

Initial Efficacy of the COVID-19 mRNA Vaccine Booster and Subsequent Breakthrough Omicron Variant Infection in Patients with B-Cell Non-Hodgkin’s Lymphoma: A Single-Center Cohort Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Patients
2.3. Statistical Analysis
3. Results
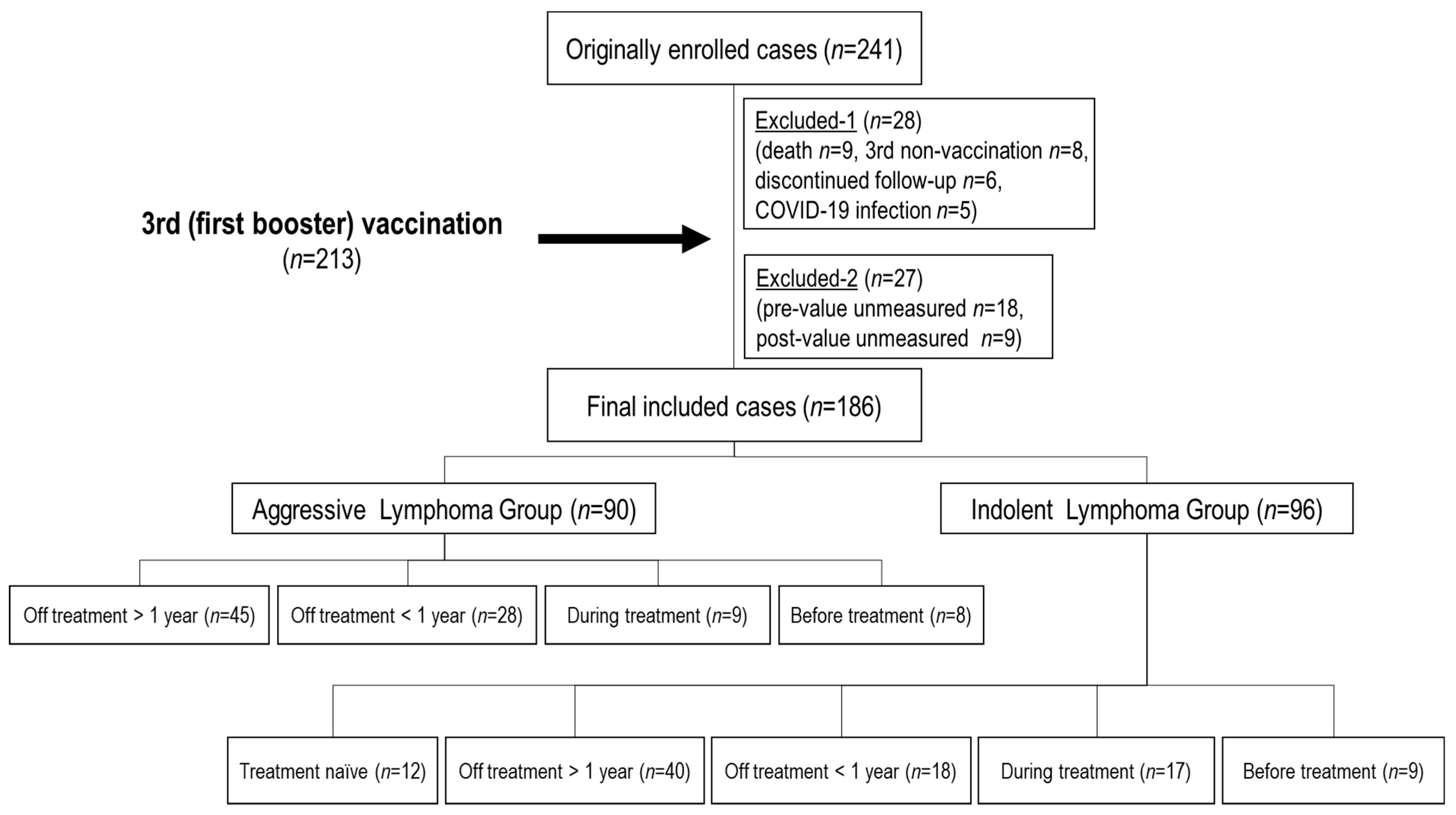
3.1. Study Population
3.2. Clinical Characteristics of Each Disease Group
3.3. Booster Effects after the Third Vaccination (Table 3)
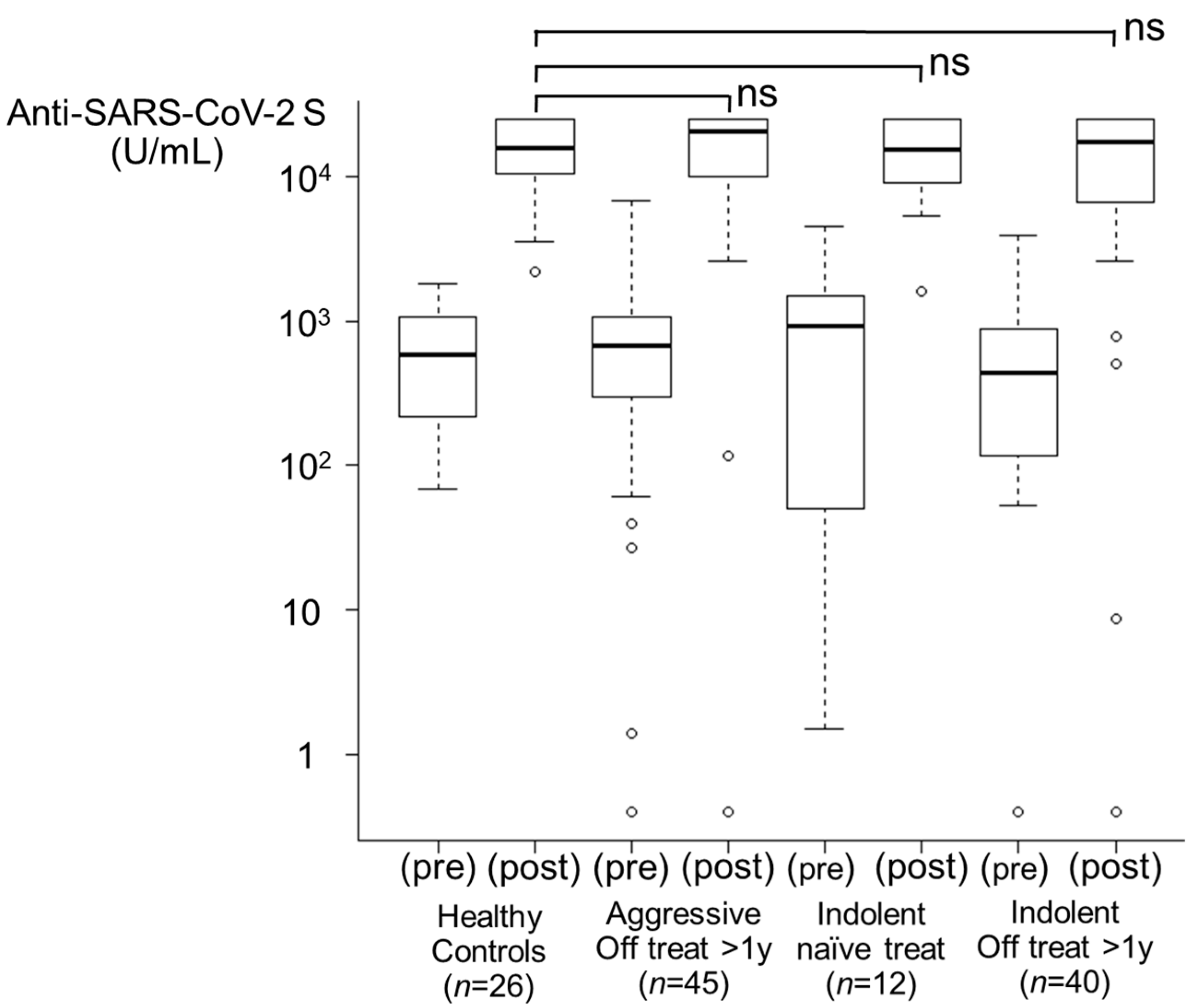
3.3.1. Healthy Control Group and Treatment-Naïve Group (Figure 2)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Histological Subtype | Aggressive Lymphoma | Indolent Lymphoma | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Treatment Status | HCs | Off >1 year | Off <1 year | During | Before | Naïve | Off >1 year | Off <1 year | During | Before |
| Number | 26 | 45 | 28 | 9 | 8 | 12 | 40 | 18 | 17 | 9 |
| Sex (M/F) | M10/F16 | M24/F21 | M16/F12 | M3/F6 | M4/F4 | M9/F3 | M22/F18 | M10/F8 | M11/F6 | M4/F5 |
| Age | 55 | 69 | 72.5 | 74 | 77 | 68 | 68.5 | 65.5 | 68 | 73 |
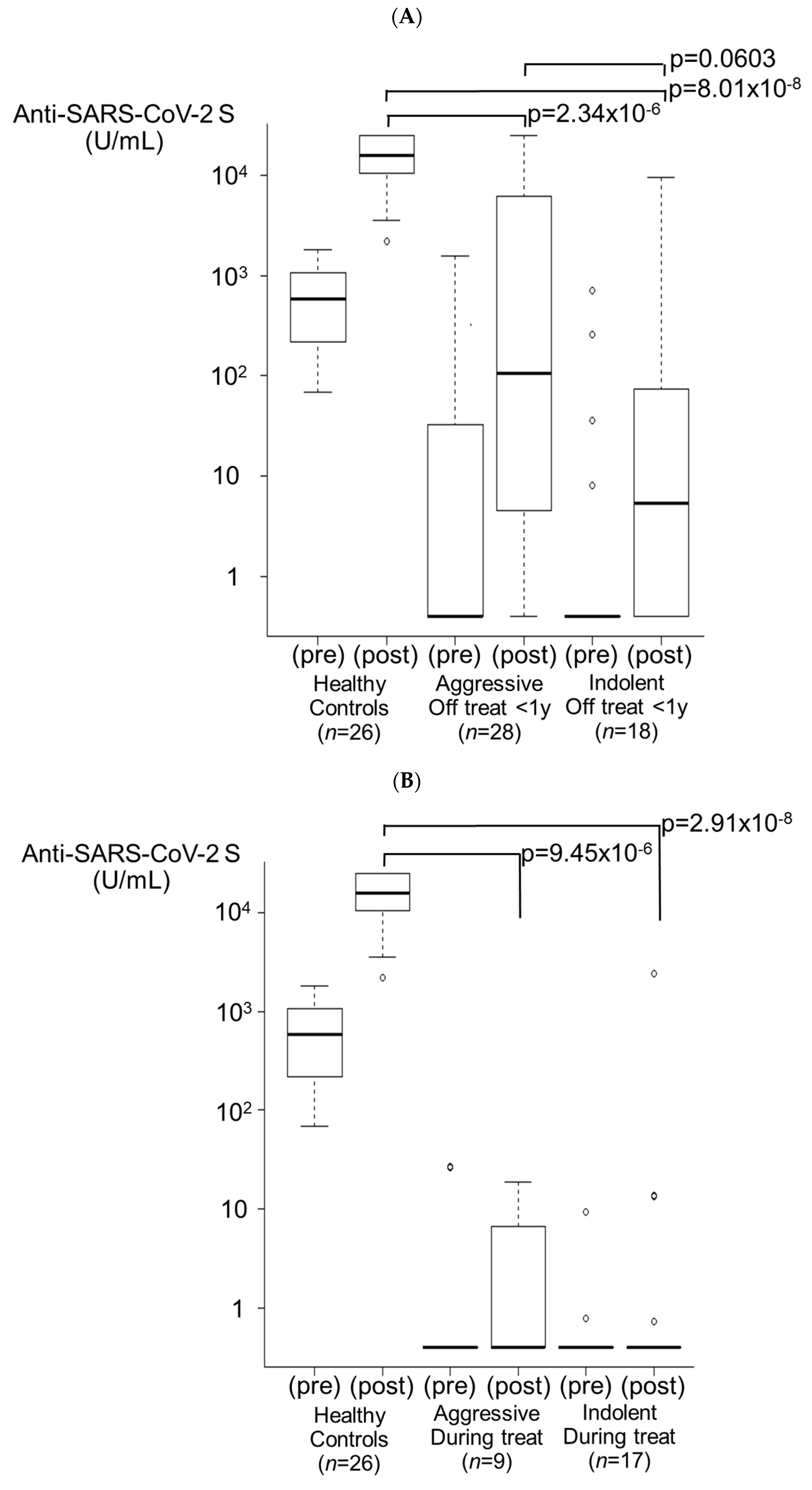
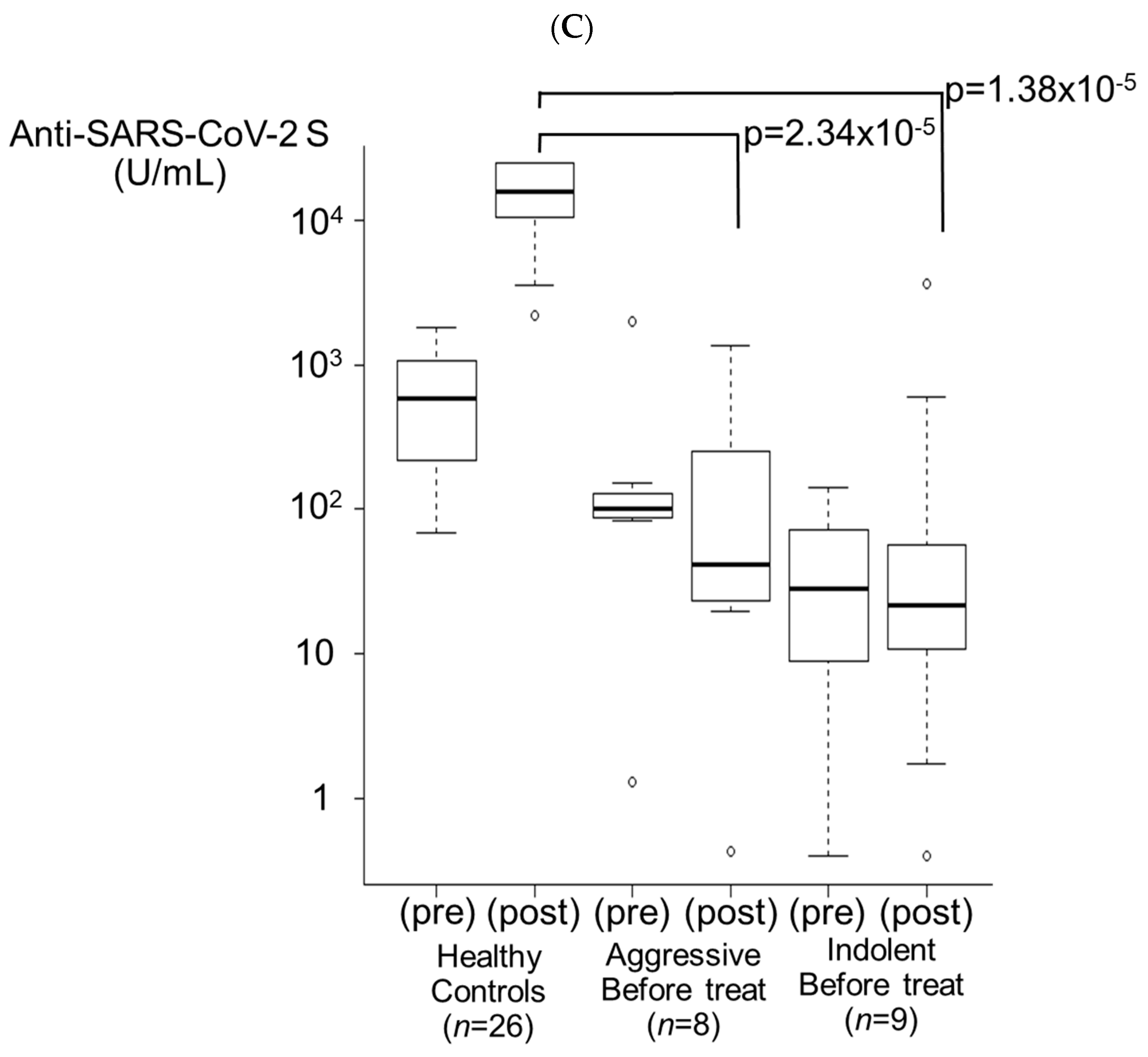
| Pre-value (U/mL) | 582.5 | 680 | <0.40 | <0.40 | 100 | 939 | 434 | <0.40 | <0.40 | 28.1 |
| Post-value (U/mL) | 15,324 | 20,419 | 109.45 | <0.40 | 41.85 | 15,459.5 | 17,071 | 8.49 | <0.40 | 21.8 |
| Seroconversion rate (%) | (-/0) | 0 (0/1) | 68.4 (13/19) | 28.6 (2/7) | (-/0) | (-/0) | 50 (1/2) | 42.9 (6/14) | 12.5 (2/16) | 50 (1/2) |
| Booster effect (%) | 100 | 97.8 | 78.6 | 11.1 | 12.5 | 100 | 97.5 | 50 | 17.6 | 22.2 |
| Antibody titer > 5000 (%) | 24 (92.3) | 42 (93.3) | 8 (28.6) | 0 (0) | 0 (0) | 11 (91.7) | 32 (80) | 2 (11.1) | 0 (0) | 0 (0) |

3.3.2. Off Treatment for >1 Year Group (Figure 2)
3.3.3. Off Treatment for <1 Year Group (Figure 3A)
3.3.4. During Treatment Group (Figure 3B)
3.3.5. Before Treatment Group (Figure 3C)


3.4. Breakthrough Infection after Booster Vaccination (Table 4A,B)
| (A) | |||||||||||
| Age | Sex | Histology | Last Treatment Regimen | Lymphoma Treatment Status at the Start of Vaccination | Number of Vaccinations (Time to Onset) | Pre-infection Antibody Titer (U/mL) | Severity | Infectious Status | COVID-19 Treatment | Post-Infection Antibody Titer (U/mL) | |
| 1 | 70 | M | DLBCL | R-CHOP | Off >1 y | 3 (163) | >25,000 | mild | community infection | Usual care | >25,000 |
| 2 | 65 | F | DLBCL | R-EPOCH + MTX | Off >1 y | 3 (99) | 24,148 | mild | community infection | Usual care | >25,000 |
| 3 | 69 | M | DLBCL | R-CHOP | Off >1 y | 3 (158) | 12,142 | mild | community infection | Usual care | >25,000 |
| 4 | 54 | F | DLBCL | R-CHOP | Off >1 y | 3 (58) | 3902 | mild | community infection | Usual care | >25,000 |
| 5 | 78 | F | DLBCL | Pola-BR | Off <1 y | 4 (48) | 5523 | mild | nosocomial infection (under treatment-1 course) | Molnupiravir | 1478 |
| 6 | 44 | F | DLBCL | R-CHOP | Before | 3 (184) | 19,663 | mild | community infection | Usual care | 10,479 |
| 7 | 68 | F | DLBCL | R-CHOP | Before | 3 (195) | 1268 | mild | nosocomial infection (under treatment-5 courses) | Molnupiravir | 1327 |
| (B) | |||||||||||
| Age | Sex | Histology | Last Treatment Regimen | Lymphoma Treatment Status at the Start of Vaccination | Number of Vaccinations (Time to Onset) | Pre-Infection Antibody Titer (U/mL) | Severity | Infectious Status | COVID-19 Treatment | Post-Infection Antibody Titer (U/mL) | |
| 8 | 79 | M | FL | R-CHOP | Off >1 y | 3 (88) | 16,384 | mild | community infection | Usual care | >25,000 |
| 9 | 91 | M | FL | RTX | Off >1 y | 3 (19) | 56 | mild | nosocomial infection (other diseases) | Molnupiravir | >25,000 |
| 10 | 61 | F | MALT | BR + R maintenance | Off >1 y | 3 (5) | 46.8 | mild | community infection | Usual care | >25,000 |
| 11 | 76 | F | FL | R-CHOP/R-F + R maintenance | Off >1 y | 4 (114) | 8833 | mild | community infection | Usual care | >25,000 |
| 12 | 71 | M | FL | BR | Off >1 y | 4 (76) | 1664 | mild | community infection | Usual care | 2581 |
| 13 | 58 | M | FL | auto-SCT | Off >1 y | 4 (60) | <0.4 | moderate-1 | community infection | Usual care | <0.4 |
| 14 | 71 | M | MCL | BR | Off >1 y | 4 (75) | 38.6 | death | nosocomial infection (before treatment) | Remdesivir, Sotrovimab | 8318 |
| 15 | 51 | F | FL | GB | Off <1 y | 3 (81) | <0.4 | mild | community infection | Molnupiravir | <0.4 |
| 16 | 75 | M | FL | RTX | Off <1 y | 4 (50) | 848 | mild (sequelae) | nosocomial infection (other diseases) | Molnupiravir | 2029 |
| 17 | 51 | M | FL | CAR-T | Off <1 y | 4 (123) | 0.53 | mild | community infection | Molnupiravir | <0.4 |
| 18 | 56 | M | FL | G-CHOP + G maintenance | During | 3 (306) | <0.4 | mild | community infection | Usual care | <0.4 |
| 19 | 60 | F | FL | GB + G maintenance | During | 3 (34) | <0.4 | moderate-2 | community infection | Molnupiravir, Sotrovimab, Nirmatrelvir/Ritonavir, Remdesivir | 9366 |
| 20 | 67 | M | FL | BR + R maintenance | During | 4 (55) | 14,685 | mild | community infection | Usual care | >25,000 |
| 21 | 73 | M | FL | GB + G maintenance | During | 4 (61) | <0.4 | mild | community infection | Molnupiravir | <0.4 |
| 22 | 70 | F | FL | GB + G maintenance | During | 4 (191) | <0.4 | moderate-1 | community infection | Usual care | <0.4 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Statement on the Fifteenth Meeting of the IHR (2005) Emergency Committee on the COVID-19 Pandemic n.d. Available online: https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(COVID-19)-pandemic (accessed on 22 November 2023).
- Maneikis, K.; Šablauskas, K.; Ringelevičiūtė, U.; Vaitekėnaitė, V.; Čekauskienė, R.; Kryžauskaitė, L.; Naumovas, D.; Banys, V.; Pečeliūnas, V.; Beinortas, T.; et al. Immunogenicity of the BNT162b2 COVID-19 mRNA vaccine and early clinical outcomes in patients with haematological malignancies in Lithuania: A national prospective cohort study. Lancet Haematol. 2021, 8, e583–e592. [Google Scholar] [CrossRef]
- Jurgens, E.M.; Ketas, T.J.; Zhao, Z.; Joseph Satlin, M.; Small, C.B.; Sukhu, A.; Francomano, E.; Klasse, P.J.; Garcia, A.; Nguyenduy, E.; et al. Serologic response to mRNA COVID-19 vaccination in lymphoma patients. Am. J. Hematol. 2021, 96, E410–E413. [Google Scholar] [CrossRef]
- Chung, D.J.; Shah, G.L.; Devlin, S.M.; Ramanathan, L.V.; Doddi, S.; Pessin, M.S.; Hoover, E.; Marcello, L.T.; Young, J.C.; Boutemine, S.R.; et al. Disease- and Therapy-Specific Impact on Humoral Immune Responses to COVID-19 Vaccination in Hematologic Malignancies. Blood Cancer Discov. 2021, 2, 568–576. [Google Scholar] [CrossRef]
- Perry, C.; Luttwak, E.; Balaban, R.; Shefer, G.; Morales, M.M.; Aharon, A.; Tabib, Y.; Cohen, Y.C.; Benyamini, N.; Beyar-Katz, O.; et al. Efficacy of the BNT162b2 mRNA COVID-19 vaccine in patients with B-cell non-Hodgkin lymphoma. Blood. Adv. 2021, 5, 3053–3061. [Google Scholar] [CrossRef]
- Gurion, R.; Rozovski, U.; Itchaki, G.; Gafter-Gvili, A.; Leibovitch, C.; Raanani, P.; Ben-Zvi, H.; Szwarcwort, M.; Taylor-Abigadol, M.; Dann, E.J.; et al. Humoral serological response to the BNT162b2 vaccine is abrogated in lymphoma patients within the first 12 months following treatment with anti-CD20 antibodies. Haematologica 2022, 107, 715–720. [Google Scholar] [CrossRef]
- Duléry, R.; Lamure, S.; Delord, M.; Di Blasi, R.; Chauchet, A.; Hueso, T.; Rossi, C.; Drenou, B.; Deau Fischer, B.; Soussain, C.; et al. Prolonged in-hospital stay and higher mortality after COVID-19 among patients with non-Hodgkin lymphoma treated with B-cell depleting immunotherapy. Am. J. Hematol. 2021, 96, 934–944. [Google Scholar] [CrossRef]
- Kohn, M.; Delord, M.; Chbat, M.; Guemriche, A.; Merabet, F.; Roupie, A.L.; Lombion, N.; Farhat, H.; Longval, T.; Cabannes-Hamy, A.; et al. A third anti-SARS-CoV-2 mRNA dose does not overcome the pejorative impact of anti-CD20 therapy and/or low immunoglobulin levels in patients with lymphoma or chronic lymphocytic leukemia. Haematologica 2022, 107, 1454–1459. [Google Scholar] [CrossRef]
- Herishanu, Y.; Rahav, G.; Levi, S.; Braester, A.; Itchaki, G.; Bairey, O.; Dally, N.; Shvidel, L.; Ziv-Baran, T.; Polliack, A.; et al. Efficacy of a third BNT162b2 mRNA COVID-19 vaccine dose in patients with CLL who failed standard 2-dose vaccination. Blood 2022, 139, 678–685. [Google Scholar] [CrossRef]
- Avivi, I.; Luttwak, E.; Saiag, E.; Halperin, T.; Haberman, S.; Sarig, A.; Levi, S.; Aharon, A.; Herishanu, Y.; Perry, C. BNT162b2 mRNA COVID-19 vaccine booster induces seroconversion in patients with B-cell non-Hodgkin lymphoma who failed to respond to two prior vaccine doses. Br. J. Haematol. 2022, 196, 1329–1333. [Google Scholar] [CrossRef]
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E.; et al. Homologous and Heterologous COVID-19 Booster Vaccinations. N. Engl. J. Med. 2022, 386, 1046–1057. [Google Scholar] [CrossRef]
- Mai, A.S.; Lee, A.R.Y.B.; Tay, R.Y.K.; Shapiro, L.; Thakkar, A.; Halmos, B.; Grinshpun, A.; Herishanu, Y.; Benjamini, O.; Tadmor, T.; et al. Booster doses of COVID-19 vaccines for patients with haematological and solid cancer: A systematic review and individual patient data meta-analysis. Eur. J. Cancer 2022, 172, 65–75. [Google Scholar] [CrossRef]
- Ollila, T.A.; Masel, R.H.; Reagan, J.L.; Lu, S.; Rogers, R.D.; Paiva, K.J.; Taher, R.; Burguera-Couce, E.; Zayac, A.S.; Yakirevich, I.; et al. Seroconversion and outcomes after initial and booster COVID-19 vaccination in adults with hematologic malignancies. Cancer 2022, 128, 3319–3329. [Google Scholar] [CrossRef]
- Lee, L.Y.W.; Tilby, M.; Starkey, T.; Ionescu, M.C.; Burnett, A.; Hattersley, R.; Khan, S.; Little, M.; Liu, J.K.H.; Platt, J.R.; et al. Association of SARS-CoV-2 spike protein antibody vaccine response with infection severity in patients with cancer: A national COVID cancer cross-sectional evaluation. JAMA. Oncol. 2023, 9, 188–196. [Google Scholar] [CrossRef]
- Pagano, L.; Salmanton-García, J.; Marchesi, F.; Blennow, O.; Gomes da Silva, M.; Glenthøj, A.; van Doesum, J.; Bilgin, Y.M.; López-García, A.; Itri, F.; et al. Breakthrough COVID-19 in vaccinated patients with hematologic malignancies: Results from the EPICOVIDEHA survey. Blood 2022, 140, 2773–2787. [Google Scholar] [CrossRef]
- Kageyama, T.; Ikeda, K.; Tanaka, S.; Taniguchi, T.; Igari, H.; Onouchi, Y.; Kaneda, A.; Matsushita, K.; Hanaoka, H.; Nakada, T.A.; et al. Antibody responses to BNT162b2 mRNA COVID-19 vaccine and their predictors among healthcare workers in a tertiary referral hospital in Japan. Clin. Microbiol. Infect. 2021, 27, e1–e5. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare (Japan). COVID-19 Medical Treatment Guide, Version 9.0; Ministry of Health, Labour and Welfare: Tokyo, Japan, 2023.
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone. Marrow. Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Uaprasert, N.; Pitakkitnukun, P.; Tangcheewinsirikul, N.; Chiasakul, T.; Rojnuckarin, P. Immunogenicity and risks associated with impaired immune responses following SARS-CoV-2 vaccination and booster in hematologic malignancy patients: An updated meta-analysis. Blood Cancer J. 2022, 12, 173. [Google Scholar] [CrossRef]
- Salles, G.; Barrett, M.; Foà, R.; Maurer, J.; O’Brien, S.; Valente, N.; Wenger, M.; Maloney, D.G. Rituximab in B-Cell Hematologic Malignancies: A Review of 20 Years of Clinical Experience. Adv. Ther. 2017, 34, 2232–2273. [Google Scholar] [CrossRef]
- Piro, L.D.; White, C.A.; Grillo-López, A.J.; Janakiraman, N.; Saven, A.; Beck, T.M.; Varns, C.; Shuey, S.; Czuczman, M.; Lynch, J.W.; et al. Extended Rituximab (anti-CD20 monoclonal antibody) therapy for relapsed or refractory low-grade or follicular non-Hodgkin’s lymphoma. Ann. Oncol. 1999, 10, 655–661. [Google Scholar] [CrossRef]
- Ishio, T.; Tsukamoto, S.; Yokoyama, E.; Izumiyama, K.; Saito, M.; Muraki, H.; Kobayashi, M.; Mori, A.; Morioka, M.; Kondo, T. Anti-CD20 antibodies and bendamustine attenuate humoral immunity to COVID-19 vaccination in patients with B-cell non-Hodgkin lymphoma. Ann. Hematol. 2023, 102, 1421–1431. [Google Scholar] [CrossRef]
- Kamegai, K.; Iwamoto, N.; Togano, T.; Maeda, K.; Takamatsu, Y.; Miyazato, Y.; Ishikane, M.; Mizokami, M.; Sugiyama, M.; Iida, S.; et al. A fatal breakthrough COVID-19 case following Bendamustine-Rituximab therapy. Int. J. Infect. Dis. 2022, 121, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Arai, T.; Mukai, S.; Kazama, R.; Ogawa, Y.; Nishida, K.; Hatanaka, K.; Gohma, I. Persistent viral shedding of severe acute respiratory syndrome coronavirus 2 after treatment with bendamustine and rituximab: A case report. J. Infect. Chemother. 2022, 28, 810–813. [Google Scholar] [CrossRef] [PubMed]
- Nakakubo, S.; Kishida, N.; Okuda, K.; Kamada, K.; Iwama, M.; Suzuki, M.; Yokota, I.; Ito, Y.M.; Nasuhara, Y.; Boucher, R.C.; et al. Associations of COVID-19 symptoms with omicron subvariants BA.2 and BA.5, host status, and clinical outcomes in Japan: A registry-based observational study. Lancet. Infect. Dis. 2023, 23, 1244–1256. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Infectious Diseases, Ministry of Health, Labor and Welfare. Analysis of the Rate of Infected People Using Donated Blood Samples in February 2023; National Institute of Infectious Diseases, Ministry of Health, Labor and Welfare: Tokyo, Japan, 2023.
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: A cohort study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef]
- Hu, F.H.; Jia, Y.J.; Zhao, D.Y.; Fu, X.L.; Zhang, W.Q.; Tang, W.; Hu, S.Q.; Wu, H.; Ge, M.W.; Du, W.; et al. Clinical outcomes of the severe acute respiratory syndrome coronavirus 2 Omicron and Delta variant: Systematic review and meta-analysis of 33 studies covering 6037144 coronavirus disease 2019-positive patients. Clin. Microbiol. Infect. 2023, 29, 835–844. [Google Scholar] [CrossRef]
- Zhu, X.; Jiang, Q.; Lu, J.; Sun, Y.; Zhao, X.; Yang, S.; Tang, F.; Yu, W.; Zhao, T.; Liu, X.; et al. COVID-19 infection in patients with haematological malignancies: A single-centre survey in the latest Omicron wave in China. Br. J. Haematol. 2023, 202, 31–39. [Google Scholar] [CrossRef]
- Shafat, T.; Grupel, D.; Porges, T.; Levi, I.; Yagel, Y.; Nesher, L. Treatment with obinutuzumab leads to worse outcomes in haematological patients diagnosed with Omicron variant COVID-19. Br. J. Haematol. 2022, 198, 826–829. [Google Scholar] [CrossRef]
- Haggenburg, S.; Hofsink, Q.; Rutten, C.E.; Nijhof, I.S.; Hazenberg, M.D.; Goorhuis, A. SARS-CoV-2 vaccine-induced humoral and cellular immunity in patients with hematologic malignancies. Semin. Hematol. 2022, 59, 192–197. [Google Scholar] [CrossRef]
- Chien, K.S.; Peterson, C.B.; Young, E.; Chihara, D.; Manasanch, E.E.; Ramdial, J.L.; Thompson, P.A. Outcomes of breakthrough COVID-19 infections in patients with hematologic malignancies. Blood Adv. 2023, 7, 5691–5697. [Google Scholar] [CrossRef] [PubMed]

| Age | 71 (39–92) | |
| Sex | M 47, F 43 | |
| Disease | ||
| DLBCL | 82 | |
| IVL | 5 | |
| PCNSL | 1 | |
| PML-BL | 1 | |
| Unclassifiable | 1 | |
| Treatment Status | ||
| Off >1 year | 45 | |
| Off <1 year | 28 | |
| During | 9 | |
| Before | 8 | |
| Treatment Regimen | ||
| R-CHOP like | 72 | |
| R + salvage | 16 | |
| SCT | 7 (auto 6, allo 1) | |
| BR (/R monotherapy) | 3 | |
| Vaccine subtype | First/Second doses | Third dose |
| BNT162b2 | 80 | 58 |
| mRNA-1273 | 10 | 32 |
| Age | 69 (38–87) | |
| Sex | M 56, F 40 | |
| Disease | ||
| FL | 61 | |
| CLL/SLL * | 9 | |
| LPL | 9 | |
| MZL ** | 7 | |
| MCL | 7 | |
| Others | 3 | |
| Treatment Status | ||
| Naïve | 12 | |
| Off >1 year | 40 | |
| Off <1 year | 18 | |
| During | 17 | |
| Before | 9 | |
| Treatment Regimen | ||
| R (G)-CHOP like | 37 | |
| R (G)-B/R-BAC | 30 | |
| R (G) monotherapy | 8 | |
| BTK inhibitors | 7 | |
| R-salvage | 4 | |
| SCT (auto-) | 2 | |
| CAR-T | 1 | |
| Others | 5 | |
| Vaccine subtype | First/Second doses | Third dose |
| BNT162b2 | 82 | 65 |
| mRNA-1273 | 14 | 31 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saito, M.; Mori, A.; Ishio, T.; Kobayashi, M.; Tsukamoto, S.; Kajikawa, S.; Yokoyama, E.; Kanaya, M.; Izumiyama, K.; Muraki, H.; et al. Initial Efficacy of the COVID-19 mRNA Vaccine Booster and Subsequent Breakthrough Omicron Variant Infection in Patients with B-Cell Non-Hodgkin’s Lymphoma: A Single-Center Cohort Study. Viruses 2024, 16, 328. https://doi.org/10.3390/v16030328
Saito M, Mori A, Ishio T, Kobayashi M, Tsukamoto S, Kajikawa S, Yokoyama E, Kanaya M, Izumiyama K, Muraki H, et al. Initial Efficacy of the COVID-19 mRNA Vaccine Booster and Subsequent Breakthrough Omicron Variant Infection in Patients with B-Cell Non-Hodgkin’s Lymphoma: A Single-Center Cohort Study. Viruses. 2024; 16(3):328. https://doi.org/10.3390/v16030328
Chicago/Turabian StyleSaito, Makoto, Akio Mori, Takashi Ishio, Mirei Kobayashi, Shihori Tsukamoto, Sayaka Kajikawa, Emi Yokoyama, Minoru Kanaya, Koh Izumiyama, Haruna Muraki, and et al. 2024. "Initial Efficacy of the COVID-19 mRNA Vaccine Booster and Subsequent Breakthrough Omicron Variant Infection in Patients with B-Cell Non-Hodgkin’s Lymphoma: A Single-Center Cohort Study" Viruses 16, no. 3: 328. https://doi.org/10.3390/v16030328