
Emergence of Crimean–Congo Hemorrhagic Fever Virus in Eastern Senegal in 2022
 , , , , , , , , , add
Show full author list
, , , , , , , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
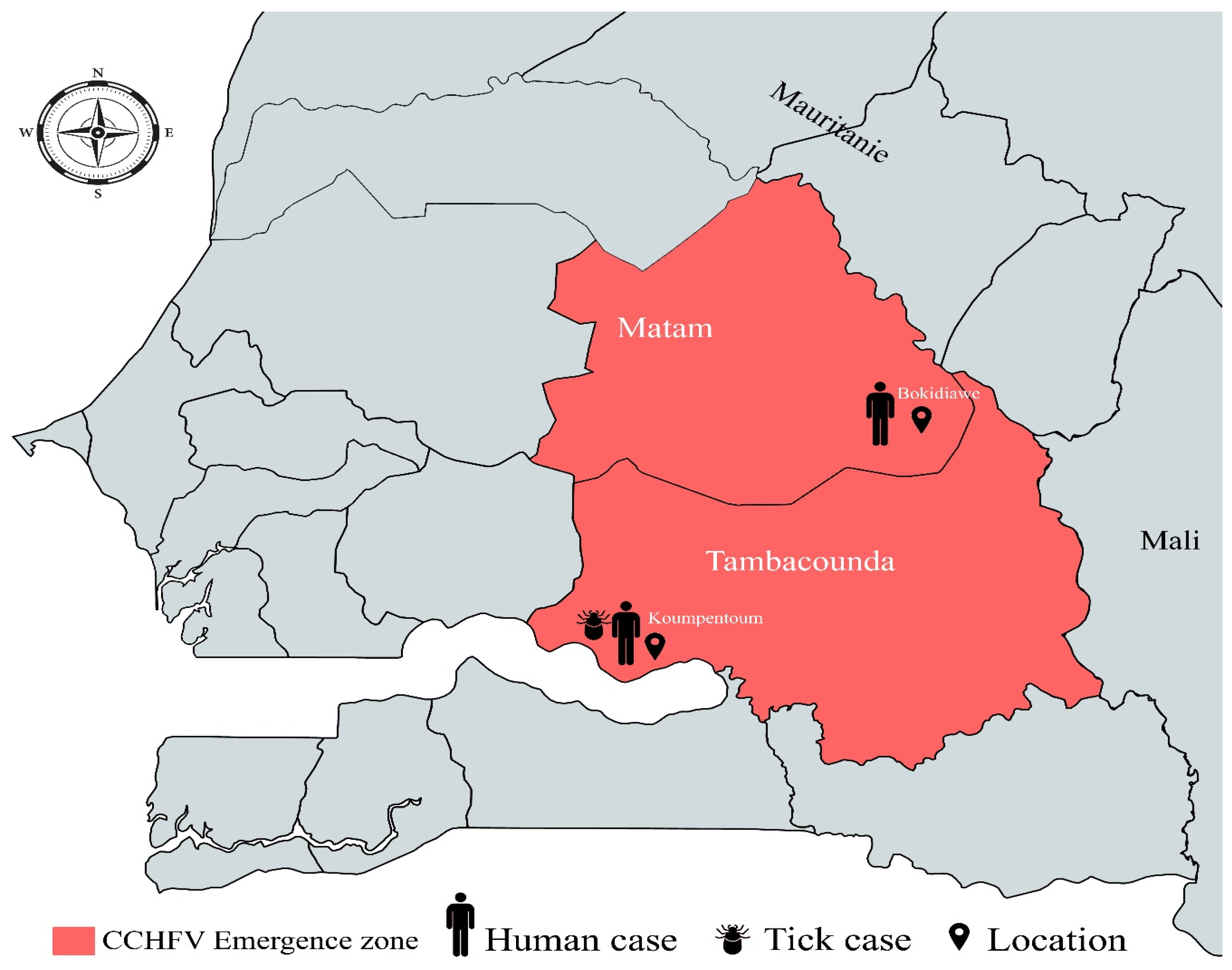
2.1. Study Area
2.2. Human Serum Collection
2.3. Animal Sample Collection
2.4. Tick Collection
2.5. Laboratory Tests
2.6. Viral Genome Sequencing and Phylogenetic Analyses
3. Results
3.1. Human Case Presentation
- Detection of one Human case in Koumpentoum, Tambacounda region
- Detection of one Human case in Bokidiawe, Matam region
3.2. Detection of CCHFV IgG Antibodies in Animals
3.3. Viral Detection in Ticks
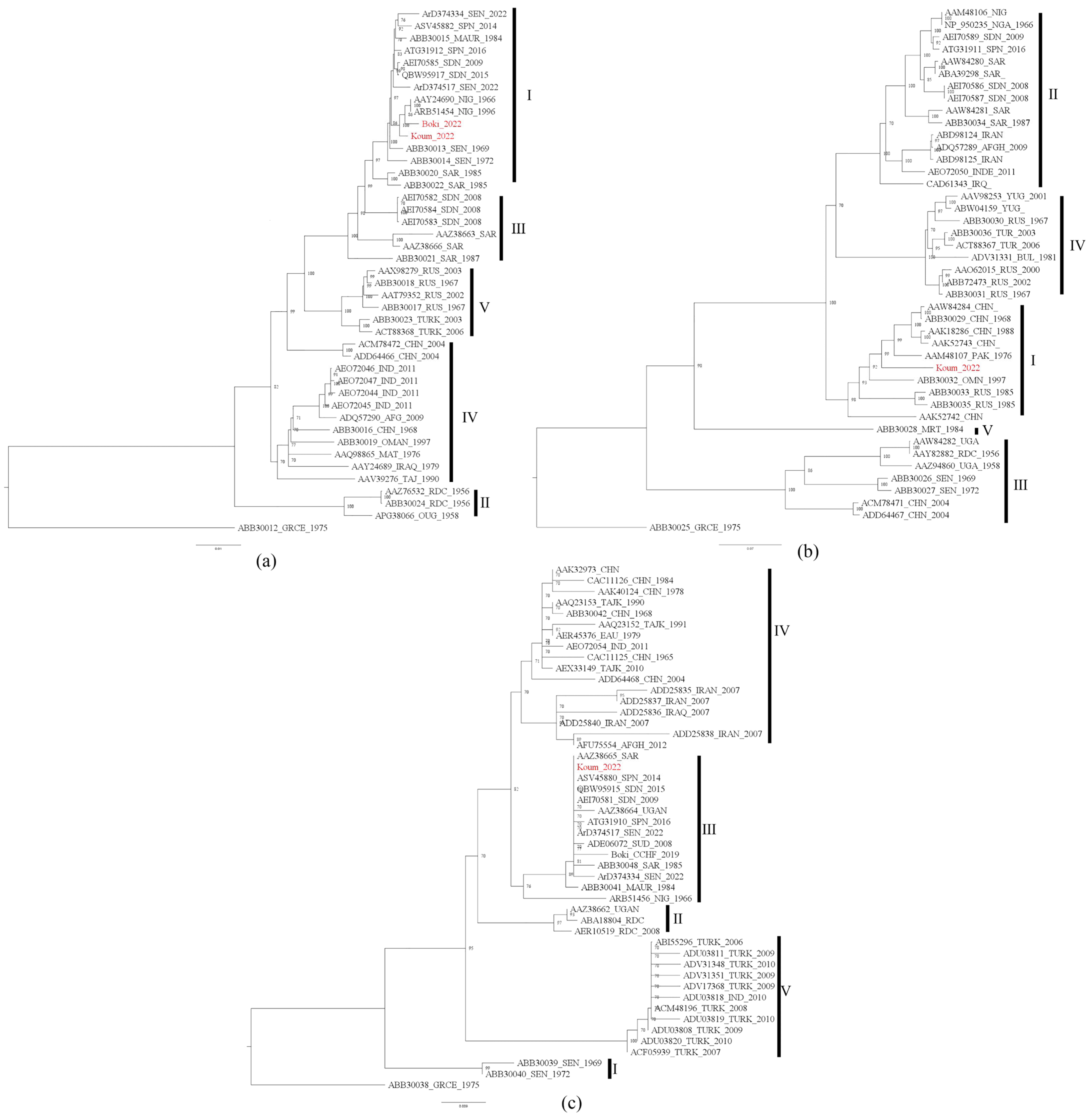
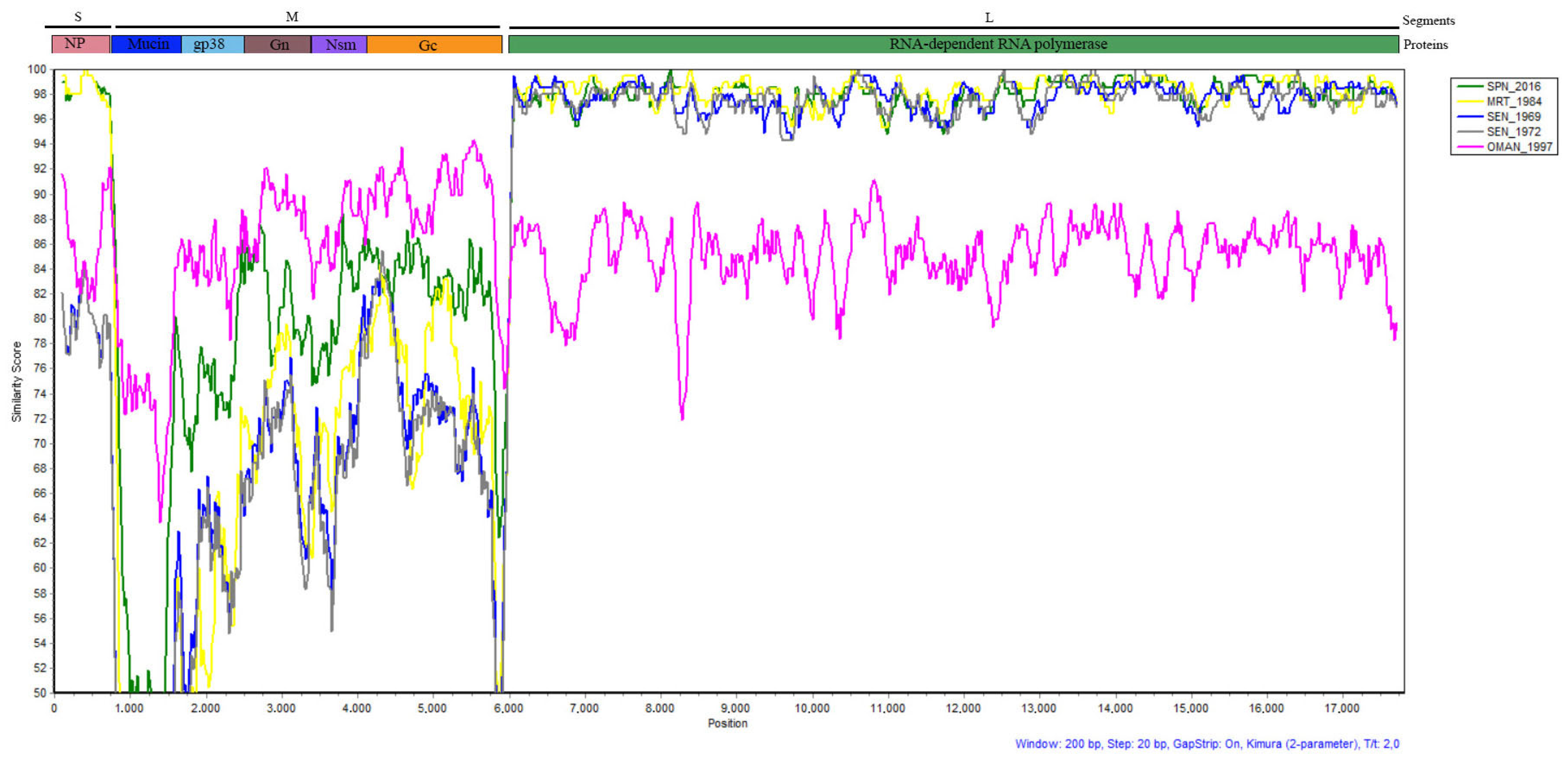
3.4. Phylogenetic Analyses
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ergonul, O.; Whitehouse, C.A. Crimean-Congo Hemorrhagic Fever: A Global Perspective; Springer: Berlin/Heidelberg, Germany, 2007. [Google Scholar] [CrossRef]
- Bente, D.A.; Forrester, N.L.; Watts, D.M.; McAuley, A.J.; Whitehouse, C.A.; Bray, M. Crimean-Congo Hemorrhagic Fever: History, Epidemiology, Pathogenesis, Clinical Syndrome and Genetic Diversity. Antivir. Res. 2013, 100, 159–189. [Google Scholar] [CrossRef]
- International Committee on Taxonomy of Viruses (ICTV). Virus Taxonomy: The Classification and Nomenclature of Viruses—The Online (10th) Report of the ICTV. Available online: https://talk.ictvonline.org/ictv-reports/ictv_online_report/ (accessed on 4 May 2022).
- Whitehouse, C.A. Crimean-Congo Hemorrhagic Fever. Antivir. Res. 2004, 64, 145–160. [Google Scholar] [CrossRef]
- Morikawa, S.; Saijo, M.; Kurane, I. Recent Progress in Molecular Biology of Crimean–Congo Hemorrhagic Fever. Comp. Immunol. Microbiol. Infect. Dis. 2007, 30, 375–389. [Google Scholar] [CrossRef]
- Nasirian, H. New Aspects about Crimean-Congo Hemorrhagic Fever (CCHF) Cases and Associated Fatality Trends: A Global Systematic Review and Meta-Analysis. Comp. Immunol. Microbiol. Infect. Dis. 2020, 69, 101429. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention Signs and Symptoms. Crimean-Congo Hemorrhagic Fever (CCHF). Available online: https://www.cdc.gov/vhf/crimean-congo/symptoms/index.html (accessed on 14 June 2022).
- Hewson, R.; Gmyl, A.; Gmyl, L.; Smirnova, S.E.; Karganova, G.; Jamil, B.; Hasan, R.; Chamberlain, J.; Clegg, C. Evidence of Segment Reassortment in Crimean-Congo Haemorrhagic Fever Virus. J. Gen. Virol. 2004, 85, 3059–3070. [Google Scholar] [CrossRef]
- Shayan, S.; Bokaean, M.; Shahrivar, M.R.; Chinikar, S. Crimean-Congo Hemorrhagic Fever. Lab. Med. 2015, 46, 180–189. [Google Scholar] [CrossRef]
- Papa, A.; Marklewitz, M.; Paraskevopoulou, S.; Garrison, A.R.; Alkhovsky, S.V.; Avšič-Županc, T.; Bente, D.A.; Bergeron, É.; Burt, F.; Di Paola, N.; et al. History and Classification of Aigai Virus (Formerly Crimean–Congo Haemorrhagic Fever Virus Genotype VI). J. Gen. Virol. 2022, 103, 001734. [Google Scholar] [CrossRef]
- Saluzzo, J.-F.; Camicas, J.-L.; Chartier, C.; Martinez, D.; Digoutte, J.-P. Le Virus de La Fièvre Hémorragique de Crimée-Congo (CCHF) En Mauritanie. Cah.-ORSTOM Entomol. Méd. Parasitol. 1986, 24, 129–137. [Google Scholar]
- Dieng, I.; Barry, M.A.; Diagne, M.M.; Diop, B.; Ndiaye, M.; Faye, M.; Ndione, M.H.D.; Dieng, M.M.; Bousso, A.; Fall, G.; et al. Detection of Crimean Congo Haemorrhagic Fever Virus in North-Eastern Senegal, Bokidiawé 2019. Emerg. Microbes Infect. 2020, 9, 2485. [Google Scholar] [CrossRef]
- Mhamadi, M.; Badji, A.; Dieng, I.; Gaye, A.; Ndiaye, E.H.; Ndiaye, M.; Mhamadi, M.; Toure, C.T.; Barry, A.; Ndiaye, O.; et al. Multiple Genotypes of Crimean-Congo Hemorrhagic Fever Virus Detected in Ticks during a One Health Survey in Agnam, Northeastern Senegal. Emerg. Microbes Infect. 2022, 11, 2711–2714. [Google Scholar] [CrossRef]
- Zeller, H.G.; Cornet, J.-P.; Diop, A.; Camicas, J.-L. Crimean—Congo Hemorrhagic Fever in Ticks (Acari: Ixodidae) and Ruminants: Field Observations of an Epizootic in Bandia, Senegal (1989–1992). J. Med. Entomol. 1997, 34, 511–516. [Google Scholar] [CrossRef]
- Bob, N.S.; Barry, M.A.; Diagne, M.M.; Faye, M.; Ndione, M.H.D.; Diallo, A.; Diop, M.; Diop, B.; Faye, O.; Loucoubar, C.; et al. Detection of Rift Valley Fever Virus Lineage H From South Africa Through the Syndromic Sentinel Surveillance Network in Senegal. Open Forum Infect. Dis. 2021, 9, ofab655. [Google Scholar] [CrossRef]
- Dia, N.; Diene Sarr, F.; Thiam, D.; Faye Sarr, T.; Espié, E.; OmarBa, I.; Coly, M.; Niang, M.; Richard, V. Influenza-Like Illnesses in Senegal: Not Only Focus on Influenza Viruses. PLoS ONE 2014, 9, e93227. [Google Scholar] [CrossRef]
- Hoogstraal, H.; Hoogstraal, H. African Ixodoidea. Ticks of the Sudan (with Special Reference to Equatoria Province and with Preliminary Reviews Pf the Genera Boophilus, Margaropus, and Hyalomma). Afr. Ixodoidea l Ticks Sudan 1956, 1, 1–1105. [Google Scholar]
- Walker, A.; Bouattour, A.; Camicas, J.-L.; Estrada-Peña, A.; Horak, I.; Latif, A.; Pegram, R.G.; Preston, P.M. Ticks of Domestic Animals in Africa: A Guide to Identification of Species; Bioscience Reports: Edinburgh, UK, 2014; ISBN 978-0-9545173-0-4. [Google Scholar]
- Weidmann, M.; Faye, O.; Faye, O.; Wahed, A.A.E.; Batejat, C.; Manugerra, J.C.; Adjami, A.; Niedrig, M.; Hufert, F.T.; Sall, A.A. Development of Mobile Laboratory for Viral Hemorrhagic Fever Detection in Africa. J. Infect. Dis. 2018, 218, 1622–1630. [Google Scholar] [CrossRef]
- Mhamadi, M.; Badji, A.; Dieng, I.; Gaye, A.; Ndiaye, E.H.; Ndiaye, M.; Mhamadi, M.; Touré, C.T.; Mbaye, M.R.; Barry, M.A.; et al. Crimean–Congo Hemorrhagic Fever Virus Survey in Humans, Ticks, and Livestock in Agnam (Northeastern Senegal) from February 2021 to March 2022. Trop. Med. Infect. Dis. 2022, 7, 324. [Google Scholar] [CrossRef]
- Katoh, K.; Misawa, K.; Kuma, K.; Miyata, T. MAFFT: A Novel Method for Rapid Multiple Sequence Alignment Based on Fast Fourier Transform. Nucleic Acids Res. 2002, 30, 3059–3066. [Google Scholar] [CrossRef]
- Nguyen, L.-T.; Schmidt, H.A.; von Haeseler, A.; Minh, B.Q. IQ-TREE: A Fast and Effective Stochastic Algorithm for Estimating Maximum-Likelihood Phylogenies. Mol. Biol. Evol. 2015, 32, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Rambaut, A. FigTree; Version 1.3.1; Institute of Evolutionary Biology, University of Edinburgh: Edinburgh, UK, 2010; Available online: http://tree.bio.ed.ac.uk/software/figtree/ (accessed on 28 September 2023).
- Lole, K.; Bollinger, R.; Paranjape, R.; Gadkari, D.; Kulkarni, S.; Novak, N.; Ingersoll, R.; Sheppard, H.; Ray, S. Full-Length Human Immunodeficiency Virus Type 1 Genomes from Subtype C-Infected Seroconverters in India, with Evidence of Intersubtype Recombination. J. Virol. 1999, 73, 152–160. [Google Scholar] [CrossRef]
- Wilson, M.L.; Gonzalez, J.-P.; LeGuenno, B.; Cornet, J.-P.; Guillaud, M.; Calvo, M.-A.; Digoutte, J.-P.; Camicas, J.-L. Epidemiology of Crimean-Congo Hemorrhagic Fever in Senegal: Temporal and Spatial Patterns. In Hemorrhagic Fever with Renal Syndrome, Tick- and Mosquito-Borne Viruses; Calisher, C.H., Ed.; Springer Vienna: Vienna, Austria, 1990; pp. 323–340. ISBN 978-3-211-82217-3. [Google Scholar]
- World Health Organization. Regional Office for Africa Weekly Bulletin on Outbreak and Other Emergencies: Week 33: 8–14 August 2022. Available online: https://iris.who.int/bitstream/handle/10665/361771/OEW33-0814082022.pdf?sequence=1&isAllowed=y (accessed on 28 September 2023).
- Nasirian, H. Ticks Infected with Crimean-Congo Hemorrhagic Fever Virus (CCHFV): A Decision Approach Systematic Review and Meta-Analysis Regarding Their Role as Vectors. Travel Med. Infect. Dis. 2022, 47, 102309. [Google Scholar] [CrossRef]
- Camicas, J.-L.; Cornet, J.-P.; Gonzalez, J.-P.; Wilson, M.; Adam, F.; Zeller, H. La Fièvre Hémorragique de Crimée-Congo Au Sénégal: Dernières Données Sur l’écologie Du Virus CCHF. Bull. Soc. Pathol. Exot. 1994, 87, 11–16. [Google Scholar] [PubMed]
- Gueye, A.; Mbengue, M.; Diouf, A. Ticks and hemoparasitic diseases in cattle in Senegal. IV. The southern Sudan area. Rev. Elev. Med. Vet. Pays Trop. 1990, 42, 517–528. [Google Scholar] [CrossRef]
- Logan, T.M.; Linthicum, K.J.; Bailey, C.L.; Watts, D.M.; Moulton, J.R. Experimental Transmission of Crimean-Congo Hemorrhagic Fever Virus by Hyalomma Truncatum Koch. Am. J. Trop. Med. Hyg. 1989, 40, 207–212. [Google Scholar] [CrossRef]
- Shepherd, A.J.; Swanepoel, R.; Cornel, A.J.; Mathee, O. Experimental Studies on the Replication and Transmission of Crimean-Congo Hemorrhagic Fever Virus in Some African Tick Species. Am. J. Trop. Med. Hyg. 1989, 40, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Nasirian, H. Crimean-Congo Hemorrhagic Fever (CCHF) Seroprevalence: A Systematic Review and Meta-Analysis. Acta Trop. 2019, 196, 102–120. [Google Scholar] [CrossRef]
- Mangombi, J.; Roqueplo, C.; Sambou, M.; Dahmani, M.; Mediannikov, O.; Comtet, L.; Davoust, B. Seroprevalence of Crimean-Congo Hemorrhagic Fever in Domesticated Animals in Northwestern Senegal. In Vector-Borne Zoonotic Diseases; Mary Ann Liebert, Inc.: Larchmont, NY, USA, 2020; Volume 20. [Google Scholar] [CrossRef]
- Brandt, M.; Hiernaux, P.; Rasmussen, K.; Tucker, C.J.; Wigneron, J.-P.; Diouf, A.A.; Herrmann, S.M.; Zhang, W.; Kergoat, L.; Mbow, C.; et al. Changes in Rainfall Distribution Promote Woody Foliage Production in the Sahel. Commun. Biol. 2019, 2, 133. [Google Scholar] [CrossRef]
- Brandt, M.; Mbow, C.; Diouf, A.A.; Verger, A.; Samimi, C.; Fensholt, R. Ground- and Satellite-Based Evidence of the Biophysical Mechanisms behind the Greening Sahel. Glob. Chang. Biol. 2015, 21, 1610–1620. [Google Scholar] [CrossRef]
- Food and Agriculture Organization of the United Nations. Characteristics, Patterns and Drivers of Rural Migration in Senegal; FAO: Rome, Italy, 2020; ISBN 978-92-5-131123-3. [Google Scholar]
- Estrada-Peña, A.; Vatansever, Z.; Gargili, A.; Buzgan, T. An Early Warning System for Crimean-Congo Haemorrhagic Fever Seasonality in Turkey Based on Remote Sensing Technology. Geospat. Health 2007, 2, 127. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site | Species | Number of Samples | Number of CCHFV-Positive Samples (%) |
|---|---|---|---|
| Sheep | 73 | 27 (36.98) | |
| Bokidiawe | Goats | 22 | 16 (72.72) |
| Total | 95 | 43 (45.26) | |
| Sheep | 18 | 2 (11.11) | |
| Koumpentoum | Goats | 57 | 2 (3.5) |
| Total | 75 | 7 (9.33) |
| Species | Bokidiawe | Koumpentoum | Total | |||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| Hyalomma impeltatum | 74 | 74.7 | 0 | 0.0 | 74 | 6.4 |
| Hyalomma marginatum rufipes | 2 | 2.0 | 344 * | 32.6 | 346 | 30.0 |
| Hyalomma truncatum | 0 | 0.0 | 134 | 12.7 | 134 | 11.6 |
| Others § | 23 | 23.2 | 577 | 54.7 | 600 | 52.0 |
| Total | 99 | 1055 | 1154 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sene, O.; Sagne, S.N.; Ngom, D.; Diagne, M.M.; Badji, A.; Khoulé, A.; Ndiaye, E.H.; Sankhe, S.; Loucoubar, C.; Diallo, M.; et al. Emergence of Crimean–Congo Hemorrhagic Fever Virus in Eastern Senegal in 2022. Viruses 2024, 16, 315. https://doi.org/10.3390/v16020315
Sene O, Sagne SN, Ngom D, Diagne MM, Badji A, Khoulé A, Ndiaye EH, Sankhe S, Loucoubar C, Diallo M, et al. Emergence of Crimean–Congo Hemorrhagic Fever Virus in Eastern Senegal in 2022. Viruses. 2024; 16(2):315. https://doi.org/10.3390/v16020315
Chicago/Turabian StyleSene, Ousseynou, Samba Niang Sagne, Déthié Ngom, Moussa Moise Diagne, Aminata Badji, Aliou Khoulé, El Hadji Ndiaye, Safietou Sankhe, Cheikh Loucoubar, Mawlouth Diallo, and et al. 2024. "Emergence of Crimean–Congo Hemorrhagic Fever Virus in Eastern Senegal in 2022" Viruses 16, no. 2: 315. https://doi.org/10.3390/v16020315