
Nationwide Laboratory Surveillance of Progressive Multifocal Leukoencephalopathy in Japan: Fiscal Years 2011–2020
 , , , , , add
Show full author list
, , , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. CSF Specimens and Clinical Data
2.2. Real-Time PCR Testing for JCV in the CSF
2.3. Statistical Analysis
3. Results
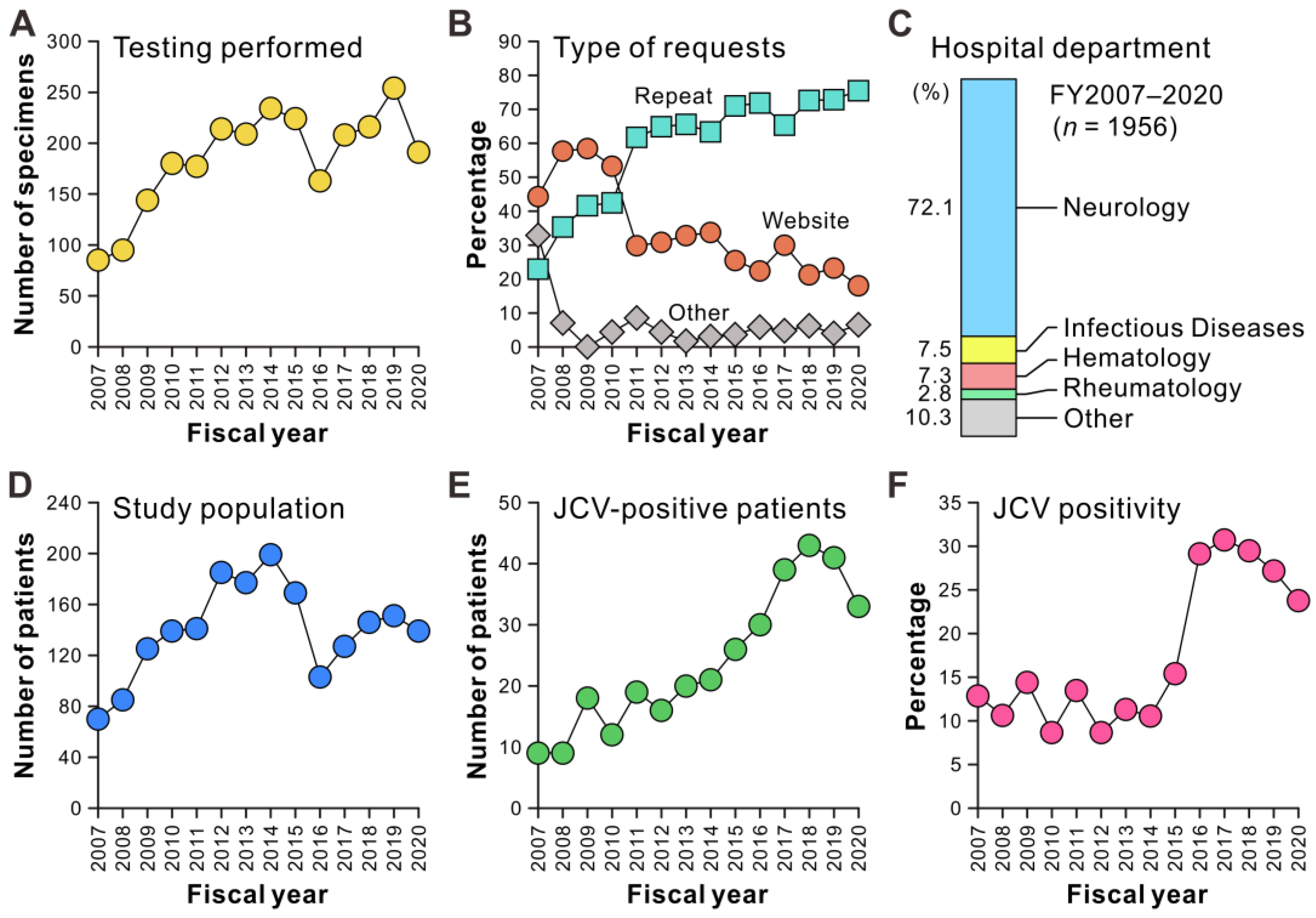
3.1. Long-Term Performance of Laboratory Surveillance of PML Using PCR Testing for JCV in the CSF
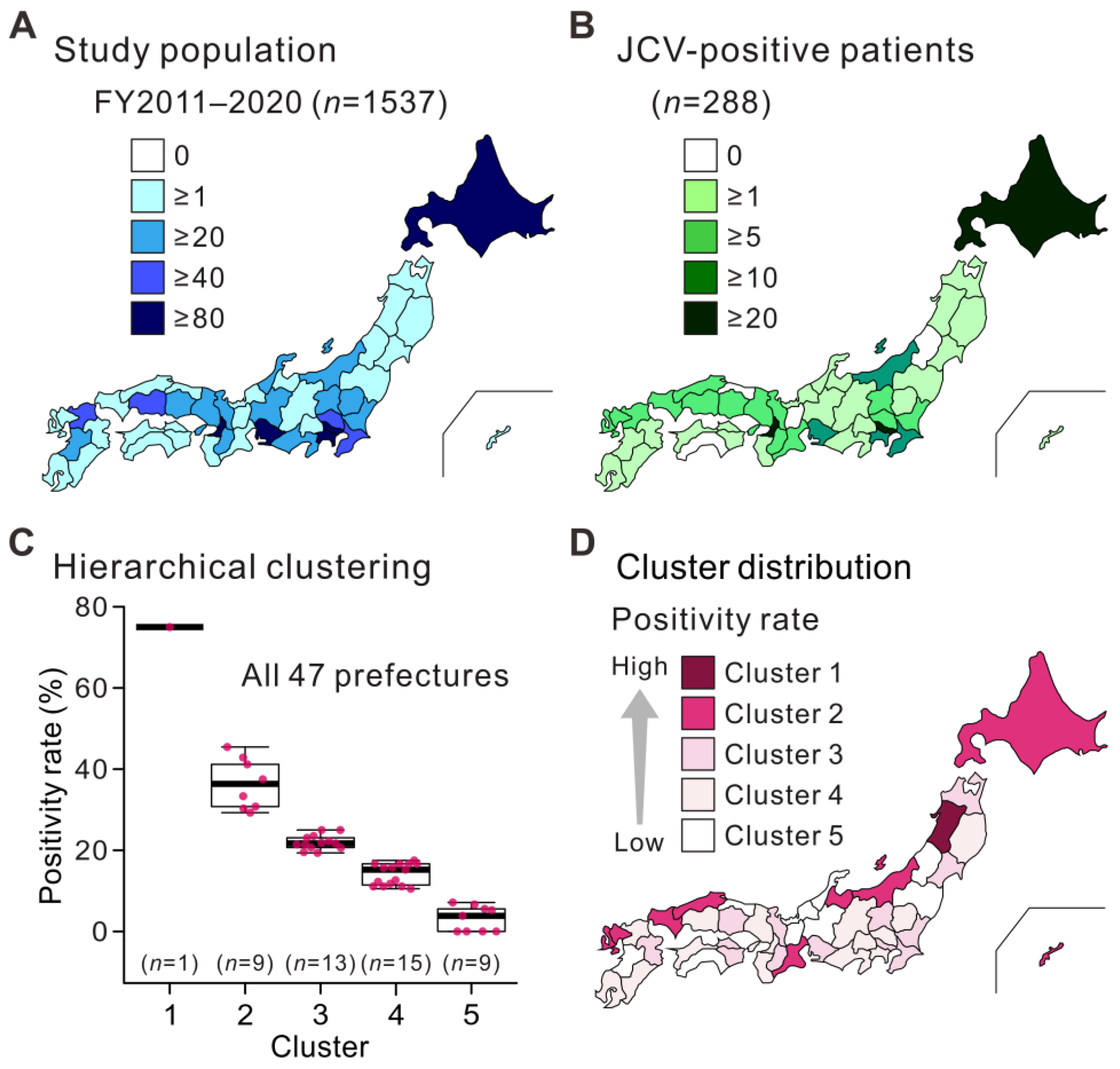
3.2. Geographic Distribution of the Study Population and Patients with JCV-Positive CSF
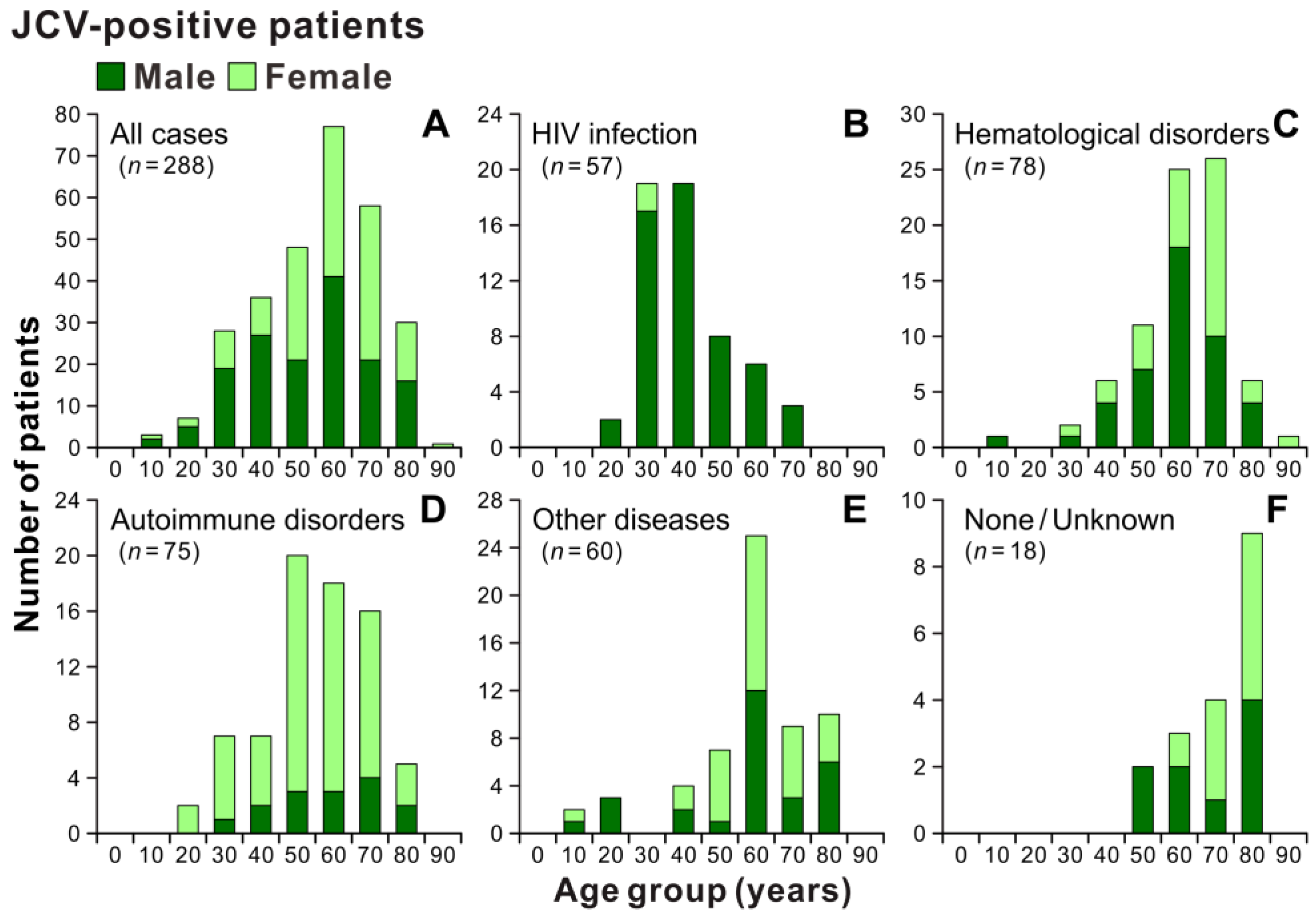
3.3. Overview of Patients with JCV-Positive CSF
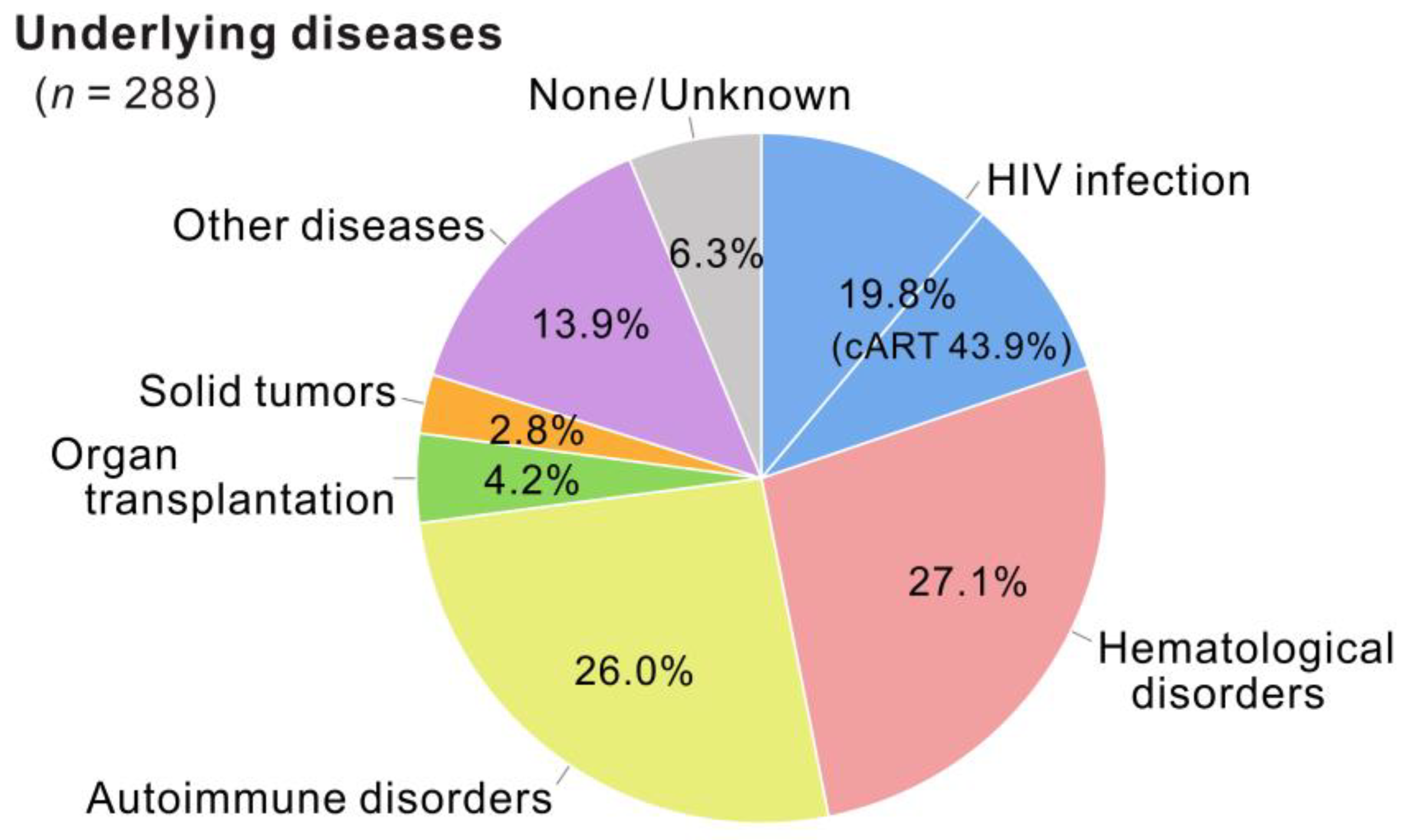
3.4. Categories of Underlying Conditions of Patients with JCV-Positive CSF
3.5. Patients with JCV-Positive CSF and Hematological Disorders
3.6. Patients with JCV-Positive CSF and Autoimmune Disorders
3.7. Patients with JCV-Positive CSF and Other Underlying Diseases
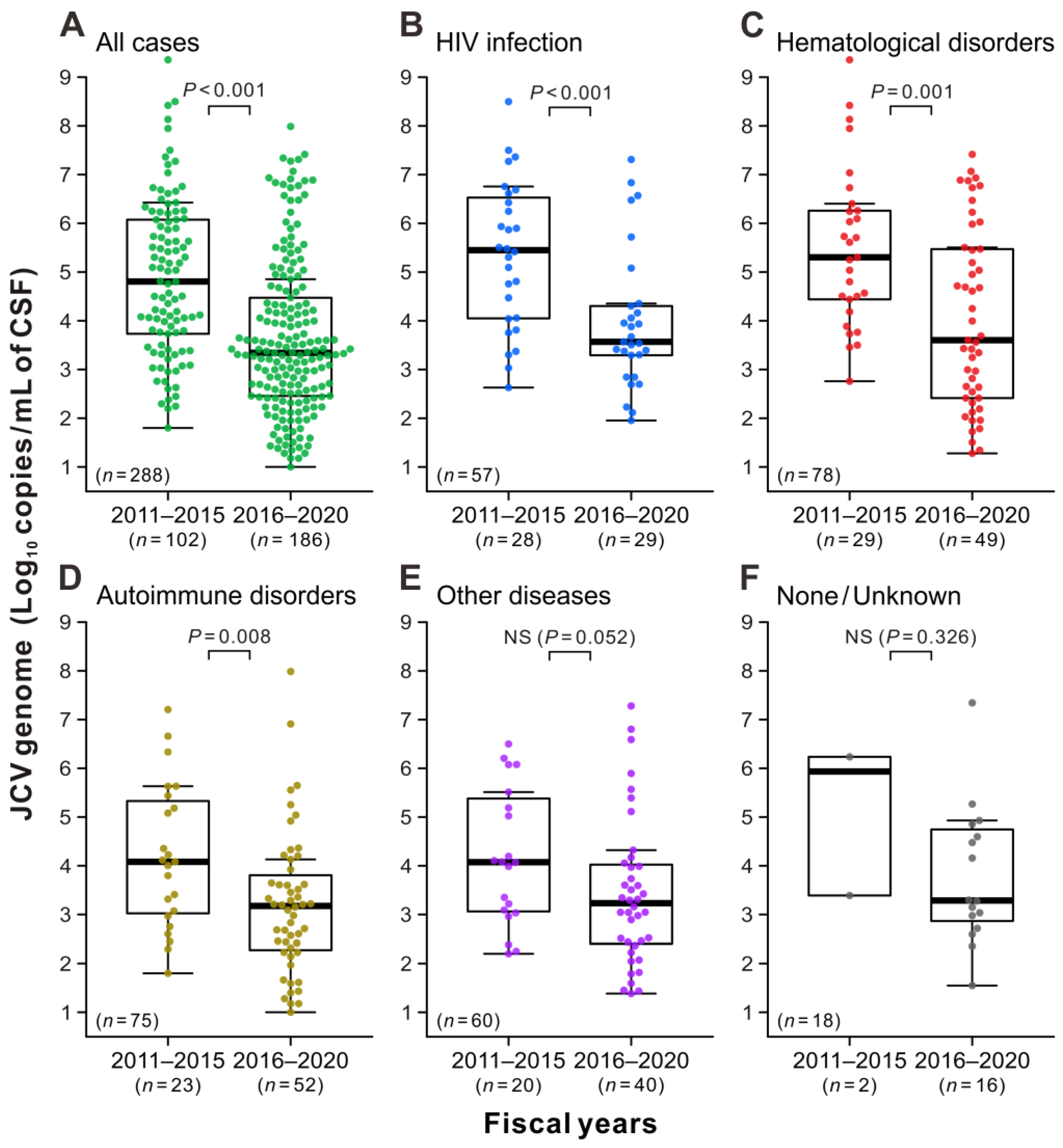
3.8. Copy Numbers of JCV in the CSF
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Major, E.O.; Yousry, T.A.; Clifford, D.B. Pathogenesis of Progressive Multifocal Leukoencephalopathy and Risks Associated with Treatments for Multiple Sclerosis: A Decade of Lessons Learned. Lancet Neurol. 2018, 17, 467–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortese, I.; Reich, D.S.; Nath, A. Progressive Multifocal Leukoencephalopathy and the Spectrum of JC Virus-Related Disease. Nat. Rev. Neurol. 2021, 17, 37–51. [Google Scholar] [CrossRef] [PubMed]
- Pavlovic, D.; Patel, M.A.; Patera, A.C.; Peterson, I. Progressive Multifocal Leukoencephalopathy Consortium. T Cell Deficiencies as a Common Risk Factor for Drug Associated Progressive Multifocal Leukoencephalopathy. Immunobiology 2018, 223, 508–517. [Google Scholar] [CrossRef] [PubMed]
- Shishido-Hara, Y. Progressive Multifocal Leukoencephalopathy and Promyelocytic Leukemia Nuclear Bodies: A Review of Clinical, Neuropathological, and Virological Aspects of JC Virus-Induced Demyelinating Disease. Acta Neuropathol. 2010, 120, 403–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, P.J.; Siddell, S.G.; Lefkowitz, E.J.; Mushegian, A.R.; Adriaenssens, E.M.; Alfenas-Zerbini, P.; Dempsey, D.M.; Dutilh, B.E.; García, M.L.; Curtis Hendrickson, R.; et al. Recent Changes to Virus Taxonomy Ratified by the International Committee on Taxonomy of Viruses (2022). Arch. Virol. 2022, 167, 2429–2440. [Google Scholar] [CrossRef] [PubMed]
- ICTV Genus: Betapolyomavirus | ICTV. Available online: https://ictv.global/report/chapter/polyomaviridae/polyomaviridae/betapolyomavirus (accessed on 3 March 2023).
- Dörries, K. Molecular Biology and Pathogenesis of Human Polyomavirus Infections. Dev. Biol. Stand. 1998, 94, 71–79. [Google Scholar]
- Zheng, H.-Y.; Kitamura, T.; Takasaka, T.; Chen, Q.; Yogo, Y. Unambiguous Identification of JC Polyomavirus Strains Transmitted from Parents to Children. Arch. Virol. 2004, 149, 261–273. [Google Scholar] [CrossRef]
- Ferenczy, M.W.; Marshall, L.J.; Nelson, C.D.S.; Atwood, W.J.; Nath, A.; Khalili, K.; Major, E.O. Molecular Biology, Epidemiology, and Pathogenesis of Progressive Multifocal Leukoencephalopathy, the JC Virus-Induced Demyelinating Disease of the Human Brain. Clin. Microbiol. Rev. 2012, 25, 471–506. [Google Scholar] [CrossRef] [Green Version]
- Monaco, M.C.; Atwood, W.J.; Gravell, M.; Tornatore, C.S.; Major, E.O. JC Virus Infection of Hematopoietic Progenitor Cells, Primary B Lymphocytes, and Tonsillar Stromal Cells: Implications for Viral Latency. J. Virol. 1996, 70, 7004–7012. [Google Scholar] [CrossRef] [Green Version]
- Marzocchetti, A.; Wuthrich, C.; Tan, C.S.; Tompkins, T.; Bernal-Cano, F.; Bhargava, P.; Ropper, A.H.; Koralnik, I.J. Rearrangement of the JC Virus Regulatory Region Sequence in the Bone Marrow of a Patient with Rheumatoid Arthritis and Progressive Multifocal Leukoencephalopathy. J. Neurovirol. 2008, 14, 455–458. [Google Scholar] [CrossRef] [Green Version]
- Tan, C.S.; Dezube, B.J.; Bhargava, P.; Autissier, P.; Wüthrich, C.; Miller, J.; Koralnik, I.J. Detection of JC Virus DNA and Proteins in the Bone Marrow of HIV-Positive and HIV-Negative Patients: Implications for Viral Latency and Neurotropic Transformation. J. Infect. Dis. 2009, 199, 881–888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egli, A.; Infanti, L.; Dumoulin, A.; Buser, A.; Samaridis, J.; Stebler, C.; Gosert, R.; Hirsch, H.H. Prevalence of Polyomavirus BK and JC Infection and Replication in 400 Healthy Blood Donors. J. Infect. Dis. 2009, 199, 837–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ault, G.S.; Stoner, G.L. Human Polyomavirus JC Promoter/Enhancer Rearrangement Patterns from Progressive Multifocal Leukoencephalopathy Brain Are Unique Derivatives of a Single Archetypal Structure. J. Gen. Virol. 1993, 74, 1499–1507. [Google Scholar] [CrossRef]
- Yogo, Y.; Zhong, S.; Shibuya, A.; Kitamura, T.; Homma, Y. Transcriptional Control Region Rearrangements Associated with the Evolution of JC Polyomavirus. Virology 2008, 380, 118–123. [Google Scholar] [CrossRef] [Green Version]
- White, M.K.; Khalili, K. Pathogenesis of Progressive Multifocal Leukoencephalopathy-Revisited. J. Infect. Dis. 2011, 203, 578–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleinschmidt-DeMasters, B.K.; Tyler, K.L. Progressive Multifocal Leukoencephalopathy Complicating Treatment with Natalizumab and Interferon Beta-1a for Multiple Sclerosis. N. Engl. J. Med. 2005, 353, 369–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langer-Gould, A.; Atlas, S.W.; Green, A.J.; Bollen, A.W.; Pelletier, D. Progressive Multifocal Leukoencephalopathy in a Patient Treated with Natalizumab. N. Engl. J. Med. 2005, 353, 375–381. [Google Scholar] [CrossRef] [Green Version]
- Van Assche, G.; Van Ranst, M.; Sciot, R.; Dubois, B.; Vermeire, S.; Noman, M.; Verbeeck, J.; Geboes, K.; Robberecht, W.; Rutgeerts, P. Progressive Multifocal Leukoencephalopathy after Natalizumab Therapy for Crohn’s Disease. N. Engl. J. Med. 2005, 353, 362–368. [Google Scholar] [CrossRef] [Green Version]
- Seppälä, H.; Virtanen, E.; Saarela, M.; Laine, P.; Paulín, L.; Mannonen, L.; Auvinen, P.; Auvinen, E. Single-Molecule Sequencing Revealing the Presence of Distinct JC Polyomavirus Populations in Patients with Progressive Multifocal Leukoencephalopathy. J. Infect. Dis. 2017, 215, 889–895. [Google Scholar] [CrossRef] [Green Version]
- Ciardi, M.R.; Zingaropoli, M.A.; Iannetta, M.; Prezioso, C.; Perri, V.; Pasculli, P.; Lichtner, M.; d’Ettorre, G.; Altieri, M.; Conte, A.; et al. JCPyV NCCR Analysis in PML Patients with Different Risk Factors: Exploring Common Rearrangements as Essential Changes for Neuropathogenesis. Virol. J. 2020, 17, 23. [Google Scholar] [CrossRef] [Green Version]
- Nakamichi, K.; Shimokawa, T. Database and Statistical Analyses of Transcription Factor Binding Sites in the Non-Coding Control Region of JC Virus. Viruses 2021, 13, 2314. [Google Scholar] [CrossRef] [PubMed]
- Wilczek, M.P.; Pike, A.M.C.; Craig, S.E.; Maginnis, M.S.; King, B.L. Rearrangement in the Hypervariable Region of JC Polyomavirus Genomes Isolated from Patient Samples and Impact on Transcription Factor-Binding Sites and Disease Outcomes. Int. J. Mol. Sci. 2022, 23, 5699. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.S.; Koralnik, I.J. Progressive Multifocal Leukoencephalopathy and Other Disorders Caused by JC Virus: Clinical Features and Pathogenesis. Lancet Neurol. 2010, 9, 425–437. [Google Scholar] [CrossRef] [Green Version]
- Khanna, N.; Elzi, L.; Mueller, N.J.; Garzoni, C.; Cavassini, M.; Fux, C.A.; Vernazza, P.; Bernasconi, E.; Battegay, M.; Hirsch, H.H.; et al. Incidence and Outcome of Progressive Multifocal Leukoencephalopathy over 20 Years of the Swiss HIV Cohort Study. Clin. Infect. Dis. 2009, 48, 1459–1466. [Google Scholar] [CrossRef]
- Brew, B.J.; Davies, N.W.S.; Cinque, P.; Clifford, D.B.; Nath, A. Progressive Multifocal Leukoencephalopathy and Other Forms of JC Virus Disease. Nat. Rev. Neurol. 2010, 6, 667–679. [Google Scholar] [CrossRef] [PubMed]
- Berger, J.R.; Cree, B.A.; Greenberg, B.; Hemmer, B.; Ward, B.J.; Dong, V.M.; Merschhemke, M. Progressive Multifocal Leukoencephalopathy after Fingolimod Treatment. Neurology 2018, 90, e1815–e1821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kothary, N.; Diak, I.-L.; Brinker, A.; Bezabeh, S.; Avigan, M.; Dal Pan, G. Progressive Multifocal Leukoencephalopathy Associated with Efalizumab Use in Psoriasis Patients. J. Am. Acad. Dermatol. 2011, 65, 546–551. [Google Scholar] [CrossRef]
- Keene, D.L.; Legare, C.; Taylor, E.; Gallivan, J.; Cawthorn, G.M.; Vu, D. Monoclonal Antibodies and Progressive Multifocal Leukoencephalopathy. Can. J. Neurol. Sci. 2011, 38, 565–571. [Google Scholar] [CrossRef]
- Molloy, E.S.; Calabrese, L.H. Progressive Multifocal Leukoencephalopathy Associated with Immunosuppressive Therapy in Rheumatic Diseases: Evolving Role of Biologic Therapies. Arthritis Rheumatol. 2012, 64, 3043–3051. [Google Scholar] [CrossRef]
- Carson, K.R.; Newsome, S.D.; Kim, E.J.; Wagner-Johnston, N.D.; von Geldern, G.; Moskowitz, C.H.; Moskowitz, A.J.; Rook, A.H.; Jalan, P.; Loren, A.W.; et al. Progressive Multifocal Leukoencephalopathy Associated with Brentuximab Vedotin Therapy: A Report of 5 Cases from the Southern Network on Adverse Reactions (SONAR) Project. Cancer 2014, 120, 2464–2471. [Google Scholar] [CrossRef] [Green Version]
- Melis, M.; Biagi, C.; Småbrekke, L.; Nonino, F.; Buccellato, E.; Donati, M.; Vaccheri, A.; Motola, D. Drug-Induced Progressive Multifocal Leukoencephalopathy: A Comprehensive Analysis of the WHO Adverse Drug Reaction Database. CNS Drugs 2015, 29, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Maas, R.P.P.W.M.; Muller-Hansma, A.H.G.; Esselink, R.A.J.; Murk, J.-L.; Warnke, C.; Killestein, J.; Wattjes, M.P. Drug-Associated Progressive Multifocal Leukoencephalopathy: A Clinical, Radiological, and Cerebrospinal Fluid Analysis of 326 Cases. J. Neurol. 2016, 263, 2004–2021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raisch, D.W.; Rafi, J.A.; Chen, C.; Bennett, C.L. Detection of Cases of Progressive Multifocal Leukoencephalopathy Associated with New Biologicals and Targeted Cancer Therapies from the FDA’s Adverse Event Reporting System. Expert Opin. Drug Saf. 2016, 15, 1003–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agyemang, E.; Bailey, L.; Talbot, J. Additional Risk Minimisation Measures for Medicinal Products in the European Union: A Review of the Implementation and Effectiveness of Measures in the United Kingdom by One Marketing Authorisation Holder. Pharm. Med. 2017, 31, 101–112. [Google Scholar] [CrossRef] [Green Version]
- Colin, O.; Favrelière, S.; Quillet, A.; Neau, J.-P.; Houeto, J.-L.; Lafay-Chebassier, C.; Pérault-Pochat, M.-C. French Pharmacovigilance Network Drug-Induced Progressive Multifocal Leukoencephalopathy: A Case/Noncase Study in the French Pharmacovigilance Database. Fundam. Clin. Pharmacol. 2017, 31, 237–244. [Google Scholar] [CrossRef]
- Oshima, Y.; Tanimoto, T.; Yuji, K.; Tojo, A. Drug-Associated Progressive Multifocal Leukoencephalopathy in Multiple Sclerosis Patients. Mult. Scler. 2019, 25, 1141–1149. [Google Scholar] [CrossRef]
- Butzkueven, H.; Moore, N.; Aydemir, A.; Sõnajalg, J.; Bezemer, I.; Korhonen, P.; Sabidó, M. CLARION Study Group The CLARION Study Design and Status Update: A Long-Term, Registry-Based Study Evaluating Adverse Events of Special Interest in Patients with Relapsing Multiple Sclerosis Newly Started on Cladribine Tablets. Curr. Med. Res. Opin. 2022, 38, 1167–1176. [Google Scholar] [CrossRef]
- Hagan, J.B.; Ender, E.; Divekar, R.D.; Pongdee, T.; Rank, M.A. Risk for Postmarket Black Box Warnings in FDA-Approved Monoclonal Antibodies. Mayo Clin. Proc. Innov. Qual. Outcomes 2022, 6, 69–76. [Google Scholar] [CrossRef]
- Netravathi, M.; Mahadevan, A.; Satishchandra, P.; Shobha, N.; Mailankody, P.; Kandavel, T.; Jitender, S.; Anantaram, G.; Nagarathna, S.; Govekar, S.; et al. Progressive Multifocal Leukoencephalopathy (PML) Associated with HIV Clade C--Is Not Uncommon. J. Neurovirol. 2013, 19, 198–208. [Google Scholar] [CrossRef]
- Sainz-de-la-Maza, S.; Casado, J.L.; Pérez-Elías, M.J.; Moreno, A.; Quereda, C.; Moreno, S.; Corral, I. Incidence and Prognosis of Immune Reconstitution Inflammatory Syndrome in HIV-Associated Progressive Multifocal Leucoencephalopathy. Eur. J. Neurol. 2016, 23, 919–925. [Google Scholar] [CrossRef]
- Graf, L.M.; Rosenkranz, S.C.; Hölzemer, A.; Hagel, C.; Goebell, E.; Jordan, S.; Friese, M.A.; Addo, M.M.; Schulze Zur Wiesch, J.; Beisel, C. Clinical Presentation and Disease Course of 37 Consecutive Cases of Progressive Multifocal Leukoencephalopathy (PML) at a German Tertiary-Care Hospital: A Retrospective Observational Study. Front. Neurol. 2021, 12, 632535. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Wu, H.; Subapriya, R.; Kaur, A.; Pasham, S.R.; Upadhaya, R.; Sriwastava, S. Single-Center Experience on Progressive Multifocal Leukoencephalopathy (PML) Cases, Neuroimaging Relevance, and Management at West Virginia University (WVU). J. Med. Virol. 2022, 94, 4015–4022. [Google Scholar] [CrossRef] [PubMed]
- Kartau, M.; Auvinen, E.; Verkkoniemi-Ahola, A.; Mannonen, L.; Helanterä, I.; Anttila, V.-J. JC Polyomavirus DNA Detection in Clinical Practice. J. Clin. Virol. 2022, 146, 105051. [Google Scholar] [CrossRef] [PubMed]
- Antinori, A.; Cingolani, A.; Lorenzini, P.; Giancola, M.L.; Uccella, I.; Bossolasco, S.; Grisetti, S.; Moretti, F.; Vigo, B.; Bongiovanni, M.; et al. Clinical Epidemiology and Survival of Progressive Multifocal Leukoencephalopathy in the Era of Highly Active Antiretroviral Therapy: Data from the Italian Registry Investigative Neuro AIDS (IRINA). J. Neurovirol. 2003, 9, 47–53. [Google Scholar] [CrossRef]
- Marzocchetti, A.; Tompkins, T.; Clifford, D.B.; Gandhi, R.T.; Kesari, S.; Berger, J.R.; Simpson, D.M.; Prosperi, M.; De Luca, A.; Koralnik, I.J. Determinants of Survival in Progressive Multifocal Leukoencephalopathy. Neurology 2009, 73, 1551–1558. [Google Scholar] [CrossRef] [Green Version]
- Mateen, F.J.; Muralidharan, R.; Carone, M.; van de Beek, D.; Harrison, D.M.; Aksamit, A.J.; Gould, M.S.; Clifford, D.B.; Nath, A. Progressive Multifocal Leukoencephalopathy in Transplant Recipients. Ann. Neurol. 2011, 70, 305–322. [Google Scholar] [CrossRef] [Green Version]
- Jamilloux, Y.; Néel, A.; Lecouffe-Desprets, M.; Fèvre, A.; Kerever, S.; Guillon, B.; Bouvry, D.; Varron, L.; Redares, C.; Dominique, S.; et al. Progressive Multifocal Leukoencephalopathy in Patients with Sarcoidosis. Neurology 2014, 82, 1307–1313. [Google Scholar] [CrossRef]
- Kartau, M.; Verkkoniemi-Ahola, A.; Paetau, A.; Palomäki, M.; Janes, R.; Ristola, M.; Lappalainen, M.; Anttila, V.-J. The Incidence and Predisposing Factors of John Cunningham Virus-Induced Progressive Multifocal Leukoencephalopathy in Southern Finland: A Population-Based Study. Open Forum Infect. Dis. 2019, 6, ofz024. [Google Scholar] [CrossRef]
- Dalla-Pozza, P.; Hentzien, M.; Allavena, C.; Doe de Maindreville, A.; Bouiller, K.; Valantin, M.-A.; Lafont, E.; Zaegel-Faucher, O.; Cheret, A.; Martin-Blondel, G.; et al. Progressive Multifocal Leukoencephalopathy in Patients with Immunovirological Control and at Least 6 Months of Combination Antiretroviral Therapy. AIDS 2022, 36, 539–549. [Google Scholar] [CrossRef]
- Neff, R.T.; Hurst, F.P.; Falta, E.M.; Bohen, E.M.; Lentine, K.L.; Dharnidharka, V.R.; Agodoa, L.Y.; Jindal, R.M.; Yuan, C.M.; Abbott, K.C. Progressive Multifocal Leukoencephalopathy and Use of Mycophenolate Mofetil after Kidney Transplantation. Transplantation 2008, 86, 1474–1478. [Google Scholar] [CrossRef]
- Molloy, E.S.; Calabrese, L.H. Progressive Multifocal Leukoencephalopathy: A National Estimate of Frequency in Systemic Lupus Erythematosus and Other Rheumatic Diseases. Arthritis Rheumatol. 2009, 60, 3761–3765. [Google Scholar] [CrossRef] [PubMed]
- Amend, K.L.; Turnbull, B.; Foskett, N.; Napalkov, P.; Kurth, T.; Seeger, J. Incidence of Progressive Multifocal Leukoencephalopathy in Patients without HIV. Neurology 2010, 75, 1326–1332. [Google Scholar] [CrossRef] [PubMed]
- Christensen, K.L.Y.; Holman, R.C.; Hammett, T.A.; Belay, E.D.; Schonberger, L.B. Progressive Multifocal Leukoencephalopathy Deaths in the USA, 1979–2005. Neuroepidemiology 2010, 35, 178–184. [Google Scholar] [CrossRef]
- Carvour, M.L.; Harms, J.P.; Lynch, C.F.; Mayer, R.R.; Meier, J.L.; Liu, D.; Torner, J.C. Differential Survival for Men and Women with HIV/AIDS-Related Neurologic Diagnoses. PLoS ONE 2015, 10, e0123119. [Google Scholar] [CrossRef] [PubMed]
- Melliez, H.; Mary-Krause, M.; Bocket, L.; Guiguet, M.; Abgrall, S.; De Truchis, P.; Katlama, C.; Martin-Blondel, G.; Henn, A.; Revest, M.; et al. Risk of Progressive Multifocal Leukoencephalopathy in the Combination Antiretroviral Therapy Era in the French Hospital Database on Human Immunodeficiency Virus (ANRS-C4). Clin. Infect. Dis. 2018, 67, 275–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sipilä, J.O.T.; Soilu-Hänninen, M.; Rautava, P.; Kytö, V. Progressive Multifocal Leukoencephalopathy in Finland: A Cross-Sectional Registry Study. J. Neurol. 2019, 266, 515–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joly, M.; Conte, C.; Cazanave, C.; Le Moing, V.; Tattevin, P.; Delobel, P.; Sommet, A.; Martin-Blondel, G. Progressive Multifocal Leukoencephalopathy: Epidemiology and Spectrum of Predisposing Conditions. Brain 2022, 146, awac237. [Google Scholar] [CrossRef]
- Dastmalchi, M.; Laki, J.; Lundberg, I.E.; Iacobaeus, E. Progressive Multifocal Leukoencephalopathy in a Patient with Polymyositis: Case Report and Literature Review. J. Rheumatol. 2012, 39, 1299–1303. [Google Scholar] [CrossRef] [Green Version]
- Ohara, H.; Kataoka, H.; Nakamichi, K.; Saijo, M.; Ueno, S. Favorable Outcome after Withdrawal of Immunosuppressant Therapy in Progressive Multifocal Leukoencephalopathy after Renal Transplantation: Case Report and Literature Review. J. Neurol. Sci. 2014, 341, 144–146. [Google Scholar] [CrossRef]
- Schwenk, H.; Ramirez-Avila, L.; Sheu, S.-H.; Wuthrich, C.; Waugh, J.; Was, A.; Degirolami, U.; Burchett, S.; Koralnik, I.J.; Ahmed, A. Progressive Multifocal Leukoencephalopathy in Pediatric Patients: Case Report and Literature Review. Pediatr. Infect. Dis. J. 2014, 33, e99–e105. [Google Scholar] [CrossRef] [Green Version]
- Henegar, C.E.; Eudy, A.M.; Kharat, V.; Hill, D.D.; Bennett, D.; Haight, B. Progressive Multifocal Leukoencephalopathy in Patients with Systemic Lupus Erythematosus: A Systematic Literature Review. Lupus 2016, 25, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Fournier, A.; Martin-Blondel, G.; Lechapt-Zalcman, E.; Dina, J.; Kazemi, A.; Verdon, R.; Mortier, E.; de La Blanchardière, A. Immune Reconstitution Inflammatory Syndrome Unmasking or Worsening AIDS-Related Progressive Multifocal Leukoencephalopathy: A Literature Review. Front. Immunol. 2017, 8, 577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueno, T.; Sato, N.; Kon, T.; Haga, R.; Nunomura, J.-I.; Nakamichi, K.; Saijo, M.; Tomiyama, M. Progressive Multifocal Leukoencephalopathy Associated with Thymoma with Immunodeficiency: A Case Report and Literature Review. BMC Neurol. 2018, 18, 37. [Google Scholar] [CrossRef] [Green Version]
- Ishii, K.; Yamamoto, F.; Homma, S.; Okada, Y.; Nakamichi, K.; Saijo, M.; Tamaoka, A. Probable Progressive Multifocal Leukoencephalopathy-Immune Reconstitution Inflammatory Syndrome with Immunosuppressant Dose Reduction Following Lung Transplantation: A Case Report and Literature Review. BMC Neurol. 2019, 19, 263. [Google Scholar] [CrossRef] [Green Version]
- Hamaguchi, M.; Suzuki, K.; Fujita, H.; Uzuka, T.; Matsuda, H.; Shishido-Hara, Y.; Arai, S.; Nakamura, T.; Kikuchi, S.; Nakamichi, K.; et al. Successful Treatment of Non-HIV Progressive Multifocal Leukoencephalopathy: Case Report and Literature Review. J. Neurol. 2020, 267, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Breville, G.; Koralnik, I.J.; Lalive, P.H. Brainstem Progressive Multifocal Leukoencephalopathy. Eur. J. Neurol. 2021, 28, 1016–1021. [Google Scholar] [CrossRef]
- Koutsavlis, I. Progressive Multifocal Leukoencephalopathy in Multiple Myeloma. A Literature Review and Lessons to Learn. Ann. Hematol. 2021, 100, 1–10. [Google Scholar] [CrossRef]
- Edahiro, T.; Fukushima, N.; Otani, T.; Nakamori, M.; Nakamichi, K.; Chishaki, R.; Fujino, K.; Mino, T.; Yoshida, T.; Sugihara, S.; et al. Progressive Multifocal Leukoencephalopathy in Relapsed Ph+ Acute Lymphoblastic Leukemia after Cord Blood Transplantation and Blinatumomab Treatment: A Case Report and Literature Review. Acta Haematol. 2022, 145, 655–660. [Google Scholar] [CrossRef]
- Sriwastava, S.; Khan, E.; Khalid, S.H.; Kaur, A.; Feizi, P. Progressive Multifocal Leukoencephalopathy in an Immunocompetent Patient: A Case Report and Review of Literature. J. Med. Virol. 2022, 94, 2860–2869. [Google Scholar] [CrossRef]
- Berger, J.R.; Aksamit, A.J.; Clifford, D.B.; Davis, L.; Koralnik, I.J.; Sejvar, J.J.; Bartt, R.; Major, E.O.; Nath, A. PML Diagnostic Criteria: Consensus Statement from the AAN Neuroinfectious Disease Section. Neurology 2013, 80, 1430–1438. [Google Scholar] [CrossRef] [Green Version]
- Nakamichi, K.; Mizusawa, H.; Yamada, M.; Kishida, S.; Miura, Y.; Shimokawa, T.; Takasaki, T.; Lim, C.-K.; Kurane, I.; Saijo, M. Characteristics of Progressive Multifocal Leukoencephalopathy Clarified through Internet-Assisted Laboratory Surveillance in Japan. BMC Neurol. 2012, 12, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamichi, K.; Kishida, S.; Tanaka, K.; Suganuma, A.; Sano, Y.; Sano, H.; Kanda, T.; Maeda, N.; Kira, J.-I.; Itoh, A.; et al. Sequential Changes in the Non-Coding Control Region Sequences of JC Polyomaviruses from the Cerebrospinal Fluid of Patients with Progressive Multifocal Leukoencephalopathy. Arch. Virol. 2013, 158, 639–650. [Google Scholar] [CrossRef]
- Nakamichi, K.; Tajima, S.; Lim, C.-K.; Saijo, M. High-Resolution Melting Analysis for Mutation Scanning in the Non-Coding Control Region of JC Polyomavirus from Patients with Progressive Multifocal Leukoencephalopathy. Arch. Virol. 2014, 159, 1687–1696. [Google Scholar] [CrossRef] [PubMed]
- Nakamichi, K.; Kawamoto, M.; Ishii, J.; Saijo, M. Improving Detection of JC Virus by Ultrafiltration of Cerebrospinal Fluid before Polymerase Chain Reaction for the Diagnosis of Progressive Multifocal Leukoencephalopathy. BMC Neurol. 2019, 19, 252. [Google Scholar] [CrossRef] [Green Version]
- Nakamichi, K.; Inoue, N.; Shimokawa, T.; Kurane, I.; Lim, C.-K.; Saijo, M. Detection of Human Herpesviruses in the Cerebrospinal Fluid from Patients Diagnosed with or Suspected of Having Progressive Multifocal Leukoencephalopathy. BMC Neurol. 2013, 13, 200. [Google Scholar] [CrossRef] [Green Version]
- Nakamichi, K.; Kurane, I.; Saijo, M. Evaluation of a Quantitative Real-Time PCR Assay for the Detection of JC Polyomavirus DNA in Cerebrospinal Fluid without Nucleic Acid Extraction. Jpn. J. Infect. Dis. 2011, 64, 211–216. [Google Scholar] [CrossRef]
- Nakamichi, K.; Lim, C.-K.; Saijo, M. Stability of JC Virus DNA in Cerebrospinal Fluid Specimens Preserved with Guanidine Lysis Buffer for Quantitative PCR Testing. Jpn. J. Infect. Dis. 2014, 67, 307–310. [Google Scholar] [CrossRef] [Green Version]
- Result of the Population Estimates: Statistics Bureau Statistics Bureau. Available online: https://www.stat.go.jp/english/data/jinsui/2.html (accessed on 3 March 2023).
- Matsuoka, S.; Nagashima, M.; Sadamasu, K.; Mori, H.; Kawahata, T.; Zaitsu, S.; Nakamura, A.; de Souza, M.S.; Matano, T. Estimating HIV-1 Incidence in Japan from the Proportion of Recent Infections. Prev. Med. Rep. 2019, 16, 100994. [Google Scholar] [CrossRef]
- Anand, P.; Hotan, G.C.; Vogel, A.; Venna, N.; Mateen, F.J. Progressive Multifocal Leukoencephalopathy: A 25-Year Retrospective Cohort Study. Neurol. Neuroimmunol. Neuroinflamm. 2019, 6, e618. [Google Scholar] [CrossRef] [Green Version]
- Govender, R.D.; Hashim, M.J.; Khan, M.A.; Mustafa, H.; Khan, G. Global Epidemiology of HIV/AIDS: A Resurgence in North America and Europe. J. Epidemiol. Glob. Health 2021, 11, 296–301. [Google Scholar] [CrossRef]
- Nakahara, J.; Tomaske, L.; Kume, K.; Takata, T.; Kamada, M.; Deguchi, K.; Kufukihara, K.; Schneider, R.; Gold, R.; Ayzenberg, I. Three Cases of Non-Carryover Fingolimod-PML: Is the Risk in Japan Increased? Neurol. Neuroimmunol. Neuroinflamm. 2019, 6, e559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawachi, I.; Otaka, H.; Iwasaki, K.; Takeshima, T.; Ueda, K. Treatment Status and Healthcare Cost Trends for Patients with Multiple Sclerosis in Japan: A Claims Database Analysis. Neurol. Ther. 2022, 11, 1253–1268. [Google Scholar] [CrossRef] [PubMed]
- Gheuens, S.; Pierone, G.; Peeters, P.; Koralnik, I.J. Progressive Multifocal Leukoencephalopathy in Individuals with Minimal or Occult Immunosuppression. J. Neurol. Neurosurg. Psychiatry 2010, 81, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Boziki, M.; Metallidis, S.; Habidou, E.; Afrantou, T.; Bakirtzis, C.; Cheva, A.; Finitsis, S.; Grigoriadis, N. Progressive Multifocal Leukoencephalopathy in an Elderly Immunocompetent-Appearing Patient: Relevance with L-Selectin (CD62L) Expression and Immunosenescence. Clin. Neurol. Neurosurg. 2021, 205, 106625. [Google Scholar] [CrossRef] [PubMed]
- World Health Statistics 2022: Monitoring Health for the SDGs, Sustainable Development Goals. Available online: https://www.who.int/publications-detail-redirect/9789240051157 (accessed on 3 March 2023).
- Warnke, C.; von Geldern, G.; Markwerth, P.; Dehmel, T.; Hoepner, R.; Gold, R.; Pawlita, M.; Kümpfel, T.; Mäurer, M.; Stangel, M.; et al. Cerebrospinal Fluid JC Virus Antibody Index for Diagnosis of Natalizumab-Associated Progressive Multifocal Leukoencephalopathy. Ann. Neurol. 2014, 76, 792–801. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | No. (%) of JCV-Positive Cases a | p-Value c | |||||
|---|---|---|---|---|---|---|---|
| Entire Period b | FY2011–2015 | FY2016–2020 | |||||
| HIV infection | 57/210 | (27.1) | 28/135 | (20.7) | 29/75 | (38.7) | 0.006 * |
| Hematological disorders | 78/305 | (25.6) | 29/162 | (17.9) | 49/143 | (34.3) | 0.001 * |
| Autoimmune disorders | 75/331 | (22.7) | 23/135 | (17.0) | 52/196 | (26.5) | 0.045 * |
| Organ transplantation | 12/47 | (25.5) | 6/30 | (20.0) | 6/17 | (35.3) | 0.306 |
| Solid organ tumors | 8/90 | (8.9) | 4/58 | (6.9) | 4/32 | (12.5) | 0.447 |
| Other diseases | 40/171 | (23.4) | 10/105 | (9.5) | 30/66 | (45.5) | <0.001 * |
| None/unknown | 18/383 | (4.7) | 2/246 | (0.8) | 16/137 | (11.7) | <0.001 * |
| Total | 288/1537 | (18.7) | 102/871 | (11.7) | 186/666 | (27.9) | <0.001 * |
| Underlying Disease b | No. (%) of JCV-Positive Cases a | % of Total d | |||||
|---|---|---|---|---|---|---|---|
| FY2011–2015 | FY2016–2020 | Entire Period c | |||||
| Diffuse large B-cell lymphoma | 7/26 | (26.9) | 8/32 | (25.0) | 15/58 | (25.9) | 19.2 |
| Multiple myeloma | 1/3 | (33.3) | 8/19 | (42.1) | 9/22 | (40.9) | 11.5 |
| Chronic lymphocytic leukemia | 3/6 | (50.0) | 5/6 | (83.3) | 8/12 | (66.7) | 10.3 |
| Non-Hodgkin lymphoma (unspecified) | 2/20 | (10.0) | 6/15 | (40.0) | 8/35 | (22.9) | 10.3 |
| Mucosa-associated lymphoid tissue lymphoma | 3/5 | (60.0) | 1/2 | (50.0) | 4/7 | (57.1) | 5.1 |
| Follicular lymphoma | 1/10 | (10.0) | 3/9 | (33.3) | 4/19 | (21.1) | 5.1 |
| Essential thrombocythemia | 0/0 | − e | 3/3 | (100) | 3/3 | (100) | 3.8 |
| Acute myeloid leukemia | 2/19 | (10.5) | 1/6 | (16.7) | 3/25 | (12.0) | 3.8 |
| Adult T-cell leukemia/lymphoma | 2/13 | (15.4) | 1/12 | (8.3) | 3/25 | (12.0) | 3.8 |
| Acute lymphoid leukemia | 1/16 | (6.3) | 2/10 | (20.0) | 3/26 | (11.5) | 3.8 |
| Primary macroglobulinemia | 2/3 | (66.7) | 0/0 | − | 2/3 | (66.7) | 2.6 |
| Idiopathic CD4 lymphocytopenia | 1/2 | (50.0) | 1/1 | (100) | 2/3 | (66.7) | 2.6 |
| Hodgkin lymphoma | 0/4 | (0) | 2/2 | (100) | 2/6 | (33.3) | 2.6 |
| Angioimmunoblastic T-cell lymphoma | 1/1 | (100) | 0/0 | − | 1/1 | (100) | 1.3 |
| Thyroid lymphoma | 1/1 | (100) | 0/0 | − | 1/1 | (100) | 1.3 |
| Small lymphocytic lymphoma | 1/1 | (100) | 0/0 | − | 1/1 | (100) | 1.3 |
| Hypereosinophilic syndrome | 0/0 | − | 1/1 | (100) | 1/1 | (100) | 1.3 |
| Sézary syndrome | 0/0 | − | 1/1 | (100) | 1/1 | (100) | 1.3 |
| Mycosis fungoides | 0/0 | − | 1/1 | (100) | 1/1 | (100) | 1.3 |
| Mantle cell lymphoma | 0/1 | (0) | 1/1 | (100) | 1/2 | (50.0) | 1.3 |
| Lymphoplasmacytic lymphoma | 0/2 | (0) | 1/1 | (100) | 1/3 | (33.3) | 1.3 |
| Aplastic anemia | 0/1 | (0) | 1/2 | (50.0) | 1/3 | (33.3) | 1.3 |
| Lymphoblastic lymphoma | 0/1 | (0) | 1/3 | (33.3) | 1/4 | (25.0) | 1.3 |
| Chronic myeloid leukemia | 1/4 | (25.0) | 0/3 | (0) | 1/7 | (14.3) | 1.3 |
| Myelodysplastic syndrome | 0/5 | (0) | 1/4 | (25.0) | 1/9 | (11.1) | 1.3 |
| Other diseases | 0/18 | (0) | 0/9 | (0) | 0/27 | (0) | 0 |
| Total | 29/162 | (17.9) | 49/143 | (34.3) | 78/305 | (25.6) | 100 |
| Underlying Disease b | No. (%) of JCV-Positive Cases a | % of Total d | |||||
|---|---|---|---|---|---|---|---|
| FY2011–2015 | FY2016–2020 | Entire Period c | |||||
| Systemic lupus erythematosus | 13/36 | (36.1) | 21/37 | (56.8) | 34/73 | (46.6) | 45.3 |
| Rheumatoid arthritis | 2/31 | (6.5) | 8/34 | (23.5) | 10/65 | (15.4) | 13.3 |
| Multiple sclerosis | 1/9 | (11.1) | 6/58 | (10.3) | 7/67 | (10.4) | 9.3 |
| Dermatomyositis | 1/2 | (50.0) | 3/4 | (75.0) | 4/6 | (66.7) | 5.3 |
| Autoimmune hemolytic anemia | 0/0 | − e | 3/3 | (100) | 3/3 | (100) | 4.0 |
| Eosinophilic granulomatosis with polyangiitis | 1/2 | (50.0) | 2/3 | (67.0) | 3/5 | (60.0) | 4.0 |
| Sjögren syndrome | 1/2 | (50.0) | 2/4 | (50.0) | 3/6 | (50.0) | 4.0 |
| Antineutrophil cytoplasmic antibody- associated vasculitis | 1/3 | (33.3) | 2/6 | (33.3) | 3/9 | (33.3) | 4.0 |
| Pemphigus foliaceus | 1/1 | (100) | 1/1 | (100) | 2/2 | (100) | 2.7 |
| Autoimmune hepatitis | 0/1 | (0) | 1/1 | (100) | 1/2 | (50.0) | 1.3 |
| Systemic scleroderma | 0/2 | (0) | 1/1 | (100) | 1/3 | (33.3) | 1.3 |
| Polymyalgia rheumatica | 1/3 | (33.3) | 0/1 | (0) | 1/4 | (25.0) | 1.3 |
| Myelin oligodendrocyte glycoprotein antibody-associated disease | 0/0 | − | 1/4 | (25.0) | 1/4 | (25.0) | 1.3 |
| Granulomatosis with polyangiitis | 1/3 | (33.3) | 0/2 | (0) | 1/5 | (20.0) | 1.3 |
| Microscopic polyangiitis | 0/5 | (0) | 1/2 | (50.0) | 1/7 | (14.3) | 1.3 |
| Other diseases | 0/35 | (0) | 0/35 | (0) | 0/70 | (0) | 0 |
| Total | 23/135 | (17.0) | 52/196 | (26.5) | 75/331 | (22.7) | 100 |
| Underlying Diseases a | Complications | Entire Period (FY2011–2020) | ||
|---|---|---|---|---|
| No. (%) of JCV-Positive Cases b | % of Disease c | |||
| Systemic lupus erythematosus | None | 10/32 | (31.3) | 29.4 |
| Lupus nephritis | 12/22 | (54.5) | 35.3 | |
| Antiphospholipid syndrome | 4/4 | (100) | 11.8 | |
| Lupus nephritis, Sjögren syndrome | 2/2 | (100) | 5.9 | |
| Rheumatoid arthritis | 2/2 | (100) | 5.9 | |
| Sjögren syndrome | 2/5 | (40.0) | 5.9 | |
| Non-Hodgkin lymphoma | 1/1 | (100) | 2.9 | |
| Systemic scleroderma, polymyositis | 1/1 | (100) | 2.9 | |
| Others | 0/4 | (0) | 0 | |
| Rheumatoid arthritis | None | 6/44 | (13.6) | 60.0 |
| Mixed connective tissue disease, malignant lymphoma | 1/1 | (100) | 10.0 | |
| Hodgkin lymphoma | 1/1 | (100) | 10.0 | |
| Non-Hodgkin lymphoma | 1/5 | (20.0) | 10.0 | |
| Chronic kidney disease | 1/6 | (16.7) | 10.0 | |
| Others | 0/8 | (0) | 0 | |
| Multiple sclerosis | None | 7/64 | (10.9) | 100 |
| Rheumatoid arthritis, non-Hodgkin lymphoma | 0/1 | (0) | 0 | |
| Hyperthyroidism | 0/1 | (0) | 0 | |
| Behçet disease | 0/1 | (0) | 0 | |
| Autoimmune hemolytic anemia | None | 2/2 | (100) | 66.7 |
| Malignant lymphoma | 1/1 | (100) | 33.3 | |
| Sjögren syndrome | None | 1/2 | (50.0) | 33.3 |
| Non-Hodgkin lymphoma | 2/2 | (100) | 66.7 | |
| Chronic hepatitis C | 0/1 | (0) | 0 | |
| Interstitial pneumonia | 0/1 | (0) | 0 | |
| ANCA-associated vasculitis | None | 1/6 | (16.7) | 33.3 |
| ANCA-associated glomerulonephritis | 2/2 | (100) | 66.7 | |
| IgG4-related disease | 0/1 | (0) | 0 | |
| Microscopic polyangiitis | None | 0/5 | (0) | 0 |
| Chronic kidney disease, interstitial pneumonia | 0/1 | (0) | 0 | |
| Chronic kidney disease | 1/1 | (100) | 100 | |
| Total | − d | 61/230 | (26.5) | − |
| Category | Subcategory a | Entire Period (FY2011–2020) | ||
|---|---|---|---|---|
| No. (%) of JCV-Positive Cases b | % of Category c | |||
| Organ transplantation | Kidney | 9/32 | (28.1) | 75.0 |
| Liver | 2/12 | (16.7) | 16.7 | |
| Lung | 1/1 | (100) | 8.3 | |
| Heart | 0/2 | (0) | 0 | |
| Solid organ tumors | Liver | 2/14 | (14.3) | 25.0 |
| Hypopharynx | 1/1 | (100) | 12.5 | |
| Thymus | 1/3 | (33.3) | 12.5 | |
| Esophagus | 1/6 | (16.7) | 12.5 | |
| Stomach | 1/7 | (14.3) | 12.5 | |
| Lung | 1/25 | (4.0) | 12.5 | |
| Others d | 1/34 | (2.9) | 12.5 | |
| Brain diseases | − e | 0/25 | (0) | − |
| Heart diseases | − | 0/5 | (0) | − |
| Lung diseases | Interstitial pneumonia | 1/5 | (20.0) | 100 |
| Others | 0/1 | (0) | 0 | |
| Liver diseases | Hepatitis C-related cirrhosis | 2/7 | (28.6) | 66.7 |
| Cirrhosis (unspecified) | 1/2 | (50.0) | 33.3 | |
| Others | 0/8 | (0) | 0 | |
| Kidney diseases | CKD (renal failure) | 10/29 | (34.5) | 62.5 |
| CKD (nephrotic syndrome) | 1/2 | (50.0) | 6.3 | |
| CKD (nephrosclerosis) | 1/3 | (33.3) | 6.3 | |
| CKD (unspecified) | 1/3 | (33.3) | 6.3 | |
| CKD (polycystic kidney disease) | 1/4 | (25.0) | 6.3 | |
| CKD (chronic glomerulonephritis) | 1/7 | (14.3) | 6.3 | |
| CKD (diabetic nephropathy) | 1/9 | (11.1) | 6.3 | |
| Others | 0/2 | (0) | 0 | |
| Infectious diseases | Non-tuberculous mycobacterial infection | 1/1 | (100) | 100 |
| Others | 0/4 | (0) | 0 | |
| Primary immunodeficiency syndromes | Good syndrome | 4/4 | (100) | 66.7 |
| Combined immunodeficiency syndrome | 1/1 | (100) | 16.7 | |
| Chronic granulomatous disease | 1/3 | (33.3) | 16.7 | |
| Others | 0/4 | (0) | 0 | |
| Other diseases | Sarcoidosis | 7/15 | (46.7) | 53.8 |
| Comorbidity f | 5/9 | (55.6) | 38.5 | |
| Amyloidosis | 1/2 | (50.0) | 7.7 | |
| Others | 0/16 | (0) | 0 | |
| Total | − | 60/308 | (19.5) | − |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamichi, K.; Miura, Y.; Shimokawa, T.; Takahashi, K.; Suzuki, T.; Funata, N.; Harada, M.; Mori, K.; Sanjo, N.; Yukitake, M.; et al. Nationwide Laboratory Surveillance of Progressive Multifocal Leukoencephalopathy in Japan: Fiscal Years 2011–2020. Viruses 2023, 15, 968. https://doi.org/10.3390/v15040968
Nakamichi K, Miura Y, Shimokawa T, Takahashi K, Suzuki T, Funata N, Harada M, Mori K, Sanjo N, Yukitake M, et al. Nationwide Laboratory Surveillance of Progressive Multifocal Leukoencephalopathy in Japan: Fiscal Years 2011–2020. Viruses. 2023; 15(4):968. https://doi.org/10.3390/v15040968
Chicago/Turabian StyleNakamichi, Kazuo, Yoshiharu Miura, Toshio Shimokawa, Kenta Takahashi, Tadaki Suzuki, Nobuaki Funata, Masafumi Harada, Koichiro Mori, Nobuo Sanjo, Motohiro Yukitake, and et al. 2023. "Nationwide Laboratory Surveillance of Progressive Multifocal Leukoencephalopathy in Japan: Fiscal Years 2011–2020" Viruses 15, no. 4: 968. https://doi.org/10.3390/v15040968