
Improved Performance of the QuantiFERON-SARS-CoV-2 Assay with the Extended Set
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
- Convalescent subjects (n = 30, mean age 32 ± 10.7, range (19–57) years, 14 males and 16 females): individuals with previous COVID-19 infection with a positive nasopharyngeal swab and clinically symptomatic (mild to moderate symptoms). None of the participants had been vaccinated before blood drawing. The median time between PCR-confirmed COVID-19 diagnosis and plasma samples was 28 days (range between 17 and 59 days).
- Vaccinated healthy subjects (n = 39, mean age 42.9 ± 15, range (18–64) years, 17 males and 22 females): SARS-CoV-2 naïve individuals with no history of COVID-19 symptoms or positive SARS-CoV-2 test who had been fully vaccinated with one of the COVID-19 vaccines available in our country at the time of the study: Sinovac (n = 28), Janssen (n = 7), or Sputnik (n = 4). Subjects were considered fully vaccinated if they received the second dose of the homologous two-dose vaccine regimen (for Sinovac and Sputnik) or a dose of the one dose vaccine (Janssen) without receiving a booster dose. At the first blood collection, the median time from completed vaccination was 32 days (range (16–55) days). Ten patients out of this group (vaccinated with Sinovac) agreed for a second follow-up three months after the second dose of the vaccine (median 97, range (88–108) days).
- Healthy, unvaccinated subjects (n = 6, mean age 43.6 ± 14.2, range (19–57) years, three males and three females): SARS-CoV-2 naïve and unvaccinated individuals were included as a negative control group.
2.2. Methods
2.2.1. Humoral Immune Response
2.2.2. T-Cell Response
2.3. Statistical Analysis
3. Results
3.1. Humoral Response
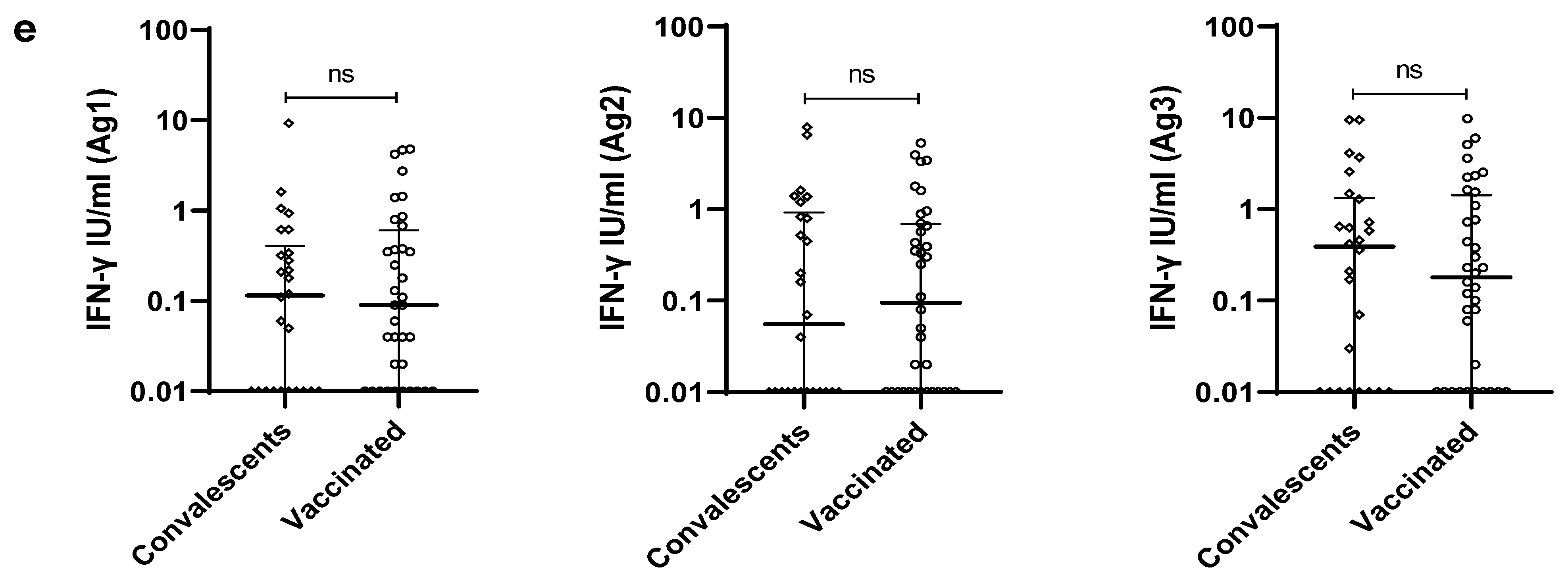
3.2. SARS-CoV-2 Specific T-Cell Response
3.3. Evaluation of the Immune Response to SARS-CoV-2 Vaccine after Three-Month Follow Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ni, L.; Ye, F.; Cheng, M.-L.; Feng, Y.; Deng, Y.-Q.; Zhao, H.; Wei, P.; Ge, J.; Gou, M.; Li, X.; et al. Detection of SARS-CoV-2-Specific Humoral and Cellular Immunity in COVID-19 Convalescent Individuals. Immunity 2020, 52, 971–977.e3. [Google Scholar] [CrossRef] [PubMed]
- Sette, A.; Crotty, S. Adaptive Immunity to SARS-CoV-2 and COVID-19. Cell 2021, 184, 861–880. [Google Scholar] [CrossRef] [PubMed]
- Agrati, C.; Castilletti, C.; Goletti, D.; Meschi, S.; Sacchi, A.; Matusali, G.; Bordoni, V.; Petrone, L.; Lapa, D.; Notari, S.; et al. Coordinate Induction of Humoral and Spike Specific T-Cell Response in a Cohort of Italian Health Care Workers Receiving BNT162b2 MRNA Vaccine. Microorganisms 2021, 9, 1315. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, I.; Mattiuzzo, G.; Page, M.; Minor, P.; Griffiths, E.; Nuebling, M.; Moorthy, V. WHO International Standard for Evaluation of the Antibody Response to COVID-19 Vaccines: Call for Urgent Action by the Scientific Community. Lancet Microbe 2022, 3, e235–e240. [Google Scholar] [CrossRef]
- Freeman, J.; Conklin, J. Standardization of Two SARS-CoV-2 Serology Assays to the WHO 20/136 Human Standard Reference Material. J. Virol. Methods 2022, 300, 114430. [Google Scholar] [CrossRef]
- Seow, J.; Graham, C.; Merrick, B.; Acors, S.; Pickering, S.; Steel, K.J.A.; Hemmings, O.; O’Byrne, A.; Kouphou, N.; Galao, R.P.; et al. Longitudinal Observation and Decline of Neutralizing Antibody Responses in the Three Months Following SARS-CoV-2 Infection in Humans. Nat. Microbiol. 2020, 5, 1598–1607. [Google Scholar] [CrossRef]
- Zhu, L.; Xu, X.; Zhu, B.; Guo, X.; Xu, K.; Song, C.; Fu, J.; Yu, H.; Kong, X.; Peng, J.; et al. Kinetics of SARS-CoV-2 Specific and Neutralizing Antibodies over Seven Months after Symptom Onset in COVID-19 Patients. Microbiol. Spectr. 2021, 9, e0059021. [Google Scholar] [CrossRef]
- Sekine, T.; Perez-Potti, A.; Rivera-Ballesteros, O.; Strålin, K.; Gorin, J.-B.; Olsson, A.; Llewellyn-Lacey, S.; Kamal, H.; Bogdanovic, G.; Muschiol, S.; et al. Robust T Cell Immunity in Convalescent Individuals with Asymptomatic or Mild COVID-19. Cell 2020, 183, 158–168.e14. [Google Scholar] [CrossRef]
- Legros, V.; Denolly, S.; Vogrig, M.; Boson, B.; Siret, E.; Rigaill, J.; Pillet, S.; Grattard, F.; Gonzalo, S.; Verhoeven, P.; et al. A Longitudinal Study of SARS-CoV-2-Infected Patients Reveals a High Correlation between Neutralizing Antibodies and COVID-19 Severity. Cell. Mol. Immunol. 2021, 18, 318–327. [Google Scholar] [CrossRef]
- Tarke, A.; Sidney, J.; Methot, N.; Zhang, Y.; Dan, J.M.; Goodwin, B.; Rubiro, P.; Sutherland, A.; da Antunes, R.S.; Frazier, A.; et al. Negligible Impact of SARS-CoV-2 Variants on CD4+ and CD8+ T Cell Reactivity in COVID-19 Exposed Donors and Vaccinees. BioRxiv 2021. [Google Scholar] [CrossRef]
- Geers, D.; Shamier, M.C.; Bogers, S.; den Hartog, G.; Gommers, L.; Nieuwkoop, N.N.; Schmitz, K.S.; Rijsbergen, L.C.; van Osch, J.A.T.; Dijkhuizen, E.; et al. SARS-CoV-2 Variants of Concern Partially Escape Humoral but Not T-Cell Responses in COVID-19 Convalescent Donors and Vaccinees. Sci. Immunol. 2021, 6, eabj1750. [Google Scholar] [CrossRef] [PubMed]
- Bonifacius, A.; Tischer-Zimmermann, S.; Dragon, A.C.; Gussarow, D.; Vogel, A.; Krettek, U.; Gödecke, N.; Yilmaz, M.; Kraft, A.R.M.; Hoeper, M.M.; et al. COVID-19 Immune Signatures Reveal Stable Antiviral T Cell Function despite Declining Humoral Responses. Immunity 2021, 54, 340–354.e6. [Google Scholar] [CrossRef] [PubMed]
- Le Bert, N.; Chia, W.N.; Wan, W.Y.; Teo, A.K.J.; Chong, S.Z.-R.; Tan, N.; Tan, D.S.C.; Chia, A.; Tan, I.B.; Kunasegaran, K.; et al. Widely Heterogeneous Humoral and Cellular Immunity after Mild SARS-CoV-2 Infection in a Homogeneous Population of Healthy Young Men. Emerg. Microbes Infect. 2021, 10, 2141–2150. [Google Scholar] [CrossRef] [PubMed]
- Agrati, C.; Castilletti, C.; Goletti, D.; Sacchi, A.; Bordoni, V.; Mariotti, D.; Notari, S.; Matusali, G.; Meschi, S.; Petrone, L.; et al. Persistent Spike-Specific T Cell Immunity despite Antibody Reduction after 3 Months from SARS-CoV-2 BNT162b2-MRNA Vaccine. Sci. Rep. 2022, 12, 6687. [Google Scholar] [CrossRef]
- Schwarz, M.; Mzoughi, S.; Lozano-Ojalvo, D.; Tan, A.T.; Bertoletti, A.; Guccione, E. T Cell Immunity Is Key to the Pandemic Endgame: How to Measure and Monitor It. Curr. Res. Immunol. 2022, 3, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Deborska-Materkowska, D.; Perkowska-Ptasinska, A.; Sadowska, A.; Gozdowska, J.; Ciszek, M.; Serwanska-Swietek, M.; Domagala, P.; Miszewska-Szyszkowska, D.; Sitarek, E.; Jozwik, A.; et al. Diagnostic Utility of Monitoring Cytomegalovirus-Specific Immunity by QuantiFERON-Cytomegalovirus Assay in Kidney Transplant Recipients. BMC Infect. Dis. 2018, 18, 179. [Google Scholar] [CrossRef]
- Shafeque, A.; Bigio, J.; Hogan, C.A.; Pai, M.; Banaei, N. Fourth-Generation QuantiFERON-TB Gold Plus: What Is the Evidence? J. Clin. Microbiol. 2020, 58, e01950-19. [Google Scholar] [CrossRef]
- QuantiFERON SARS-CoV-2 Starter Set Blood Collection Tubes Instructions for Use (Handbook)—QIAGEN. Available online: https://www.qiagen.com/ca/resources/resourcedetail?id=2a36a234-bfde-45f4-ae08-7c28ef95df7b&lang=en (accessed on 21 January 2023).
- Krüttgen, A.; Klingel, H.; Haase, G.; Haefner, H.; Imöhl, M.; Kleines, M. Evaluation of the QuantiFERON SARS-CoV-2 Interferon-ɣ Release Assay in MRNA-1273 Vaccinated Health Care Workers. J. Virol. Methods 2021, 298, 114295. [Google Scholar] [CrossRef]
- Martínez-Gallo, M.; Esperalba, J.; Pujol-Borrell, R.; Sandá, V.; Arrese-Muñoz, I.; Fernández-Naval, C.; Antón, A.; Cardona, V.; Labrador-Horrillo, M.; Pumarola, T.; et al. Commercialized Kits to Assess T-Cell Responses against SARS-CoV-2 S Peptides. A Pilot Study in Health Care Workers. Med. Clin. Engl. Ed. 2022, 159, 116–123. [Google Scholar] [CrossRef]
- Tychala, A.; Meletis, G.; Katsimpourlia, E.; Gkeka, I.; Dimitriadou, R.; Sidiropoulou, E.; Skoura, L. Evaluation of the QuantiFERON SARS-CoV-2 Assay to Assess Cellular Immunogenicity of the BNT162b2 MRNA COVID-19 Vaccine in Individuals with Low and High Humoral Response. Hum. Vaccines Immunother. 2021, 17, 5148–5149. [Google Scholar] [CrossRef]
- Barreiro, P.; Sanz, J.C.; San Román, J.; Pérez-Abeledo, M.; Carretero, M.; Megías, G.; Viñuela-Prieto, J.M.; Ramos, B.; Canora, J.; Martínez-Peromingo, F.J.; et al. A Pilot Study for the Evaluation of an Interferon Gamma Release Assay (IGRA) To Measure T-Cell Immune Responses after SARS-CoV-2 Infection or Vaccination in a Unique Cloistered Cohort. J. Clin. Microbiol. 2022, 60, e02199-21. [Google Scholar] [CrossRef]
- Tormo, N.; Giménez, E.; Martínez-Navarro, M.; Albert, E.; Navalpotro, D.; Torres, I.; Gimeno, C.; Navarro, D. Performance Comparison of a Flow Cytometry Immunoassay for Intracellular Cytokine Staining and the QuantiFERON® SARS-CoV-2 Test for Detection and Quantification of SARS-CoV-2-Spike-Reactive-IFN-γ-Producing T Cells after COVID-19 Vaccination. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Aiello, A.; Coppola, A.; Vanini, V.; Petrone, L.; Cuzzi, G.; Salmi, A.; Altera, A.M.G.; Tortorella, C.; Gualano, G.; Gasperini, C.; et al. Accuracy of QuantiFERON SARS-CoV-2 Research Use Only Assay and Characterization of the CD4+ and CD8+ T Cell-SARS-CoV-2 Response: Comparison with a Homemade Interferon-γ Release Assay. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2022, 122, 841–849. [Google Scholar] [CrossRef] [PubMed]
- Van Praet, J.; Reynders, M.; De Bacquer, D.; Viaene, L.; Schoutteten, M.K.; Caluwé, R.; Doubel, P.; Heylen, L.; De Bel, A.V.; Van Vlem, B.; et al. Predictors and Dynamics of the Humoral and Cellular Immune Response to SARS-CoV-2 MRNA Vaccines in Hemodialysis Patients: A Multicenter Observational Study. J. Am. Soc. Nephrol. JASN 2021, 32, 3208–3220. [Google Scholar] [CrossRef] [PubMed]
- Bonelli, M.M.; Mrak, D.; Perkmann, T.; Haslacher, H.; Aletaha, D. SARS-CoV-2 Vaccination in Rituximab-Treated Patients: Evidence for Impaired Humoral but Inducible Cellular Immune Response. Ann. Rheum. Dis. 2021, 80, 1355–1356. [Google Scholar] [CrossRef] [PubMed]
- Busà, R.; Sorrentino, M.C.; Russelli, G.; Amico, G.; Miceli, V.; Miele, M.; Di Bella, M.; Timoneri, F.; Gallo, A.; Zito, G.; et al. Specific Anti-SARS-CoV-2 Humoral and Cellular Immune Responses After Booster Dose of BNT162b2 Pfizer-BioNTech MRNA-Based Vaccine: Integrated Study of Adaptive Immune System Components. Front. Immunol. 2022, 13, 856657. [Google Scholar] [CrossRef] [PubMed]
- QuantiFERON SARS-CoV-2 Extended Set Blood Collection Tubes Instructions for Use (Handbook)—QIAGEN. Available online: https://www.qiagen.com/us/resources/resourcedetail?id=60729925-a7b2-4cf3-8d28-52e4106af16b&lang=en (accessed on 21 January 2023).
- Jaganathan, S.; Stieber, F.; Rao, S.N.; Nikolayevskyy, V.; Manissero, D.; Allen, N.; Boyle, J.; Howard, J. Preliminary Evaluation of QuantiFERON SARS-CoV-2 and QIAreach Anti-SARS-CoV-2 Total Test in Recently Vaccinated Individuals. Infect. Dis. Ther. 2021, 10, 2765–2776. [Google Scholar] [CrossRef] [PubMed]
- Stieber, F.; Allen, N.; Carpenter, K.; Hu, P.; Alagna, R.; Rao, S.; Manissero, D.; Howard, J.; Nikolayevskyy, V. Durability of COVID-19 Vaccine Induced T-Cell Mediated Immune Responses Measured Using the QuantiFERON SARS-CoV-2 Assay. Pulmonology 2023, 29, 151–153. [Google Scholar] [CrossRef]
- Johnson, S.A.; Phillips, E.; Adele, S.; Longet, S.; Malone, T.; Mason, C.; Stafford, L.; Jamsen, A.; Gardiner, S.; Deeks, A.; et al. Evaluation of QuantiFERON SARS-CoV-2 Interferon-γ Release Assay Following SARS-CoV-2 Infection and Vaccination. Clin. Exp. Immunol. 2023, uxad027. [Google Scholar] [CrossRef]
- Peng, Y.; Mentzer, A.J.; Liu, G.; Yao, X.; Yin, Z.; Dong, D.; Dejnirattisai, W.; Rostron, T.; Supasa, P.; Liu, C.; et al. Broad and Strong Memory CD4+ and CD8+ T Cells Induced by SARS-CoV-2 in UK Convalescent Individuals Following COVID-19. Nat. Immunol. 2020, 21, 1336–1345. [Google Scholar] [CrossRef] [PubMed]
- Zuo, J.; Dowell, A.C.; Pearce, H.; Verma, K.; Long, H.M.; Begum, J.; Aiano, F.; Amin-Chowdhury, Z.; Hoschler, K.; Brooks, T.; et al. Robust SARS-CoV-2-Specific T Cell Immunity Is Maintained at 6 Months Following Primary Infection. Nat. Immunol. 2021, 22, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, C.J.; Swadling, L.; Gibbons, J.M.; Pade, C.; Jensen, M.P.; Diniz, M.O.; Schmidt, N.M.; Butler, D.K.; Amin, O.E.; Bailey, S.N.L.; et al. Discordant Neutralizing Antibody and T Cell Responses in Asymptomatic and Mild SARS-CoV-2 Infection. Sci. Immunol. 2020, 5, eabf3698. [Google Scholar] [CrossRef] [PubMed]
- Kruse, M.; Dark, C.; Aspden, M.; Cochrane, D.; Competiello, R.; Peltz, M.; Torres, L.; Wrighton-Smith, P.; Dudek, M. Performance of the T-SPOT®.COVID Test for Detecting SARS-CoV-2-Responsive T Cells. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2021, 113, 155–161. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Responders | Convalescents (N = 26) | Vaccinated (N = 36) | p |
|---|---|---|---|
| At least one Ag; n (n/N%) | 18 (69.2) | 23 (63.9) | 0.661 |
| Ag 1; n (n/N%) | 11 (42.3) | 14 (38.9) | 0.787 |
| Ag 2; n (n/N%) | 10 (38.5) | 15 (41.7) | 0.800 |
| Ag 3; n (n/N%) | 15 (57.7) | 19 (52.8) | 0.700 |
| Only Ag1; n (n/N%) | 2 (7.7) | 1 (2.8) | / |
| Only Ag2; n (n/N%) | 1 (3.8) | 2 (5.6) | / |
| Only Ag3; n (n/N%) | 5 (19.2) | 4 (11.1) | / |
| Ag1 + Ag2; n (n/N%) | 0 (0) | 1 (2.8) | / |
| Ag1 + Ag3; n (n/N%) | 1 (3.8) | 3 (8.3) | / |
| Ag2 + Ag3; n (n/N%) | 1 (3.8) | 3 (8.3) | / |
| Ag1 + Ag2 + Ag3; n (n/N%) | 8 (30.8) | 9 (25) | / |
| Responders | Inactivated Vaccine (N = 26) | Vector-Based Vaccines (N = 10) | p |
|---|---|---|---|
| At least one Ag; n (n/N%) | 16 (61.5) | 7 (70) | 0.716 |
| Ag 1; n (n/N%) | 12 (46.2) | 2 (20) | 0.255 |
| Ag 2; n (n/N%) | 11 (42.3) | 4 (40) | 1.000 |
| Ag 3; n (n/N%) | 13 (50) | 6 (60) | 0.717 |
| Factors | OR | 95% CI | p |
|---|---|---|---|
| Age | 1 | [0.966–1.041] | 0.880 |
| Gender (female) | 0.64 | [0.213–1.914] | 0.423 |
| Lymphocytes | 1 | [0.999–1.001] | 0.845 |
| Time from blood collection (˂30 days) | 3.47 | [1.145–10.495] | 0.028 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamara Mahammed, L.; Bensaid, K.; Ait-Seddik, S.; Larinouna, A.; Brahimi, G.; Belkaid, R.; Hamzaoui, O.; Rouaki, S.M.; Idder, C.; Allam, I.; et al. Improved Performance of the QuantiFERON-SARS-CoV-2 Assay with the Extended Set. Viruses 2023, 15, 1179. https://doi.org/10.3390/v15051179
Lamara Mahammed L, Bensaid K, Ait-Seddik S, Larinouna A, Brahimi G, Belkaid R, Hamzaoui O, Rouaki SM, Idder C, Allam I, et al. Improved Performance of the QuantiFERON-SARS-CoV-2 Assay with the Extended Set. Viruses. 2023; 15(5):1179. https://doi.org/10.3390/v15051179
Chicago/Turabian StyleLamara Mahammed, Lydia, Kahina Bensaid, Sarah Ait-Seddik, Amel Larinouna, Ghania Brahimi, Rosa Belkaid, Ouassila Hamzaoui, Soumia Meriem Rouaki, Cherifa Idder, Ines Allam, and et al. 2023. "Improved Performance of the QuantiFERON-SARS-CoV-2 Assay with the Extended Set" Viruses 15, no. 5: 1179. https://doi.org/10.3390/v15051179