

Immunogenicity of Two Doses of BNT162b2 mRNA COVID-19 Vaccine with a ChAdOx1-S Booster Dose among Navy Personnel in Mexico
 and
and
Abstract
:1. Introduction
2. Materials and Methods
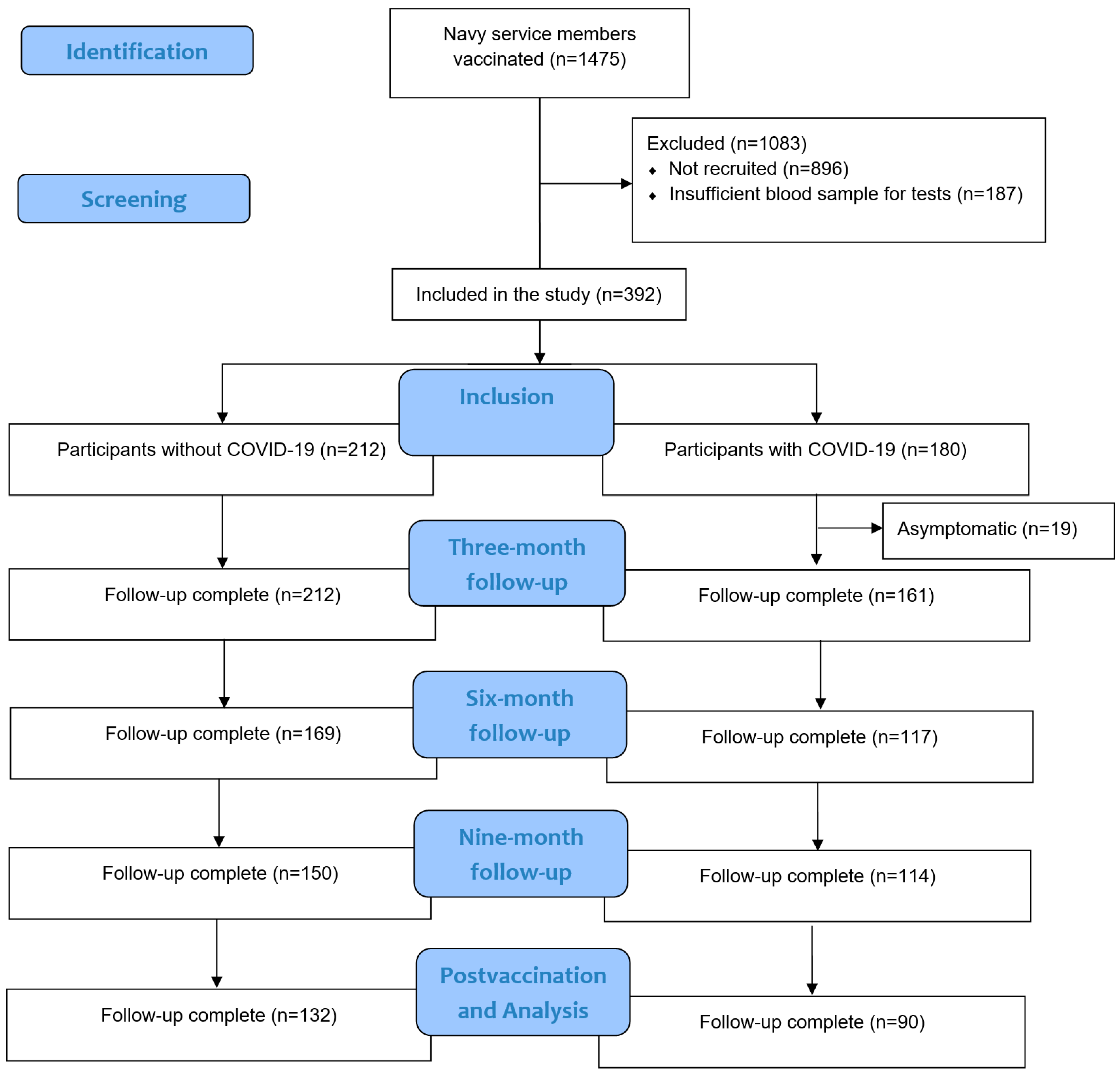
2.1. Study Design and Study Population
2.2. Vaccination Schedule and Vaccine Administration
2.3. Data Collection
2.4. Blood Collection
2.5. Serological Testing
2.5.1. IgG Nucleocapsid
2.5.2. IgG S1/S2 Spike Protein
2.6. SARS-CoV-2 Detection for Real-Time Reverse Transcriptase-Polymerase Chain Reaction (RT-PCR)
2.7. Statistical Analysis
3. Results
3.1. Description of the Study Population
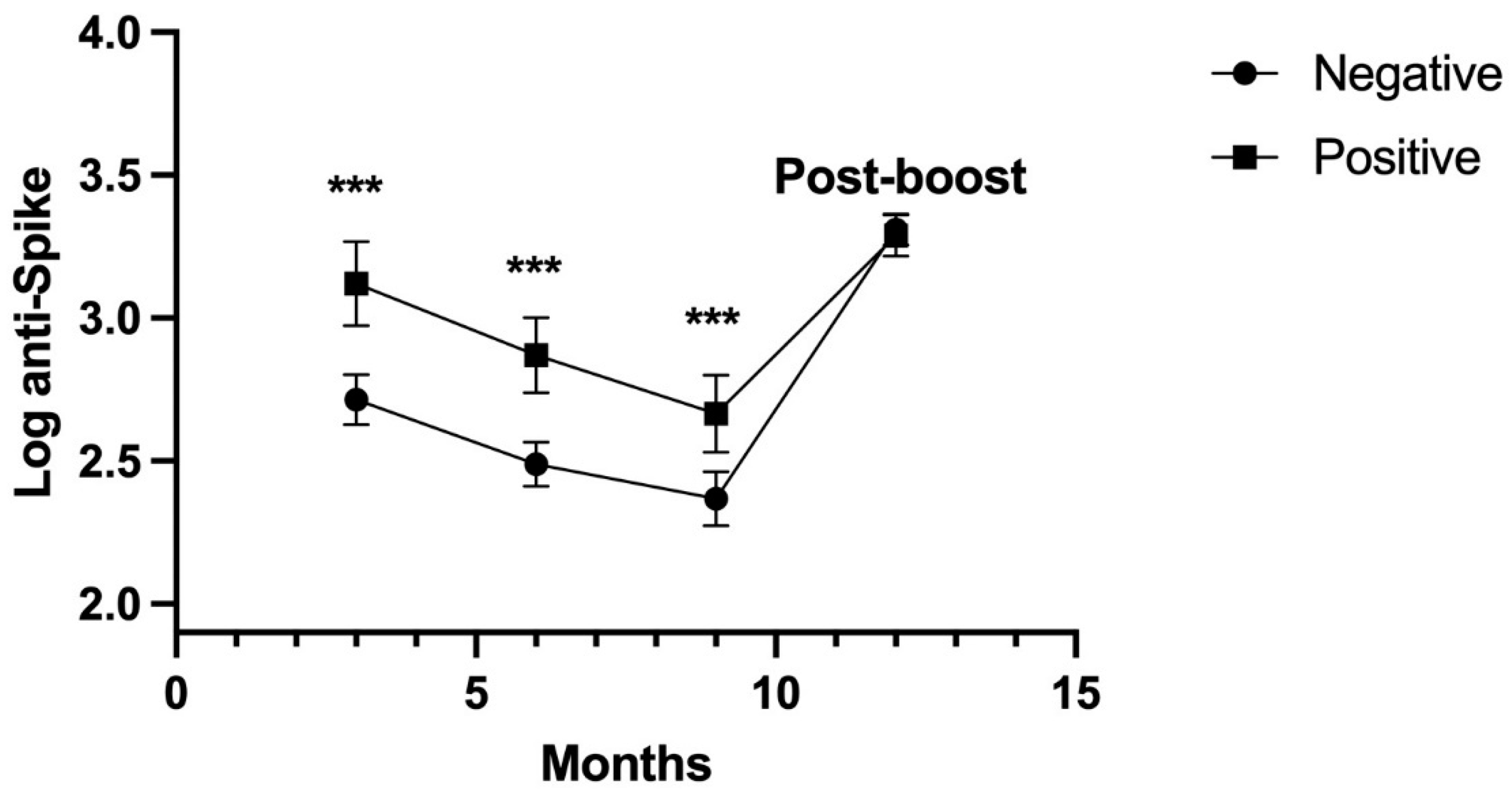
3.2. Antibodies of SARS-CoV-2 Anti-N and Anti-S
3.3. Asymptomatic
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 MRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Frenck, R.W.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Study to Describe the Safety, Tolerability, Immunogenicity, and Efficacy of RNA Vaccine Candidates Against COVID-19 in Healthy Individuals. Available online: https://clinicaltrials.gov/study/NCT04368728 (accessed on 27 February 2024).
- Kiyuka, P.K.; Agoti, C.N.; Munywoki, P.K.; Njeru, R.; Bett, A.; Otieno, J.R.; Otieno, G.P.; Kamau, E.; Clark, T.G.; van der Hoek, L.; et al. Human Coronavirus NL63 Molecular Epidemiology and Evolutionary Patterns in Rural Coastal Kenya. J. Infect. Dis. 2018, 217, 1728–1739. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M.; Vegvari, C.; Truscott, J.; Collyer, B.S. Challenges in Creating Herd Immunity to SARS-CoV-2 Infection by Mass Vaccination. Lancet 2020, 396, 1614–1616. [Google Scholar] [CrossRef]
- Wajnberg, A.; Amanat, F.; Firpo, A.; Altman, D.R.; Bailey, M.J.; Mansour, M.; McMahon, M.; Meade, P.; Mendu, D.R.; Muellers, K.; et al. Robust Neutralizing Antibodies to SARS-CoV-2 Infection Persist for Months. Science 2020, 370, 1227–1230. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.Y.; Kang, D.Y.; Kim, E.; Lee, S.; Baek, J.H.; Lee, J.-S.; Park, M.Y.; Im, J.H. Adverse Events of a Third Dose of BNT162b2 MRNA COVID-19 Vaccine among Korean Healthcare Workers. Medicine 2023, 102, e33236. [Google Scholar] [CrossRef] [PubMed]
- Link-Gelles, R.; Levy, M.E.; Natarajan, K.; Reese, S.E.; Naleway, A.L.; Grannis, S.J.; Klein, N.P.; DeSilva, M.B.; Ong, T.C.; Gaglani, M.; et al. Estimation of COVID-19 MRNA Vaccine Effectiveness and COVID-19 Illness and Severity by Vaccination Status During Omicron BA.4 and BA.5 Sublineage Periods. JAMA Netw. Open 2023, 6, e232598. [Google Scholar] [CrossRef]
- Eick-Cost, A.; Ying, S.; Wells, N. Effectiveness of mRNA-1273, BNT162b2, and JNJ-78436735 COVID-19 Vaccines among US Military Personnel before and during the Predominance of the Delta Variant. JAMA Net. Open 2022, 5, e228071. [Google Scholar] [CrossRef]
- Mallah, S.I.; Alawadhi, A.; Jawad, J.; Wasif, P.; Alsaffar, B.; Alalawi, E.; Mohamed, A.M.; Butler, A.E.; Alalawi, B.; Qayed, D.; et al. Safety and Efficacy of COVID-19 Prime-Boost Vaccinations: Homologous BBIBP-CorV versus Heterologous BNT162b2 Boosters in BBIBP-CorV-Primed Individuals. Vaccine 2023, 41, 1925–1933. [Google Scholar] [CrossRef]
- Hulme, W.J.; Horne, E.M.F.; Parker, E.P.K.; Keogh, R.H.; Williamson, E.J.; Walker, V.; Palmer, T.M.; Curtis, H.J.; Walker, A.J.; Andrews, C.D.; et al. Comparative Effectiveness of BNT162b2 versus MRNA-1273 COVID-19 Vaccine Boosting in England: Matched Cohort Study in OpenSAFELY-TPP. BMJ 2023, 380, e072808. [Google Scholar] [CrossRef]
- Sim, W.; Kang, H.; Jung, J.; Lee, J.; Ko, G.Y.; Park, H.-S.; Choi, J.; Park, K.; Oh, E.-J. Comparison of Humoral and Cellular Immune Responses between ChAd-BNT Heterologous Vaccination and BNT-BNT Homologous Vaccination Following the Third BNT Dose: A Prospective Cohort Study. Front. Immunol. 2023, 14, 1120556. [Google Scholar] [CrossRef]
- Sudjaritruk, T.; Mueangmo, O.; Saheng, J.; Winichakoon, P.; Salee, P.; Wongjak, W.; Chaito, T.; Praparattanapan, J.; Nuket, K.; Solai, N.; et al. Comparison of Immunogenicity and Reactogenicity of Five Primary Series of COVID-19 Vaccine Regimens against Circulating SARS-CoV-2 Variants of Concern among Healthy Thai Populations. Vaccines 2023, 11, 564. [Google Scholar] [CrossRef]
- Epsi, N.J.; Richard, S.A.; Lindholm, D.A.; Mende, K.; Ganesan, A.; Huprikar, N.; Lalani, T.; Fries, A.C.; Maves, R.C.; Colombo, R.E.; et al. Understanding “Hybrid Immunity”: Comparison and Predictors of Humoral Immune Responses to Severe Acute Respiratory Syndrome Coronavirus 2 Infection (SARS-CoV-2) and Coronavirus Disease 2019 (COVID-19) Vaccines. Clin. Infect. Dis. 2023, 76, e439–e449. [Google Scholar] [CrossRef] [PubMed]
- Vargas-De-León, C.; Cureño-Díaz, M.A.; Salazar, M.I.; Cruz-Cruz, C.; Loyola-Cruz, M.Á.; Durán-Manuel, E.M.; Zamora-Pacheco, E.R.; Bravata-Alcántara, J.C.; Lugo-Zamudio, G.E.; Fernández-Sánchez, V.; et al. Neutralizing Antibodies against SARS-CoV-2: Importance of Comorbidities in Health Personnel against Reinfections. Viruses 2023, 15, 2354. [Google Scholar] [CrossRef]
- Flisiak, R.; Pawłowska, M.; Rogalska-Płońska, M.; Bociąga-Jasik, M.; Kłos, K.; Piekarska, A.; Zarębska-Michaluk, D. Effect of COVID-19 on Anti-S Antibody Response in Healthcare Workers Six Months Post-Vaccination. Vaccines 2021, 9, 1325. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, F.; Buonfrate, D.; Moro, L.; Rodari, P.; Piubelli, C.; Caldrer, S.; Riccetti, S.; Sinigaglia, A.; Barzon, L. Antibody Response to the BNT162b2 mRNA COVID-19 Vaccine in Subjects with Prior SARS-CoV-2 Infection. Viruses 2021, 13, 422. [Google Scholar] [CrossRef] [PubMed]
- Bongiovanni, M.; Liuzzi, G.; Schiavon, L.; Gianturco, L.; Giuliani, G. Evaluation of the Immune Response to COVID-19 Vaccine MRNA BNT162b2 and Correlation with Previous COVID-19 Infection. J. Clin. Virol. 2021, 143, 104962. [Google Scholar] [CrossRef]
- Chiu, N.-C.; Chi, H.; Tu, Y.-K.; Huang, Y.-N.; Tai, Y.-L.; Weng, S.-L.; Chang, L.; Huang, D.T.-N.; Huang, F.-Y.; Lin, C.-Y. To Mix or Not to Mix? A Rapid Systematic Review of Heterologous Prime–Boost COVID-19 Vaccination. Expert Rev. Vaccines 2021, 20, 1211–1220. [Google Scholar] [CrossRef]
- Liu, X.; Shaw, R.H.; Stuart, A.S.V.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Safety and Immunogenicity of Heterologous versus Homologous Prime-Boost Schedules with an Adenoviral Vectored and MRNA COVID-19 Vaccine (Com-COV): A Single-Blind, Randomised, Non-Inferiority Trial. Lancet 2021, 398, 856–869. [Google Scholar] [CrossRef]
- Batmunkh, T.; Moore, K.A.; Thomson, H.; Altangerel, B.; Amraa, O.; Avaa, N.; Batbayar, L.; Batsukh, K.; Bright, K.; Burentogtokh, T.; et al. Immunogenicity, Safety, and Reactogenicity of a Half- versus Full-Dose BNT162b2 (Pfizer-BioNTech) Booster Following a Two-Dose ChAdOx1 NCoV-19, BBIBP-CorV, or Gam-COVID-Vac Priming Schedule in Mongolia: A Randomised, Controlled, Non-Inferiority Trial. Lancet Reg. Health West. Pac. 2024, 42, 100953. [Google Scholar] [CrossRef]
- Munro, A.P.S.; Feng, S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; et al. Safety, Immunogenicity, and Reactogenicity of BNT162b2 and MRNA-1273 COVID-19 Vaccines given as Fourth-Dose Boosters Following Two Doses of ChAdOx1 NCoV-19 or BNT162b2 and a Third Dose of BNT162b2 (COV-BOOST): A Multicentre, Blinded, Phase 2, Randomised Trial. Lancet Infect. Dis. 2022, 22, 1131–1141. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| COVID-19 | |||
|---|---|---|---|
| Clinical Characteristics | Present (n = 161) | Absent (n = 212) | p-Value |
| Age (Years) * | 35.7 (8.18) | 37.4 (8.50) | 0.053 |
| Sex (Male) ** | 80 (49.7%) | 111 (52.4%) | 0.610 |
| Obesity ** | 23 (14.3%) | 14 (6.60%) | 0.022 |
| Diabetes ** | 0 (0.0%) | 2 (0.9%) | 0.603 *** |
| Hypertension ** | 4 (2.5%) | 5 (2.4%) | 0.937 *** |
| Allergy ** | 1 (0.6%) | 3 (1.4%) | 0.818 *** |
| Alcoholism ** | 0.446 | ||
| Never | 28 (17.6%) | 29 (14.0%) | |
| Occasionally | 129 (81.1%) | 177 (85.5%) | |
| Three times per week | 2 (1.3%) | 1 (0.5%) | |
| Smoking ** | 0.702 | ||
| Never | 107 (67.3%) | 139 (67.5%) | |
| Occasionally | 48 (30.2%) | 62 (30.2%) | |
| 1–5 cigarettes a day | 3 (1.9%) | 5 (2.4%) | |
| 6–15 cigarettes a day | 1 (0.6%) | 0 (0.0%) | |
| COVID-19 | 3 Months M (SD) | p-Value * | 6 Months M (SD) | p-Value * | 9 Months * M (SD) | p-Value * | |
|---|---|---|---|---|---|---|---|
| log (anti-Nucleocapsid) | Present | −0.350 (0.749) | <0.001 | −0.526 (0.714) | <0.001 | −0.668 (0.702) | <0.001 |
| Absent | −1.195 (0.594) | −1.214 (0.532) | −1.129 (0.552) | ||||
| log (anti-Spike) | Present | 3.073 (0.508) | <0.001 | 2.848 (0.454) | <0.001 | 2.630 (0.466) | <0.001 |
| Absent | 2.696 (0.392) | 2.475 (0.344) | 2.349 (0.422) |
| Time | COVID-19 | Interaction | |||||||
|---|---|---|---|---|---|---|---|---|---|
| F | df | p-Value | F | df | p-Value | F | df | p-Value | |
| log(anti-nucleocapsid) * | 6.98 | 1.862 | 0.001 | 75.374 | 1 | <0.001 | 14.87 | 1.86 | <0.001 |
| log(anti-Spike) * | 164.96 | 2.527 | <0.001 | 33.01 | 1 | <0.001 | 11.88 | 2.527 | <0.001 |
| COVID-19 | 3 Months M (SD) | p-Value * | 6 Months * M (SD) | p-Value * | 9 Months * M (SD) | p-Value * | |
|---|---|---|---|---|---|---|---|
| log (anti-Nucleocapsid) | Present | n = 161 | <0.001 | n = 117 | <0.001 | n = 114 | <0.001 |
| −0.338 (0.734) | −0.509 (0.714) | −0.615 (0.698) | |||||
| Absent | n = 212 | n = 169 | n = 150 | ||||
| −1.196 (0.568) | −1.188 (0.558) | −1.103 (0.580) | |||||
| log (anti-Spike) | Present | n = 161 | <0.001 | n = 117 | <0.001 | n = 114 | <0.001 |
| 3.000 (0.525) | 2.804 (0.434) | 2.643 (0.453) | |||||
| Absent | n = 212 | n = 169 | n = 150 | ||||
| 2.644 (0.379) | 2.453 (0.333) | 2.343 (0.411) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ventura-Enríquez, Y.; Cortina-De la Rosa, E.; Díaz-Padilla, E.; Murrieta, S.; Segundo-Martínez, S.; Fernández-Sánchez, V.; Vargas-De-León, C. Immunogenicity of Two Doses of BNT162b2 mRNA COVID-19 Vaccine with a ChAdOx1-S Booster Dose among Navy Personnel in Mexico. Viruses 2024, 16, 551. https://doi.org/10.3390/v16040551
Ventura-Enríquez Y, Cortina-De la Rosa E, Díaz-Padilla E, Murrieta S, Segundo-Martínez S, Fernández-Sánchez V, Vargas-De-León C. Immunogenicity of Two Doses of BNT162b2 mRNA COVID-19 Vaccine with a ChAdOx1-S Booster Dose among Navy Personnel in Mexico. Viruses. 2024; 16(4):551. https://doi.org/10.3390/v16040551
Chicago/Turabian StyleVentura-Enríquez, Yanet, Evelyn Cortina-De la Rosa, Elizabeth Díaz-Padilla, Sandra Murrieta, Silvia Segundo-Martínez, Verónica Fernández-Sánchez, and Cruz Vargas-De-León. 2024. "Immunogenicity of Two Doses of BNT162b2 mRNA COVID-19 Vaccine with a ChAdOx1-S Booster Dose among Navy Personnel in Mexico" Viruses 16, no. 4: 551. https://doi.org/10.3390/v16040551