
HIV and COVID-19 Co-Infection: Epidemiology, Clinical Characteristics, and Treatment

{kind=link}
Abstract
:1. Introduction
2. Epidemiology
3. Clinical Outcomes
4. Clinical Characteristics
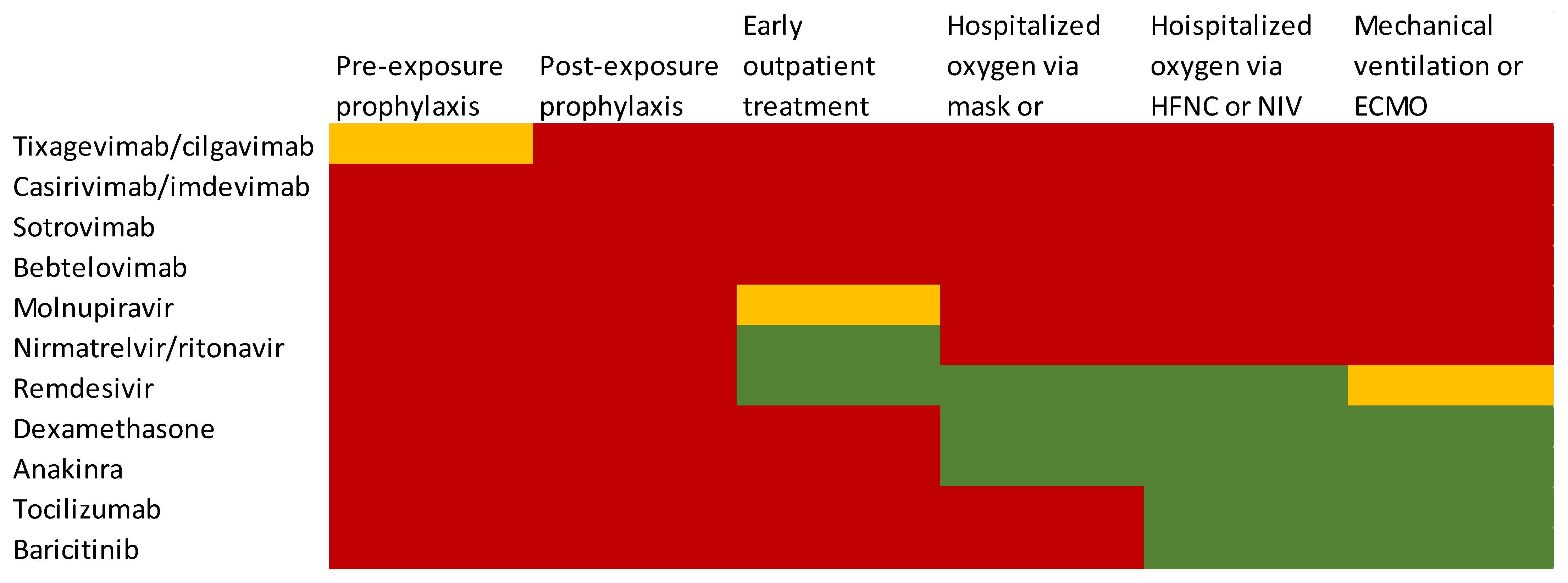
5. Management of COVID-19 in PWH
5.1. Pre-Exposure Prophylaxis
5.2. Post-Exposure Prophylaxis
5.3. Early Outpatient Treatment
5.3.1. Small Molecules
5.3.2. Monoclonal Antibodies
5.4. Hospital Treatment
5.4.1. Remdesivir
5.4.2. Dexamethasone
5.4.3. Immunosuppressants
6. Lessons Learned and Future Directions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pei, S.; Yamana, T.K.; Kandula, S.; Galanti, M.; Shaman, J. Burden and characteristics of COVID-19 in the United States during 2020. Nature 2021, 598, 338–341. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 3 February 2023).
- UNAIDS. Global HIV & AIDS STATISTICS—Fact SHEET. 2022. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 3 February 2023).
- The Global Fund. The impact of COVID-19 on HIV, TB and malaria services and systems for health: A snapshot from 502 health facilities across Africa and Asia. Available online: https://www.theglobalfund.org/me-dia/10776/COVID-19_2020-disruption-impact_report_en.pdf (accessed on 12 January 2023).
- Rosenthal, N.; Cao, Z.; Gundrum, J.; Sianis, J.; Safo, S. Risk Factors Associated with In-Hospital Mortality in a US National Sample of Patients With COVID-19. JAMA Netw. Open 2020, 3, e2029058. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Yang, Q.; Chi, J.; Dong, B.; Lv, W.; Shen, L.; Wang, Y. Comorbidities and the risk of severe or fatal outcomes associated with coronavirus disease 2019: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 99, 47–56. [Google Scholar] [CrossRef]
- Ssentongo, P.; Ssentongo, A.E.; Heilbrunn, E.S.; Ba, D.M.; Chinchilli, V.M. Association of cardiovascular disease and 10 other pre-existing comorbidities with COVID-19 mortality: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0238215. [Google Scholar] [CrossRef] [PubMed]
- Pennington, A.F.; Kompaniyets, L.; Summers, A.D.; Danielson, M.L.; Goodman, A.B.; Chevinsky, J.R.; Preston, L.E.; Schieber, L.Z.; Namulanda, G.; Courtney, J.; et al. Risk of Clinical Severity by Age and Race/Ethnicity Among Adults Hospitalized for COVID-19—United States, March–September 2020. Open Forum Infect. Dis. 2020, 8, ofaa638. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. People with Certain Medical Conditions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (accessed on 13 January 2023).
- Ambrosioni, J.; Blanco, J.L.; Reyes-Urueña, J.M.; Davies, M.-A.; Sued, O.; Marcos, M.A.; Martínez, E.; Bertagnolio, S.; Alcamí, J.; Miro, J.M.; et al. Overview of SARS-CoV-2 infection in adults living with HIV. Lancet HIV 2021, 8, e294–e305. [Google Scholar] [CrossRef]
- Kenmoe, S.; Bigna, J.J.; Modiyingi, A.F.; Ndangang, M.S.; Ngoupo, P.A.; Simo, F.B.N.; Tchatchouang, S.; Temfack, E.; Njouom, R. Case fatality rate and viral aetiologies of acute respiratory tract infections in HIV positive and negative people in Africa: The VARIAFRICA-HIV systematic review and meta-analysis. J. Clin. Virol. 2019, 117, 96–102. [Google Scholar] [CrossRef]
- Mellors, J.W.; Munoz, A.; Giorgi, J.V.; Margolick, J.B.; Tassoni, C.J.; Gupta, P.; Kingsley, L.A.; Todd, J.A.; Saah, A.J.; Detels, R.; et al. Plasma Viral Load and CD4+ Lymphocytes as Prognostic Markers of HIV-1 Infection. Ann. Intern. Med. 1997, 126, 946–954. [Google Scholar] [CrossRef]
- Fenwick, C.; Joo, V.; Jacquier, P.; Noto, A.; Banga, R.; Perreau, M.; Pantaleo, G. T-cell exhaustion in HIV infection. Immunol. Rev. 2019, 292, 149–163. [Google Scholar] [CrossRef] [Green Version]
- Schouten, J.; Wit, F.W.; Stolte, I.G.; Kootstra, N.A.; van der Valk, M.; Geerlings, S.E.; Prins, M.; Reiss, P. Cross-sectional Comparison of the Prevalence of Age-Associated Comorbidities and Their Risk Factors Between HIV-Infected and Uninfected Individuals: The AGEhIV Cohort Study. Clin. Infect. Dis. 2014, 59, 1787–1797. [Google Scholar] [CrossRef]
- Kupferschmidt, K. Where did ‘weird’ Omicron come from? Science 2021, 374, 1179. [Google Scholar] [CrossRef] [PubMed]
- Corey, L.; Beyrer, C.; Cohen, M.S.; Michael, N.L.; Bedford, T.; Rolland, M. SARS-CoV-2 Variants in Patients with Immunosuppression. N. Engl. J. Med. 2021, 385, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Oyelade, T.; Alqahtani, J.S.; Hjazi, A.M.; Li, A.; Kamila, A.; Raya, R.P. Global and Regional Prevalence and Outcomes of COVID-19 in People Living with HIV: A Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2022, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Danwang, C.; Noubiap, J.J.; Robert, A.; Yombi, J.C. Outcomes of patients with HIV and COVID-19 co-infection: A systematic review and meta-analysis. AIDS Res. Ther. 2022, 19, 3. [Google Scholar] [CrossRef]
- Luan, H.; Song, I.M.; Fiellin, D.A.; Ransome, Y.D. HIV Infection Prevalence Significantly Intersects With COVID-19 Infection at the Area Level: A US County-Level Analysis. Am. J. Ther. 2021, 88, 125–131. [Google Scholar] [CrossRef]
- Park, L.S.; McGinnis, K.A.; Gordon, K.S.; Justice, A.C.; Leyden, W.; Silverberg, M.J.; Skarbinski, J.; Jefferson, C.; Horberg, M.; Certa, J.; et al. SARS-CoV-2 Testing and Positivity Among Persons with and Without HIV in 6 US Cohorts. Am. J. Ther. 2022, 90, 249–255. [Google Scholar] [CrossRef]
- Rasmussen, L.D.; Cowan, S.; Gerstoft, J.; Kronborg, G.; Johansen, I.S.; Larsen, C.S.; Weise, L.; Dalager-Pedersen, M.; Leth, S.; Nielsen, L.N.; et al. Outcomes following severe acute respiratory syndrome coronavirus 2 infection among individuals with and without HIV in Denmark. Aids 2022, 37, 311–321. [Google Scholar] [CrossRef]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA 2020, 323, 1843–1844. [Google Scholar] [CrossRef] [Green Version]
- Aydillo, T.; Gonzalez-Reiche, A.S.; Aslam, S.; van de Guchte, A.; Khan, Z.; Obla, A.; Dutta, J.; van Bakel, H.; Aberg, J.; García-Sastre, A.; et al. Shedding of Viable SARS-CoV-2 after Immunosuppressive Therapy for Cancer. N. Engl. J. Med. 2020, 383, 2586–2588. [Google Scholar] [CrossRef]
- Miró, J.M.; Ambrosioni, J.; Blanco, J.L. COVID-19 in patients with HIV—Authors’ reply. Lancet HIV 2020, 7, e383–e384. [Google Scholar] [CrossRef]
- Shalev, N.; Scherer, M.; Lasota, E.D.; Antoniou, P.; Yin, M.T.; Zucker, J.; Sobieszczyk, M.E. Clinical Characteristics and Outcomes in People Living with Human Immunodeficiency Virus Hospitalized for Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 2294–2297. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; The Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Inciarte, A.; Gonzalez-Cordon, A.; Rojas, J.; Torres, B.; De Lazzari, E.; De La Mora, L.; Martinez-Rebollar, M.; Laguno, M.; Callau, P.; Gonzalez-Navarro, A.; et al. Clinical characteristics, risk factors, and incidence of symptomatic coronavirus disease 2019 in a large cohort of adults living with HIV: A single-center, prospective observational study. Aids 2020, 34, 1775–1780. [Google Scholar] [CrossRef] [PubMed]
- Vizcarra, P.; Pérez-Elías, M.J.; Quereda, C.; Moreno, A.; Vivancos, M.J.; Dronda, F.; Casado, J.L.; Moreno, S.; Fortún, J.; Navas, E.; et al. Description of COVID-19 in HIV-infected individuals: A single-centre, prospective cohort. Lancet HIV 2020, 7, e554–e564. [Google Scholar] [CrossRef] [PubMed]
- Karmen-Tuohy, S.; Carlucci, P.M.; Zervou, F.N.; Zacharioudakis, I.M.; Rebick, G.; Klein, E.; Reich, J.; Jones, S.; Rahimian, J. Outcomes Among HIV-Positive Patients Hospitalized With COVID-19. JAIDS J. Acquir. Immune Defic. Syndr. 2020, 85, 6–10. [Google Scholar] [CrossRef]
- Gervasoni, C.; Meraviglia, P.; Riva, A.; Giacomelli, A.; Oreni, L.; Minisci, D.; Atzori, C.; Ridolfo, A.; Cattaneo, D. Clinical Features and Outcomes of Patients with Human Immunodeficiency Virus With COVID-19. Clin. Infect. Dis. 2020, 71, 2276–2278. [Google Scholar] [CrossRef]
- Bhaskaran, K.; Rentsch, C.T.; MacKenna, B.; Schultze, A.; Mehrkar, A.; Bates, C.J.; Eggo, R.M.; E Morton, C.; Bacon, S.C.J.; Inglesby, P.; et al. HIV infection and COVID-19 death: A population-based cohort analysis of UK primary care data and linked national death registrations within the OpenSAFELY platform. Lancet HIV 2020, 8, e24–e32. [Google Scholar] [CrossRef]
- Miyashita, H.; Kuno, T. Prognosis of coronavirus disease 2019 (COVID-19) in patients with HIV infection in New York City. HIV Med. 2020, 22, e1–e2. [Google Scholar] [CrossRef]
- Tesoriero, J.M.; Swain, C.-A.E.; Pierce, J.L.; Zamboni, L.; Wu, M.; Holtgrave, D.R.; Gonzalez, C.J.; Udo, T.; Morne, J.E.; Hart-Malloy, R.; et al. COVID-19 Outcomes Among Persons Living with or Without Diagnosed HIV Infection in New York State. JAMA Netw. Open 2021, 4, e2037069. [Google Scholar] [CrossRef]
- Mellor, M.M.; Bast, A.C.; Jones, N.R.; Roberts, N.W.; Ordóñez-Mena, J.M.; Reith, A.J.; Butler, C.C.; Matthews, P.C.; Dorward, J. Risk of adverse coronavirus disease 2019 outcomes for people living with HIV. Aids 2021, 35, F1–F10. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Rosalind, J.; Christian, K.; Kurniawan, A. Human immunodeficiency virus and mortality from coronavirus disease 2019: A systematic review and meta-analysis. South. Afr. J. HIV Med. 2021, 22, 7. [Google Scholar] [CrossRef] [PubMed]
- Ssentongo, P.; Heilbrunn, E.S.; Ssentongo, A.E.; Advani, S.; Chinchilli, V.M.; Nunez, J.J.; Du, P. Epidemiology and outcomes of COVID-19 in HIV-infected individuals: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 6283. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Xie, Y.; Hu, S.; Ai, W.; Tao, Y.; Tang, H.; Jing, F.; Tang, W. Systematic Review and Meta-Analyses of The Interaction Between HIV Infection And COVID-19: Two Years’ Evidence Summary. Front. Immunol. 2022, 13, 864838. [Google Scholar] [CrossRef]
- Dzinamarira, T.; Murewanhema, G.; Chitungo, I.; Ngara, B.; Nkambule, S.J.; Madziva, R.; Herrera, H.; Mukwenha, S.; Cuadros, D.F.; Iradukunda, P.G.; et al. Risk of mortality in HIV-infected COVID-19 patients: A systematic review and meta-analysis. J. Infect. Public Health 2022, 15, 654–661. [Google Scholar] [CrossRef]
- Bertagnolio, S.; Thwin, S.S.; Silva, R.; Nagarajan, S.; Jassat, W.; Fowler, R.; Haniffa, R.; Reveiz, L.; Ford, N.; Doherty, M.; et al. Clinical features of, and risk factors for, severe or fatal COVID-19 among people living with HIV admitted to hospital: Analysis of data from the WHO Global Clinical Platform of COVID-19. Lancet HIV 2022, 9, e486–e495. [Google Scholar] [CrossRef] [PubMed]
- Boulle, A.; Davies, M.-A.; Hussey, H.; Ismail, M.; Morden, E.; Vundle, Z.; Zweigenthal, V.; Mahomed, H.; Paleker, M.; Pienaar, D. Risk factors for COVID-19 death in a population cohort study from the Western Cape Province, South Africa. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, e2005–e2015. [Google Scholar] [CrossRef]
- Yang, X.; Sun, J.; Patel, R.C.; Zhang, J.; Guo, S.; Zheng, Q.; Olex, A.L.; Olatosi, B.; Weissman, S.B.; Islam, J.Y.; et al. Associations between HIV infection and clinical spectrum of COVID-19: A population level analysis based on US National COVID Cohort Collaborative (N3C) data. Lancet HIV 2021, 8, e690–e700. [Google Scholar] [CrossRef]
- Nachega, J.B.; Kapata, N.; Sam-Agudu, N.A.; Decloedt, E.H.; Katoto, P.D.; Nagu, T.; Mwaba, P.; Yeboah-Manu, D.; Chanda-Kapata, P.; Ntoumi, F.; et al. Minimizing the impact of the triple burden of COVID-19, tuberculosis and HIV on health services in sub-Saharan Africa. Int. J. Infect. Dis. 2021, 113, S16–S21. [Google Scholar] [CrossRef]
- Heidary, M.; Asadi, A.; Noorbakhsh, N.; Dashtbin, S.; Asadollahi, P.; Dranbandi, A.; Navidifar, T.; Ghanavati, R. COVID-19 in HIV-positive patients: A systematic review of case reports and case series. J. Clin. Lab. Anal. 2022, 36, e24308. [Google Scholar] [CrossRef]
- Lang, R.; Humes, E.; Coburn, S.B.; Horberg, M.A.; Fathi, L.F.; Watson, E.; Jefferson, C.R.; Park, L.S.; Gordon, K.S.; Akgün, K.M.; et al. Analysis of Severe Illness After Postvaccination COVID-19 Breakthrough Among Adults with and Without HIV in the US. JAMA Netw. Open 2022, 5, e2236397. [Google Scholar] [CrossRef]
- Dandachi, D.; Geiger, G.; Montgomery, M.W.; Karmen-Tuohy, S.; Golzy, M.; Antar, A.A.; Llibre, J.M.; Camazine, M.; Santiago, D.-D.; Carlucci, P.M.; et al. Characteristics, Comorbidities, and Outcomes in a Multicenter Registry of Patients with Human Immunodeficiency Virus and Coronavirus Disease 2019. Clin. Infect. Dis. 2021, 73, e1964–e1972. [Google Scholar] [CrossRef] [PubMed]
- Kamis, K.F.M.; Barbera, L.; Abdo, M.; Rowan, S.E.; Hussain, C.; Gardner, E.M.; Johnson, S.C.; MaWhinney, S.S.; Davis, A.J.; Carlson, J.; et al. Risk Factors for Hospitalization in People with HIV and COVID-19. Am. J. Ther. 2021, 88, e22. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, A.E.; Ignacio, R.A.B.; Whitney, B.M.; Delaney, J.A.; Nance, R.M.; Bamford, L.; Wooten, D.; Keruly, J.C.; Burkholder, G.; Napravnik, S.; et al. Factors Associated with Severity of COVID-19 Disease in a Multicenter Cohort of People With HIV in the United States, March–December 2020. Am. J. Ther. 2022, 90, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Nomah, D.K.; Reyes-Urueña, J.; Díaz, Y.; Moreno, S.; Aceiton, J.; Bruguera, A.; Vivanco-Hidalgo, R.M.; Llibre, J.M.; Domingo, P.; Falcó, V.; et al. Sociodemographic, clinical, and immunological factors associated with SARS-CoV-2 diagnosis and severe COVID-19 outcomes in people living with HIV: A retrospective cohort study. Lancet HIV 2021, 8, e701–e710. [Google Scholar] [CrossRef] [PubMed]
- Cabello, A.; Zamarro, B.; Nistal, S.; Victor, V.; Hernández, J.; Prieto-Pérez, L.; Carrillo, I.; Álvarez, B.; Fernández-Roblas, R.; Hernández-Segurado, M.; et al. COVID-19 in people living with HIV: A multicenter case-series study. Int. J. Infect. Dis. 2021, 102, 310–315. [Google Scholar] [CrossRef] [PubMed]
- del Amo, J.; Polo, R.; Moreno, S.; Díaz, A.; Martínez, E.; Arribas, J.R.; Jarrín, I.; Hernán, M.A. Incidence and Severity of COVID-19 in HIV-Positive Persons Receiving Antiretroviral Therapy. Ann. Intern. Med. 2020, 173, 536–541. [Google Scholar] [CrossRef]
- Bertagnolio, S.; Silva, R.; Nagarajan, S.; Thwin, S.; Jassat, W.; Fowler, R.; Haniffa, R.; Reveiz, L.; Ford, N.; Doherty, M.; et al. Are people living with HIV at higher risk of severe and fatal COVID-19? In Proceedings of the 24th International AIDS Conference, Montreal, QC, Canada, 29 July–2 August 2022. [Google Scholar]
- Chun, H.M.; Milligan, K.; Agyemang, E.; Ford, N.; Rangaraj, A.; Desai, S.; Wilder-Smith, A.; Vitoria, M.; Zulu, I. A Systematic Review of COVID-19 Vaccine Antibody Responses in People With HIV. Open Forum Infect. Dis. 2022, 9, ofac579. [Google Scholar] [CrossRef]
- Bessen, C.; Plaza-Sirvent, C.; Simsek, A.; Bhat, J.; Marheinecke, C.; Urlaub, D.; Bonowitz, P.; Busse, S.; Schumann, S.; Blanco, E.V.; et al. Impact of SARS-CoV-2 vaccination on systemic immune responses in people living with HIV. Front. Immunol. 2022, 13, 1049070. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Meyerowitz, E.A.; Kim, A.Y.; Ard, K.L.; Basgoz, N.; Chu, J.T.; Hurtado, R.M.; Lee, C.K.; He, W.; Minukas, T.; Nelson, S.; et al. Disproportionate burden of coronavirus disease 2019 among racial minorities and those in congregate settings among a large cohort of people with HIV. Aids 2020, 34, 1781–1787. [Google Scholar] [CrossRef]
- Etienne, N.; Karmochkine, M.; Slama, L.; Pavie, J.; Batisse, D.; Usubillaga, R.; Letembet, V.-A.; Brazille, P.; Canouï, E.; Slama, D.; et al. HIV infection and COVID-19: Risk factors for severe disease. AIDS 2020, 34, 1771–1774. [Google Scholar] [CrossRef] [PubMed]
- Collins, L.F.; Moran, C.A.; Oliver, N.T.; Moanna, A.; Lahiri, C.D.; Colasanti, J.A.; Kelley, C.F.; Nguyen, M.L.; Marconi, V.C.; Armstrong, W.S.; et al. Clinical characteristics, comorbidities and outcomes among persons with HIV hospitalized with coronavirus disease 2019 in Atlanta, Georgia. Aids 2020, 34, 1789–1794. [Google Scholar] [CrossRef] [PubMed]
- Childs, K.; Post, F.A.; Norcross, C.; Ottaway, Z.; Hamlyn, E.; Quinn, K.; Juniper, T.; Taylor, C. Hospitalized Patients With COVID-19 and Human Immunodeficiency Virus: A Case Series. Clin. Infect. Dis. 2020, 71, 2021–2022. [Google Scholar] [CrossRef] [PubMed]
- Härter, G.; Spinner, C.D.; Roider, J.; Bickel, M.; Krznaric, I.; Grunwald, S.; Schabaz, F.; Gillor, D.; Postel, N.; Mueller, M.C.; et al. COVID-19 in people living with human immunodeficiency virus: A case series of 33 patients. Infection 2020, 48, 681–686. [Google Scholar] [CrossRef]
- Calza, L.; Bon, I.; Tadolini, M.; Borderi, M.; Colangeli, V.; Badia, L.; Verucchi, G.; Rossini, G.; Vocale, C.; Gaibani, P.; et al. COVID-19 in patients with HIV-1 infection: A single-centre experience in northern Italy. Infection 2021, 49, 333–337. [Google Scholar] [CrossRef]
- D’Souza, G.; Springer, G.; Gustafson, D.; Kassaye, S.; Alcaide, M.L.; Ramirez, C.; Sharma, A.; Palella, F.J.; Tien, P.C.; Detels, R.; et al. COVID-19 symptoms and SARS-CoV-2 infection among people living with HIV in the US: The MACS/WIHS combined cohort study. HIV Res. Clin. Trials 2020, 21, 130–139. [Google Scholar] [CrossRef]
- Huang, D.; Zunong, J.; Li, M.; Li, D.; Gong, J.; Vermund, S.H.; Hu, Y. COVID-19 Clinical Presentation Among HIV-Infected Persons in China: A Systematic Review. Curr. HIV/AIDS Rep. 2022, 19, 167–176. [Google Scholar] [CrossRef]
- Coleman, H.; Snell, L.B.; Simons, R.; Douthwaite, S.T.; Lee, M.J. Coronavirus disease 2019 and Pneumocystis jirovecii pneumonia: A diagnostic dilemma in HIV. Aids 2020, 34, 1258–1260. [Google Scholar] [CrossRef]
- Mang, S.; Kaddu-Mulindwa, D.; Metz, C.; Becker, A.; Seiler, F.; Smola, S.; Maßmann, A.; Becker, S.L.; Papan, C.; Bals, R.; et al. Pneumocystis jirovecii Pneumonia and Severe Acute Respiratory Syndrome Coronavirus 2 Coinfection in a Patient with Newly Diagnosed HIV-1 Infection. Clin. Infect. Dis. 2021, 72, 1487–1489. [Google Scholar] [CrossRef]
- Merchant, E.A.; Flint, K.; Barouch, D.H.; Blair, B.M. Co-infection with coronavirus disease 2019, previously undiagnosed human immunodeficiency virus, Pneumocystis jirovecii pneumonia and cytomegalovirus pneumonitis, with possible immune reconstitution inflammatory syndrome. Idcases 2021, 24, e01153. [Google Scholar] [CrossRef]
- Bertolini, M.; Mutti, M.F.; Barletta, J.A.; Falak, A.; Cuatz, D.; Sisto, A.; A Ragusa, M.; Claros, N.O.F.; Rolón, M.J. COVID-19 associated with AIDS-related disseminated histoplasmosis: A case report. Int. J. STD AIDS 2020, 31, 1222–1224. [Google Scholar] [CrossRef] [PubMed]
- Kingery, J.R.; Safford, M.M.; Martin, P.; Lau, J.D.; Rajan, M.; Wehmeyer, G.T.; Li, H.A.; Alshak, M.N.; Jabri, A.; Kofman, A.; et al. Health Status, Persistent Symptoms, and Effort Intolerance One Year After Acute COVID-19 Infection. J. Gen. Intern. Med. 2022, 37, 1218–1225. [Google Scholar] [CrossRef] [PubMed]
- Peluso, M.J.; Spinelli, M.A.; Deveau, T.-M.; Forman, C.A.; Munter, S.E.; Mathur, S.; Tang, A.F.; Lu, S.; Goldberg, S.A.; Arreguin, M.I.; et al. Postacute sequelae and adaptive immune responses in people with HIV recovering from SARS-CoV-2 infection. Aids 2022, 36, F7–F16. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, R.T.; Bedimo, R.; Hoy, J.F.; Landovitz, R.J.; Smith, D.M.; Eaton, E.F.; Lehmann, C.; Springer, S.A.; Sax, P.E.; Thompson, M.A.; et al. Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults: 2022 Recommendations of the International Antiviral Society–USA Panel. JAMA 2022, 329, 63–84. [Google Scholar] [CrossRef]
- National Institutes of Health, COVID-19 Treatment Guidelines. 2022. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 17 January 2022).
- Bhimraj, A.; Morgan, R.L.; Shumaker, A.H.; Lavergne, V.; Baden, L.; Cheng, V.C.-C.; Edwards, K.M.; Gandhi, R.; Muller, W.J.; O’Horo, J.C.; et al. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with (COVID-19). Clin. Infect. Dis. 2020, 27, ciaa478. [Google Scholar] [CrossRef]
- BHIVA. British HIV Association Update on COVID Treatments for People with HIV. Available online: https://www.bhiva.org/update-on-COVID-treatments-for-people-with-HIV (accessed on 28 December 2022).
- National Institutes of Health. Guidance for COVID-19 and People with HIV. Guidelines Working Groups of the NIH Office of AIDS Research Advisory Council and US Department of Health and Human Services (HHS). Available online: https://clinicalinfo.hiv.gov/en/guidelines/guidance-COVID-19-and-people-hiv/whats-new-COVID-19-and-hiv-guidance (accessed on 28 December 2022).
- EACS. EACS Guidelines v11.1. Available online: https://www.eacsociety.org/guidelines/eacs-guidelines/ (accessed on 28 December 2022).
- Kling, K.D.; Janulis, P.; Demonbreun, A.R.; Sancilio, A.; Berzins, B.; Krueger, K.; Achenbach, C.; Price, R.; Sullivan, M.; Caputo, M.; et al. No difference in anti-spike antibody and surrogate viral neutralization following SARS-CoV-2 booster vaccination in persons with HIV compared to controls (CO-HIV Study). Front. Immunol. 2023, 13, 1048776. [Google Scholar] [CrossRef]
- Costiniuk, C.T.; Singer, J.; Lee, T.; Langlois, M.-A.; Arnold, C.; Galipeau, Y.; Needham, J.; Kulic, I.; Jenabian, M.-A.; Burchell, A.N.; et al. COVID-19 vaccine immunogenicity in people with HIV. Aids 2023, 37, F1–F10. [Google Scholar] [CrossRef]
- Nault, L.; Marchitto, L.; Goyette, G.; Tremblay-Sher, D.; Fortin, C.; Martel-Laferrière, V.; Trottier, B.; Richard, J.; Durand, M.; Kaufmann, D.; et al. COVID-19 vaccine immunogenicity in people living with HIV-1. Vaccine 2022, 40, 3633–3637. [Google Scholar] [CrossRef]
- Vergori, A.; Lepri, A.C.; Cicalini, S.; Matusali, G.; Bordoni, V.; Lanini, S.; Meschi, S.; Iannazzo, R.; Mazzotta, V.; Colavita, F.; et al. Immunogenicity to COVID-19 mRNA vaccine third dose in people living with HIV. Nat. Commun. 2022, 13, 4922. [Google Scholar] [CrossRef]
- Yin, J.; Chen, Y.; Li, Y.; Wang, C.; Zhang, X. Immunogenicity and efficacy of COVID-19 vaccines in people living with HIV: A systematic review and meta-analysis. Int. J. Infect. Dis. 2022, 124, 212–223. [Google Scholar] [CrossRef]
- Levin, M.J.; Ustianowski, A.; De Wit, S.; Launay, O.; Avila, M.; Templeton, A.; Yuan, Y.; Seegobin, S.; Ellery, A.; Levinson, D.J.; et al. Intramuscular AZD7442 (Tixagevimab–Cilgavimab) for Prevention of COVID-19. N. Engl. J. Med. 2022, 386, 2188–2200. [Google Scholar] [CrossRef] [PubMed]
- Evusheld (r). Summary of Product Characteristics. 2022. Available online: https://www.ema.europa.eu/en/documents/product-information/evusheld-epar-product-information_en.pdf (accessed on 3 February 2023).
- Aggarwal, A.; Stella, A.; Walker, G.; Akerman, A.; Milogiannakis, V.; Brilot, F.; Amatayakul-Chantler, S.; Roth, N.; Coppola, G.; Schofield, P.; et al. SARS-CoV-2 Omicron: Evasion of potent humoral responses and resistance to clinical immunotherapeutics relative to viral variants of concern. EBioMedicine 2022, 84, 104270. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Dcosta, B.M.; Landau, N.R.; Tada, T. Resistance of SARS-CoV-2 Omicron BA.1 and BA.2 Variants to Vaccine-Elicited Sera and Therapeutic Monoclonal Antibodies. Viruses 2022, 14, 1334. [Google Scholar] [CrossRef] [PubMed]
- Tao, K.; Tzou, P.L.; Pond, S.L.K.; Ioannidis, J.P.A.; Shafer, R.W. Susceptibility of SARS-CoV-2 Omicron Variants to Therapeutic Monoclonal Antibodies: Systematic Review and Meta-analysis. Microbiol. Spectr. 2022, 10, e0092622. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. FDA releases important information about risk of COVID-19 due to certain variants not neutralized by Evusheld. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-releases-important-information-about-risk-COVID-19-due-certain-variants-not-neutralized-evusheld (accessed on 3 February 2023).
- Touret, F.; Baronti, C.; Pastorino, B.; Villarroel, P.M.S.; Ninove, L.; Nougairède, A.; de Lamballerie, X. In vitro activity of therapeutic antibodies against SARS-CoV-2 Omicron BA.1, BA.2 and BA.5. Sci. Rep. 2022, 12, 12609. [Google Scholar] [CrossRef] [PubMed]
- Planas, D.; Bruel, T.; Staropoli, I.; Guivel-Benhassine, F.; Porrot, F.; Maes, P.; Grzelak, L.; Prot, M.; Mougari, S.; Planchais, C.; et al. Resistance of Omicron subvariants BA.2.75.2, BA.4.6, and BQ.1.1 to neutralizing antibodies. Nat. Commun. 2022, 14, 824. [Google Scholar] [CrossRef]
- IDSA. IDSA Guideline on the Treatment and Management of COVID-19. Available online: https://www.idsociety.org/globalassets/idsa/practice-guidelines/COVID-19/treatment/idsa-COVID-19-gl-tx-and-mgmt_na-ppx-2023-01-20.pdf#toc-14 (accessed on 3 February 2023).
- O’Brien, M.P.; Forleo-Neto, E.; Musser, B.J.; Isa, F.; Chan, K.-C.; Sarkar, N.; Bar, K.J.; Barnabas, R.V.; Barouch, D.H.; Cohen, M.S.; et al. Subcutaneous REGEN-COV Antibody Combination to Prevent COVID-19. N. Engl. J. Med. 2021, 385, 1184–1195. [Google Scholar] [CrossRef]
- Wilhelm, A.; Widera, M.; Grikscheit, K.; Toptan, T.; Schenk, B.; Pallas, C.; Metzler, M.; Kohmer, N.; Hoehl, S.; Marschalek, R.; et al. Limited neutralisation of the SARS-CoV-2 Omicron subvariants BA.1 and BA.2 by convalescent and vaccine serum and monoclonal antibodies. Ebiomedicine 2022, 82, 104158. [Google Scholar] [CrossRef]
- Fiaschi, L.; Dragoni, F.; Schiaroli, E.; Bergna, A.; Rossetti, B.; Giammarino, F.; Biba, C.; Gidari, A.; Lai, A.; Nencioni, C.; et al. Efficacy of Licensed Monoclonal Antibodies and Antiviral Agents against the SARS-CoV-2 Omicron Sublineages BA.1 and BA.2. Viruses 2022, 14, 1374. [Google Scholar] [CrossRef]
- Kabinger, F.; Stiller, C.; Schmitzová, J.; Dienemann, C.; Kokic, G.; Hillen, H.S.; Höbartner, C.; Cramer, P. Mechanism of molnupiravir-induced SARS-CoV-2 mutagenesis. Nat. Struct. Mol. Biol. 2021, 28, 740–746. [Google Scholar] [CrossRef]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of COVID-19 in Nonhospitalized Patients. N. Engl. J. Med. 2022, 386, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Hill, C.S.; Sarkar, S.; Tse, L.V.; Woodburn, B.M.D.; Schinazi, R.F.; Sheahan, T.P.; Baric, R.S.; Heise, M.T.; Swanstrom, R. β-d-N4-hydroxycytidine Inhibits SARS-CoV-2 Through Lethal Mutagenesis But Is Also Mutagenic To Mammalian Cells. J. Infect. Dis. 2021, 224, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Owen, D.R.; Allerton, C.M.N.; Anderson, A.S.; Aschenbrenner, L.; Avery, M.; Berritt, S.; Boras, B.; Cardin, R.D.; Carlo, A.; Coffman, K.J.; et al. An oral SARS-CoV-2 M pro inhibitor clinical candidate for the treatment of COVID-19. Science 2021, 374, 1586–1593. [Google Scholar] [CrossRef] [PubMed]
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; Baniecki, M.; Hendrick, V.M.; Damle, B.; Simón-Campos, A.; et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with COVID-19. N. Engl. J. Med. 2022, 386, 1397–1408. [Google Scholar] [CrossRef] [PubMed]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Preliminary report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early Remdesivir to Prevent Progression to Severe COVID-19 in Outpatients. N. Engl. J. Med. 2022, 386, 305–315. [Google Scholar] [CrossRef]
- Suzuki, Y.; Shibata, Y.; Minemura, H.; Nikaido, T.; Tanino, Y.; Fukuhara, A.; Kanno, R.; Saito, H.; Suzuki, S.; Inokoshi, Y.; et al. Real-world clinical outcomes of treatment with molnupiravir for patients with mild-to-moderate coronavirus disease 2019 during the Omicron variant pandemic. Clin. Exp. Med. 2022, 5, 1–9. [Google Scholar] [CrossRef]
- Zheng, B.; A Green, A.C.; Tazare, J.; Curtis, H.J.; Fisher, L.; Nab, L.; Schultze, A.; Mahalingasivam, V.; Parker, E.P.K.; Hulme, W.J.; et al. Comparative effectiveness of sotrovimab and molnupiravir for prevention of severe COVID-19 outcomes in patients in the community: Observational cohort study with the OpenSAFELY platform. BMJ 2022, 379, e071932. [Google Scholar] [CrossRef]
- Khoo, S.H.; FitzGerald, R.; Saunders, G.; Middleton, C.; Ahmad, S.; Edwards, C.J.; Hadjiyiannakis, D.; Walker, L.; Lyon, R.; Shaw, V.; et al. Molnupiravir versus placebo in unvaccinated and vaccinated patients with early SARS-CoV-2 infection in the UK (AGILE CST-2): A randomised, placebo-controlled, double-blind, phase 2 trial. Lancet Infect. Dis. 2022, 23, 183–195. [Google Scholar] [CrossRef]
- Najjar-Debbiny, R.; Gronich, N.; Weber, G.; Khoury, J.; Amar, M.; Stein, N.; Goldstein, L.H.; Saliba, W. Effectiveness of Molnupiravir in High-Risk Patients: A Propensity Score Matched Analysis. Clin. Infect. Dis. 2022, 76, ciac781. [Google Scholar] [CrossRef]
- Najjar-Debbiny, R.; Gronich, N.; Weber, G.; Khoury, J.; Amar, M.; Stein, N.; Goldstein, L.H.; Saliba, W. Effectiveness of Paxlovid in Reducing Severe Coronavirus Disease 2019 and Mortality in High-Risk Patients. Clin. Infect. Dis. 2022, 2, ciac443. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.M.; Joyce, B.; Plumb, I.D.; Sahakian, S.; Feldstein, L.R.; Barkley, E.; Paccione, M.; Deckert, J.; Sandmann, D.; Gerhart, J.L.; et al. Paxlovid Associated with Decreased Hospitalization Rate Among Adults with COVID-19—United States, April–September 2022. MMWR. Morb. Mortal. Weekly Rep. 2022, 71, 1531–1537. [Google Scholar] [CrossRef] [PubMed]
- Yip, T.C.F.; Lui, G.C.Y.; Lai, M.S.M.; Wong, V.W.S.; Tse, Y.K.; Ma, B.H.M.; Hui, E.; Leung, M.K.W.; Chan, H.L.Y.; Hui, D.S.C.; et al. Impact of the Use of Oral Antiviral Agents on the Risk of Hospitalization in Community Coronavirus Disease 2019 Patients (COVID-19). Clin. Infect. Dis. 2022, 29, ciac687. [Google Scholar] [CrossRef]
- Wai, A.K.-C.; Chan, C.Y.; Cheung, A.W.-L.; Wang, K.; Chan, S.C.-L.; Lee, T.T.-L.; Luk, L.Y.-F.; Yip, E.T.-F.; Ho, J.W.-K.; Tsui, O.W.-K.; et al. Association of Molnupiravir and Nirmatrelvir-Ritonavir with preventable mortality, hospital admissions and related avoidable healthcare system cost among high-risk patients with mild to moderate COVID-19. Lancet Reg. Health-West. Pac. 2023, 30, 100602. [Google Scholar] [CrossRef]
- Tiseo, G.; Barbieri, C.; Galfo, V.; Occhineri, S.; Matucci, T.; Almerigogna, F.; Kalo, J.; Sponga, P.; Cesaretti, M.; Marchetti, G.; et al. Efficacy and Safety of Nirmatrelvir/Ritonavir, Molnupiravir, and Remdesivir in a Real-World Cohort of Outpatients with COVID-19 at High Risk of Progression: The PISA Outpatient Clinic Experience. Infect. Dis. Ther. 2022, 12, 257–271. [Google Scholar] [CrossRef]
- CNN. Fauci says his COVID rebounded after Paxlovid. Available online: https://edition.cnn.com/2022/06/30/health/COVID-paxlovid-fauci-rebound/index.html (accessed on 19 January 2023).
- Malden, D.E.; Hong, V.; Lewin, B.J.; Ackerson, B.K.; Lipsitch, M.; Lewnard, J.A.; Tartof, S.Y. Hospitalization and emergency department encounters for COVID-19 after paxlovid treatment—California, December 2021–May 2022. MMWR Morb. Mortal Wkly. Rep. 2022, 71, 830–833. [Google Scholar] [CrossRef]
- Epling, B.P.; Rocco, J.M.; Boswell, K.L.; Laidlaw, E.; Galindo, F.; Kellogg, A.; Das, S.; Roder, A.; Ghedin, E.; Kreitman, A.; et al. Clinical, Virologic, and Immunologic Evaluation of Symptomatic Coronavirus Disease 2019 Rebound Following Nirmatrelvir/Ritonavir Treatment. Clin. Infect. Dis. 2022, ciac663. [Google Scholar] [CrossRef]
- Ranganath, N.; O’Horo, J.C.; Challener, D.W.; Tulledge-Scheitel, S.M.; Pike, M.L.; O’Brien, R.M.; Razonable, R.R.; Shah, A. Rebound Phenomenon After Nirmatrelvir/Ritonavir Treatment of Coronavirus Disease 2019 (COVID-19) in High-Risk Persons. Clin. Infect. Dis. 2022, 76, e537–e539. [Google Scholar] [CrossRef]
- Wang, L.; Berger, N.A.; Davis, P.B.; Kaelber, D.C.; Volkow, N.D.; Xu, R. COVID-19 rebound after Paxlovid and Molnupiravir during January–June 2022. medRxiv 2022. MedRxiv:22:2022.06.21.22276724. [Google Scholar] [CrossRef]
- Lai, C.; Hsueh, P. Coronavirus disease 2019 rebounds following nirmatrelvir/ritonavir treatment. J. Med. Virol. 2022, 95, e28430. [Google Scholar] [CrossRef]
- Gupta, A.; Gonzalez-Rojas, Y.; Juarez, E.; Casal, M.C.; Moya, J.; Falci, D.R.; Sarkis, E.; Solis, J.; Zheng, H.; Scott, N.; et al. Early Treatment for COVID-19 with SARS-CoV-2 Neutralizing Antibody Sotrovimab. N. Engl. J. Med. 2021, 385, 1941–1950. [Google Scholar] [CrossRef] [PubMed]
- Gliga, S.; Luebke, N.; Killer, A.; Gruell, H.; Walker, A.; Dilthey, A.T.; Thielen, A.; Lohr, C.; Flaßhove, C.; Krieg, S.; et al. Rapid Selection of Sotrovimab Escape Variants in Severe Acute Respiratory Syndrome Coronavirus 2 Omicron-Infected Immunocompromised Patients. Clin. Infect. Dis. 2022, 76, 408–415. [Google Scholar] [CrossRef]
- Adachi, E.; Saito, M.; Koga, M.; Tsutsumi, T.; Yotsuyanagi, H. Favorable Outcome Following Sotrovimab Monoclonal Antibody in a Patient with Prolonged SARS-CoV-2 Omicron Infection with HIV/AIDS. Intern. Med. 2022, 61, 3459–3462. [Google Scholar] [CrossRef] [PubMed]
- Montejano, R.; Marcelo, C.; Falces-Romero, I.; del Valle, L.G.; De Soto, T.; Garcia-Rodríguez, J.; Arribas, J.R. Efficacy of sotrovimab for persistent coronavirus disease-2019 in a severely immunocompromised person living with HIV. Aids 2022, 36, 751–753. [Google Scholar] [CrossRef] [PubMed]
- Westendorf, K.; Žentelis, S.; Wang, L.; Foster, D.; Vaillancourt, P.; Wiggin, M.; Lovett, E.; van der Lee, R.; Hendle, J.; Pustilnik, A.; et al. LY-CoV1404 (bebtelovimab) potently neutralizes SARS-CoV-2 variants. Cell Rep. 2022, 39, 110812. [Google Scholar] [CrossRef]
- Dryden-Peterson, S.; Kim, A.; Joyce, M.-R.; A Johnson, J.; Kim, A.Y.; Baden, L.R.; E Woolley, A. Bebtelovimab for High-Risk Outpatients with Early COVID-19 in a Large US Health System. Open Forum Infect. Dis. 2022, 9, ofac565. [Google Scholar] [CrossRef]
- McCreary, E.K.; E Kip, K.; Collins, K.; E Minnier, T.; Snyder, G.M.; Steiner, A.; Meyers, R.; Borneman, T.; Adam, M.; Thurau, L.; et al. Evaluation of Bebtelovimab for Treatment of COVID-19 During the SARS-CoV-2 Omicron Variant Era. Open Forum Infect. Dis. 2022, 9, ofac517. [Google Scholar] [CrossRef]
- WHO Solidarity Trial Consortium. Repurposed Antiviral Drugs for COVID-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar] [CrossRef]
- WHO Solidarity Trial. Remdesivir and three other drugs for hospitalised patients with COVID-19: Final results of the WHO Solidarity randomised trial and updated meta-analyses. Lancet 2022, 399, 1941–1953. [Google Scholar] [CrossRef]
- WHO. Therapeutics and COVID-19: A Living Guidelines v12.2. Available online: https://app.magicapp.org/#/guideline/nBkO1E/rec/noRNGw (accessed on 19 January 2023).
- Garibaldi, B.T.; Wang, K.; Robinson, M.L.; Betz, J.; Alexander, G.C.; Andersen, K.M.; Joseph, C.S.; Mehta, H.B.; Korwek, K.; E Sands, K.; et al. Real-World Effectiveness of Remdesivir in Adults Hospitalized with Coronavirus Disease 2019 (COVID-19): A Retrospective, Multicenter Comparative Effectiveness Study. Clin. Infect. Dis. 2022, 75, e516–e524. [Google Scholar] [CrossRef]
- Garibaldi, B.T.; Wang, K.; Robinson, M.L.; Zeger, S.L.; Bandeen-Roche, K.; Wang, M.-C.; Alexander, G.C.; Gupta, A.; Bollinger, R.; Xu, Y. Comparison of Time to Clinical Improvement With vs. Without Remdesivir Treatment in Hospitalized Patients With COVID-19. JAMA Netw. Open 2021, 4, e213071. [Google Scholar] [CrossRef] [PubMed]
- Ohl, M.E.; Miller, D.R.; Lund, B.C.; Kobayashi, T.; Miell, K.R.; Beck, B.F.; Alexander, B.; Crothers, K.; Sarrazin, M.S.V. Association of Remdesivir Treatment with Survival and Length of Hospital Stay Among US Veterans Hospitalized With COVID-19. JAMA Netw. Open 2021, 4, e2114741. [Google Scholar] [CrossRef] [PubMed]
- Elsawah, H.K.; Elsokary, M.A.; Abdallah, M.S.; ElShafie, A.H. Efficacy and safety of remdesivir in hospitalized COVID-19 patients: Systematic review and meta-analysis including network meta-analysis. Rev. Med. Virol. 2021, 31, e2187. [Google Scholar] [CrossRef] [PubMed]
- Ackley, T.W.; McManus, D.; Topal, J.E.; Cicali, B.; Shah, S. A Valid Warning or Clinical Lore: An Evaluation of Safety Outcomes of Remdesivir in Patients with Impaired Renal Function from a Multicenter Matched Cohort. Antimicrob. Agents Chemother. 2021, 65, e02290-20. [Google Scholar] [CrossRef] [PubMed]
- Stancampiano, F.; Jhawar, N.; Alsafi, W.; Valery, J.; Harris, D.; Kempaiah, P.; Shah, S.; Heckman, M.; Siddiqui, H.; Libertin, C. Use of remdesivir for COVID-19 pneumonia in patients with advanced kidney disease: A retrospective multicenter study. Clin. Infect. Pract. 2022, 16, 100207. [Google Scholar] [CrossRef]
- Shytaj, I.L.; Fares, M.; Gallucci, L.; Lucic, B.; Tolba, M.M.; Zimmermann, L.; Adler, J.M.; Xing, N.; Bushe, J.; Gruber, A.D.; et al. The FDA-Approved Drug Cobicistat Synergizes with Remdesivir to Inhibit SARS-CoV-2 Replication In Vitro and Decreases Viral Titers and Disease Progression in Syrian Hamsters. Mbio 2022, 13, e0370521. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group; Sterne, J.A.C.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Annane, D.; Azevedo, L.C.P.; Berwanger, O.; et al. Association Between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19: A Meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar] [CrossRef]
- University of Liverpool. Liverpool COVID-19 Drug Interactions. Available online: https://www.covid19-druginteractions.org/checker (accessed on 19 January 2023).
- Gutierrez, M.D.M.; Mur, I.; Mateo, M.G.; Vidal, F.; Domingo, P. Pharmacological considerations for the treatment of COVID-19 in people living with HIV (PLWH). Expert Opin. Pharmacother. 2021, 22, 1127–1141. [Google Scholar] [CrossRef]
- Kyriazopoulou, E.; Panagopoulos, P.; Metallidis, S.; Dalekos, G.N.; Poulakou, G.; Gatselis, N.; Karakike, E.; Saridaki, M.; Loli, G.; Stefos, A.; et al. An open label trial of anakinra to prevent respiratory failure in COVID-19. eLife 2021, 10, e66125. [Google Scholar] [CrossRef]
- Audemard-Verger, A.; Le Gouge, A.; Pestre, V.; Courjon, J.; Langlois, V.; Vareil, M.-O.; Devaux, M.; Bienvenu, B.; Leroy, V.; Goulabchand, R.; et al. Efficacy and safety of anakinra in adults presenting deteriorating respiratory symptoms from COVID-19: A randomized controlled trial. PLoS ONE 2022, 17, e0269065. [Google Scholar] [CrossRef]
- Davidson, M.; Menon, S.; Chaimani, A.; Evrenoglou, T.; Ghosn, L.; Graña, C.; Henschke, N.; Cogo, E.; Villanueva, G.; Ferrand, G.; et al. Interleukin-1 blocking agents for treating COVID-19. Cochrane Database Syst. Rev. 2022, 1, CD015308. [Google Scholar] [CrossRef]
- Abani, O.; Abbas, A.; Abbas, F.; Abbas, M.; Abbasi, S.; Abbass, H.; Abbott, A.; Abdallah, N.; Abdelaziz, A.; Abdelfattah, M.; et al. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef] [PubMed]
- Godolphin, P.J.; Fisher, D.J.; Berry, L.R.; Derde, L.P.G.; Diaz, J.V.; Gordon, A.C.; Lorenzi, E.; Marshall, J.C.; Murthy, S.; Shankar-Hari, M.; et al. Association between tocilizumab, sarilumab and all-cause mortality at 28 days in hospitalised patients with COVID-19: A network meta-analysis. PLoS ONE 2022, 17, e0270668. [Google Scholar] [CrossRef] [PubMed]
- Piscoya, A.; del Riego, A.P.; Cerna-Viacava, R.; Rocco, J.; Roman, Y.M.; Escobedo, A.A.; Pasupuleti, V.; White, C.M.; Hernandez, A.V. Efficacy and harms of tocilizumab for the treatment of COVID-19 patients: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0269368. [Google Scholar] [CrossRef] [PubMed]
- Almeida, P.R.L.; Person, O.C.; Puga, M.E.D.S.; Giusti, M.F.; Pinto, A.C.P.N.; Rocha, A.P.; Atallah, N. Effectiveness and safety of tocilizumab for COVID-19: A systematic review and meta-analysis of randomized clinical trials. Sao Paulo Med. J. 2022, 12, S1516-31802022005023216. [Google Scholar] [CrossRef] [PubMed]
- Küçükşahin, O.; Erden, A.; Karakaş, Ö.; Güven, S.C.; Armağan, B.; Şahiner, E.S.; Inan, O.; Kurtipek, A.C.; Gemcioğlu, E.; Karaahmetoğlu, S.; et al. Comparison of anakinra and tocilizumab in management of severe COVID-19: A retrospective cohort study. Turk. J. Med. Sci. 2022, 52, 1486–1494. [Google Scholar] [CrossRef]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus Remdesivir for Hospitalized Adults with COVID-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef]
- Ely, E.W.; Ramanan, A.V.; E Kartman, C.; de Bono, S.; Liao, R.; Piruzeli, M.L.B.; Goldman, J.D.; Saraiva, J.F.K.; Chakladar, S.; Marconi, V.C.; et al. Efficacy and safety of baricitinib plus standard of care for the treatment of critically ill hospitalised adults with COVID-19 on invasive mechanical ventilation or extracorporeal membrane oxygenation: An exploratory, randomised, placebo-controlled trial. Lancet Respir. Med. 2022, 10, 327–336. [Google Scholar] [CrossRef]
- Manoharan, S.; Ying, L.Y. Does baricitinib reduce mortality and disease progression in SARS-CoV-2 virus infected patients? A systematic review and meta analysis. Respir. Med. 2022, 202, 106986. [Google Scholar] [CrossRef]
- Cherian, J.J.; Eerike, M.; Bagepally, B.S.; Das, S.; Panda, S. Efficacy and safety of baricitinib and tocilizumab in hospitalized patients with COVID-19: A comparison using systematic review and meta-analysis. Front. Pharmacol. 2022, 13, 1004308. [Google Scholar] [CrossRef] [PubMed]
- Waterfield, K.C.; Shah, G.H.; Etheredge, G.D.; Ikhile, O. Consequences of COVID-19 crisis for persons with HIV: The impact of social determinants of health. BMC Public Health 2021, 21, 299. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.K.; Brooks, D.J.; Ikejezie, J.; Gacic-Dobo, M.; Dumolard, L.; Nedelec, Y.; Steulet, C.; Kassamali, Z.; Acma, A.; Ajong, B.N.; et al. COVID-19 Mortality and Progress Toward Vaccinating Older Adults—World Health Organization, Worldwide, 2020–2022. MMWR. Morb. Mortal. Weekly Rep. 2023, 72, 113–118. [Google Scholar] [CrossRef]
- UNAIDS. Full Report—In Danger: UNAIDS Global AIDS Update 2022. Available online: https://www.unaids.org/en/resources/documents/2022/in-danger-global-aids-update (accessed on 3 February 2023).
- Logie, C.H. Lessons learned from HIV can inform our approach to COVID-19 stigma. J. Int. AIDS Soc. 2020, 23, e25504.6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, T.; Reber, S.; Reeves, R. Race Gaps in COVID-19 Deaths Are Even Bigger than They Appear. Available online: https://www.brookings.edu/blog/up-front/2020/06/16/race-gaps-in-COVID-19-deaths-are-even-bigger-than-they-appear (accessed on 3 February 2023).
- CDC. HIV Self-Testing Guidance. Available online: https://wwwcdcgov/nchhstp/dear_colleague/2020/dcl-042820-HIV-self-testing-guidance (accessed on 3 February 2023).
- WHO. Policy brief: WHO Recommends HIV Self-Testing—Evidence Update and Considerations for Success. Available online: www.who.int/publications/i/item/who-recommends-hiv-self-testing-evidence-update (accessed on 3 February 2023).
- Figueroa, C.; Johnson, C.; Ford, N.; Sands, A.; Dalal, S.; Meurant, R.; Prat, I.; Hatzold, K.; Urassa, W.; Baggaley, R. Reliability of HIV rapid diagnostic tests for self-testing compared with testing by health-care workers: A systematic review and meta-analysis. Lancet HIV 2018, 5, e277–e290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevenson, E.M.; Terry, S.; Copertino, D.; Leyre, L.; Danesh, A.; Weiler, J.; Ward, A.R.; Khadka, P.; McNeil, E.; Bernard, K.; et al. SARS-CoV-2 mRNA vaccination exposes latent HIV to Nef-specific CD8+ T-cells. Nat. Commun. 2022, 13, 4888. [Google Scholar] [CrossRef]
- Mu, Z.; Haynes, B.; Cain, D. HIV mRNA Vaccines—Progress and Future Paths. Vaccines 2021, 9, 134. [Google Scholar] [CrossRef]
- Leggat, D.J.; Cohen, K.W.; Willis, J.R.; Fulp, W.J.; Decamp, A.C.; Kalyuzhniy, O.; Cottrell, C.A.; Menis, S.; Finak, G.; Ballweber-Fleming, L.; et al. Vaccination induces HIV broadly neutralizing antibody precursors in humans. Science 2022, 378, eadd6502. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basoulis, D.; Mastrogianni, E.; Voutsinas, P.-M.; Psichogiou, M. HIV and COVID-19 Co-Infection: Epidemiology, Clinical Characteristics, and Treatment. Viruses 2023, 15, 577. https://doi.org/10.3390/v15020577
Basoulis D, Mastrogianni E, Voutsinas P-M, Psichogiou M. HIV and COVID-19 Co-Infection: Epidemiology, Clinical Characteristics, and Treatment. Viruses. 2023; 15(2):577. https://doi.org/10.3390/v15020577
Chicago/Turabian StyleBasoulis, Dimitris, Elpida Mastrogianni, Pantazis-Michail Voutsinas, and Mina Psichogiou. 2023. "HIV and COVID-19 Co-Infection: Epidemiology, Clinical Characteristics, and Treatment" Viruses 15, no. 2: 577. https://doi.org/10.3390/v15020577