
Evaluation of Aerosol Drug Delivery Options during Adult Mechanical Ventilation in the COVID-19 Era

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
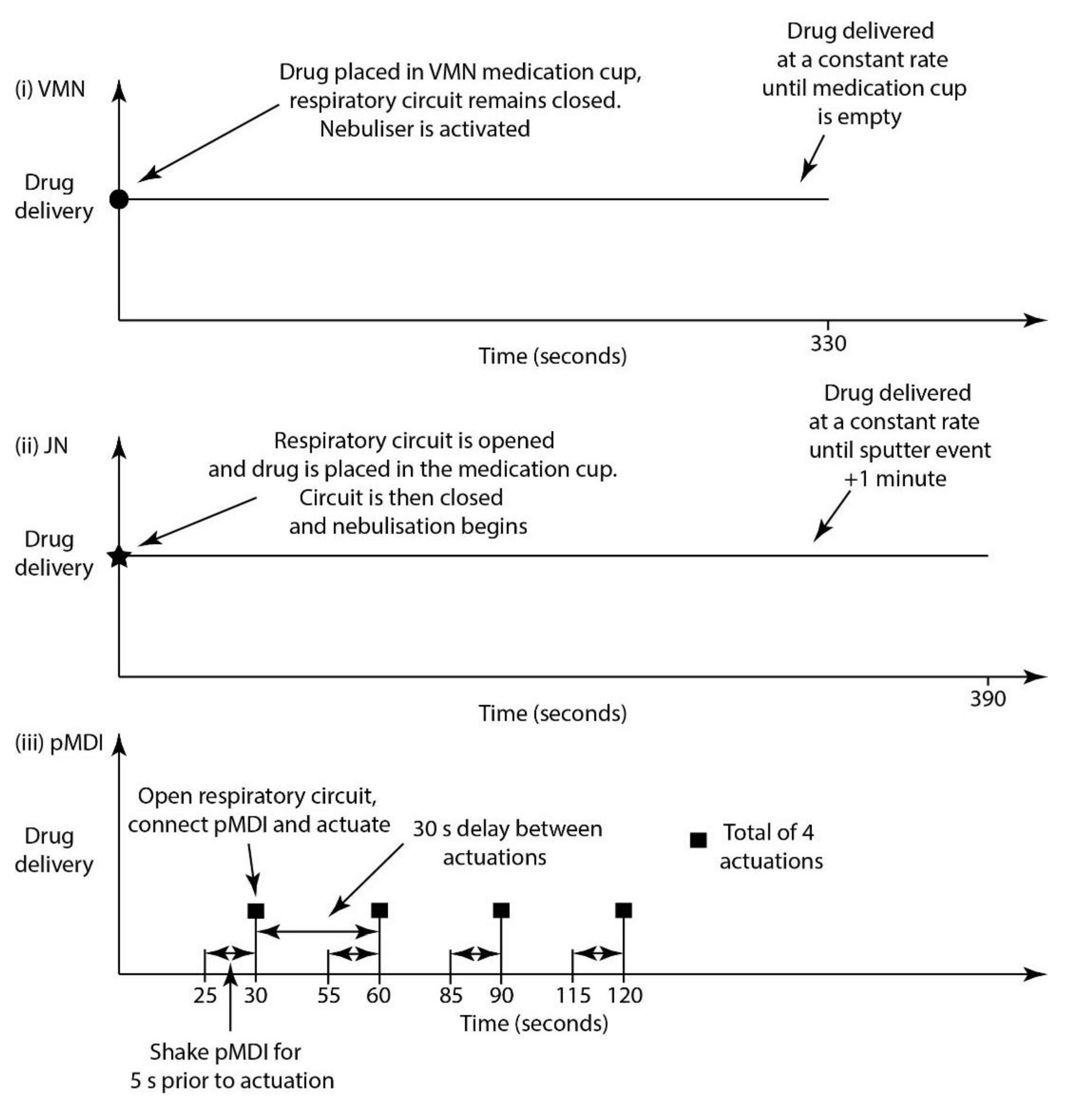
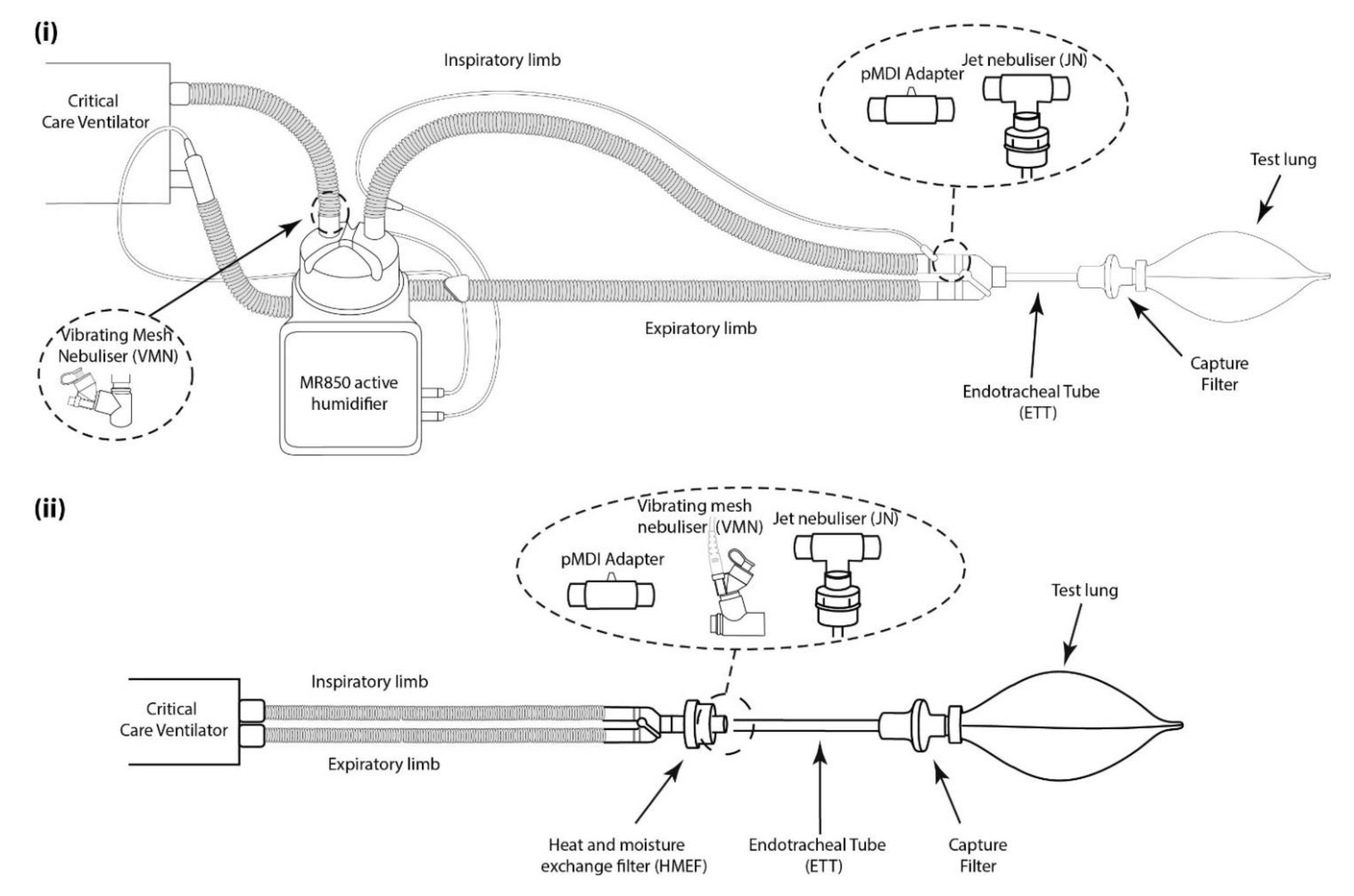
2.1. Drug Delivery Devices
2.2. Drug Delivery Determination
2.3. Aerosol Dose Efficiency during Simulated Invasive Mechanical Ventilation
2.4. Residual Drug Determination
2.5. Ventilator Circuit Pressure Determination
2.6. Data Analysis
3. Results
3.1. Droplet Size Determination
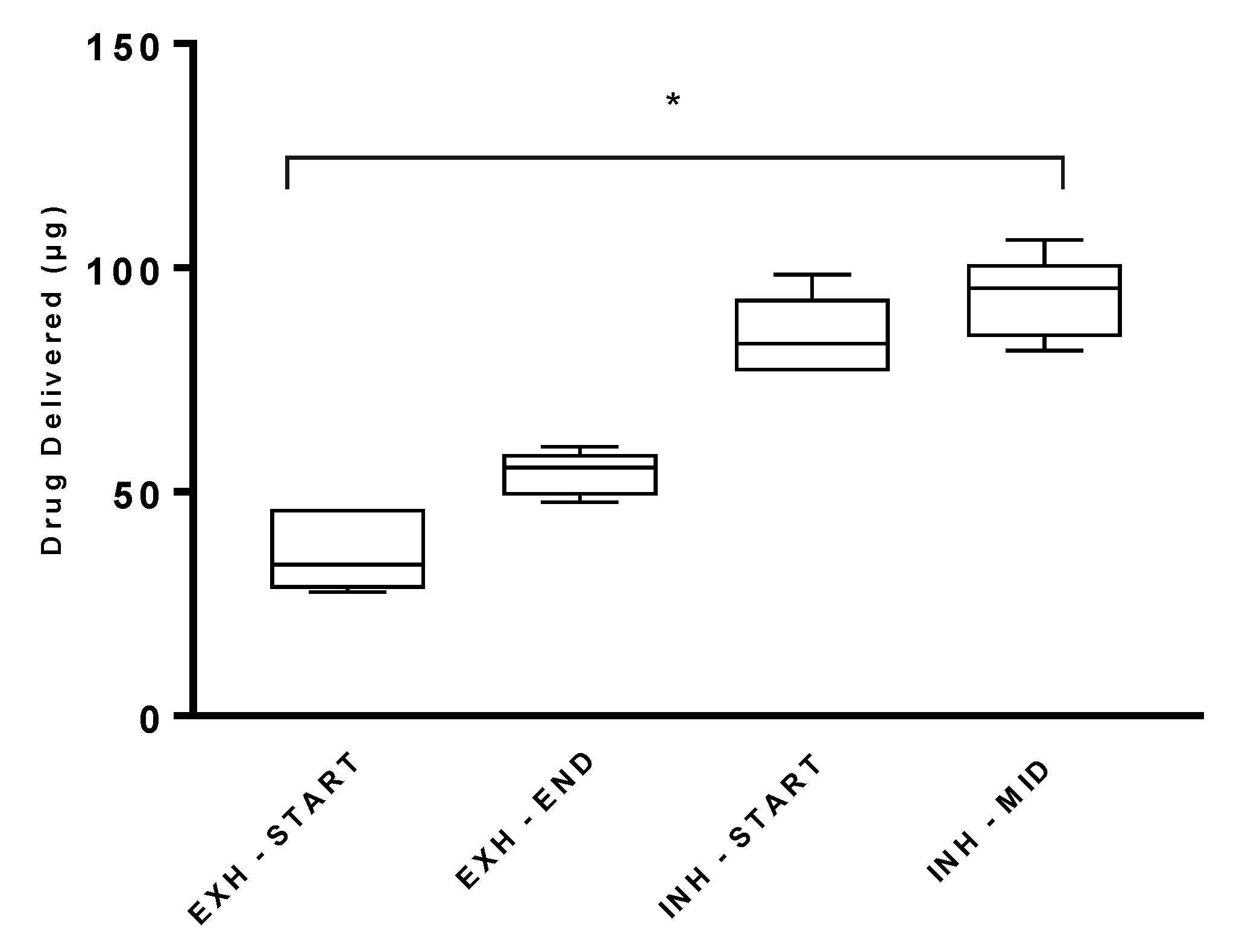
3.2. Effect of pMDI Actuation Timing during the Respiratory Cycle on Drug Delivery
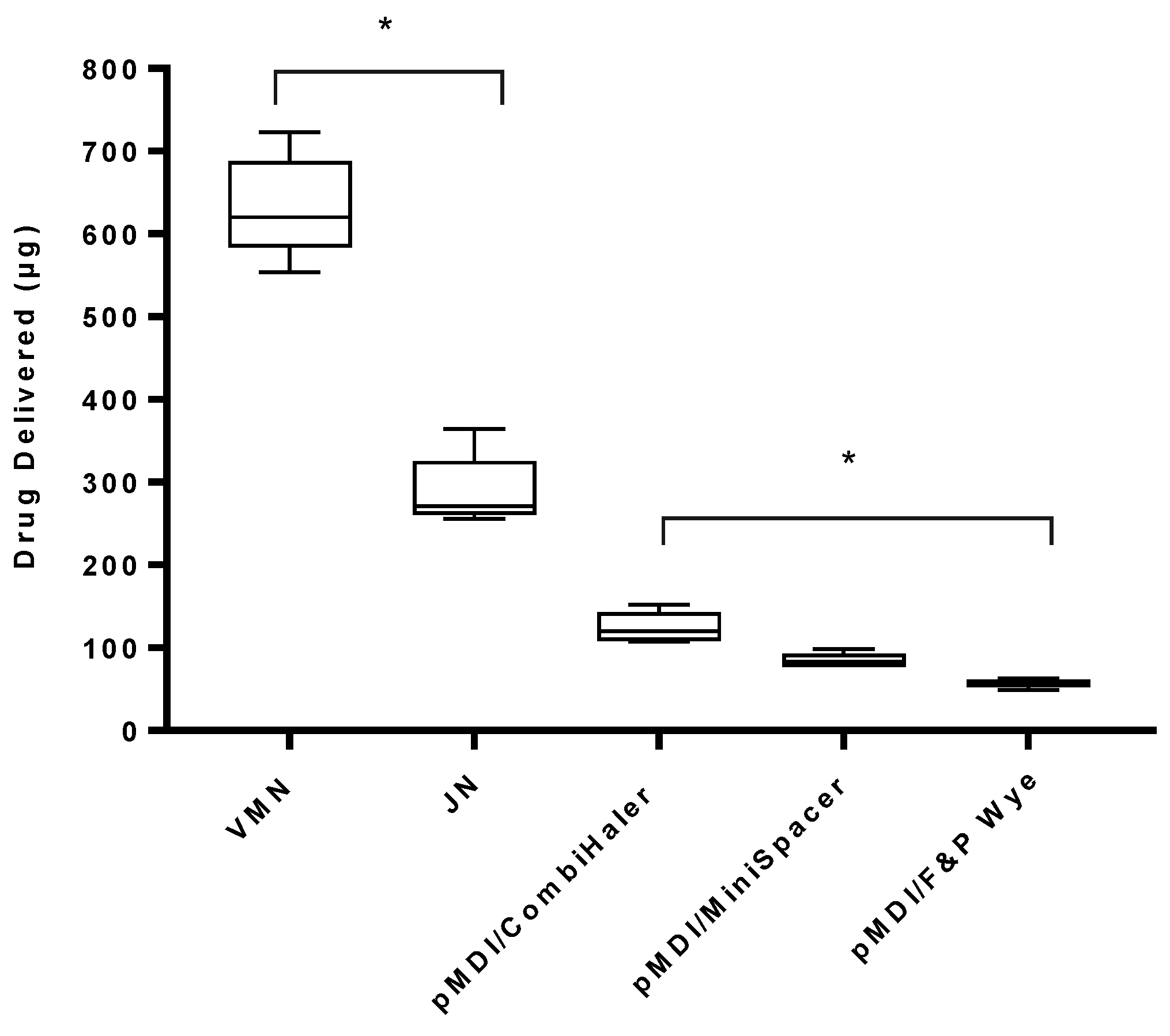
3.3. Aerosol Drug Delivery during Simulated Mechanical Ventilation
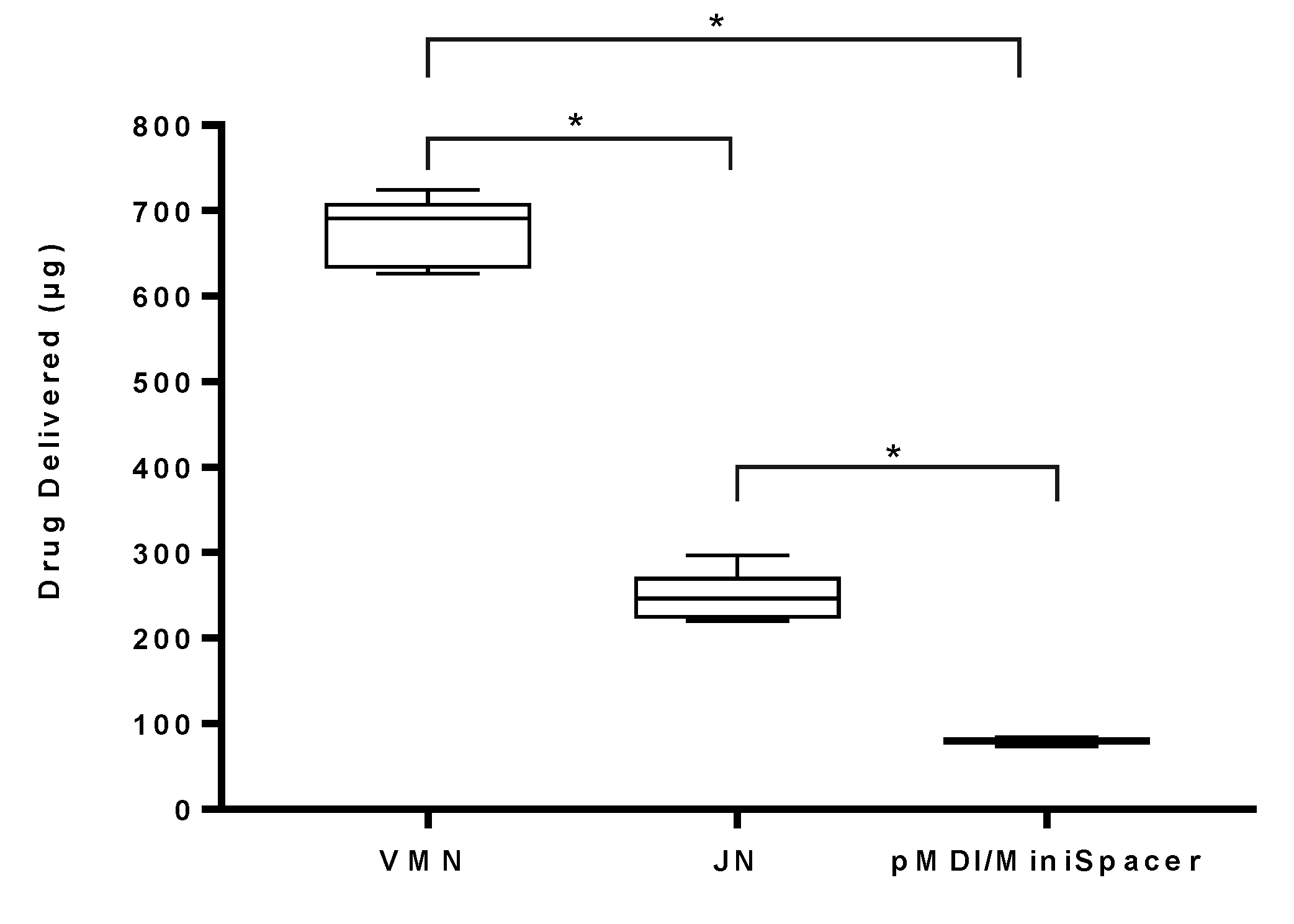
3.3.1. Standard Ventilation
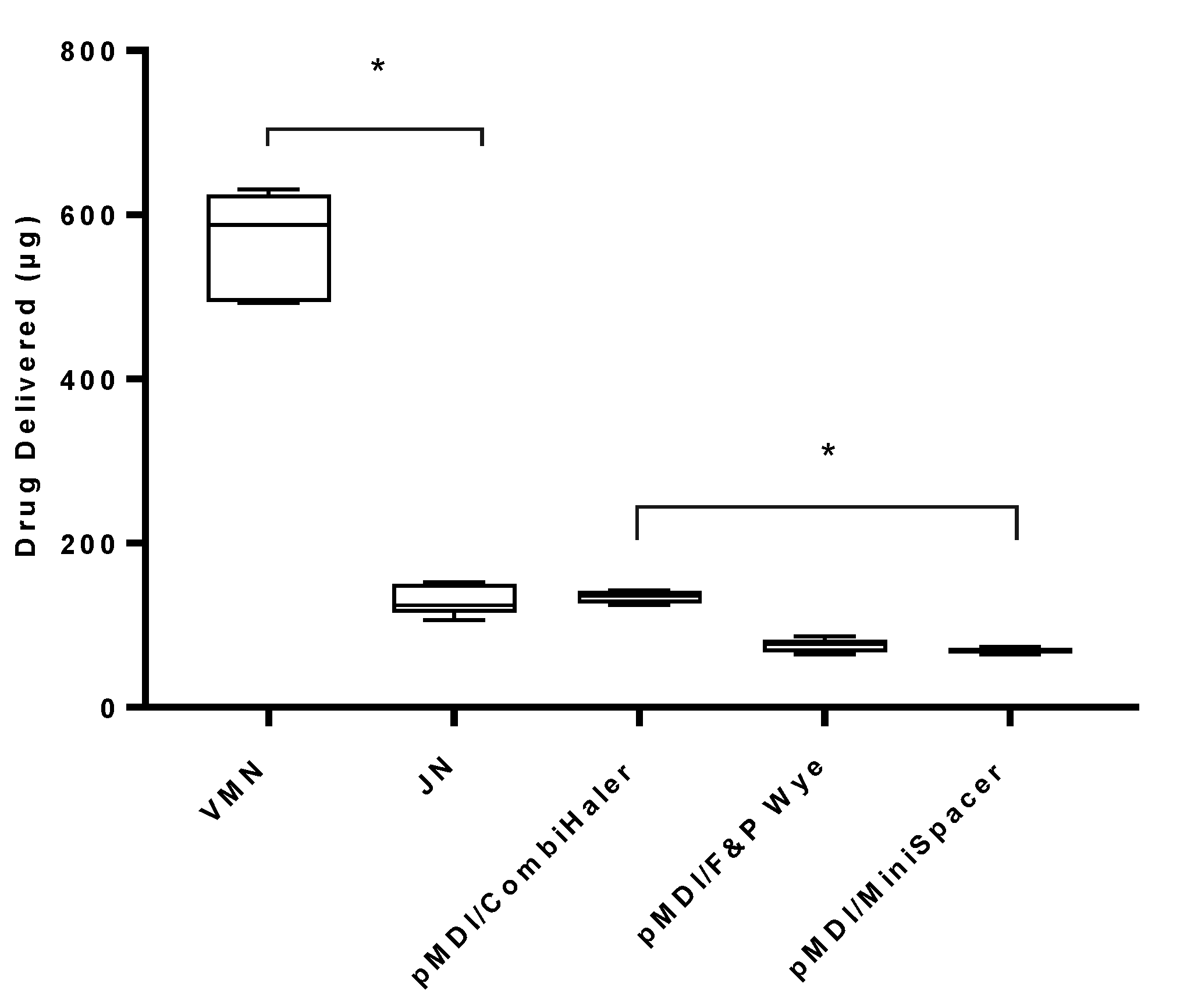
3.3.2. Lung-Protective, Low Tidal Volume (LTV) Ventilation
3.4. Percentage Residual Drug Remaining in the VMN and JN Devices
3.5. Exhaled Drug Determination during Simulated Mechanical Ventilation
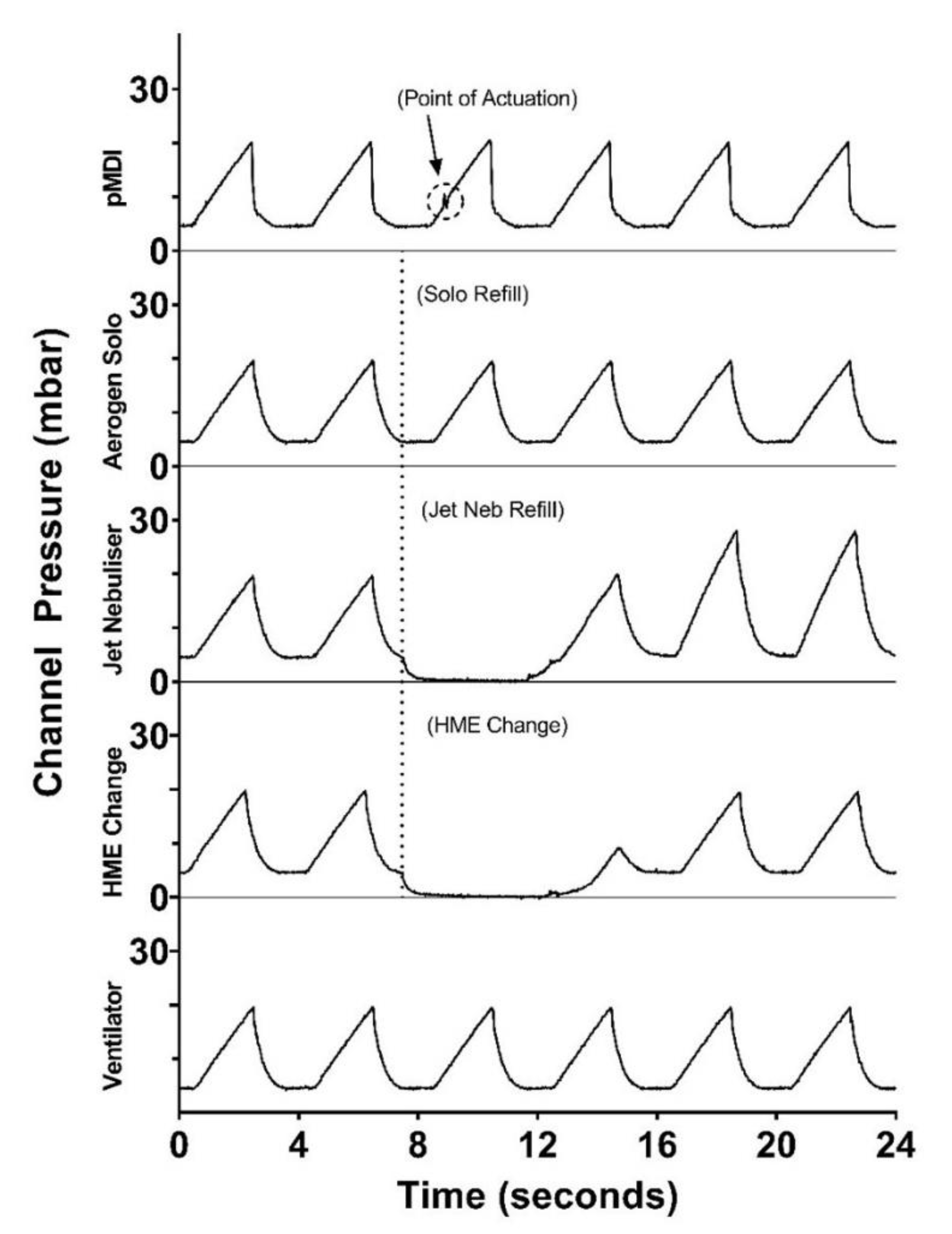
3.6. Effect of Nebuliser Refill/pMDI Actuation Use/HME Change on Circuit Pressure
4. Discussion
4.1. Effect of Device Type on Drug Delivery
4.2. Effect of Ventilator Parameters and Humidification Type on Drug Delivery
4.3. Effect of pMDI Adapter Type on Drug Delivery
4.4. Effect of pMDI Actuation Timing on Drug Delivery
4.5. Effect of Open Circuit
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dhand, R. Basic techniques for aerosol delivery during mechanical ventilation. Respir. Care 2004, 49, 611–622. [Google Scholar]
- Dhand, R. Aerosol Delivery During Mechanical Ventilation: From Basic Techniques to New Devices. J. Aerosol Med. Pulm. Drug Deliv. 2008, 21, 45–60. [Google Scholar] [CrossRef] [Green Version]
- Ehrmann, S.; Roche-Campo, F.; Papa, G.F.S.; Isabey, D.; Brochard, L.; Apiou-Sbirlea, G. Aerosol therapy during mechanical ventilation: An international survey. Intensive Care Med. 2013, 39, 1048–1056. [Google Scholar] [CrossRef]
- Dugernier, J.; Ehrmann, S.; Sottiaux, T.; Roeseler, J.; Wittebole, X.; Dugernier, T.; Jamar, F.; Laterre, P.-F.; Reychler, G. Aerosol delivery during invasive mechanical ventilation: A systematic review. Crit. Care 2017, 21, 264. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.-L.; Fink, J.B.; Ge, H. Aerosol delivery via invasive ventilation: A narrative review. Ann. Transl. Med. 2021, 9, 588. [Google Scholar] [CrossRef]
- Dhand, R. How Should Aerosols Be Delivered During Invasive Mechanical Ventilation? Respir. Care 2017, 62, 1343–1367. [Google Scholar] [CrossRef]
- ADuarte, A.G. Inhaled bronchodilator administration during mechanical ventilation. Respir. Care 2004, 49, 623–634. [Google Scholar]
- Joyce, M.; McGrath, J.; Eain, M.M.G.; O’Sullivan, A.; Byrne, M.; MacLoughlin, R. Nebuliser Type Influences Both Patient-Derived Bioaerosol Emissions and Ventilation Parameters during Mechanical Ventilation. Pharmaceutics 2021, 13, 199. [Google Scholar] [CrossRef]
- Steckel, H.; Eskandar, F. Factors affecting aerosol performance during nebulization with jet and ultrasonic nebulizers. Eur. J. Pharm. Sci. 2003, 19, 443–455. [Google Scholar] [CrossRef]
- Ari, A. Aerosol Therapy in Pulmonary Critical Care. Respir. Care 2015, 60, 858–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhand, R. Inhalation therapy with metered-dose inhalers and dry powder inhalers in mechanically ventilated patients. Respir. Care 2005, 50, 1331. [Google Scholar]
- Ari, A. Aerosol Therapy for Ventilator-Dependent Patients: Devices, Issues, Selection & Technique. Respir. Ther. Fac. Publ. 2012. Available online: https://scholarworks.gsu.edu/rt_facpub/2 (accessed on 25 August 2021).
- Ari, A.; Harwood, R.J.; Sheard, M.M.; Fink, J.B. Pressurized Metered-Dose Inhalers Versus Nebulizers in the Treatment of Mechanically Ventilated Subjects With Artificial Airways: An In Vitro Study. Respir. Care 2015, 60, 1570–1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ari, A.; Atalay, O.T.; Harwood, R.; Sheard, M.M.; Aljamhan, E.A.; Fink, J.B. Influence of nebulizer type, position, and bias flow on aerosol drug delivery in simulated pediatric and adult lung models during mechanical ventilation. Respir. Care 2010, 55, 845–851. [Google Scholar] [PubMed]
- Ari, A.; Areabi, H.; Fink, J.B. Evaluation of aerosol generator devices at 3 locations in humidified and non-humidified circuits during adult mechanical ventilation. Respir. Care 2010, 55, 837–844. [Google Scholar]
- Hatley, R.H.; Parker, J.; Pritchard, J.; Von Hollen, D. Variability in Delivered Dose from Pressurized Metered-Dose Inhaler Formulations Due to a Delay Between Shake and Fire. J. Aerosol Med. Pulm. Drug Deliv. 2017, 30, 71–79. [Google Scholar] [CrossRef]
- Qaqish, R.; Berlinski, A. Effects of Shake-Actuation Delay on Delivered Dose and Aerosol Characteristics of an Albuterol Suspension From a Pressurized Metered-Dose Inhaler. Respir. Care 2021, 66, 1315–1322. [Google Scholar] [CrossRef]
- COVID-19 Clinical Management: Living Guidance. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-1 (accessed on 6 July 2021).
- Fink, J.B.; Ehrmann, S.; Li, J.; Dailey, P.; McKiernan, P.; Darquenne, C.; Martin, A.R.; Rothen-Rutishauser, B.; Kuehl, P.J.; Häussermann, S.; et al. Reducing Aerosol-Related Risk of Transmission in the Era of COVID-19: An Interim Guidance Endorsed by the International Society of Aerosols in Medicine. J. Aerosol Med. Pulm. Drug Deliv. 2020, 33, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.-L.; Fink, J.B.; Tsai, Y.-H.; Wan, G.-H. Managing humidity support in intubated ventilated patients with coronavirus disease 2019 (COVID-19). Infect. Control. Hosp. Epidemiol. 2020, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Eain, M.M.G.; Joyce, M.; MacLoughlin, R. An in vitro visual study of fugitive aerosols released during aerosol therapy to an invasively ventilated simulated patient. Drug Deliv. 2021, 28, 1496–1500. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, C.; McGrath, J.A.; Joyce, M.; Bennett, G.; Byrne, M.A.; MacLoughlin, R. Fugitive Aerosol Therapy Emissions during Mechanical Ventilation: In Vitro Assessment of the Effect of Tidal Volume and Use of Protective Filters. Aerosol Air Qual. Res. 2020, 20, 2604–2613. [Google Scholar] [CrossRef]
- MacLoughlin, R.J.; Higgins, B.D.; Laffey, J.G.; O’Brien, T. Optimized Aerosol Delivery to a Mechanically Ventilated Rodent. J. Aerosol Med. Pulm. Drug Deliv. 2009, 22, 323–332. [Google Scholar] [CrossRef] [Green Version]
- Laube, B.L.; Janssens, H.M.; de Jongh, F.H.C.; Devadason, S.G.; Dhand, R.; Diot, P.; Everard, M.L.; Horvath, I.; Navalesi, P.; Voshaar, T.; et al. What the pulmonary specialist should know about the new inhalation therapies. Eur. Respir. J. 2011, 37, 1308–1417. [Google Scholar] [CrossRef] [Green Version]
- ISO—ISO 27427:2013—Anaesthetic and Respiratory Equipment—Nebulizing Systems and Components. Available online: https://www.iso.org/standard/59482.html (accessed on 27 October 2020).
- Haynes, A.; Shaik, M.S.; Krarup, H.; Singh, M. Evaluation of the Malvern Spraytec® with inhalation cell for the measurement of particle size distribution from metered dose inhalers. J. Pharm. Sci. 2004, 93, 349–363. [Google Scholar] [CrossRef]
- Djedaini, K.; Billiard, M.; Mier, L.; Le Bourdelles, G.; Brun, P.; Markowicz, P.; Estagnasie, P.; Coste, F.; Boussougant, Y.; Dreyfuss, D. Changing heat and moisture exchangers every 48 h rather than 24 h does not affect their efficacy and the incidence of nosocomial pneumonia. Am. J. Respir. Crit. Care Med. 2012, 152, 1562–1569. [Google Scholar] [CrossRef] [PubMed]
- Ari, A.; Fink, J.B. Delivered dose with jet and mesh nebulisers during spontaneous breathing, noninvasive ventilation and mechanical ventilation using adult lung models. ERJ Open Res. 2021, 7, 00027–02021. [Google Scholar] [CrossRef] [PubMed]
- Dunne, R.B.; Shortt, S. Comparison of bronchodilator administration with vibrating mesh nebulizer and standard jet nebulizer in the emergency department. Am. J. Emerg. Med. 2018, 36, 641–646. [Google Scholar] [CrossRef] [Green Version]
- Lengsfeld, C.S.; Filas, B.A. Mass balance of nebulized drug delivery: Residual drug levels and the effects of an alternative air humidification method. At. Sprays 2008, 18, 495–510. [Google Scholar] [CrossRef]
- Diot, P.; Morra, L.; Smaldone, G.C. Albuterol delivery in a model of mechanical ventilation. Comparison of metered-dose inhaler and nebulizer efficiency. Am. J. Respir. Crit. Care Med. 1995, 152, 1391–1394. [Google Scholar] [CrossRef]
- Gay, P.C.; Patel, H.G.; Nelson, S.B.; Gilles, B.; Hubmayr, R.D. Metered Dose Inhalers for Bronchodilator Delivery in Intubated, Mechanically Ventilated Patients. Chest 1991, 99, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med. 2020, 46, 854–887. [Google Scholar] [CrossRef] [Green Version]
- Botta, M.; Tsonas, A.M.; Pillay, J.; Boers, L.S.; Algera, A.G.; Bos, L.D.J.; Dongelmans, D.A.; Hollmann, M.W.; Horn, J.; Vlaar, A.P.J.; et al. Ventilation management and clinical outcomes in invasively ventilated patients with COVID-19 (PRoVENT-COVID): A national, multicentre, observational cohort study. Lancet Respir. Med. 2021, 9, 139–148. [Google Scholar] [CrossRef]
- Ari, A.; Dang, T.; Al Enazi, F.H.; Alqahtani, M.M.; Alkhathami, A.; Qoutah, R.; Almamary, A.S.; Fink, J.B. Effect of Heat Moisture Exchanger on Aerosol Drug Delivery and Airway Resistance in Simulated Ventilator-Dependent Adults Using Jet and Mesh Nebulizers. J. Aerosol Med. Pulm. Drug Deliv. 2018, 31, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Sonny, W.; Ii, B. Effects of Heat and Moisture Exchangers Designed to Allow Aerosol Delivery on Airflow Resistance and Aerosol Deposition. 2010. Available online: https://scholarworks.gsu.edu/rt_theseshttps://scholarworks.gsu.edu/rt_theses/11 (accessed on 23 July 2021).
- CombiHaler Spacer Specifications—Déposition Pulmonaire des Médicaments. Available online: https://optimhal.com/en/combihaler-spacer/combihaler-spacer-specifications/ (accessed on 7 July 2021).
- Boukhettala, N.; Poree, T.; Diot, P.; Vecellio, L. In Vitro Performance of Spacers for Aerosol Delivery during Adult Mechanical Ventilation. J. Aerosol Med. Pulm. Drug Deliv. 2015, 28, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Eckes, M.; Paris, A.; Hervieu, B.; Vanlaeys, A.; Housseini, K.; Porée, T. In vitro aerosol delivery by vibrating mesh nebulizer (VMN) and pressurized metered dose inhaler (pMDI) using spacers in comparison with T adapters in mechanical ventilation. Paediatr. Qual. Life 2020, 6, 47. [Google Scholar] [CrossRef]
- Crosland, B.M.; Johnson, M.R.; Matida, E.A. Characterization of the Spray Velocities from a Pressurized Metered-Dose Inhaler. J. Aeros. Med. Pulm. Drug Deliv. 2009, 22, 85–98. [Google Scholar] [CrossRef]
- Clark, A.R. MDIs: Physics of Aerosol Formation. J. Aerosol Med. 1996, 9, S19. [Google Scholar] [CrossRef] [PubMed]
- Wilkes, W.; Fink, J.; Dhand, R. Selecting an Accessory Device with a Metered-Dose Inhaler: Variable Influence of Accessory Devices on Fine Particle Dose, Throat Deposition, and Drug Delivery with Asynchronous Actuation from a Metered-Dose Inhaler. J. Aerosol Med. 2001, 14, 351–360. [Google Scholar] [CrossRef]
- Fink, J.B.; Rubin, B.K. Problems with inhaler use: A call for improved clinician and patient education. Respir. Care 2005, 50, 1360. [Google Scholar]
- Ari, A.; Alwadeai, K.S.; Fink, J.B. Effects of Heat and Moisture Exchangers and Exhaled Humidity on Aerosol Deposition in a Simulated Ventilator-Dependent Adult Lung Model. Respir. Care 2017, 62, 538–543. [Google Scholar] [CrossRef] [Green Version]
- Gómez, C.C.; Rodríguez, Ó.P.; Torné, M.L.; Santaolalla, C.E.; Jiménez, J.F.M.; Fernández, J.G.; Perales, J.M.C.; Heili-Frades, S.B.; Monreal, M.F.; Nilsson, J.M.D.A.; et al. Clinical consensus recommendations regarding non-invasive respiratory support in the adult patient with acute respiratory failure secondary to SARS-CoV-2 infection. Med. Intensiv. 2020, 44, 429–438. [Google Scholar] [CrossRef]
- Alpin, D.M.G.; Criner, G.J.; Papi, A.; Singh, D.; Anzueto, A.; Martinez, F.J.; Agusti, A.A.; Vogelmeier, C.F. Global Initiative for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease. The 2020 GOLD Science Committee Report on COVID-19 and Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2021, 203, 24–36. [Google Scholar] [CrossRef] [PubMed]
- Respiratory Care Committee of Chinese Thoracic Society. Expert consensus on preventing nosocomial transmission during respiratory care for critically ill patients infected by 2019 novel coronavirus pneumonia. Zhonghua Jie He He Hu Xi Za Zhi 2020, 43, 288–296. [Google Scholar] [CrossRef]
- Sweeney, L.; McCloskey, A.P.; Higgins, G.; Ramsey, J.M.; Cryan, S.A.; MacLoughlin, R. Effective nebulization of interferon-γ using a novel vibrating mesh. Respir. Res. 2019, 20, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fink, J.; Dunne, P.; MacLoughlin, R.; O’Sullivan, G. Can high efficiency aerosol delivery continue after extubation? Crit. Care 2005, 9, P129. [Google Scholar] [CrossRef]
- Lide, D.R.; Ph, D. Aerosol Generation. 2016. Available online: https://www.fda.gov/downloads/ (accessed on 26 August 2021).
- MacLoughlin, R.; Telfer, C.; Clark, A.; Fink, J. Aerosol: A Novel Vehicle for Pharmacotherapy in Neonates. Curr. Pharm. Des. 2018, 23, 5928–5934. [Google Scholar] [CrossRef]
- Brennan, L.C.; O’Sullivan, A.; MacLoughlin, R. Cellular Therapy for the Treatment of Paediatric Respiratory Disease. Int. J. Mol. Sci. 2021, 22, 8906. [Google Scholar] [CrossRef]
- Brave, H.; MacLoughlin, R. State of the Art Review of Cell Therapy in the Treatment of Lung Disease, and the Potential for Aerosol Delivery. Int. J. Mol. Sci. 2020, 21, 6435. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, S.D.; Horgan, E.; Ali, A.; Masterson, C.; Laffey, J.G.; MacLoughlin, R.; O’Toole, D. Nebulized Mesenchymal Stem Cell Derived Conditioned Medium Retains Antibacterial Properties Against Clinical Pathogen Isolates. J. Aerosol. Med. Pulm. Drug Deliv. 2020, 33, 140–152. [Google Scholar] [CrossRef]
- Van Haren, F.M.P.; Page, C.; Laffey, J.G.; Artigas, A.; Camprubi-Rimblas, M.; Nunes, Q.; Smith, R.; Shute, J.; Carroll, M.; Tree, J.; et al. Nebulised heparin as a treatment for COVID-19: Scientific rationale and a call for randomised evidence. Crit. Care 2020, 24, 1–11. [Google Scholar] [CrossRef]
- Daly, S.; O’Sullivan, A.; MacLoughlin, R. Cellular Immunotherapy and the Lung. Vaccines 2021, 9, 1018. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device Type | VMD (µm) | Flow Rate (mL/min) | FPF <5 µm (%) | FPF <3 µm (%) | FPF <2 µm (%) |
|---|---|---|---|---|---|
| VMN | 4.82 ± 0.06 | 0.56 ± 0.00 | 48.03 ± 0.69 | 27.60 ± 0.64 | 15.33 ± 0.64 |
| JN | 3.42 ± 0.02 | 0.27 ± 0.00 | 72.20 ± 0.27 | 42.53 ± 0.23 | 22.89 ± 0.03 |
| pMDI | 1.61 ± 0.18 a | N/A | 94.70 ± 0.34 a | N/A | N/A |
| Device Type | Ventilation Type | Circuit Position | Humidification Type | Drug Delivery (µg) Mean ± SD | Drug Delivery (%) Mean ± SD |
|---|---|---|---|---|---|
| VMN | STD | Dry side | ACTIVE | 632.92 ± 61.95 | 25.32 ± 2.48 |
| Between HME and ETT | PASSIVE | 674.77 ± 41.19 | 26.99 ± 1.99 | ||
| LTV | Dry side | ACTIVE | 565.23 ± 66.36 | 22.61 ± 2.65 | |
| JN | STD | Inspiratory limb | ACTIVE | 288.60 ± 43.90 | 11.54 ± 1.76 |
| Between HME and ETT | PASSIVE | 247.08 ± 30.24 | 9.88 ± 1.21 | ||
| LTV | Inspiratory limb | ACTIVE | 131.08 ± 18.92 | 5.24 ± 0.76 | |
| pMDI/CombiHaler | STD | Inspiratory limb | ACTIVE | 124.62 ± 18.68 | 31.15 ± 4.67 |
| pMDI/MiniSpacer | 84.62 ± 8.97 | 21.15 ± 2.24 | |||
| pMDI/F&P Wye | At the wye | 56.92 ± 5.22 | 14.23 ± 1.30 | ||
| pMDI/MiniSpacer | Between HME and ETT | PASSIVE | 80.00 ± 4.49 | 20.00 ± 1.12 | |
| pMDI/CombiHaler | LTV | Inspiratory limb | ACTIVE | 134.46 ± 7.58 | 33.62 ± 1.90 |
| pMDI/MiniSpacer | 68.92 ± 3.67 | 17.23 ± 0.92 | |||
| pMDI/F&P Wye | 75.38 ± 8.14 | 18.85 ± 2.04 |
| Device Type | Humidification Type | Ventilation Type | Mean ± SD (% Residual Drug) | p-Value |
|---|---|---|---|---|
| VMN | ACTIVE | STD | 0.05 ± 0.08 | 0.5447 |
| PASSIVE | 0.02 ± 0.03 | |||
| ACTIVE | LTV | 0.01 ± 0.03 | 0.3589 | |
| JN | ACTIVE | STD | 57.12 ± 3.83 | 0.0741 |
| PASSIVE | 63.46 ± 5.75 | |||
| ACTIVE | LTV | 56.15 ± 12.20 | 0.8695 | |
| CombiHaler | ACTIVE | STD | 56.46 ± 9.38 | 0.1333 |
| LTV | 65.38 ± 7.40 | |||
| F&P Wye | ACTIVE | STD | 64.46 ± 6.08 | 0.6585 |
| LTV | 63.00 ± 3.70 | |||
| MiniSpacer | ACTIVE | STD | 29.38 ± 2.35 | <0.0001 |
| PASSIVE | 18.46 ± 1.28 | |||
| ACTIVE | LTV | 17.23 ± 5.93 | 0.0028 |
| Device Type | Ventilation Type | Expiratory Filter Mean ± SD (µg Drug) | Expiratory Filter Mean ± SD (% Exhaled Drug) |
|---|---|---|---|
| VMN | STD | 211.40 ± 35.90 | 8.46 ± 1.43 |
| LTV | 162.80 ± 28.40 | 6.51 ± 1.14 | |
| JN | STD | 273.20 ± 39.50 | 10.93 ± 1.58 |
| LTV | 400.30 ± 36.30 | 16.01 ± 1.45 | |
| pMDI/CombiHaler | STD | 33.54 ± 4.27 | 8.38 ± 1.07 |
| LTV | 58.15 ± 6.10 | 14.54 ± 1.52 | |
| pMDI/MiniSpacer | STD | 36.00 ± 7.43 | 9.00 ± 1.86 |
| LTV | 37.54 ± 4.56 | 9.38 ± 1.14 | |
| pMDI/F&P Wye | STD | 29.54 ± 7.49 | 7.38 ± 1.87 |
| LTV | 48.92 ± 4.54 | 12.23 ± 1.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naughton, P.J.; Joyce, M.; Mac Giolla Eain, M.; O’Sullivan, A.; MacLoughlin, R. Evaluation of Aerosol Drug Delivery Options during Adult Mechanical Ventilation in the COVID-19 Era. Pharmaceutics 2021, 13, 1574. https://doi.org/10.3390/pharmaceutics13101574
Naughton PJ, Joyce M, Mac Giolla Eain M, O’Sullivan A, MacLoughlin R. Evaluation of Aerosol Drug Delivery Options during Adult Mechanical Ventilation in the COVID-19 Era. Pharmaceutics. 2021; 13(10):1574. https://doi.org/10.3390/pharmaceutics13101574
Chicago/Turabian StyleNaughton, Piers J., Mary Joyce, Marc Mac Giolla Eain, Andrew O’Sullivan, and Ronan MacLoughlin. 2021. "Evaluation of Aerosol Drug Delivery Options during Adult Mechanical Ventilation in the COVID-19 Era" Pharmaceutics 13, no. 10: 1574. https://doi.org/10.3390/pharmaceutics13101574