
Hepatitis C and Human Pegivirus Coinfection in Patients with Chronic Hepatitis C from the Brazilian Amazon Region: Prevalence, Genotypes and Clinical Data

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
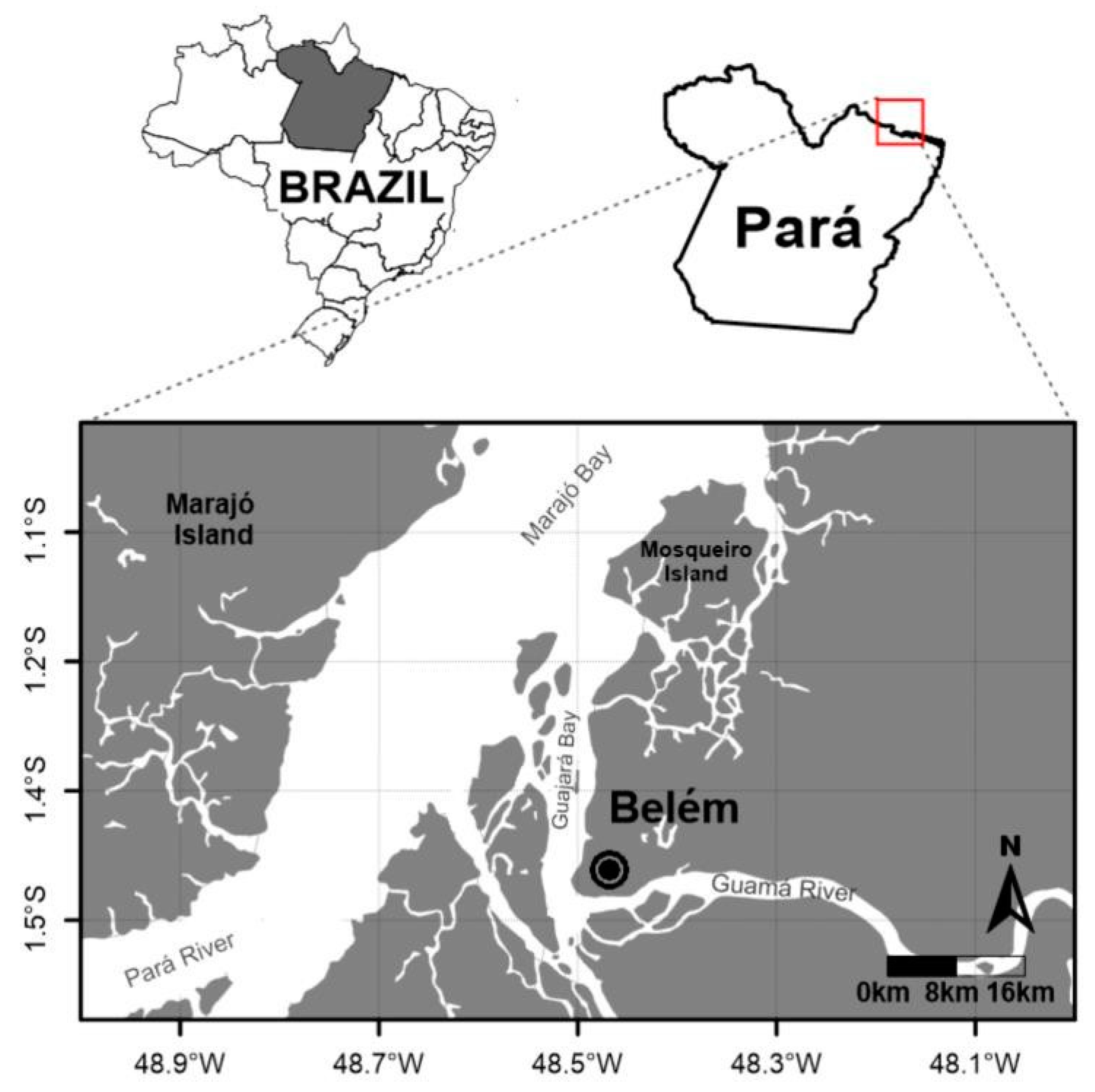
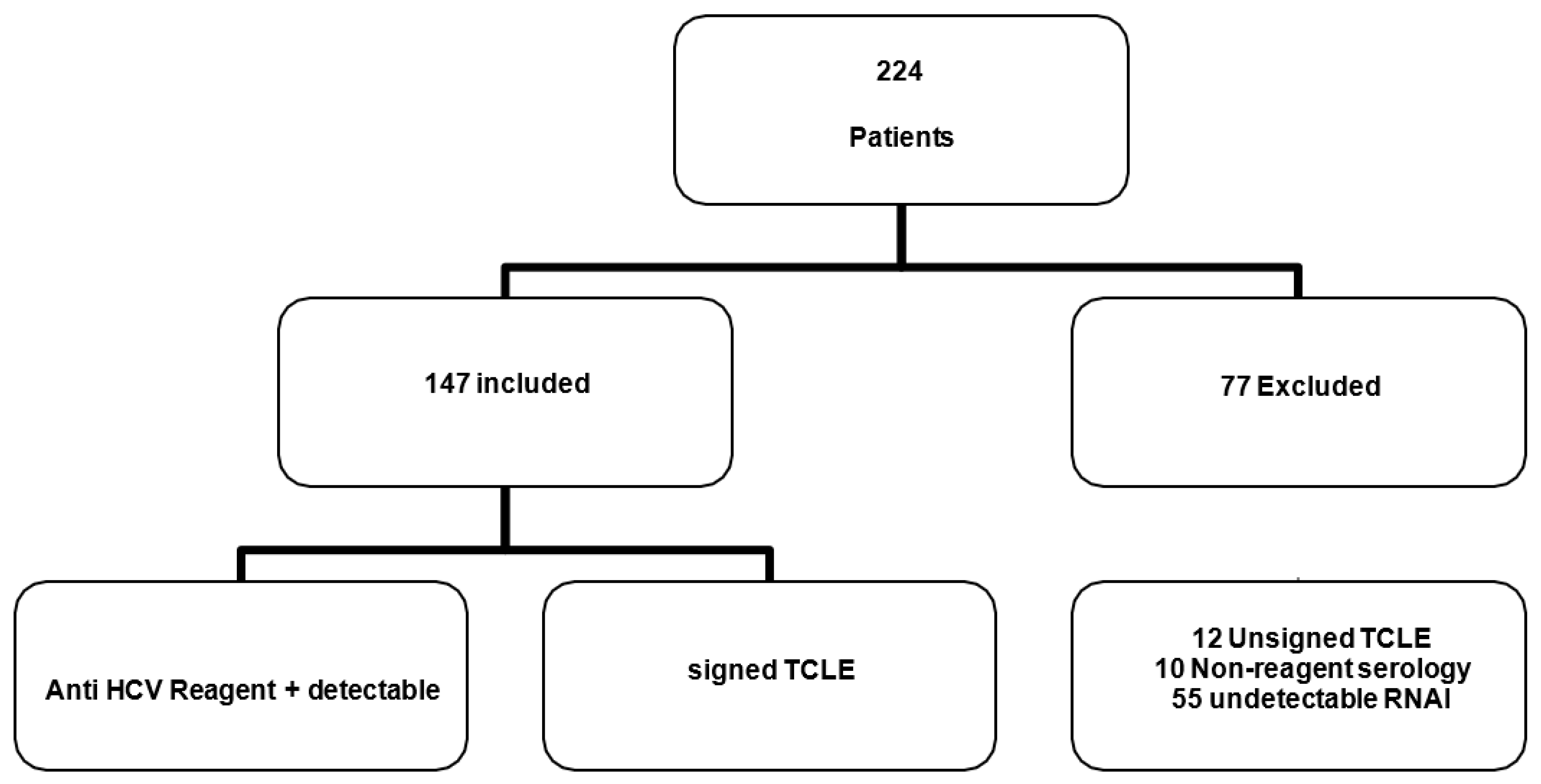
2.1. Population Study
2.2. Ethical Aspects
2.3. Serological Analysis
2.4. Viral Extraction of HCV and HPgV-1 Viruses
2.5. HCV Viral RNA Detection and Genotyping
2.6. HPgV-1 Viral RNA Detection and Genotyping
2.7. Assessment of Liver Elasticity (FibroScan Elastography)
3. Statistical Analysis
4. Results
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Slavova, S.N.; Maraninchi, R.S.; Hespanhol, M.R.; Sauvage, V.; Rodrigues, E.S.; Fontanari Krause, L.; Bittencourt, H.T.; Caro, V.; Laperche, S.; Covas, D.T.; et al. Human Pegivirus-1 (Hpgv-1) Rna Prevalence and Genotypes in Volunteer Blood Donors from the Brazilian Amazon. Transfus. Clin. Biol. 2019, 26, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Taklual, W.; Tang, S.; Yue, W. Effect of Human Pegivirus Route of Transmission on the Genetic Distribution of the Virus: An institution Based Cross-Sectional Study. Virol. J. 2019, 16, 50. [Google Scholar] [CrossRef] [PubMed]
- Giret, M.T.M.; Miraglia, J.L.; Sucupira, M.C.A.; Nishiya, A.; Levi, J.E.; Diaz, R.S.; Sabino, E.C.; Kallas, E.G. Prevalence, incidence Density, and Genotype Distribution of Gb Virus C infection in a Cohort of Recently Hiv-1-infected Subjects in Sao Paulo, Brazil. PLoS ONE 2011, 6, 18407. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.S.N.; Silva, C.P.; Barata, R.R.; Da Silva, P.V.R.; Monteiro, P.D.J.; Lamarão, L.; Burbano, R.M.R.; Nunes, M.R.T.; De Lima, P.D.L. Human Pegivirus (Hpgv, Gbv-C) Rna in Volunteer Blood Donors from a Public Hemotherapy Service in Northern Brazil. Virol. J. 2020, 17, 153. [Google Scholar] [CrossRef]
- Alcalde, R.; Nishiya, A.; Casseb, J.; Inocêncio, L.; Fonseca, L.A.; Duarte, A.J. Prevalence and Distribution of the Gbv-C/Hgv Among Hiv-1-infected Patients Under Anti-Retroviral therapy. Virus Res. 2010, 151, 148–152. [Google Scholar] [CrossRef]
- Campos, A.F.; Tengan, F.M.; Silva, S.A.A.; Levi, J.E. Influence of Hepatitis G Virus (Gb Virus C) on the Prognosis of Hiv-infected Women. Int. J. STD AIDS 2011, 22, 209–213. [Google Scholar] [CrossRef]
- Souza, A.K.V.; Komninakis, V.C.S.; Zappia, B.L.G.; Barbosa, J.A.; Mantovani, P.N.; Diaz, S.R.; Abrao, P.; Lanzara, A.G.; Granato, H.F.C.L. Evaluation of Gb Virus C/Hepatitis G Viral Load Among Hiv Type 1 Co-infected Patients in São Paulo, Brazil. Aids Res. Hum. Retroviruses 2012, 28, 289–294. [Google Scholar]
- Blackard, J.T.; Ma, G.; Polen, C.; Dubois, J.C.; Gast, J.; Radens, C.M.; Sterling, R.K.; Sherman, K.E. Recombination Among Gb Virus C (Gbv-C) Isolates in the United States. J. Gen. Virol. 2016, 97, 1537–1544. [Google Scholar] [CrossRef]
- Slavova, S.N.; Silveira, R.M.; Rodrigues, E.S.; Diefenbachc, C.F.; Zimmermannd, A.M.; Covasa, D.T.; Kashima, S. Human Pegivirus- 1 (Hpgv-1, Gbv-C) Rna Prevalence and Genotype Diversity Among Volunteer Blood Donors from an intra-Hospital Hemotherapy Service in Southern Brazil. Transfus. Apher. Sci. 2019, 58, 174–178. [Google Scholar] [CrossRef]
- Dhifallah, B.I.; Ayouni, K.; Chouiha, A.; Sadraoui, A.; Hogga, N.; Hammami, W.; Ben Yahya, A.; Triki, H. Genotype Distribution and Prevalence of Human Pegivirus Among High-Risk Populations in Tunisia. Intervirology 2016, 59, 170–178. [Google Scholar] [CrossRef]
- Da Mota, L.D.; Finger-Jardim, F.; Silva, C.M.; Germano, F.N.; Nader, M.M.; Gonçalves, C.V.; Da Hora, V.P.; Silveira, J.; Basso, R.P.; Soares, M.A.; et al. High Prevalence and Autochtonous Transmission of Human Pegivirus (Hpgv-1) in Blood Donors in the Extreme Southern of Brazil. J. Med. Virol. 2019, 91, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Ramezani, A.; Banifazl, M.; Aghakhani, A. Gb Virus C Overview: Insights into Clinical Implication. J. Gastroenterol. Hepatol. Res. 2013, 2, 343–349. [Google Scholar]
- Alvarado-Mora, M.V.; Botelho, L.; Nishiya, A.; Neto, R.A.; Gomes-Gouvêa, M.S.; Gutiérrez, M.F.; Carrilho, F.J.; Pinho, J.R. Frequency and Genotypic Distribution of Gb Virus C (Gbv-C) in the Colombian Population with Hepatitis B (Hbv) Or Hepatitis C (Hcv) infection. Virol. J. 2011, 8, 345. [Google Scholar] [CrossRef] [PubMed]
- Hazari, S.; Acharya, S.K.; Panda, S.K. Development and Evolution of Qualitative Comparative Reverse Transcription Polymerase Chain Reaction (Rt- Pcr) For Hepatitis C Virus Rna in Serum Using Transcribed Thio-Rna As internal Control. J. Virol. Methods 2004, 116, 45–54. [Google Scholar] [CrossRef]
- Naito, H.; Abe, K. Genotyping System of Gbv-C/Vhg Type 1 To Type 4 By the Polymerase Chain Reaction Using Type-Specific Primers and Geographical Distribution of Viral Genotypes. J. Virol. Methods 2001, 91, 3–9. [Google Scholar] [CrossRef]
- Bonnard, P.; Elsharkawy, A.; Zalata, K.; Delarocque-Astagneau, E.; Biard, L.; Le Fouler, L.; Hassan, A.B.; Abdel-Hamid, M.; El-Daly, M.; Gamal, M.E.; et al. Comparison of Liver Biopsy and Noninvasive Techniques For Liver Fibrosis Assessment in Patients infected with Hcv-Genotype 4 in Egypt. J. Viral Hepat. 2014, 22, 245–253. [Google Scholar] [CrossRef]
- Lampe, E.; De Oliveira, J.M.; Pereira, J.L.; Saback, F.L.; Yoshida, C.F.; Niel, C. Hepatitis G Virus (Gbv-C) infection Among Brazilian Patients with Chronic Liver Disease and Blood Donors. Clin. Diag Virol. 1998, 9, 1–7. [Google Scholar] [CrossRef]
- Leao-Filho, G.C.; Lopes, E.P.; Ferraz, A.A.; Moura, I.; Pernambuco, J.R.; Reis, C.; Silva, A.E.; Ferraz, M.L. Hepatitis G Virus infection in Patients with Hepatocellular Carcinoma in Recife, Brazil. Jpn. J. Clin. Oncol. 2007, 378, 632–636. [Google Scholar] [CrossRef]
- Pinho, J.R.; Zanotto, P.M.; Ferreira, J.L.; Sumita, L.M.; Carrilho, F.J.; Da Silva, L.C.; Capacci, M.L.; Silva, A.O.; Guz, B.; Gonçales, F.L., Jr.; et al. High Prevalence of Gb Virus C in Brazil and Molecular Evidence For intrafamilial Transmission. J. Clin. Microbiol. 1999, 37, 1634–1637. [Google Scholar] [CrossRef]
- Pereira, L.M.; Spinelli, V.; Ximenes, R.A.; Cavalcanti, M.S.; Melo, R.; Jucá, N.; Mizokami, M.; Mcfarlane, I.G. Chronic Hepatitis C infection: Influence of the Viral Load, Genotypes, and Gbv-C/Vhg Coinfection on the Severity of the Disease in A Brazilian Population. J. Med. Virol. 2002, 67, 27–32. [Google Scholar] [CrossRef]
- Jõgeda, E.L.; Huik, K.; Pauskar, M.; Kallas, E.; Karki, T.; Des Jarlais, D.; Uusküla, A.; Lutsar, I.; Avi, R. Prevalence and Genotypes of Gbv-C and Its Associations with Hiv infection Among Persons Who inject Drugs in Eastern Europe. J. Med. Virol. 2017, 89, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Trinks, J.; Maestri, M.; Oliveto, F.; Del Pino, N.; Weissenbacher, M.; Torres, O.W.; Oubiña, J.R. Human Pegivirus Molecular Epidemiology in Argentina: Potential Contribution of Latin American Migration to Genotype 3 Circulation. J. Med. Virol. 2014, 86, 2076–2083. [Google Scholar] [CrossRef] [PubMed]
- Savassi-Ribas, F.; Pereira, J.G.; Horta, M.A.P.; Wagner, T.C.S.; Matuck, T.A.; Monteiro De Carvalho, D.B.; Mello, F.C.A.; Varella, R.B.; Soares, C.C. Human Pegivirus-1 infection in Kidney Transplant Recipients: A Single-Center Experience. J. Med. Virol. 2020, 92, 2961–2968. [Google Scholar] [CrossRef]
- Castro, G.L.C.; Amoras, E.G.S.; Araujo, M.S.M.; Conde, S.R.S.S.; Vallinoto, A.C.R. Hepatitis C Virus Genotypes and Associated Risk Factors in the State of Pará, Northern Brazil. Braz. J. Infect Dis. 2020, 24, 304–309. [Google Scholar] [CrossRef]
- Guimarães, V.S.; Melo, T.G.; Ferreira, R.C.D.; Almeida, S.F.; Martins, L.C. Prevalence of Hepatitis C Virus Genotypes in the State of Pará, Brazil. Rev. Soc. Bras. Med. Trop. 2018, 51, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Duarte, C. Detecção E Quantificação Do Vírus Da Hepatite C Através De Rt-Pcr Em Tempo-Real. Master’s Thesis, Universidade Federal Do Paraná, Curitiba, Brazil, 2006. [Google Scholar]
- Lopes, C.L.R.; Teles, S.A.; Espírito-Santo, M.P.; Lampe, E.; Rodrigues, F.P.; Motta-Castro, A.R.C.; Marinho, T.A.; Reis, N.R.; Silva, A.M.C.; Martins, R.M.B. Prevalence, Risk Factors and Genotypes of Hepatitis C among Drug Users. Rev. Saúde Pública 2009, 43 (Suppl. 1), 43–50. [Google Scholar] [CrossRef]
- Silva, L.K.; Silva, M.B.; Rodart, I.F.; Lopes, G.B.; Costa, F.Q.; Melo, M.E.; Gusmão, E.; Reis, M.G. Prevalence of Hepatitis C Virus (HCV) infection and HCV Genotypes of Hemodialysis Patients in Salvador, Northeastern Brazil. Braz. J. Med. Biol. Res. 2006, 39, 595–602. [Google Scholar] [CrossRef]
- Zarife, M.A.S.A.; Oliveira, E.C.P.; Romeu, J.M.S.L.; Reis, M.G. Detection of Hepatitis C Virus Genotype 4 in Salvador, Ba. Case Report. Rev. Soc. Bras. Med. Trop. 2006, 39, 567–569. [Google Scholar] [CrossRef]
- Shahid, M.; Idrees, M.; Butt, A.M.; Raza, S.M.; Amin, I.; Rasul, A.; Afzal, S.; Zahid, S.; Nawaz, R. Short Article: Hepatitis C and G Virus Coinfection in Punjab, Pakistan: Incidence and Its Correlation Analysis with Clinical Data. Eur. J. Gastroenterol. Hepatol. 2019, 31, 389–392. [Google Scholar] [CrossRef]
- Yu, Y.; Wan, Z.; Wang, J.H.; Yang, X.; Zhang, C. Review of Human Pegivirus: Prevalence, Transmission, Pathogenesis, and Clinical Implication. Virulence 2022, 13, 324–341. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Primer | Sequence a (Specificity/Polarity) | Isolate Designed for Primer Sequences b |
|---|---|---|
| HG1 | 5′-GGTCGTAAATCCC GGTCACC-3′ (universal/sense) | PNF2161 (U44402; 139 to 158) |
| HG1R | 5′-CCCACTGGTCCTT GTCAACT-3′ (universal/antisense) | PNF2161 (U44402; 381 to 400) |
| HG2R | 5′-ATTGAAGGGCGA CGTGGACC-3′ (universal/antisense) | PNF2161 (U44402; 331 to 350) |
| Mix A | ||
| G38 | 5′-TGTAATAAGGACC CGGCGMT-3′ | GBV-C (U36380; 239 (type to 257) 1-specific/sense) |
| G41 | 5′-TGGTCAAGGTCCC TCTG-3′ | HGV-VT2 (AB013193; (type 28 to 44) 3-specific/sense) |
| Mix B | ||
| G35 | 5′-GGGTCTTAAGAG AAGGTTAAGA-3′ | PNF2161 (U44402; 177 to 198) (type 2-specific/sense) |
| G40 | 5′-GGGTYAAGGCAC CTCTTA-3′ | HGV-MY14 (type (AB021287; 28 to 45) 4-specific/sense) |
| Variables | HCV Monoinfected (n = 106) | HCV/HPgV-1 (+) (n = 41) | Odds Ratio | IC (95%) | p Value |
|---|---|---|---|---|---|
| Sex | |||||
| Masculine | 57 (53.8) | 23 (56.1) | 1.09 | (0.53–2.26) | 0.94 |
| Feminine | 49 (46.2) | 18 (43.9) | |||
| Marital status | |||||
| Single/widowed | 42 (39.6) | 15 (36.6) | 0.87 | (0.41–1.85) | 0.88 |
| Married/stable union | 64 (60.4) | 26 (63.4) | |||
| Age range | |||||
| 18–40 | 32 (30.2) | 8 (19.5) | 0.56 | (0.23–1.34) | 0.27 |
| ≥41 | 74 (69.8) | 33 (80.5) | |||
| Education | |||||
| Up to 8 years | 29 (27.4) | 16 (39) | 1.69 | (0.79–3.63) | 0.24 |
| >8 years | 77 (72.6) | 25 (61) | |||
| Income | |||||
| Up to 2 wages | 68 (64.2) | 26 (63.4) | 0.96 | (0.45–2.04) | 0.91 |
| >2 salaries | 38 (35.8) | 15 (36.6) | |||
| Condom use | |||||
| Yes | 31 (29.2) | 13 (31.7) | 0.89 | (0.40–1.94) | 0.95 |
| No | 75 (70.8) | 28 (68.3) | |||
| Number of sexual partners (2 or more) | |||||
| Yes | 30 (28.3) | 12 (29.3) | 1.04 | (0.47–2.32) | 0.93 |
| No | 76 (71.7) | 29 (70.7) | |||
| STI history | |||||
| Yes | 29 (27.4) | 13 (31.7) | 1.23 | (0.56–2.70) | 0.75 |
| No | 77 (72.6) | 28 (68.3) | |||
| Manicure | |||||
| Yes | 54 (51) | 15 (36.6) | 0.55 | (0.26–1.16) | 0.16 |
| No | 52 (49) | 26 (63.4) | |||
| Injecting drug use | |||||
| Yes | 9 (8.5) | 1 (2.4) | 0.26 | (0.03–2.19) | 0.31 |
| No | 97 (91.5) | 40 (97.6) | |||
| Tattoo | |||||
| Yes | 34 (32.1) | 8 (19.5) | 0.51 | (0.21–1.22) | 0.19 |
| No | 72 (67.9) | 33 (80.5) | |||
| Transplant | |||||
| Yes | 1 (0.9) | 1 (2.4) | 2.62 | (0.16–42.9) | 0.92 |
| No | 105 (99.1) | 40 (97.6) | |||
| Hemodialysis | |||||
| Yes | 1 (0.9) | 1 (2.4) | 2.62 | (0.16–42.9) | 0.92 |
| No | 105 (99.1) | 40 (97.6) | |||
| Blood transfusion | |||||
| Yes | 19 (17.9) | 7 (17.1) | 0.94 | (0.36–2.44) | 0.90 |
| No | 87 (82.1) | 34 (82.9) | |||
| Total | Male | Female | p Value | |
|---|---|---|---|---|
| Genotype HPgV-1 (n = 41) | n (%) | n (%) | n (%) | |
| 1 | 15 (36.6) | 8 (19.5) | 7 (17.0) | 0.95 a |
| 2 | 26 (63.4) | 15(36.5) | 11(27.0) | |
| Genotype HCV/HPgV-1 (n = 41) | ||||
| 1 | 28 (68.3) | 16 (39) | 12 (29.3) | 0.88 b |
| 3 | 13 (31.7) | 7 (17) | 6 (14.7) | |
| Genotype HCV monoinfected (n = 106) | ||||
| 1 | 58(54.7) | 30 (28.3) | 28 (26.4) | 0.87 a |
| 3 | 48 (45.3) | 25 (23.6) | 23 (21.7) |
| Laboratory Tests | Monoinfected (HCV) n = 106 | Coinfected (HCV/HPgV-1) n = 41 | p Value |
|---|---|---|---|
| LIVER STIFFNESS (kPa) | 7.53 ± 3.2 | 7.28 ± 2.7 | 0.31 |
| AST, U/L | 69.08 ± 1.79 | 85.54 ± 1.82 | 0.26 |
| ALT U/L | 75.47 ± 1.83 | 86.93 ± 1.96 | 0.38 |
| HCV RNA, Log IU/mL | 815.88 ± 15.82 | 619.875 ± 20.17 | 0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nunes, P.F.; da Cruz Coelho, E.; da Silva, J.R.; da Silva Costa, C.C.; Sampaio, R.M.A.; Frade, P.C.R.; Ponteira, N.A.; da Cruz, S.S.; Seabra, A.D.; Carneiro, D.M.; et al. Hepatitis C and Human Pegivirus Coinfection in Patients with Chronic Hepatitis C from the Brazilian Amazon Region: Prevalence, Genotypes and Clinical Data. Viruses 2023, 15, 1892. https://doi.org/10.3390/v15091892
Nunes PF, da Cruz Coelho E, da Silva JR, da Silva Costa CC, Sampaio RMA, Frade PCR, Ponteira NA, da Cruz SS, Seabra AD, Carneiro DM, et al. Hepatitis C and Human Pegivirus Coinfection in Patients with Chronic Hepatitis C from the Brazilian Amazon Region: Prevalence, Genotypes and Clinical Data. Viruses. 2023; 15(9):1892. https://doi.org/10.3390/v15091892
Chicago/Turabian StyleNunes, Patrícia Ferreira, Evelen da Cruz Coelho, Joseane Rodrigues da Silva, Camila Carla da Silva Costa, Regiane Miranda Arnund Sampaio, Paula Cristina Rodrigues Frade, Nagib Abdon Ponteira, Samara Silveira da Cruz, Aline Damasceno Seabra, Debora Monteiro Carneiro, and et al. 2023. "Hepatitis C and Human Pegivirus Coinfection in Patients with Chronic Hepatitis C from the Brazilian Amazon Region: Prevalence, Genotypes and Clinical Data" Viruses 15, no. 9: 1892. https://doi.org/10.3390/v15091892