

Risks of Adverse Outcomes for Hospitalized COVID-19 Patients during the Four Waves in Brazil According to SARS-CoV-2 Variants, Age Group, and Vaccine Status

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Koelle, K.; Martin, M.A.; Antia, R.; Lopman, B.; Dean, N.E. The changing epidemiology of SARS-CoV-2. Science 2022, 375, 1116–1121. [Google Scholar] [CrossRef]
- WHO. Tracking SARS-CoV-2 Variants. 2022. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on 17 August 2023).
- de Souza, F.S.H.; Hojo-Souza, N.S.; Batista, B.D.D.O.; da Silva, C.M.; Guidoni, D.L. On the analysis of mortality risk factors for hospitalized COVID-19 patients: A data-driven study using the major Brazilian database. PLoS ONE 2021, 16, e0248580. [Google Scholar] [CrossRef]
- Sabino, E.C.; Buss, L.F.; Carvalho, M.P.S.; Prete, C.A.; Crispim, M.A.E.; Fraiji, N.A.; Parag, K.V.; da Silva Peixoto, P.; Kraemer, M.U.G.; Oikawa, M.K.; et al. Resurgence of COVID-19 in Manaus, Brazil, despite high seroprevalence. Lancet 2021, 397, 452–455. [Google Scholar] [CrossRef]
- Naveca, F.G.; Nascimento, V.; de Souza, V.C.; de Corado, A.L.; Nascimento, F.; Silva, G.; Costa, Á.; Duarte, D.; Pessoa, K.; Mejía, M.; et al. COVID-19 in Amazonas, Brazil, Was Driven by the Persistence of Endemic Lineages and P.1 Emergence. Nat. Med. 2021, 27, 1230–1238. [Google Scholar] [CrossRef]
- de Souza, F.S.H.; Hojo-Souza, N.S.; da Silva, C.M.; Guidoni, D.L. Second wave of COVID-19 in Brazil: Younger at higher risk. Eur. J. Epidemiol. 2021, 36, 441–443. [Google Scholar] [CrossRef]
- National Center for Immunization and Respiratory Diseases (NCIRD); Division of Viral Diseases. CDC COVID-19 Science Briefs [Internet]; Science Brief: Omicron (B.1.1.529) Variant; Centers for Disease Control and Prevention (US): Atlanta, GA, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK575856/ (accessed on 17 August 2023).
- Mohapatra, R.K.; El-Shall, N.A.; Tiwari, R.; Nainu, F.; Kandi, V.; Sarangi, A.K.; Mohammed, T.A.; Desingu, P.A.; Chakraborty, C.; Dhama, K. Need of booster vaccine doses to counteract the emergence of SARS-CoV-2 variants in the context of the Omicron variant and increasing COVID-19 cases: An update. Hum. Vaccines Immunother. 2022, 18, 2065824. [Google Scholar] [CrossRef]
- Conass. Painel Nacional: COVID-19. 2022. Available online: https://www.conass.org.br/painelconasscovid19/ (accessed on 17 August 2023).
- Cota, W. Monitoring the Number of COVID-19 Cases and Deaths in Brazil at Municipal and Federative Units Level. Available online: https://coronavirusbra1.github.io/ (accessed on 17 August 2023).
- Fiocruz. Fundação Oswaldo Cruz. Dashboard Genomic Networks: SARS-CoV-2 Genomic Surveillance in Brazil. Available online: https://www.genomahcov.fiocruz.br/dashboard-en/ (accessed on 17 August 2023).
- Katzourakis, A. COVID-19: Endemic doesn’t mean harmless. Nature 2022, 601, 485. [Google Scholar] [CrossRef]
- Hojo-Souza, N.S.; Freitas, V.L.S.; Guidoni, D.L.; de Souza, F.S.H. Clinical symptoms profile of hospitalized COVID-19 Brazilian patients according to SARS-CoV-2 variants. Epidemiol. Health 2023. accepted for publication. [Google Scholar] [CrossRef]
- Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Imunização e Doenças Transmissíveis. Plano Nacional de Operacionalização da Vacinação Contra a COVID-19, 12th ed.; Ministério da Saúde: Brasília, Brazil, 2022. Available online: https://www.gov.br/saude/pt-br/coronavirus/publicacoes-tecnicas/guias-e-planos/plano-nacional-de-operacionalizacao-da-vacinacao-contra-covid-19.pdf (accessed on 17 August 2023).
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.P.G.; et al. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: Results of a systematic review and meta-regression. Lancet 2022, 399, 924–944. [Google Scholar] [CrossRef]
- Menni, C.; May, A.; Polidori, L.; Louca, P.; Wolf, J.; Capdevila, J.; Hu, C.; Ourselin, S.; Steves, C.J.; Valdes, A.M.; et al. COVID-19 vaccine waning and effectiveness and side-effects of boosters: A prospective community study from the ZOE COVID Study. Lancet Infect Dis. 2022, 22, 1002–1010. [Google Scholar] [CrossRef]
- Willett, B.J.; Grove, J.; MacLean, O.A.; Wilkie, C.; De Lorenzo, G.; Furnon, W.; Cantoni, D.; Scott, S.; Logan, N.; Ashraf, S.; et al. SARS-CoV-2 Omicron is an immune escape variant with an altered cell entry pathway. Nat. Microbiol. 2022, 7, 1161–1179. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Guo, Y.; Iketani, S.; Nair, M.S.; Li, Z.; Mohri, H.; Wang, M.; Yu, J.; Bowen, A.D.; Chang, J.Y.; et al. Antibody evasion by SARS-CoV-2 Omicron subvariants BA. 2.12. 1, BA. 4 and BA. 5. Nature 2022, 608, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Tizazu, A.M.; Mengist, H.M.; Demeke, G. Aging, inflammaging and immunosenescence as risk factors of severe COVID-19. Immun. Ageing 2022, 19, 53. [Google Scholar] [CrossRef] [PubMed]
- Discacciati, M.G.; Siani, S.; Campa, A.; Nakaya, H.I. Why should obese youth be prioritized in COVID-19 vaccination programs? A nationwide retrospective study. Lancet Reg. Health-Am. 2022, 7, 100167. [Google Scholar] [CrossRef] [PubMed]
- de Jesus, M.A.; Hojo-Souza, N.S.; de Moraes, T.R.; Guidoni, D.L.; de Souza, F.S. Profile of Brazilian inpatients with COVID-19 vaccine breakthrough infection and risk factors for unfavorable outcome. Rev. Panam. De Salud Pública 2023, 46, e106. [Google Scholar] [CrossRef]
- Giovanetti, M.; Fonseca, V.; Wilkinson, E.; Tegally, H.; San, E.J.; Althaus, C.L.; de Alcantara, L.C.J.; Xavier, J.; Slavov, S.N.; Viala, V.L.; et al. Replacement of the Gamma by the Delta variant in Brazil: Impact of lineage displacement on the ongoing pandemic. Virus Evol. 2022, 8, veac024. [Google Scholar] [CrossRef]
- Dejnirattisai, W.; Huo, J.; Zhou, D.; Zahradník, J.; Supasa, P.; Liu, C.; Murphy, D.; Duyvesteyn, H.M.E.; Ginn, H.M.; Mentzer, A.J.; et al. SARS-CoV-2 Omicron-B. 1.1. 529 leads to widespread escape from neutralizing antibody responses. Cell 2022, 185, 467–484. [Google Scholar] [CrossRef]
- Silva, S.J.R.D.; Kohl, A.; Pena, L.; Pardee, K. Recent insights into SARS-CoV-2 omicron variant. Rev. Med. Virol. 2023, 33, e2373. [Google Scholar] [CrossRef]
- Wolter, N.; Jassat, W.; Walaza, S.; Welch, R.; Moultrie, H.; Groome, M.; Cohen, C.; Amoako, D.G.; Everatt, J.; Bhiman, J.N.; et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: A data linkage study. Lancet 2022, 399, 437–446. [Google Scholar] [CrossRef]
- Jassat, W.; Abdool Karim, S.S.; Ozougwu, L.; Welch, R.; Mudara, C.; Masha, M.; Rousseau, P.; Wolmarans, M.; Selikow, A.; Govender, N.; et al. Trends in Cases, Hospitalizations, and Mortality Related to the Omicron BA. 4/BA. 5 Subvariants in South Africa. Clin. Infect. Dis. 2023, 76, 1468–1475. [Google Scholar] [CrossRef]
- Colnago, M.; Benvenuto, G.A.; Casaca, W.; Negri, R.G.; Fernandes, E.G.; Cuminato, J.A. Risk Factors Associated with Mortality in Hospitalized Patients with COVID-19 during the Omicron Wave in Brazil. Bioengineering 2022, 9, 584. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Ramírez, L.; Solis-Tejeda, I.; Ayon-Aguilar, J.; Mayoral-Ortiz, A.; Sosa-Jurado, F.; Pelayo, R.; Santos-López, G.; Cortes-Hernandez, P. Decrease in COVID-19 adverse outcomes in adults during the Delta and Omicron SARS-CoV-2 waves, after vaccination in Mexico. Front. Public Health 2022, 10, 1010256. [Google Scholar] [CrossRef] [PubMed]
- Alcendor, D.J.; Matthews-Juarez, P.; Smoot, D.; Hildreth, J.E.; Lamar, K.; Tabatabai, M.; Wilus, D.; Juarez, P.D. Breakthrough COVID-19 infections in the US: Implications for prolonging the pandemic. Vaccines 2022, 10, 755. [Google Scholar] [CrossRef]
- Garcia-Beltran, W.F.; Denis, K.J.S.; Hoelzemer, A.; Lam, E.C.; Nitido, A.D.; Sheehan, M.L.; Berrios, C.; Ofoman, O.; Chang, C.C.; Balazs, A.B.; et al. mRNA-based COVID-19 vaccine boosters induce neutralizing immunity against SARS-CoV-2 Omicron variant. Cell 2022, 185, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Gao, B.; He, L.; Bao, Y.; Chen, Y.; Lu, G.; Zhang, Y.; Xu, Y.; Su, B.; Xu, J.; Wang, Y.; et al. Repeated vaccination of inactivated SARS-CoV-2 vaccine dampens neutralizing antibodies against Omicron variants in breakthrough infection. Cell Res. 2023, 33, 258–261. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| W1 (n = 193,391) | W2 (n = 339,234) | W3 (n = 71,218) | W4 (n = 29,977) | |
|---|---|---|---|---|
| Age, median (IQR), years | 62 (26.00) | 58 (21.00) | 71 (34.00) | 74 (36.00) |
| Age group | ||||
| 18–39 | 24,365 (12.60%) | 49,312 (14.54%) | 7816 (10.97%) | 2663 (8.88%) |
| 40–59 | 62,846 (32.50%) | 133,280 (39.29%) | 13,528 (19.00%) | 4449 (14.84%) |
| 60–79 | 76,635 (39.63%) | 126,891 (37.41%) | 28,662 (40.25%) | 11,854 (39.54%) |
| ≥80 | 29,545 (15.28%) | 29,751 (8.77%) | 21,212 (29.78%) | 11,011 (36.73%) |
| Gender | ||||
| Female | 85,217 (44.06%) | 151,835 (44.76%) | 34,739 (48.78%) | 15,606 (52.06%) |
| Male | 108,174 (55.94%) | 187,399 (55.24%) | 36,479 (51.22%) | 14,371 (47.94%) |
| Region | ||||
| Midwest | 25,562 (13.22%) | 31,530 (9.29%) | 5754 (8.08%) | 2719 (9.07%) |
| North | 6287 (3.25%) | 12,447 (3.67%) | 3136 (4.40%) | 679 (2.27%) |
| Northeast | 30,260 (15.65%) | 41,348 (12.19%) | 8656 (12.15%) | 2884 (9.62%) |
| South | 31,260 (16.16%) | 80,465 (23.72%) | 15,450 (21.69%) | 6183 (20.63%) |
| Southeast | 100,022 (51.72%) | 173,444 (51.13%) | 38,222 (53.67%) | 17,512 (58.42%) |
| Vaccine status | ||||
| Booster | 0 (0.00%) | 0 (0.00%) | 9141 (12.84%) | 18,393 (61.36%) |
| Fully | 0 (0.00%) | 3432 (1.01%) | 35,978 (50.52%) | 7518 (25.08%) |
| Partial | 0 (0.00%) | 24,248 (7.15%) | 3580 (5.03%) | 1049 (3.50%) |
| Unvaccinated | 193,391 (100.00%) | 311,554 (91.84%) | 22,519 (31.62%) | 3017 (10.06%) |
| W1 (n = 193,391) | W2 (n = 339,234) | W3 (n = 71,218) | W4 (n = 29,977) | |
|---|---|---|---|---|
| Cardiac disease | n = 171,767 | n = 300,788 | n = 60,415 | n = 25,555 |
| 71,486 (41.62%) | 108,552 (36.09%) | 27,292 (45.17%) | 12,123 (47.44%) | |
| Hematological disease | n = 147,698 | n = 261,765 | n = 50,213 | n = 21,338 |
| 1567 (1.06%) | 1706 (0.65%) | 813 (1.62%) | 393 (1.84%) | |
| Down’s syndrome | n = 147,701 | n = 261,604 | n = 50,089 | n = 21,306 |
| 441 (0.30%) | 828 (0.32%) | 242 (0.48%) | 87 (0.41%) | |
| Liver disease | n = 147,575 | n = 261,454 | n = 50,097 | n = 21,331 |
| 1933 (1.31%) | 2159 (0.83%) | 861 (1.72%) | 395 (1.85%) | |
| Asthma | n = 148,643 | n = 263,535 | n = 50,313 | n = 21,498 |
| 5339 (3.59%) | 8038 (3.05%) | 1725 (3.43%) | 867 (4.03%) | |
| Diabetes | n = 165,434 | n = 289,125 | n = 57,070 | n = 23,936 |
| 52,729 (31.87%) | 74,602 (25.80%) | 18,233 (31.95%) | 7275 (30.39%) | |
| Neurologic disease | n = 149,868 | n = 263,795 | n = 52,003 | n = 22,161 |
| 8625 (5.76%) | 8818 (3.34%) | 5668 (10.90%) | 2795 (12.61%) | |
| Pulmonary disease | n = 149,696 | n = 264,003 | n = 51,517 | n = 22,008 |
| 8239 (5.50%) | 8583 (3.25%) | 4349 (8.44%) | 2401 (10.91%) | |
| Immunosuppression | n = 148,417 | n = 262,564 | n = 51,055 | n = 21,699 |
| 5678 (3.83%) | 5723 (2.18%) | 3464 (6.78%) | 1612 (7.43%) | |
| Obesity | n = 148,911 | n = 271,813 | n = 50,854 | n = 21,341 |
| 12,762 (8.57%) | 35,609 (13.10%) | 4320 (8.49%) | 1253 (5.87%) | |
| Kidney disease | n = 149,768 | n = 263,708 | n = 51,484 | n = 21,828 |
| 9009 (6.02%) | 9071 (3.44%) | 4510 (8.76%) | 1845 (8.45%) | |
| Other comorbidity | n = 163,410 | n = 289,066 | n = 59,418 | n = 25,120 |
| 57,513 (35.20%) | 87,598 (30.30%) | 25,366 (42.69%) | 11,337 (45.13%) |
| W1 (n = 193,391) | W2 (n = 339,234) | W3 (n = 71,218) | W4 (n = 29,977) | |
|---|---|---|---|---|
| In-hospital death | n = 193,391 | n = 339,234 | n = 71,218 | n = 29,977 |
| 65,148 (33.69%) | 125,231 (36.92%) | 25,634 (35.99%) | 8527 (28.45%) | |
| IMV | n = 171,605 | n = 307,010 | n = 63,026 | n = 26,440 |
| 36,457 (21.24%) | 74,676 (24.32%) | 12,056 (19.13%) | 3966 (15.00%) | |
| NIV | n = 171,605 | n = 307,010 | n = 63,026 | n = 26,440 |
| 91,059 (53.06%) | 189,946 (61.87%) | 33,769 (53.58%) | 13,521 (51.14%) | |
| ICU | n = 178,350 | n = 312,958 | n = 65,604 | n = 27,699 |
| 69,287 (38.85%) | 118,250 (37.78%) | 24,873 (37.91%) | 9253 (33.41%) |
| W1 (n = 193,391) | W2 (n = 339,234) | W3 (n = 71,218) | W4 (n = 29,977) | |
|---|---|---|---|---|
| In-hospital death | n = 193,391 | n = 339,234 | n = 71,218 | n = 29,977 |
| 18–39 | 10.22% (2490/24,365) | 16.78% (8275/49,312) | 10.85% (848/7816) | 9.65% (257/2663) |
| 40–59 | 19.66% (12,353/62,846) | 27.53% (36,698/133,280) | 24.64% (3333/13,528) | 21.06% (937/4449) |
| 60–79 | 42.10% (32,267/76,635) | 48.11% (61,042/126,891) | 38.17% (10,941/28,662) | 29.26% (3468/11,854) |
| ≥80 | 61.05% (18,038/29,545) | 64.59% (19,216/29,751) | 49.56% (10,512/21,212) | 35.10% (3865/11,011) |
| IMV | n = 171,605 | n = 307,010 | n = 63,026 | n = 26,440 |
| 18–39 | 11.80% (2561/21,696) | 16.86% (7554/44,798) | 10.63% (721/6781) | 10.03% (228/2274) |
| 40–59 | 16.50% (9227/55,918) | 22.06% (26,657/120,840) | 18.57% (2218/11,946) | 16.25% (626/3852) |
| 60–79 | 26.42% (17,959/67,964) | 29.46% (33,782/114,689) | 22.88% (5825/25,463) | 17.37% (1819/10,474) |
| ≥80 | 25.78% (6710/26,027) | 25.05% (6683/26,683) | 17.48% (3292/18,836) | 13.14% (1293/9840) |
| NIV | n = 171,605 | n = 307,010 | n = 63,026 | n = 26,440 |
| 18–39 | 47.14% (10,227/21,696) | 63.16% (28,294/44,798) | 33.30% (2258/6781) | 29.38% (668/2274) |
| 40–59 | 54.14% (30,274/55,918) | 63.45% (76,673/120,840) | 48.63% (5809/11,946) | 41.07% (1582/3852) |
| 60–79 | 52.65% (35,785/67,964) | 59.29% (67,995/114,689) | 54.46% (13,867/25,463) | 51.87% (5433/10,474) |
| ≥80 | 56.76% (14,773/26,027) | 63.65% (16,984/26,683) | 62.83% (11,835/18,836) | 59.33% (5838/9840) |
| ICU | n = 178,350 | n = 312,958 | n = 65,604 | n = 27,699 |
| 18–39 | 27.38% (6197/22,633) | 31.04% (14,172/45,656) | 26.17% (1880/7183) | 25.80% (626/2426) |
| 40–59 | 33.76% (19,664/58,253) | 35.94% (44,275/123,201) | 37.52% (4681/12,476) | 34.29% (1402/4089) |
| 60–79 | 44.08% (31,066/70,482) | 42.31% (49,435/116,829) | 41.55% (11,000/26,472) | 35.51% (3895/10,968) |
| ≥80 | 45.81% (12,360/26,982) | 38.02% (10,368/27,272) | 37.55% (7312/19,473) | 32.60% (3330/10,216) |
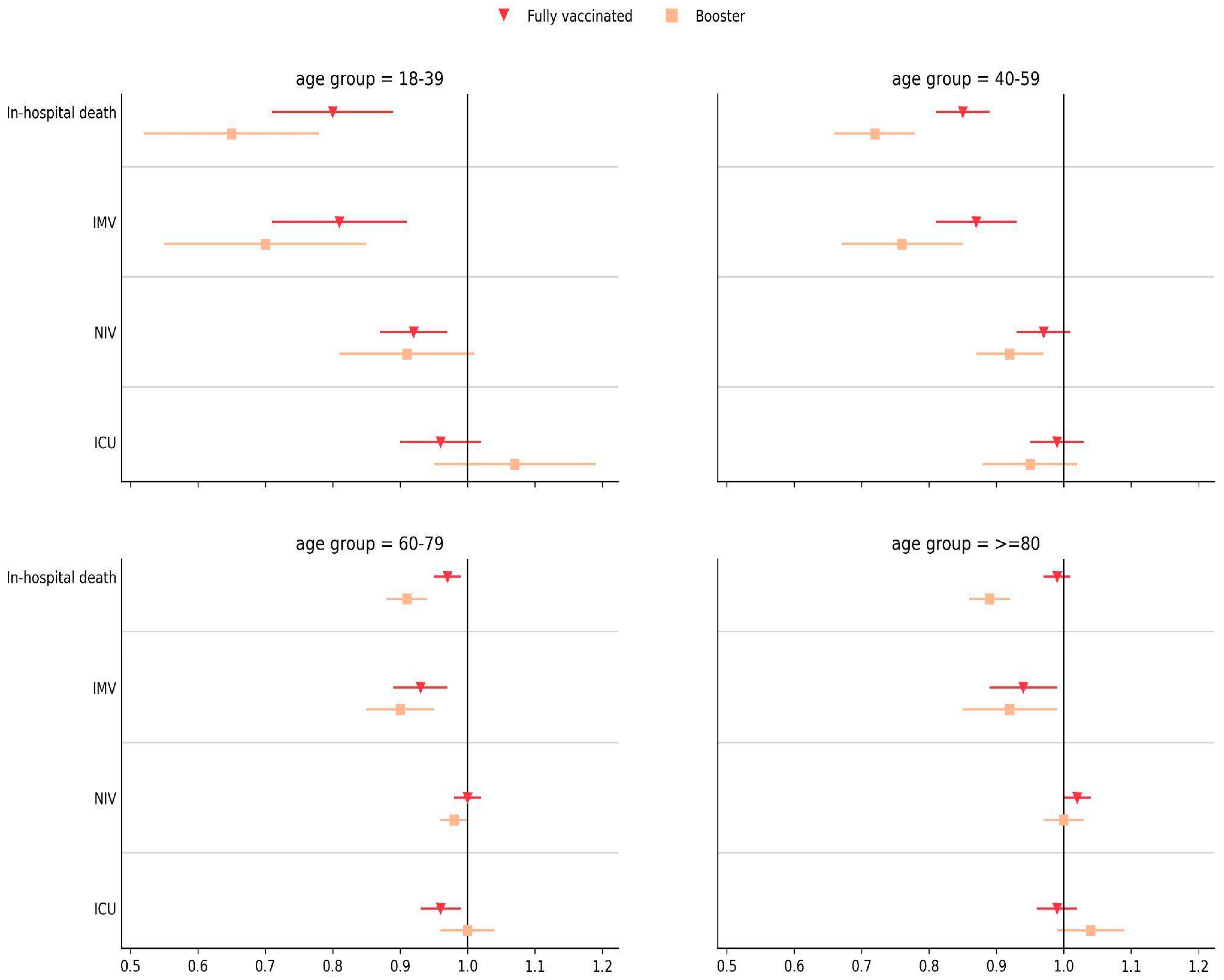
| Age Group | Fully Vaccinated × Unvaccinated/Partially Vaccinated (W3) | Booster Vaccinated × Unvaccinated/Partially Vaccinated (W4) |
|---|---|---|
| 18–39 | 0.83 (0.73–0.94), p < 0.005 | 0.73 (0.54–0.98), p = 0.034 |
| 40–59 | 0.89 (0.84–0.95), p < 0.001 | 0.59 (0.52–0.68), p < 0.001 |
| 60–79 | 0.97 (0.94–1.00), p = 0.057 | 0.77 (0.71–0.83), p < 0.001 |
| ≥80 | 1.00 (0.97–1.03), p = 0.796 | 0.70 (0.65–0.75), p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hojo-Souza, N.S.; Jassat, W.; Guidoni, D.L.; de Souza, F.S.H. Risks of Adverse Outcomes for Hospitalized COVID-19 Patients during the Four Waves in Brazil According to SARS-CoV-2 Variants, Age Group, and Vaccine Status. Viruses 2023, 15, 1997. https://doi.org/10.3390/v15101997
Hojo-Souza NS, Jassat W, Guidoni DL, de Souza FSH. Risks of Adverse Outcomes for Hospitalized COVID-19 Patients during the Four Waves in Brazil According to SARS-CoV-2 Variants, Age Group, and Vaccine Status. Viruses. 2023; 15(10):1997. https://doi.org/10.3390/v15101997
Chicago/Turabian StyleHojo-Souza, Natália Satchiko, Waasila Jassat, Daniel Ludovico Guidoni, and Fernanda Sumika Hojo de Souza. 2023. "Risks of Adverse Outcomes for Hospitalized COVID-19 Patients during the Four Waves in Brazil According to SARS-CoV-2 Variants, Age Group, and Vaccine Status" Viruses 15, no. 10: 1997. https://doi.org/10.3390/v15101997