
Efficacy, Convenience, Safety and Durability of DTG-Based Antiretroviral Therapies: Evidence from a Prospective Study by the Italian MaSTER Cohort
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Outcomes
2.3. Statistical Approach
3. Results
3.1. Patient Characteristics
3.2. DTG Regimen Performance and Rates of Interruption
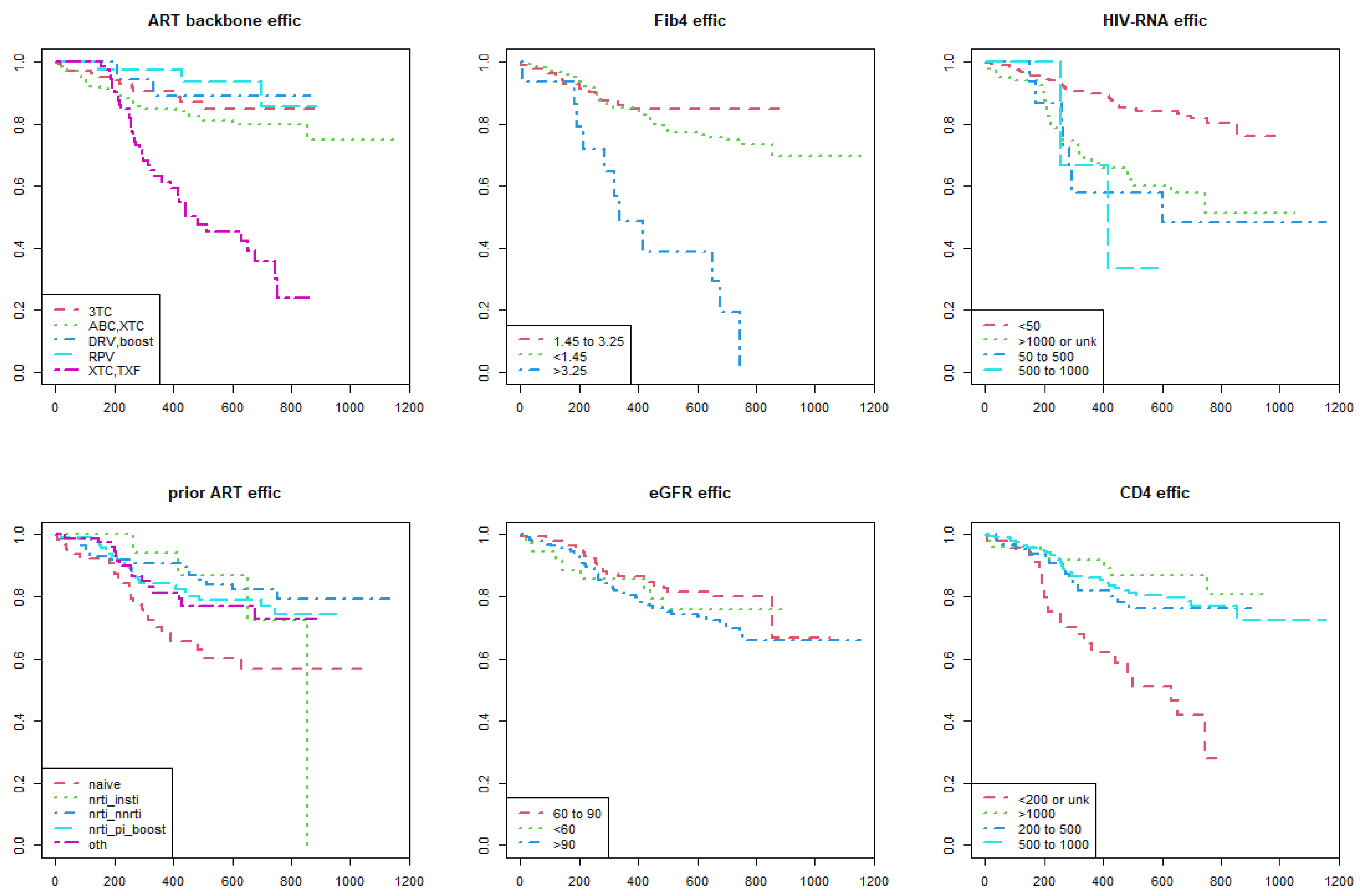
3.3. Associations with Efficacy Events
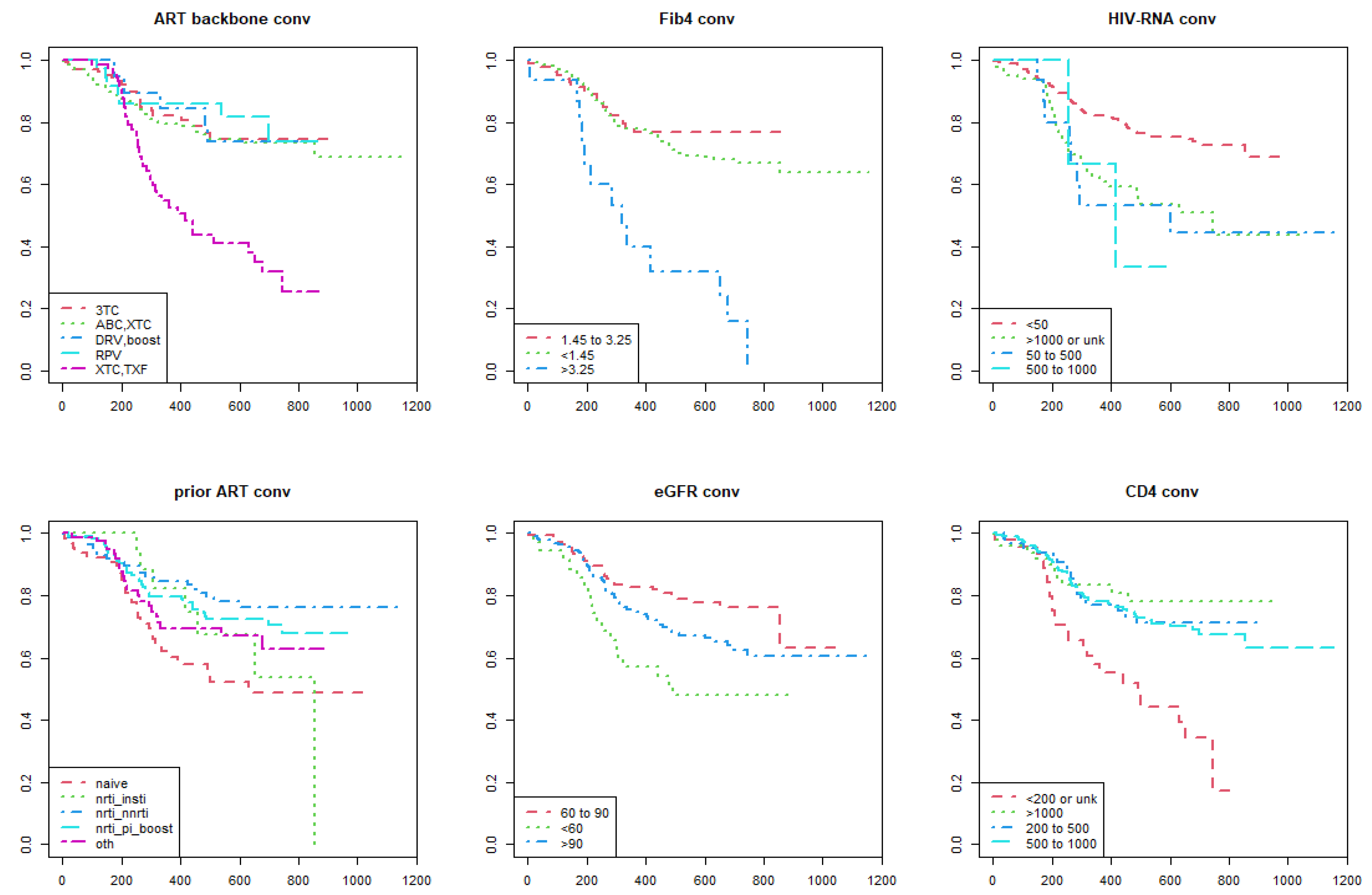
3.4. Associations with Convenience Events
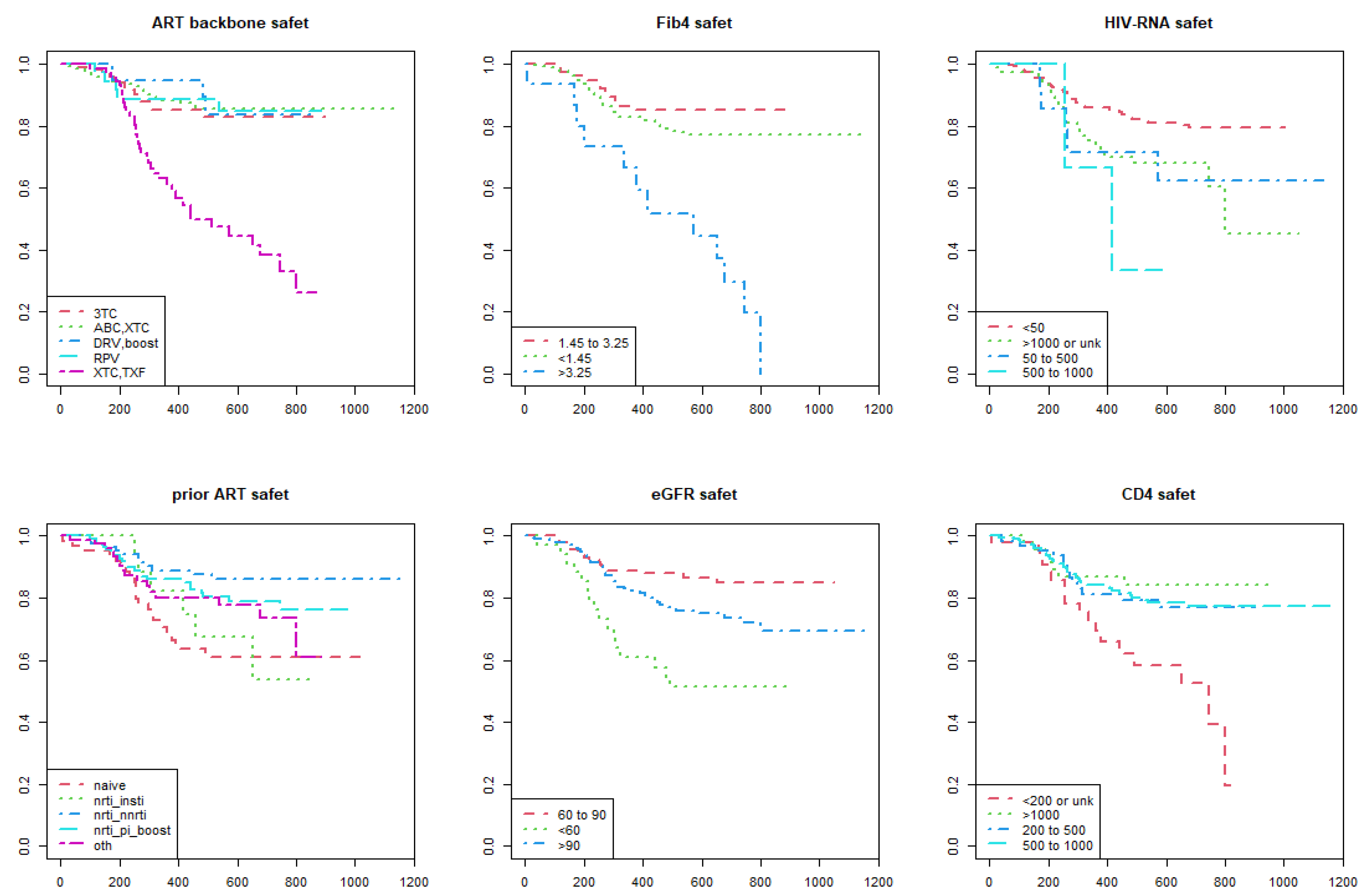
3.5. Associations with Safety Events
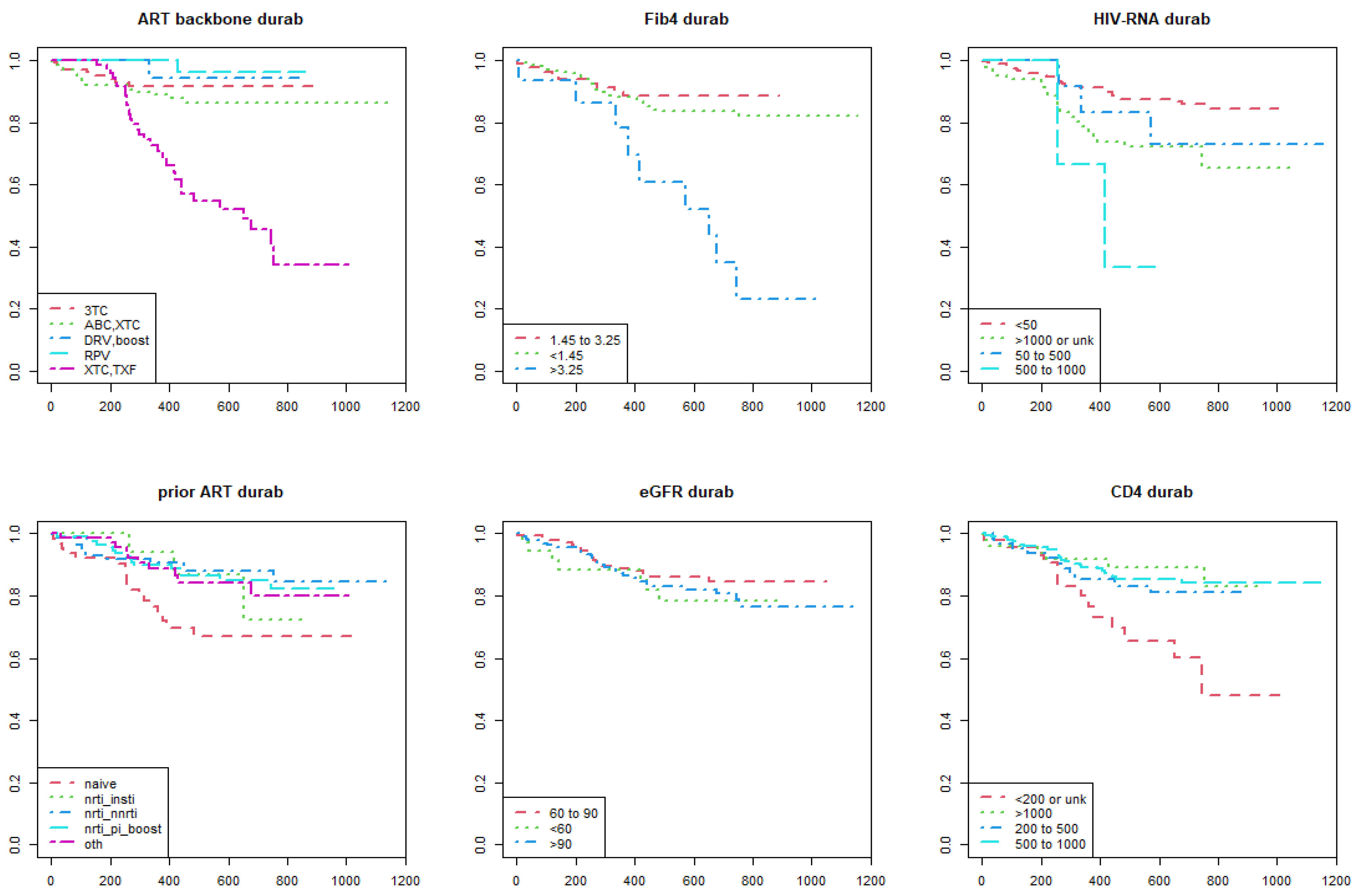
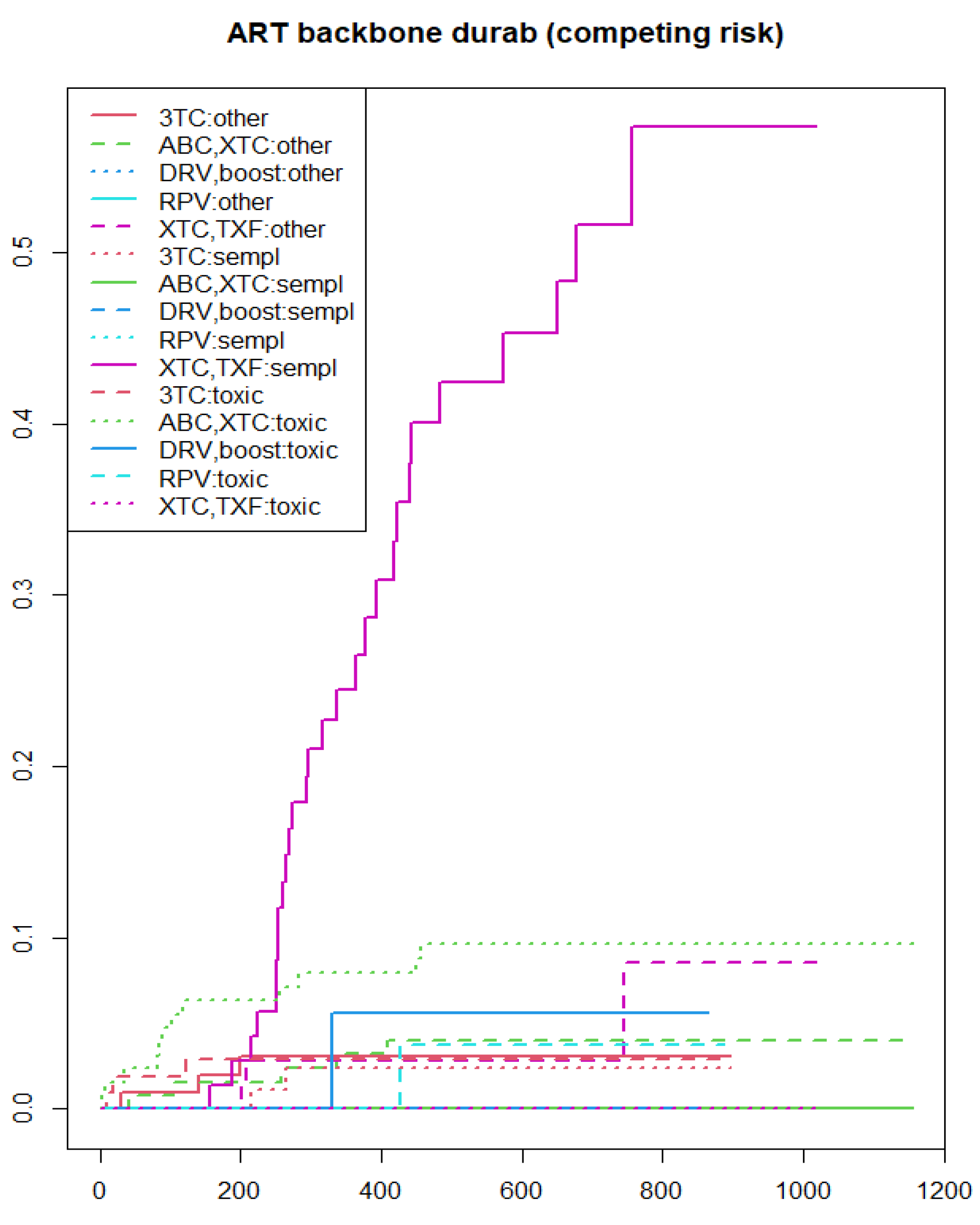
3.6. Associations with Durability Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Department of Health and Human Services. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. Available online: https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-arv (accessed on 16 December 2022).
- Saag, M.S.; Gandhi, R.T.; Hoy, J.F.; Landovitz, R.J.; Thompson, M.A.; Sax, P.E.; Smith, D.M.; Benson, C.A.; Buchbinder, S.P.; Del Rio, C.; et al. Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults: 2020 Recommendations of the International Antiviral Society–USA Panel. JAMA 2020, 324, 1651. [Google Scholar] [CrossRef] [PubMed]
- EACS Guidelines Version 11.1. October 2022. Available online: https://www.google.com.hk/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwjCttGYsIj-AhUiplYBHRn4AGsQFnoECBMQAQ&url=https%3A%2F%2Fwww.eacsociety.org%2Fmedia%2Fguidelines-11.1_final_09-10.pdf&usg=AOvVaw037dzErMAsmQvupsMPixgn (accessed on 18 December 2022).
- Raffi, F.; Rachlis, A.; Stellbrink, H.J.; Hardy, W.D.; Torti, C.; Orkin, C.; Bloch, M.; Podzamczer, D.; Pokrovsky, V.; Pulido, F.; et al. Once-daily dolutegravir versus raltegravir in antiretroviral-naive adults with HIV-1 infection: 48 week results from the randomised, double-blind, non-inferiority SPRING-2 study. Lancet 2013, 381, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Nickel, K.; Halfpenny, N.J.; Snedecor, S.J.; Punekar, Y.S. Comparative efficacy, safety and durability of dolutegravir relative to common core agents in treatment-naïve patients infected with HIV-1: An update on a systematic review and network meta-analysis. BMC Infect Dis. 2021, 21, 222. [Google Scholar] [CrossRef]
- Raffi, F.; Esser, S.; Nunnari, G.; Pérez-Valero, I.; Waters, L. Switching regimens in virologically suppressed HIV-1-infected patients: Evidence base and rationale for integrase strand transfer inhibitor (INSTI)-containing regimens. HIV Med. 2016, 17 (Suppl. S5), 3–16. [Google Scholar] [CrossRef] [PubMed]
- Rich, S.N.; Nasta, P.; Quiros-Roldan, E.; Fusco, P.; Tondinelli, A.; Costa, C.; Fornabaio, C.; Mazzini, N.; Prosperi, M.; Torti, C.; et al. Outcome performance of INSTI-based regimens including the metrics of efficacy, safety, durability and convenience. Poster presentation n° PP261. In Proceedings of the XXI National Congress SIMIT, Rome, Italy, 20–23 November 2022. [Google Scholar]
- Torti, C.; Raffetti, E.; Donato, F.; Castelli, F.; Maggiolo, F.; Angarano, G.; Mazzotta, F.; Gori, A.; Sighinolfi, L.; Pan, A.; et al. Cohort Profile: Standardized Management of Antiretroviral Therapy Cohort (MASTER Cohort). Int. J. Epidemiol. 2017, 46, e12. [Google Scholar] [CrossRef] [PubMed]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef]
- Falcone, E.L.; Mangili, A.; Skinner, S.; Alam, A.; Polak, J.F.; Wanke, C.A. Framingham risk score and early markers of atherosclerosis in a cohort of adults infected with HIV. Antivir. Ther. 2011, 16, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Therneau, T.; Grambsch, P. Modeling Survival Data: Extending the Cox Model; Springer: New York, NY, USA, 2000; Available online: https://CRAN.R-project.org/package=survival (accessed on 16 December 2022).
- Ankan, A.; Wortel, I.M.; Textor, J. Testing Graphical Causal Models Using the R Package “dagitty”. Curr. Protoc. 2021, 1, e45. [Google Scholar] [CrossRef] [PubMed]
- Stekhoven, D.J.; Bühlmann, P. MissForest—Non-parametric missing value imputation for mixed-type data. Bioinformatics 2012, 28, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.K.; Patel, K.K.; Pujari, S.; Patel, J.K.; Kumar, A. Virological outcome and frequency of low-level viremia in patients receiving generic dolutegravir-containing regimen at a large tertiary care clinic in Western India. Indian J. Sex Transm. Dis. AIDS 2021, 42, 31–37. [Google Scholar] [CrossRef]
- Iacob, D.G.; Luminos, M.; Benea, O.E.; Tudor, A.M.; Olariu, C.M.; Iacob, S.A.; Ruta, S. Liver fibrosis progression in a cohort of young HIV and HIV/HBV co-infected patients: A longitudinal study using non-invasive APRI and Fib-4 scores. Front. Med. 2022, 9, 888050. [Google Scholar] [CrossRef]
- Costiniuk, C.T.; Sigal, A.; Jenabian, M.A.; Nijs, P.; Wilson, D. Short communication: Lower baseline CD4 count is associated with a greater propensity toward virological failure in a cohort of South African HIV patients. AIDS Res. Hum. Retrovir. 2014, 30, 531–534. [Google Scholar] [CrossRef] [PubMed]
- Casado, J.L. Renal and Bone Toxicity with the Use of Tenofovir: Understanding at the End. AIDS Rev. 2016, 18, 59–68. [Google Scholar]
- Casado, J.L.; Santiuste, C.; Vazquez, M.; Bañón, S.; Rosillo, M.; Gomez, A.; Perez-Elías, M.J.; Caballero, C.; Rey, J.M.; Moreno, S. Bone mineral density decline according to renal tubular dysfunction and phosphaturia in tenofovir-exposed HIV-infected patients. AIDS 2016, 30, 1423–1431. [Google Scholar] [CrossRef]
- Lapadula, G.; Torti, C.; Maggiolo, F.; Casari, S.; Suter, F.; Minoli, L.; Pezzoli, C.; Pietro, M.D.; Migliorino, G.; Quiros-Roldan, E.; et al. Predictors of clinical progression among HIV-1-positive patients starting HAART with CD4+ T-cell counts > or =200 cells/mm3. Antivir. Ther. 2007, 12, 941–947. [Google Scholar] [CrossRef] [PubMed]
- Antiretroviral Therapy Cohort Collaboration. Importance of Baseline Prognostic Factors with Increasing Time Since Initiation of Highly Active Antiretroviral Therapy: Collaborative Analysis of Cohorts of HIV-1–Infected Patients. J. Acquir. Immune Defic. Syndr. 2007, 46, 607–615. [Google Scholar] [CrossRef] [Green Version]
- O’Halloran, J.A.; Sahrmann, J.; Butler, A.M.; Olsen, M.A.; Powderly, W.G. Brief Report: Integrase Strand Transfer Inhibitors Are Associated with Lower Risk of Incident Cardiovascular Disease in People Living with HIV. J. Acquir. Immune Defic. Syndr. 2020, 84, 396–399. [Google Scholar] [CrossRef]
- Neesgaard, B.; Greenberg, L.; Miró, J.M.; Grabmeier-Pfistershammer, K.; Wandeler, G.; Smith, C.; De Wit, S.; Wit, F.; Pelchen-Matthews, A.; Mussini, C.; et al. Associations between integrase strand-transfer inhibitors and cardiovascular disease in people living with HIV: A multicentre prospective study from the RESPOND cohort consortium. Lancet HIV 2022, 9, e474–e485. [Google Scholar] [CrossRef] [PubMed]
- Rajbhandari, R.; Jun, T.; Khalili, H.; Chung, R.T.; Ananthakrishnan, A.N. HBV/HIV coinfection is associated with poorer outcomes in hospitalized patients with HBV or HIV. J. Viral. Hepat. 2016, 23, 820–829. [Google Scholar] [CrossRef] [Green Version]
- Weber, R.; Ruppik, M.; Rickenbach, M.; Spoerri, A.; Furrer, H.; Battegay, M.; Cavassini, M.; Calmy, A.; Bernasconi, E.; Schmid, P.; et al. Decreasing mortality and changing patterns of causes of death in the Swiss HIV Cohort Study. HIV Med. 2013, 14, 195–207. [Google Scholar] [CrossRef] [PubMed]
- Coffin, C.; Osiowy, C.; Myers, R.; Gill, M.J. Virology and clinical sequelae of long-term antiviral therapy in a North American cohort of hepatitis B virus (HBV)/human immunodeficiency virus type 1 (HIV-1) co-infected patients. J. Clin. Virol. 2013, 57, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Zerbato, J.M.; Avihingsanon, A.; Singh, K.P.; Zhao, W.; Deleage, C.; Rosen, E.; Cottrell, M.L.; Rhodes, A.; Dantanarayana, A.; Tumpach, C.; et al. HIV DNA persists in hepatocytes in people with HIV-hepatitis B co-infection on antiretroviral therapy. EBioMedicine 2023, 87, 104391. [Google Scholar] [CrossRef]
- Ciccullo, A.; Baldin, G.; Borghi, V.; Lagi, F.; Latini, A.; D’Ettorre, G.; Oreni, L.; Fusco, P.; Capetti, A.; Fabbiani, M.; et al. Real-Life Impact of Drug Toxicity on Dolutegravir Tolerability: Clinical Practice Data from a Multicentres Italian Cohort. Viruses 2022, 14, 163. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.K.; Post, F.A.; Arribas, J.R.; Eron, J.J.; Wohl, D.A.; Clarke, A.E.; Sax, P.E.; Stellbrink, H.-J.; Esser, S.; Pozniak, A.L.; et al. Renal safety of tenofovir alafenamide vs. tenofovir disoproxil fumarate: A pooled analysis of 26 clinical trials. AIDS 2019, 33, 1455–1465. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Gui, X.; Ke, H.; Xiong, Y.; Gao, S. Combination antiretroviral therapy is associated with reduction in liver fibrosis scores in patients with HIV and HBV co-infection. AIDS Res. Ther. 2021, 18, 98. [Google Scholar] [CrossRef] [PubMed]
- Mendeni, M.; Focà, E.; Gotti, D.; Ladisa, N.; Angarano, G.; Albini, L.; Castelnuovo, F.; Carosi, G.; Quiros-Roldan, E.; Torti, C. Evaluation of liver fibrosis: Concordance analysis between noninvasive scores (APRI and FIB-4) evolution and predictors in a cohort of HIV-infected patients without hepatitis C and B infection. Clin. Infect. Dis. 2011, 52, 1164–1173. [Google Scholar] [CrossRef] [Green Version]
- Borges, A.H. Combination antiretroviral therapy and cancer risk. Curr. Opin. HIV AIDS 2017, 12, 12–19. [Google Scholar] [CrossRef]
- Prosperi, M.C.F.; Cozzi-Lepri, A.; Castagna, A.; Mussini, C.; Murri, R.; Giacometti, A.; Torti, C.; Costantini, A.; Narciso, P.; Ghinelli, F.; et al. Incidence of malignancies in HIV-infected patients and prognostic role of current CD4 cell count: Evidence from a large Italian cohort study. Clin. Infect. Dis. 2010, 50, 1316–1321. [Google Scholar] [CrossRef]
- Insight Start Study Group. Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection. N. Engl. J. Med. 2015, 373, 795–807. [Google Scholar] [CrossRef] [Green Version]
- Shmakova, A.; Germini, D.; Vassetzky, Y. HIV-1, HAART and cancer: A complex relationship. Int. J. Cancer 2020, 146, 2666–2679. [Google Scholar] [CrossRef]
- Torres, H.; Rallapalli, V.; Saxena, A.; Granwehr, B.; Viola, G.; Ariza-Heredia, E.; Adachi, J.; Chemaly, R.; Marfatia, R.; Jiang, Y.; et al. Efficacy and safety of antiretrovirals in HIV-infected patients with cancer. Clin. Microbiol. Infect. 2014, 20, O672–O679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torti, C.; Lapadula, G.; Antinori, A.; Quirino, T.; Maserati, R.; Castelnuovo, F.; Maggiolo, F.; De Luca, A.; Paraninfo, G.; Antonucci, F.; et al. Hyperbilirubinemia during atazanavir treatment in 2,404 patients in the Italian atazanavir expanded access program and MASTER Cohorts. Infection 2009, 37, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Taramasso, L.; Tatarelli, P.; Ricci, E.; Madeddu, G.; Menzaghi, B.; Squillace, N.; De Socio, G.V.; Martinelli, C.; Gulminetti, R.; Maggi, P.; et al. Improvement of lipid profile after switching from efavirenz or ritonavir-boosted protease inhibitors to rilpivirine or once-daily integrase inhibitors: Results from a large observational cohort study (SCOLTA). BMC Infect. Dis. 2018, 18, 357. [Google Scholar] [CrossRef] [PubMed]
- Sax, P.E.; Erlandson, K.M.; Lake, J.E.; McComsey, G.A.; Orkin, C.; Esser, S.; Brown, T.T.; Rockstroh, J.K.; Wei, X.; Carter, C.C.; et al. Weight Gain Following Initiation of Antiretroviral Therapy: Risk Factors in Randomized Comparative Clinical Trials. Clin. Infect. Dis. 2020, 71, 1379–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazzitelli, M.; Fusco, P.; Brogna, M.; Vallone, A.; D’Argenio, L.; Beradelli, G.; Foti, G.; Mangano, C.; Carpentieri, M.S.; Cosco, L.; et al. Weight of Clinical and Social Determinants of Metabolic Syndrome in People Living with HIV. Viruses 2022, 14, 1339. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics of Full Population (N = 371) | N° or Median | % or (IQR) |
|---|---|---|
| Age (years) | 53 | (45–58) |
| Female sex | 92 | 24.8% |
| Country (Italy) | 309 | 83.3% |
| Year of starting DTG | ||
| 2018 | 21 | 5.7% |
| 2019 | 297 | 80.1% |
| 2020 | 42 | 11.3% |
| 2021 | 11 | 3.0% |
| Prior cART | ||
| Naïve | 71 | 19.1% |
| NRTI/INSTI | 18 | 4.9% |
| NRTI/NNRTI | 87 | 23.5% |
| NRTI/PI-boosted | 127 | 34.2% |
| Others | 68 | 18.3% |
| cART backbone | ||
| FTC/TDF | 48 | 12.9% |
| 3TC | 106 | 28.6% |
| 3TC/ABC | 128 | 34.5% |
| RPV | 36 | 9.7% |
| Cobi/DRV | 18 | 4.9% |
| FTC/TAF | 27 | 7.3% |
| 3TC/TDF | 5 | 1.3% |
| ABC/FTC | 1 | 0.3% |
| DRV/RTV | 2 | 0.5% |
| Mode of transmission | ||
| Other | 25 | 6.7% |
| MSM | 102 | 27.5% |
| PWID | 80 | 21.6% |
| Heterosexual | 164 | 44.2% |
| HBsAg chronic carriers | 7 | 1.9% |
| Positive HCV Ab participants | 9 | 2.4% |
| Prior/baseline cancer | 33 | 8.9% |
| Baseline HIV RNA Log10 copies/mL | 1.7 | (1.7–2.09) |
| Baseline CD4 T-cells/mm3 | 640.5 | (420.25–856.25) |
| Baseline CD8 T-cells/mm3 | 806.5 | (571.75–1112.5) |
| Baseline CD4/CD8 ratio | 0.76 | (0.48–1.1) |
| Baseline FIB-4 score | 1.08 | (0.74–1.55) |
| Baseline eGFR (ml/min) | 92.34 | (79.33–104.02) |
| Baseline Framingham score | 12 | (10–15) |
| DTG regimens performance | ||
| Efficacy events | 81 | 25.2% |
| Convenience events | 107 | 33.2% |
| Safety events | 76 | 23.6% |
| Durability events | 58 | 18.0% |
| Total participant interruptions | 58 | 15.6% |
| Due to cART simplification | 30 | 51.7% |
| Due to toxicity | 17 | 29.3% |
| Due to virological failure | 4 | 6.9% |
| Due to loss to follow-up | 2 | 3.5% |
| Due to other reasons | 4 | 6.9% |
| Death | 1 | 1.7% |
| Total follow up time (days) | 556 | (316.5–722.5) |
| Hazards of Interruption (95% Confidence Interval; p-Value) Due to: | ||||
|---|---|---|---|---|
| Efficacy | Convenience | Safety | Durability | |
| Age (per 10 years old older) | 0.89 (0.72–1.10; 0.30) | 0.99 (0.82–1.19; 0.91) | 0.99 (0.80–1.24; 0.96) | 0.98 (0.76–1.26; 0.88) |
| Sex | ||||
| Female | Reference category | Reference category | Reference category | Reference category |
| Male | 0.95 (0.57–1.58; 0.85) | 0.78 (0.51–1.18; 0.25) | 0.81 (0.49–1.34; 0.41) | 0.92 (0.51–1.65; 0.77) |
| Nationality | ||||
| Non-Italian | Reference category | Reference category | Reference category | Reference category |
| Italian | 0.64 (0.38–1.08; 0.10) | 0.65 (0.41–1.04; 0.07) | 0.74 (0.42–1.30; 0.29) | 0.71 (0.37–1.34; 0.29) |
| Risk group | ||||
| Heterosexual | Reference category | Reference category | Reference category | Reference category |
| PWID | 1.05 (0.59–1.87; 0.87) | 1.14 (0.70–1.84; 0.61) | 1.35 (0.79–2.30; 0.28) | 0.93 (0.48–1.81; 0.82) |
| MSM | 1.35 (0.81–2.27; 0.25) | 1.18 (0.74–1.87; 0.49) | 0.87 (0.48–1.56; 0.63) | 1.14 (0.62–2.07; 0.68) |
| Other | 1.11 (0.34–2.85; 0.83) | 1.20 (0.54–2.67; 0.66) | 0.91 (0.32–2.57; 0.86) | 0.27 (0.04–1.98; 0.20) |
| Diagnosis year | 0.69 (0.41–1.16; 0.16) | 0.83 (0.53–1.29; 0.40) | 1.17 (0.71–1.92; 0.54) | 1.00 (0.56–1.82; 0.98) |
| cART backbone | ||||
| 3TC | Reference category | Reference category | Reference category | Reference category |
| ABC/XTC | 1.30 (0.65–2.59; 0.46) | 1.05 (0.60–1.83; 0.86) | 0.74 (0.37–1.51; 0.41) | 1.31 (0.57–3.05; 0.53) |
| DRV-boosted | 0.62 (0.14–2.77; 0.53) | 0.93 (0.35–2.48; 0.88) | 0.77 (0.22–2.70; 0.69) | 0.47 (0.06–3.77; 0.48) |
| RPV | 0.55 (0.16–1.95; 0.35) | 0.80 (0.34–1.90; 0.62) | 0.80 (0.29–2.21; 0.66) | 0.27 (0.03–2.19; 0.22) |
| XTC/TXF | 4.85 (2.53–9.28; <0.01) | 3.10 (1.82–5.30; <0.01) | 3.86 (2.08–7.14; <0.01) | 5.71 (2.62–12.43; <0.01) |
| cART status | ||||
| Experienced | Reference category | Reference category | Reference category | Reference category |
| Naïve | 2.26 (1.39–3.67; <0.01) | 1.97 (1.28–3.04; <0.01) | 2.08 (1.26–3.45; <0.01) | 2.49 (1.42–4.36; <0.01) |
| Previous cART | ||||
| Naïve | Reference category | Reference category | Reference category | Reference category |
| NRTI/INSTI | 0.49 (0.17–1.40; 0.18) | 1.72 (0.31–1.64; 0.43) | 0.85 (0.34–2.12; 0.73) | 0.49 (0.14–1.65; 0.25) |
| NRTI/NNRTI | 0.35 (0.18–0.67; <0.01) | 0.37 (0.21–0.67; <0.01) | 0.30 (0.14–0.62; <0.01) | 0.35 (0.16–0.74; <0.01) |
| NRTI/PI-boosted | 0.47 (0.26–0.83; <0.01) | 0.50 (0.30–0.84; <0.01) | 0.48 (0.26–0.88; 0.02) | 0.41 (0.21–0.80; <0.01) |
| Other | 0.52 (0.27–1.00; 0.05) | 0.65 (0.37–1.13; 0.13) | 0.63 (0.33–1.21; 0.16) | 0.44 (0.20–0.96; 0.04) |
| Positive HBsAg at baseline | ||||
| NO | Reference category | Reference category | Reference category | Reference category |
| YES | 1.83 (0.58–5.80; 0.31) | 2.70 (1.10–6.64; 0.03) | 2.65 (0.97–7.25; 0.06) | 1.50 (0.37–6.14; 0.57) |
| Positive HCV Ab at baseline | ||||
| NO | Reference category | Reference category | Reference category | Reference category |
| YES | 0.87 (0.53–1.45; 0.60) | 0.94 (0.61–1.45; 0.79) | 1.16 (0.71–1.89; 0.56) | 1.02 (0.57–1.82; 0.94) |
| Baseline HIV RNA (per log10 copies/mL) | 1.43 (1.26–1.62; <0.01) | 1.32 (1.18–1.48; <0.01) | 1.26 (1.10–1.45; <0.01) | 1.36 (1.17–1.58; <0.01) |
| Baseline CD4+ T-cell count (per 100/mm3) | 0.87 (0.81–0.93; <0.01) | 0.90 (0.85–0.96; <0.01) | 0.89 (0.82–0.95; <0.01) | 0.88 (0.81–0.96; <0.01) |
| Baseline CD8+ T-cell count (per 100/mm3) | 0.98 (0.93–1.03; 0.35) | 0.98 (0.93–1.02; 0.30) | 0.97 (0.92–1.03; 0.32) | 0.99 (0.94–1.06; 0.87) |
| Baseline CD4/CD8 ratio | 0.44 (0.26–0.7; <0.01) | 0.62 (0.41–0.94; 0.02) | 0.60 (0.37–0.97; 0.04) | 0.45 (0.25–0.82; <0.01) |
| eGFR (ml/min) | ||||
| 60–90 mL/min | Reference category | Reference category | Reference category | Reference category |
| <60 mL/min | 1.20 (0.54–2.68; 0.65) | 2.61 (1.45–4.70; <0.01) | 4.06 (2.05–8.04; <0.01) | 1.43 (0.60–3.42; 0.42) |
| FIB4 score | ||||
| 1.45–3.25 | Reference category | Reference category | Reference category | Reference category |
| >3.25 | 6.96 (3.06–15.82; <0.01) | 5.27 (2.58–10.78; <0.01) | 6.50 (2.87–14.72; <0.01) | 6.05 (2.40–15.24; <0.01) |
| Baseline Framingham score (per unit) | 0.94 (0.89–1.00; 0.07) | 0.96 (0.91–1.03; 0.24) | 0.93 (0.87–0.99; 0.03) | 0.92 (0.86–0.98; 0.02) |
| Baseline cancer diagnosis | ||||
| NO | Reference category | Reference category | Reference category | Reference category |
| YES | 1.55 (0.80–3.00; 0.20) | 1.35 (0.74–2.46; 0.33) | 1.64 (0.84–3.19; 0.15) | 2.29 (1.16–4.54; 0.02) |
| Hazards of Interruption (95% Confidence Interval; p-Value) Due to: | ||||
|---|---|---|---|---|
| Efficacy | Convenience | Safety | Durability | |
| cART backbone | ||||
| 3TC a | Reference category | Reference category | Reference category | Reference category |
| ABC/XTC | 1.37 (0.66–2.85; 0.40) | 1.19 (0.65–2.16; 0.57) | 0.95 (0.44–2.05; 0.90) | 1.47 (0.61–3.58; 0.39) |
| DRV-boosted | 0.62 (0.13–2.98; 0.55) | 0.78 (0.27–2.26; 0.64) | 0.64 (0.17–2.46; 0.52) | 0.45 (0.05–3.90; 0.46) |
| RPV | 0.41 (0.11–1.54; 0.19) | 0.71 (0.29–1.76; 0.46) | 0.80 (0.27–2.36; 0.68) | 0.19 (0.02–1.57; 0.12) |
| XTC/TXF | 4.25 (1.94–9.34; <0.01) | 2.55 (1.30–5.00; <0.01) | 3.61 (1.68–7.76; <0.01) | 6.10 (2.42–15.38; <0.01) |
| Previous cART | ||||
| Naïve b | Reference category | Reference category | Reference category | Reference category |
| NRTI/INSTI | 0.52 (0.17–1.54; 0.23) | 0.69 (0.29–1.64; 0.40) | 0.82 (0.32–2.13; 0.69) | 0.45 (0.13–1.59; 0.22) |
| NRTI/NNRTI | 0.36 (0.18–0.70; <0.01) | 0.37 (0.20–0.67; <0.01) | 0.29 (0.14–0.62; <0.01) | 0.34 (0.16–0.72; <0.01) |
| NRTI/PI-boosted | 0.48 (0.26–0.87; 0.01) | 0.50 (0.30–0.84; <0.01) | 0.48 (0.26–0.87; 0.02) | 0.40 (0.20–0.79; <0.01) |
| Other | 0.55 (0.28–1.08; 0.08) | 0.63 (0.35–1.14; 0.13) | 0.61 (0.31–1.21; 0.16) | 0.42 (0.19–0.94; 0.03) |
| Baseline HIV RNA (per log10 copies/mL) c | 1.35 (1.14–1.60; <0.01) | 1.28 (1.10–1.50; <0.01) | 1.15 (0.95–1.38; 0.15) | 1.31 (1.07–1.60; <0.01) |
| Baseline CD4+ T-cell count (per 100/mm3) d | 0.95 (0.88–1.03; 0.23) | 0.96 (0.90–1.03; 0.30) | 0.92 (0.84–1.00; 0.06) | 0.95 (0.87–1.05; 0.32) |
| Baseline CD8+ T-cell count (per 100/mm3) e | 0.99 (0.94–1.04; 0.67) | 0.99 (0.95–1.03; 0.60) | 1.00 (0.95–1.05; 0.85) | 1.01 (0.95–1.07; 0.76) |
| Efficacy | Convenience | Safety | Durability | |
|---|---|---|---|---|
| Tenofovir-containing regimens |  | | | |
| Naïve status | | | | |
| Prior cART not containing an INSTI |  | | | |
| HBsAg positive carriers |  | | | |
| Baseline HIV RNA | | | | |
| Baseline CD4+ T-cell count | | | | |
| Baseline CD4/CD8 ratio | | | | |
| eGFR < 60 mL/min | | | | |
| FIB4 score > 3.25 | | | | |
| Baseline Framingham score | | | | |
| Baseline cancer diagnosis | | | | |
Not a statistically significant association; protective factor; risk factor; cART, combination antiretroviral treatment; INSTI, integrase strand inhibitors; HBsAg, hepatitis B antigen; eGFR, estimated Glomerular Filtration Rate.Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fusco, P.; Nasta, P.; Quiros-Roldan, E.; Tondinelli, A.; Costa, C.; Fornabaio, C.; Mazzini, N.; Prosperi, M.; Torti, C.; Carosi, G. Efficacy, Convenience, Safety and Durability of DTG-Based Antiretroviral Therapies: Evidence from a Prospective Study by the Italian MaSTER Cohort. Viruses 2023, 15, 924. https://doi.org/10.3390/v15040924
Fusco P, Nasta P, Quiros-Roldan E, Tondinelli A, Costa C, Fornabaio C, Mazzini N, Prosperi M, Torti C, Carosi G. Efficacy, Convenience, Safety and Durability of DTG-Based Antiretroviral Therapies: Evidence from a Prospective Study by the Italian MaSTER Cohort. Viruses. 2023; 15(4):924. https://doi.org/10.3390/v15040924
Chicago/Turabian StyleFusco, Paolo, Paola Nasta, Eugenia Quiros-Roldan, Alice Tondinelli, Cecilia Costa, Chiara Fornabaio, Nicola Mazzini, Mattia Prosperi, Carlo Torti, and Giampiero Carosi. 2023. "Efficacy, Convenience, Safety and Durability of DTG-Based Antiretroviral Therapies: Evidence from a Prospective Study by the Italian MaSTER Cohort" Viruses 15, no. 4: 924. https://doi.org/10.3390/v15040924