
Risk Factors Associated with Opportunistic Infections among People Living with HIV/AIDS and Receiving an Antiretroviral Therapy in Gabon, Central Africa

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sampling
2.2. Ethical Consideration
2.3. Sampling for HIV Viral Load and CD4 Counts
2.4. Diagnosis of Other Pathogenic (Viral, Parasitic, and Bacteriological) Infections
2.5. Occurrence of Opportunistic Infections
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Patients
3.2. Prevalence, Distribution, and Spectrum of Opportunistic Infections
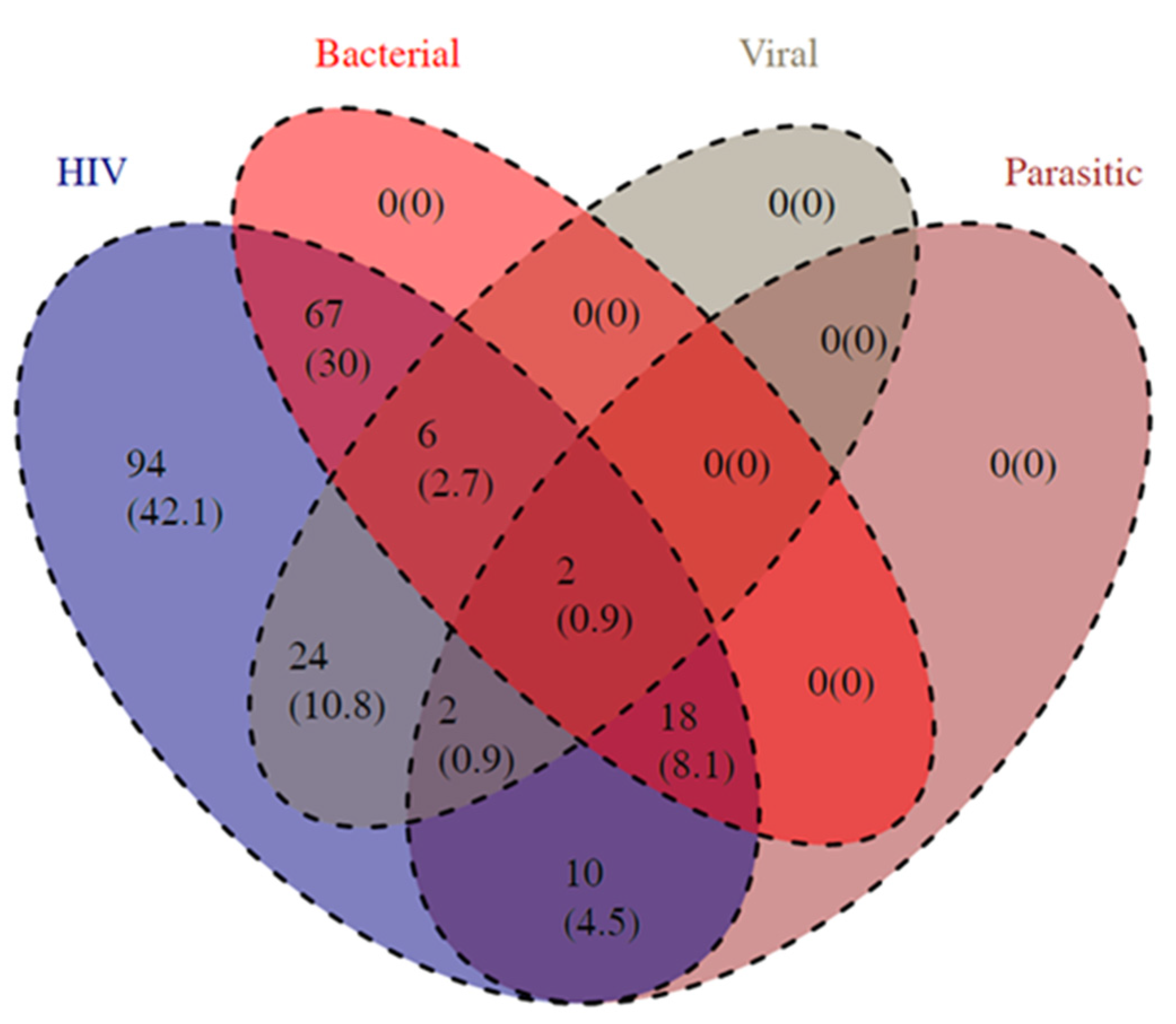
3.3. Different Combinations of Opportunistic Infections among People Living with HIV
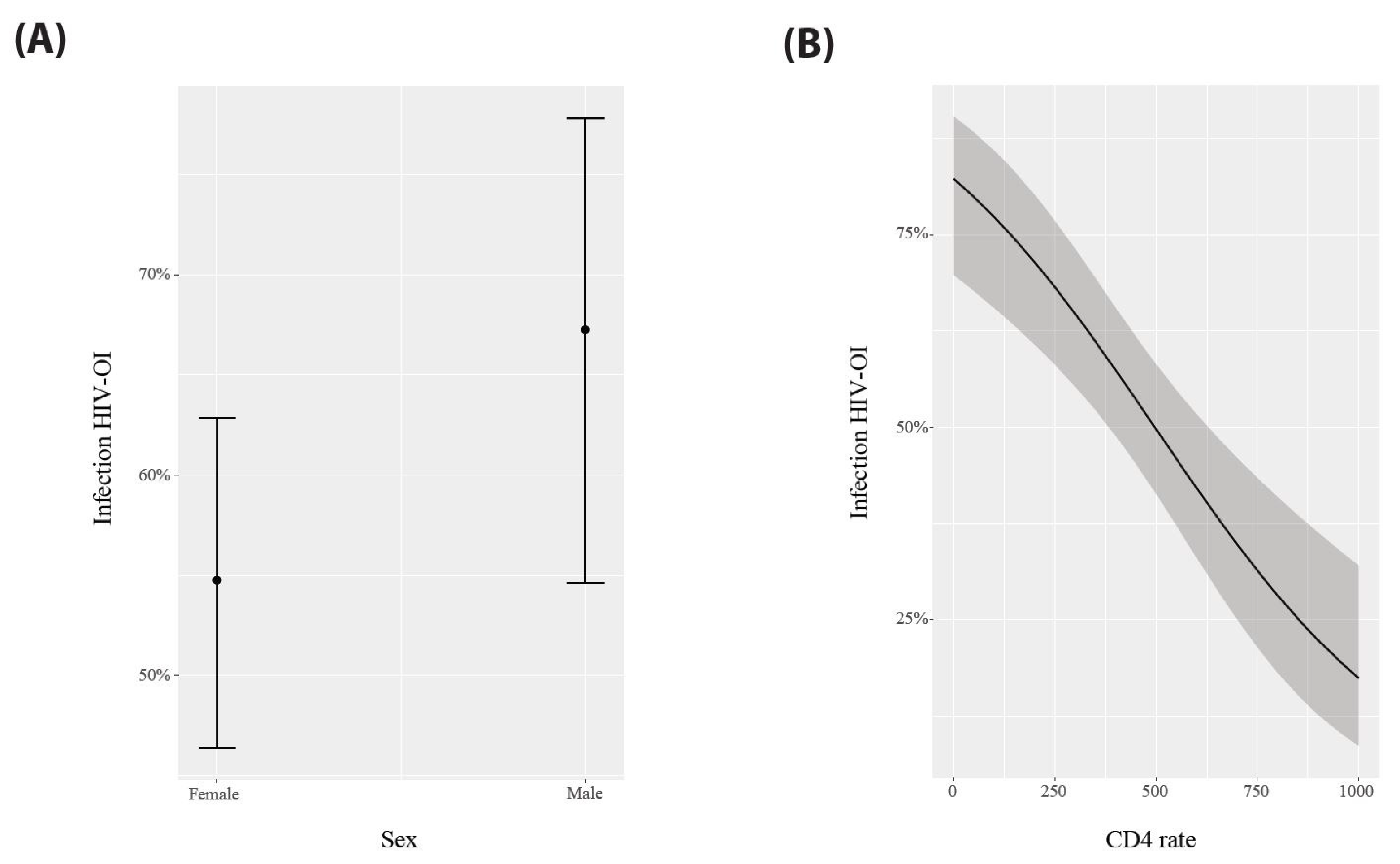
3.4. Risk Factors Associated with the Occurrence of Opportunistic Infections
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Woldegeorgis, B.Z.; Kerbo, A.A.; Obsa, M.S.; Mokonnon, T.M. A systematic review and meta-analysis of antimicrobial resistance knowledge, attitudes, and practices: Current evidence to build a strong national antimicrobial drug resistance narrative in Ethiopia. PLoS ONE 2023, 18, e0287042. [Google Scholar] [CrossRef] [PubMed]
- Palella, F.J., Jr.; Baker, R.K.; Moorman, A.C.; Chmiel, J.S.; Wood, K.C.; Brooks, J.T.; Holmberg, S.D. Mortality in the highly active antiretroviral therapy era: Changing causes of death and disease in the HIV outpatient study. J. Acquir. Immune Defic. Syndr. 2006, 43, 27–34. [Google Scholar] [CrossRef]
- Mirani, G.; Williams, P.L.; Chernoff, M.; Abzug, M.J.; Levin, M.J.; Seage, G.R., 3rd; Oleske, J.M.; Purswani, M.U.; Hazra, R.; Traite, S.; et al. Changing Trends in Complications and Mortality Rates Among US Youth and Young Adults with HIV Infection in the Era of Combination Antiretroviral Therapy. Clin. Infect. Dis. 2015, 61, 1850–1861. [Google Scholar] [CrossRef] [PubMed]
- Arefaine, Z.G.; Abebe, S.; Bekele, E.; Adem, A.; Adama, Y.; Brockmeyer, N.H.; Coenenberg, J.; Potthoff, A.; Gebremeskel, T.G. Incidence and predictors of HIV related opportunistic infections after initiation of highly active antiretroviral therapy at Ayder Referral Hospital, Mekelle, Ethiopia: A retrospective single centered cohort study. PLoS ONE 2020, 15, e0229757. [Google Scholar] [CrossRef] [PubMed]
- Solomon, F.B.; Angore, B.N.; Koyra, H.C.; Tufa, E.G.; Berheto, T.M.; Admasu, M. Spectrum of opportunistic infections and associated factors among people living with HIV/AIDS in the era of highly active anti-retroviral treatment in Dawro Zone hospital: A retrospective study. BMC Res. Notes 2018, 11, 604. [Google Scholar] [CrossRef] [PubMed]
- Dagnaw Tegegne, K.; Cherie, N.; Tadesse, F.; Tilahun, L.; Kassaw, M.W.; Biset, G. Incidence and Predictors of Opportunistic Infections among Adult HIV Infected Patients on Anti-Retroviral Therapy at Dessie Comprehensive Specialized Hospital, Ethiopia: A Retrospective Follow-Up Study. HIV AIDS 2022, 14, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Paton, N.I.; Ditangco, R. AIDS-defining illness diagnosed within 90 days after starting highly active antiretroviral therapy among patients from the TREAT Asia HIV Observational Database. Int. J. STD AIDS 2007, 18, 446–452. [Google Scholar] [CrossRef]
- Cuvelier, M.L.; Léonard, P.; Rikir, E.; Belachew, S. When HIV gets into the brain. Rev. Med. Liege 2008, 63, 338–341. [Google Scholar]
- Niriella, M.A.; Kasturiratne, A.; Pathmeswaran, A.; De Silva, S.T.; Perera, K.R.; Subasinghe, S.; Kodisinghe, S.K.; Piyaratna, T.; Vithiya, K.; Dassanayaka, A.S.; et al. Lean non-alcoholic fatty liver disease (lean NAFLD): Characteristics, metabolic outcomes and risk factors from a 7-year prospective, community cohort study from Sri Lanka. Hepatol. Int. 2019, 13, 314–322. [Google Scholar] [CrossRef]
- Iroezindu, M.O.; Agbaji, O.O.; Daniyam, C.A.; Isiguzo, G.C.; Isichei, C.; Akanbi, M.O. Liver function test abnormalities in Nigerian patients with human immunodeficiency virus and hepatitis B virus co-infection. Int. J. STD AIDS 2013, 24, 461–467. [Google Scholar] [CrossRef]
- Putranti, A.; Asmarawati, T.P.; Rachman, B.E.; Hadi, U. Oral candidiasis as clinical manifestation of HIV/AIDS infection in Airlangga University hospital patients. IOP Conf. Ser. Earth Environ. Sci. 2018, 125, 012063. [Google Scholar] [CrossRef]
- UNAIDS. Dernières Statistiques sur L’état de L’épidémie de Sida. 13 July 2023. Available online: https://www.unaids.org/fr/resources/documents/2023/UNAIDS_FactSheet (accessed on 9 October 2023).
- EDSG. Prévalence de L’infection à VIH au Gabon. 2012. Available online: https://gabon.unfpa.org/sites/default/files/pub-pdf/EDS%20II.pdf (accessed on 9 October 2023).
- Engone-Ondo, J.D.; Mouinga-Ondémé, A.; Lékana-Douki, S.E.; Diané, A.; Mamimandjiami, A.I.; Banga, O.; Ndong-Atome, G.R.; Aghokeng, A.F. High rate of virological failure and HIV drug resistance in semi-rural Gabon and implications for dolutegravir-based regimen efficacy. J. Antimicrob. Chemother. 2021, 76, 1051–1056. [Google Scholar] [CrossRef]
- WHO. Update of Recommendations on First- and Second-Line Antiretroviral Regimens; WHO: Geneva, Switzerland, 2019.
- Okome-Nkoumou, M.; Guiyedi, V.; Ondounda, M.; Efire, N.; Clevenbergh, P.; Dibo, M.; Dzeing-Ella, A. Opportunistic diseases in HIV-infected patients in Gabon following the administration of highly active antiretroviral therapy: A retrospective study. Am. J. Trop. Med. Hyg. 2014, 90, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Mouinga-Ondémé, A.; Boundenga, L.; Koumba Koumba, I.P.; Idam Mamimandjiami, A.; Diané, A.; Engone-Ondo, J.D.; Djuicy, D.D.; Sica, J.; Mombo, L.E.; Gessain, A.; et al. Human T-Lymphotropic virus type 1 and human immunodeficiency virus co-infection in rural Gabon. PLoS ONE 2022, 17, e0271320. [Google Scholar] [CrossRef] [PubMed]
- Liégeois, F.; Vella, C.; Eymard-Duvernay, S.; Sica, J.; Makosso, L.; Mouinga-Ondémé, A.; Mongo, A.D.; Boué, V.; Butel, C.; Peeters, M.; et al. Virological failure rates and HIV-1 drug resistance patterns in patients on first-line antiretroviral treatment in semirural and rural Gabon. J. Int. AIDS Soc. 2012, 15, 17985. [Google Scholar] [CrossRef]
- Bivigou-Mboumba, B.; Amougou-Atsama, M.; Zoa-Assoumou, S.; M’Boyis Kamdem, H.; Nzengui-Nzengui, G.F.; Ndojyi-Mbiguino, A.; Njouom, R.; François-Souquière, S. Hepatitis B infection among HIV infected individuals in Gabon: Occult hepatitis B enhances HBV DNA prevalence. PLoS ONE 2018, 13, e0190592. [Google Scholar] [CrossRef]
- Van Der Pol, B.; Ferrero, D.V.; Buck-Barrington, L.; Hook, E.W.; Lenderman, C.; Quinn, T.C.; Gaydos, C.A.; Lovchik, J.C.; Schachter, J.; Moncada, J.; et al. Multicenter Evaluation of the BDProbeTec ET System for Detection of Chlamydia trachomatis and Neisseria gonorrhoeae in Urine Specimens, Female Endocervical Swabs, and Male Urethral Swabs. J. Clin. Microbiol. 2001, 39, 1008–1016. [Google Scholar] [CrossRef]
- Barton, K. MuMIn: Multi-Model Inference. 2009. Available online: http://r-forge.r-project.org/projects/mumin/ (accessed on 30 January 2009).
- Burnham, K.P.; Anderson, D.R. Multimodel Inference: Understanding AIC and BIC in Model Selection. Sociol. Methods Res. 2004, 33, 261–304. [Google Scholar] [CrossRef]
- Mongo-Delis, A.; Mombo, L.E.; Mickala, P.; Bouassa, W.; Bouedy, W.S.; M’Batchi, B.; Bisseye, C. Factors associated with adherence to ARV treatment in people living with HIV/AIDS in a rural area (Koula-Moutou) in East Gabon. Afr. J. AIDS Res. 2019, 18, 51–57. [Google Scholar] [CrossRef]
- Weldearegawi, T.Z.; Gerensea, H.; Berihu, H.; Gidey, G.; Welearegay, M.Z. The magnitude of opportunistic infections and associated factors in HIV-infected adults on antiretroviral therapy in southern zone Tigray, Ethiopia: A cross-sectional study. Pan Afr. Med. J. 2020, 35, 126. [Google Scholar] [CrossRef]
- Girma, D.; Dejene, H.; Adugna Geleta, L.; Tesema, M.; Bati, F. Time to occurrence, predictors, and patterns of opportunistic infections incidence among HIV-positive patients attending Antiretroviral Therapy Clinic of Salale University Comprehensive Specialized Hospital: A retrospective cohort study. Medicine 2022, 101, e29905. [Google Scholar] [CrossRef] [PubMed]
- Charleine, M.B.; Bridy, M.D.; Coella, M.J.; Marion, N.O.M.; Magalie, E.M.; Michelle, N.O.G.; Philomene, K.N.; Marielle, B.A. Adverse effects related to HAART in Gabonese PLHIV: Frequency, severity and relationship with observance. Health Sci. Dis. 2023, 24, 16–23. [Google Scholar]
- Fite, M.B.; Aga, D.J. Spectrum of Opportunistic Disease and Associated Factors among Patients Attending ART Clinic, Nekemte Specialized Hospital, Western Ethiopia. bioRxiv 2020. [Google Scholar] [CrossRef]
- Mitiku, H.; Weldegebreal, F.; Teklemariam, Z. Magnitude of opportunistic infections and associated factors in HIV-infected adults on antiretroviral therapy in eastern Ethiopia. HIV AIDS 2015, 7, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Moges, N.A.; Kassa, G.M.; Boneya, D.J. Rate of HIV transmission and associated factors among HIV-exposed infants in selected health facilities of East and West Gojjam Zones, Northwest Ethiopia; retrospective cohort study. BMC Infect. Dis. 2017, 17, 475. [Google Scholar] [CrossRef] [PubMed]
- Damtie, D.; Yismaw, G.; Woldeyohannes, D.; Anagaw, B. Common opportunistic infections and their CD4 cell correlates among HIV-infected patients attending at antiretroviral therapy clinic of Gondar University Hospital, Northwest Ethiopia. BMC Res. Notes 2013, 6, 534. [Google Scholar] [CrossRef]
- Dereje, N.; Moges, K.; Nigatu, Y.; Holland, R. Prevalence and Predictors of Opportunistic Infections among HIV Positive Adults on Antiretroviral Therapy (On-ART) versus Pre-ART in Addis Ababa, Ethiopia: A Comparative Cross-Sectional Study. HIV AIDS 2019, 11, 229–237. [Google Scholar] [CrossRef]
- Sun, H.Y.; Chen, M.Y.; Hsieh, S.M.; Sheng, W.H.; Chang, S.Y.; Hsiao, C.F.; Hung, C.C.; Chang, S.C. Changes in the clinical spectrum of opportunistic illnesses in persons with HIV infection in Taiwan in the era of highly active antiretroviral therapy. Jpn. J. Infect. Dis. 2006, 59, 311–316. [Google Scholar]
- Bélard, S.; Remppis, J.; Bootsma, S.; Janssen, S.; Kombila, D.U.; Beyeme, J.O.; Rossatanga, E.G.; Kokou, C.; Osbak, K.K.; Obiang Mba, R.M.; et al. Tuberculosis Treatment Outcome and Drug Resistance in Lambaréné, Gabon: A Prospective Cohort Study. Am. J. Trop. Med. Hyg. 2016, 95, 472–480. [Google Scholar] [CrossRef]
- Nkoghe, D.; Toung Mve, M.; Nnegue, S.; Okome Nkoume, M.; Iba, B.J.; Hypolite, J.; Leonard, P.; Kendjo, E. HIV seroprevalence among tuberculosis patients in Nkembo Hospital, Libreville, Gabon. Short note. Bull. Soc. Pathol. Exot. 2005, 98, 121–122. [Google Scholar]
- Kombila, D.U.; Moussavou-Kombila, J.B.; Grobusch, M.P.; Lell, B. Clinical and laboratory features of tuberculosis within a hospital population in Libreville, Gabon. Infection 2013, 41, 737–739. [Google Scholar] [CrossRef] [PubMed]
- Stolp, S.M.; Huson, M.A.; Janssen, S.; Beyeme, J.O.; Grobusch, M.P. Tuberculosis patients hospitalized in the Albert Schweitzer Hospital, Lambaréné, Gabon-a retrospective observational study. Clin. Microbiol. Infect. 2013, 19, E499–E501. [Google Scholar] [CrossRef] [PubMed]
- Corbett, E.L.; Watt, C.J.; Walker, N.; Maher, D.; Williams, B.G.; Raviglione, M.C.; Dye, C. The growing burden of tuberculosis: Global trends and interactions with the HIV epidemic. Arch. Intern. Med. 2003, 163, 1009–1021. [Google Scholar] [CrossRef] [PubMed]
- Abe, H.; Ushijima, Y.; Bikangui, R.; Ondo, G.N.; Pemba, C.M.; Zadeh, V.R.; Mpingabo, P.I.; Ueda, H.; Agnandji, S.T.; Lell, B.; et al. Genetic Diversity of Hepatitis B and C Viruses Revealed by Continuous Surveillance from 2015 to 2021 in Gabon, Central Africa. Microorganisms 2023, 11, 2046. [Google Scholar] [CrossRef] [PubMed]
- Groc, S.; Abbate, J.L.; Le Gal, F.; Gerber, A.; Tuaillon, E.; Albert, J.L.; Nkoghé, D.; Leroy, E.M.; Roche, B.; Becquart, P. High prevalence and diversity of hepatitis B and hepatitis delta virus in Gabon. J. Viral Hepat. 2019, 26, 170–182. [Google Scholar] [CrossRef]
- Poudel, K.C.; Poudel-Tandukar, K.; Nakahara, S.; Yasuoka, J.; Jimba, M. Knowing the consequences of unprotected sex with seroconcordant partner is associated with increased safer sex intentions among HIV-positive men in Kathmandu, Nepal. J. Health Popul. Nutr. 2011, 29, 191–199. [Google Scholar] [CrossRef]
- Devarbhavi, H.; Asrani, S.K.; Arab, J.P.; Nartey, Y.A.; Pose, E.; Kamath, P.S. Global burden of liver disease: 2023 update. J. Hepatol. 2023, 79, 516–537. [Google Scholar] [CrossRef]
- Hu, J.; Liu, K.; Luo, J. HIV-HBV and HIV-HCV Coinfection and Liver Cancer Development. Cancer Treat. Res. 2019, 177, 231–250. [Google Scholar] [CrossRef]
- Rosenthal, E.; Roussillon, C.; Salmon-Céron, D.; Georget, A.; Hénard, S.; Huleux, T.; Gueit, I.; Mortier, E.; Costagliola, D.; Morlat, P.; et al. Liver-related deaths in HIV-infected patients between 1995 and 2010 in France: The Mortavic 2010 study in collaboration with the Agence Nationale de Recherche sur le SIDA (ANRS) EN 20 Mortalité 2010 survey. HIV Med. 2015, 16, 230–239. [Google Scholar] [CrossRef]
- Goehringer, F.; Bonnet, F.; Salmon, D.; Cacoub, P.; Paye, A.; Chêne, G.; Morlat, P.; May, T. Causes of Death in HIV-Infected Individuals with Immunovirologic Success in a National Prospective Survey. AIDS Res. Hum. Retroviruses 2017, 33, 187–193. [Google Scholar] [CrossRef]
- Ioannou, G.N.; Bryson, C.L.; Weiss, N.S.; Miller, R.; Scott, J.D.; Boyko, E.J. The prevalence of cirrhosis and hepatocellular carcinoma in patients with human immunodeficiency virus infection. Hepatology 2013, 57, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Srirangaraj, S.; Venkatesha, D. Opportunistic infections in relation to antiretroviral status among AIDS patients from south India. Indian J. Med. Microbiol. 2011, 29, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Dembelu, M.; Woseneleh, T. Prevalence of and Factors Associated with Reoccurrence of Opportunistic Infections among Adult HIV/AIDS Patients Attending the ART Clinic at Public Health Facilities in Arba Minch Town, Southern Ethiopia. HIV AIDS 2021, 13, 867–876. [Google Scholar] [CrossRef] [PubMed]
- Pellowski, J.A.; Kalichman, S.C.; White, D.; Amaral, C.M.; Hoyt, G.; Kalichman, M.O. Real-time medication adherence monitoring intervention: Test of concept in people living with HIV infection. J. Assoc. Nurses AIDS Care 2014, 25, 646–651. [Google Scholar] [CrossRef]
- Trepka, M.J.; Fennie, K.P.; Sheehan, D.M.; Lutfi, K.; Maddox, L.; Lieb, S. Late HIV diagnosis: Differences by rural/urban residence, Florida, 2007–2011. AIDS Patient Care STDS 2014, 28, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Baker, P. Men’s health: An overlooked inequality. Br. J. Nurs. 2016, 25, 1054–1057. [Google Scholar] [CrossRef]
- Saldanha, D.; Gupta, N.; Shenoy, S.; Saralaya, V. Prevalence of opportunistic infections in AIDS patients in Mangalore, Karnataka. Trop. Dr. 2008, 38, 172–173. [Google Scholar] [CrossRef]
- Benson, C.A.; Kaplan, J.E.; Masur, H.; Pau, A.; Holmes, K.K. Treating opportunistic infections among HIV-infected adults and adolescents: Recommendations from CDC, the National Institutes of Health, and the HIV Medicine Association/Infectious Diseases Society of America. MMWR Recomm. Rep. 2004, 53, 1–112. [Google Scholar] [CrossRef]
- Dang, L.V.P.; Nguyen, Q.H.; Ishizaki, A.; Larsson, M.; Vu, N.T.P.; Do Duy, C.; Olson, L.; Dinh, T.T. Prevalence of Opportunistic Infections and Associated Factors in HIV-Infected Men Who Have Sex with Men on Antiretroviral Therapy in Bach Mai Hospital, Hanoi, Vietnam: A Case-Control Study. Am. J. Men’s Health 2020, 14, 1557988320926743. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | OIs Prevalence | Virological OIs | Bacteriological OIs | Parasitic OIs | |
|---|---|---|---|---|---|
| Gender | n (%) | n/N (%) | n (% [95% CI]) | n (% [95% CI]) | n (% [95% CI]) |
| Men | 69 (30.9) | 47/69 (68.1) | 11 (16 [8.6–27.2]) | 35 (50.7 [38.5–62.9]) | 11 (16 [8.6–27.2]) |
| Women | 154 (69.1) | 82/154 (53.2) | 23 (15 [9.9-21.8]) | 58 (37.7 [30.1–45.9]) | 21 (13.6 [8.8–20.3]) |
| Total | 223 (100) | 129/223 (57.9) | 34 (15 [11–20.8]) | 93 (41.7 [35.2–48.5]) | 32 (14.3 [10.2–19.8]) |
| Age (Years) | |||||
| 2–12 | 9(4.1) | 6/9 (66.7) | 1 (11 [0.6–49.3]) | 4 (44.4 [15.3–77.3]) | 3 (33.3 [9–69.1]) |
| 20–29 | 27(12.1) | 19/27 (70.4) | 7 (26 [11.9–46.6]) | 13 (48.1 [29.2–67.6]) | 4 (14.8 [4.9–34.6]) |
| 30–39 | 68(30.5) | 35/68 (51.5) | 14 (20.6 [12.1–32.5 | 19 (28 [18.1–40.3]) | 6 (8.8 [3.6–18.9]) |
| 40–49 | 75(33.6) | 42/75 (56) | 8 (10.7 [5–20.5]) | 37 (49.3 [37.7–61]) | 11 (14.7 [7.9–25.2]) |
| 50–77 | 44(19.7) | 27/44 (61.4) | 4 (9.1 [3–22.6]) | 20 (45.5 [30.7–61]) | 8 (18.2 [8.7–33.2]) |
| Median (IQR) 41 (27.5–54.5) | |||||
| CD4 cell count, cells/mm3 | |||||
| <200 | 35 (15.7) | 24/35 (68.6) | 8 (22.9 [11–40.6]) | 20 (57.1 [39.5–73.2) | 8 (22.9 [11–40.6]) |
| [200–499] | 127 (57) | 88/127 (69.3) | 22 (17.3 [11.4–25.3]) | 62 (48.8 [40–57.8]) | 22 (17.3 [11.4–25.3]) |
| ≥500 | 61 (27.3) | 17/61 (27.9) | 4 (6.6 [2.1–16.7]) | 11 (18 [9.8–30.4]) | 2 (3.3 [0.6–12.4]) |
| Median (IQR) 419 (93–745) | |||||
| ART regimen | |||||
| AZT − 3TC − EFV | 94 (42.2) | 54/94 (57.4) | 15 (16 [9.5–25.3]) | 40 (42.6 [32.5–53.2]) | 16 (17 [10.3–26.5]) |
| TDF − 3TC − EFV | 13 (5.8) | 8/13 (61.5) | 2 (15.4 [2.7–46.3]) | 8 (61.5 [32.3–84.9]) | 1 (7.7 [0.4–38]) |
| AZT + 3TC + NVP | 21 (9.4) | 10/21 (47.6) | 4 (19 [6.3–42.6]) | 5 (23.8 [9.1–47.5]) | 2 (9.5 [1.7–31.8]) |
| TDF + FTC + EFV | 54 (24.2) | 31/54 (57.4) | 7 (13 [5.8–25.5]) | 22 (40.7 [27.9–54.9]) | 7 (13 [5.8–25.5]) |
| Others | 41 (18.4) | 26/41 (63.4) | 6 (14.6 [6.1–29.9]) | 18 (44 [28.8–60.1]) | 6 (14.6 [6.1–30]) |
| Model No. (Rank) | Fixed Effects | Df | ΔAIC | Akaike Weight | ||
|---|---|---|---|---|---|---|
| Intercept | CD4 Rate | Sex | ||||
| 4 (1) | 1.534 | −0.0031 | + | 3 | 0 | 0.587 |
| 2 (2) | 1.726 | −0.0032 | 2 | 0.71 | 0.413 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mouinga-Ondeme, A.; Longo-Pendy, N.M.; Moussadji Kinga, I.C.; Ngoubangoye, B.; Moussavou-Boundzanga, P.; Boundenga, L.; Diane, A.; Sica, J.; Mfouo-Tynga, I.S.; Ngoungou, E.B. Risk Factors Associated with Opportunistic Infections among People Living with HIV/AIDS and Receiving an Antiretroviral Therapy in Gabon, Central Africa. Viruses 2024, 16, 85. https://doi.org/10.3390/v16010085
Mouinga-Ondeme A, Longo-Pendy NM, Moussadji Kinga IC, Ngoubangoye B, Moussavou-Boundzanga P, Boundenga L, Diane A, Sica J, Mfouo-Tynga IS, Ngoungou EB. Risk Factors Associated with Opportunistic Infections among People Living with HIV/AIDS and Receiving an Antiretroviral Therapy in Gabon, Central Africa. Viruses. 2024; 16(1):85. https://doi.org/10.3390/v16010085
Chicago/Turabian StyleMouinga-Ondeme, Augustin, Neil Michel Longo-Pendy, Ivan Cyr Moussadji Kinga, Barthélémy Ngoubangoye, Pamela Moussavou-Boundzanga, Larson Boundenga, Abdoulaye Diane, Jeanne Sica, Ivan Sosthene Mfouo-Tynga, and Edgard Brice Ngoungou. 2024. "Risk Factors Associated with Opportunistic Infections among People Living with HIV/AIDS and Receiving an Antiretroviral Therapy in Gabon, Central Africa" Viruses 16, no. 1: 85. https://doi.org/10.3390/v16010085