheletti, K.J.; Zimmerman, J.D.; Poli, J.A.; Fink, J.B.; Kajimoto, M. Physiologic Effects of Instilled and Aerosolized Surfactant Using a Breath-Synchronized Nebulizer on Surfactant-Deficient Rabbits. Pharmaceutics 2021, 13, 1580. https://doi.org/10.3390/pharmaceutics13101580
DiBlasi RM, Micheletti KJ, Zimmerman JD, Poli JA, Fink JB, Kajimoto M. Physiologic Effects of Instilled and Aerosolized Surfactant Using a Breath-Synchronized Nebulizer on Surfactant-Deficient Rabbits. Pharmaceutics. 2021; 13(10):1580. https://doi.org/10.3390/pharmaceutics13101580
Chicago/Turabian StyleDiBlasi, Robert M., Kellie J. Micheletti, Joseph D. Zimmerman, Jonathan A. Poli, James B. Fink, and Masaki Kajimoto. 2021. "Physiologic Effects of Instilled and Aerosolized Surfactant Using a Breath-Synchronized Nebulizer on Surfactant-Deficient Rabbits" Pharmaceutics 13, no. 10: 1580. https://doi.org/10.3390/pharmaceutics13101580