
Neutralizing Antibodies against SARS-CoV-2: Importance of Comorbidities in Health Personnel against Reinfections
 , , , ,
, , , ,  , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Detection of Neutralizing Antibodies against SARS-CoV-2
2.3. Epidemiological Monitoring for the Identification of Reinfection
2.4. Statistical Analysis
2.5. Ethical Aspects
3. Results
3.1. Description of the Study Population
3.2. Detection of Neutralizing Anti-SARS-CoV-2 Antibodies
3.3. Variable Dispersion Beta Regression
3.4. Reinfection after Vaccination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AIC | Akaike’s information criterion |
| B | regression coefficient |
| BCa | bias-corrected and accelerated |
| CI | confidence interval |
| COVID-19 | coronavirus disease 2019 |
| DM | type 2 diabetes |
| ELISA | Enzyme-Linked Immuno Sorbent Assay |
| HJM | Hospital Juárez de México |
| IgG | Immunoglobulin G |
| LL | lower limit |
| LU | upper limit |
| OR | odds ratios |
| qPCR | Quantitative Real-Time PCR |
| RT-PCR | real-time reverse transcription-polymerase chain reaction |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus-2 |
| SD | standard deviation |
| SE | standard error |
| TNF-α | tumor necrosis factor alpha |
| WHO | World Health Organization |
References
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel. Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef]
- Harapan, H.; Itoh, N.; Yufika, A.; Winardi, W.; Keam, S.; Te, H.; Megawati, D.; Hayati, Z.; Wagner, A.L.; Mudatsir, M. Coronavirus disease 2019 (COVID-19): A literature review. J. Infect. Public Health 2020, 13, 667–673. [Google Scholar] [CrossRef]
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 29 September 2023).
- Le, T.T.; Andreadakis, Z.; Kumar, A.; Gómez-Román, R.; Tollefsen, S.; Saville, M.; Mayhew, S. The COVID-19 vaccine development landscape. Nat. Rev. Drug Discov. 2020, 19, 305–306. [Google Scholar] [CrossRef]
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing Covid-19 vaccines at pandemic speed. N. Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef]
- WHO. Draft Landscape of COVID-19 Candidate Vaccines; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Arons, M.M.; Hatfield, K.M.; Reddy, S.C.; James, A.; Jacobs, J.R.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P. Presymptomatic SARS-CoV-2 infections and transmission in a skilled nursing facility. N. Engl. J. Med. 2020, 382, 2081–2090. [Google Scholar] [CrossRef]
- CDC COVID-19 Response Team. Characteristics of health care personnel with COVID-19—United states, 12 February–9 April, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 477–481. [Google Scholar] [CrossRef]
- Hunter, E.; Price, D.A.; Murphy, E. First experience of COVID-19 screening of health-care workers in England. Lancet 2020, 395, e77–e78. [Google Scholar] [CrossRef]
- Imperial College COVID-19 Response Team. Report 16: Role of Testing in COVID-19 Control. 2020. Available online: https://www.imperial.ac.uk/media/imperial-college/medicine/mrc-gida/2020-04-23-COVID19-Report-16 (accessed on 29 September 2023).
- Hassan, M.; Jordan, F.; Tawfick, W. Mental stress in health care professionals during COVID-19 outbreak. Ir. J. Med. Sci. 2022, 191, 2681–2687. [Google Scholar] [CrossRef]
- Ziarko, M.; Jasielska, A.; Stanisławska-Kubiak, M.; Daroszewski, P.; Samborski, W.; Mojs, E. Mental Health Outcomes Associated with COVID-19 Pandemic in a Group of Health Care Professionals. J. Behav. Health Serv. Res. 2022, 49, 22–31. [Google Scholar] [CrossRef]
- Gómez-Ochoa, S.A.; Franco, O.H.; Rojas, L.Z.; Raguindin, P.F.; Roa-Díaz, Z.M.; Wyssmann, B.M.; Romero Guevara, S.L.; Echeverría, L.E.; Glisic, M.; Muka, T. COVID-19 in Health-Care Workers: A Living Systematic Review and Meta-Analysis of Prevalence, Risk Factors, Clinical Characteristics, and Outcomes. Am. J. Epidemiol. 2021, 190, 161–175. [Google Scholar] [CrossRef]
- Bandyopadhyay, S.; Baticulon, R.E.; Kadhum, M.; Alser, M.; Ojuka, D.K.; Badereddin, Y.; Kamath, A.; Parepalli, S.A.; Brown, G.; Iharchane, S.; et al. Infection and mortality of healthcare workers worldwide from COVID-19: A systematic review. BMJ Glob. Health 2020, 5, e003097. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, N.M.; Laydon, D.; Nedjati-Gilani, G.; Imai, N.; Ainslie, K.; Baguelin, M.; Bhatia, S.; Boonyasiri, A.; Cucunubá, Z.; Cuomo-Dannenburg, G.; et al. Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID-19 Mortality and Healthcare Demand; Imperial College London: London, UK, 2020. [Google Scholar]
- Davies, N.G.; Kucharski, A.J.; Eggo, R.M.; Gimma, A.; Edmunds, W.J.; Group CC-19. The effect of non-pharmaceutical interventions on COVID-19 cases, deaths and demand for hospital services in the UK: A modelling study. Lancet Public Health 2020, 5, e375–e385. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Marie Schmidt, S.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill. 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed]
- Chee, W.T.; Wan, N.C.; Xijian, Q.; Pei, L.; Mark, C.; Charles, T.; Zhiliang, H.; Chih-Wei, C.; Barnaby, E.Y.; Wan, R.S.; et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2-spike protein-protein interaction. Nat. Biotechnol. 2020, 9, 1073–1078. [Google Scholar]
- Organización Panamericana de la Salud/Organización Mundial de la Salud. Orientaciones Provisionales Para la Detección de casos de Reinfección Por el Virus SARS-CoV-2, 29 de Octubre de 2020; OPS/OMS: Washington, DC, USA, 2020. [Google Scholar]
- Delignette-Muller, M.L.; Dutang, C. Fitdistrplus: An R Package for Fitting Distributions. J. Stat. Softw. 2015, 64, 1–34. [Google Scholar] [CrossRef]
- Grün, B.; Kosmidis, I.; Zeileis, A. Extended Beta Regression in R: Shaken, Stirred, Mixed, and Partitioned. J. Stat. Softw. 2012, 48, 1–25. [Google Scholar] [CrossRef]
- Heinze, G.; Loner, M.P.; Jiricka, L. Logistf: Firth’s Bias-Reduced Logistic Regression. R package version 1.24.1. 2022. Available online: https://CRAN.R-project.org/package=logistf (accessed on 26 April 2022).
- Canty; Ripley, B. Boot: Bootstrap R (S-Plus) Functions. R package version 1.3-28.1. 2021.
- Davison, A.C.; Hinkley, D.V. Bootstrap Methods and Their Applications; Cambridge University Press: Cambridge, UK, 1997. [Google Scholar]
- Available online: http://www.conbioetica-mexico.salud.gob.mx/descargas/pdf/normatividad/Normatinacional/10._NAL._Reglamento_de_Investigacion.pdf (accessed on 26 April 2022).
- Pilz, S.; Theiler-Schwetz, V.; Trummer, C.; Krause, R.; Ioannidis, J.P.A. SARS-CoV-2 reinfections: Overview of efficacy and duration of natural and hybrid immunity. Environ. Res. Jun. 2022, 209, 112911. [Google Scholar] [CrossRef]
- Li, L.Q.; Huang, T.; Wang, Y.Q.; Zheng-Ping, W.; Liang, Y.; Tao-Bi, H.; Hui-Yun, Z.; Weiming, S.; Yuping, W. COVID-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. J. Med. Virol. 2020, 92, 577–583. [Google Scholar] [CrossRef]
- Hua, C. Sex difference and smoking predisposition in patients with COVID-19. Lancet Respir. Med. 2020, 8, e20. [Google Scholar]
- Wenham, C.; Smith, J.; Morgan, R. COVID-19: The gendered impacts of the outbreak. Lancet 2020, 395, 846–848. [Google Scholar] [CrossRef]
- Hewagama, A.; Patel, D.; Yarlagadda, S. Stronger inflammatory/cytotoxic T-cell response in women identified by microarray analysis. Genes Immun. 2009, 10, 509–516. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 Natural Immunity. 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Sci_Brief-Natural_immunity-2021.1 (accessed on 18 November 2021).
- Klein, S.L.; Roberts, C.W. Sex Hormones and Immunity to Infection; Springer: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Kai-Wang, T.; Fan-Ngai, H.; Ip, J.D.; Wing-Ho, C.; Wan-Mui, C.; Raymond, T.; Ho-Yan, F.; Shuofeng, Y.; Hoi-Wah, T.; Chin-Ki, N.A.; et al. Coronavirus disease 2019 (COVID-19) re-infection by a phylogenetically distinct severe acute respiratory syndrome coronavirus 2 strain confirmed by whole genome sequencing. Clin. Infect. Dis. 2021, 73, e2946–e2951. [Google Scholar]
- Nguyen, N.N.; Nguyen, Y.N.; Hoang, V.T.; Million, M.; Gautret, P. SARS-CoV-2 Reinfection and Severity of the Disease: A Systematic Review and Meta-Analysis. Viruses 2023, 15, 967. [Google Scholar] [CrossRef] [PubMed]
- Peltan, I.D.; Beesley, S.J.; Webb, B.J.; Lopansri, B.K.; Sinclair, W.; Jacobs, J.R.; Brown, S.M. Evaluation of potential COVID-19 recurrence in patients with late repeat positive SARS-CoV-2 testing. PLoS ONE 2021, 16, e0251214. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.J.; Foulkes, S.; Charlett, A.; Atti, A.; Monk, E.J.M.; Simmons, R.; Wellington, E.; Cole, M.J.; Saei, A.; Oguti, B.; et al. SARS-CoV-2 infection rates of anti-body-positive compared with antibody negative health-care workers in England: A large, multicentre, prospective cohort study (SIREN). Lancet 2021, 397, 1459–1469. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef]
- Ripperger, T.J.; Uhrlaub, J.L.; Watanabe, M.; Wong, R.; Castaneda, Y.; Pizzato, H.A.; Thompson, M.R.; Bradshaw, C.; Weinkauf, C.C.; Bime, C.; et al. Orthogonal SARS-CoV-2 Serological Assays Enable Surveillance of Low-Prevalence Communities and Reveal Durable Humoral Immunity. Immunity 2020, 53, 925–933.e4. [Google Scholar] [CrossRef]
- Jaillon, S.; Berthenet, K.; Garlanda, C. Sexual dimorphism in innate immunity. Clin. Rev. Allergy Immunol. 2017, 56, 308–321. [Google Scholar] [CrossRef]
- Schröder, J. Gender differences in human sepsis. Arch. Surg. 1998, 133, 1200–1205. [Google Scholar] [CrossRef]
- Getachew, B.; Tizabi, Y. Vitamin D and COVID-19: Role of ACE2, age, gender, and ethnicity. J. Med. Virol. 2021, 93, 5285–5294. [Google Scholar] [CrossRef]
- Bean, D.J.; Monroe, J.; Turcinovic, J.; Moreau, Y.; Connor, J.H.; Sagar, M. SARS-CoV-2 reinfection associates with unstable housing and occurs in the presence of antibodies. Clin. Infect. Dis. 2022, 75, e208–e215. [Google Scholar] [CrossRef] [PubMed]
- Moser, J.; Emous, M.; Heeringa, P.; Rodenhuis-Zybert, I.A. Mechanisms and pathophysiology of SARS-CoV-2 infection of the adipose tissue. Trends Endocrinol. Metab. 2023, 11, 735–748. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Xu, X.; Hu, J.; Chen, Q.; Xu, F.; Liang, H.; Liu, N.; Zhu, H.; Lan, J.; Zhou, L.; et al. Clinical course and risk factors for recurrence of positive SARS-CoV-2 RNA: A retrospective cohort study from Wuhan, China. Aging 2020, 12, 16675–16689. [Google Scholar] [CrossRef] [PubMed]
- Talbot, H.K.; Coleman, L.A.; Crimin, K.; Zhu, Y.; Rock, M.T.; Meece, J.; Shay, D.K.; Belongia, E.A.; Griffin, M.R. Association between obesity and vulnerability and serologic response to influenza vaccination in older adults. Vaccine 2012, 30, 3937–3943. [Google Scholar] [CrossRef] [PubMed]
- Frydrych, L.M.; Bian, G.; O’Lone, D.E.; Ward, P.A.; Delano, M.J. Obesity and type 2 diabetes mellitus drive immune dysfunction, infection development, and sepsis mortality. J. Leukoc. Biol. 2018, 104, 525–534. [Google Scholar] [CrossRef]


{kind=link}
| Clinical Characteristics | History of Infection before Vaccination | p-Value | |
|---|---|---|---|
| Present n = 115 | Absent n = 147 | ||
| Age (Years) * | 43.8 (10.6) | 44.5 (10.4) | 0.570 § |
| Age (≥40 years) ** | 75 (65.2%) | 103 (70.1%) | 0.404 ‡ |
| Sex (Male) ** | 31 (27.0%) | 38 (25.9%) | 0.840 ‡ |
| Diabetes ** | 9 (7.8%) | 10 (6.8%) | 0.751 ‡ |
| Obesity ** | 6 (5.2%) | 5 (2.4%) | 0.677 † |
| Hypertension ** | 16 (13.9%) | 23 (15.6%) | 0.696 ‡ |
| Alcoholism ** | 9 (7.8%) | 19 (12.9%) | 0.185 ‡ |
| Smoking ** | 8 (7.0%) | 15 (10.2%) | 0.357 ‡ |
| Asthma ** | 6 (5.2%) | 4 (2.7%) | 0.477 † |
| Thyroid diseases ** | 5 (4.3%) | 5 (3.4%) | 0.943 † |
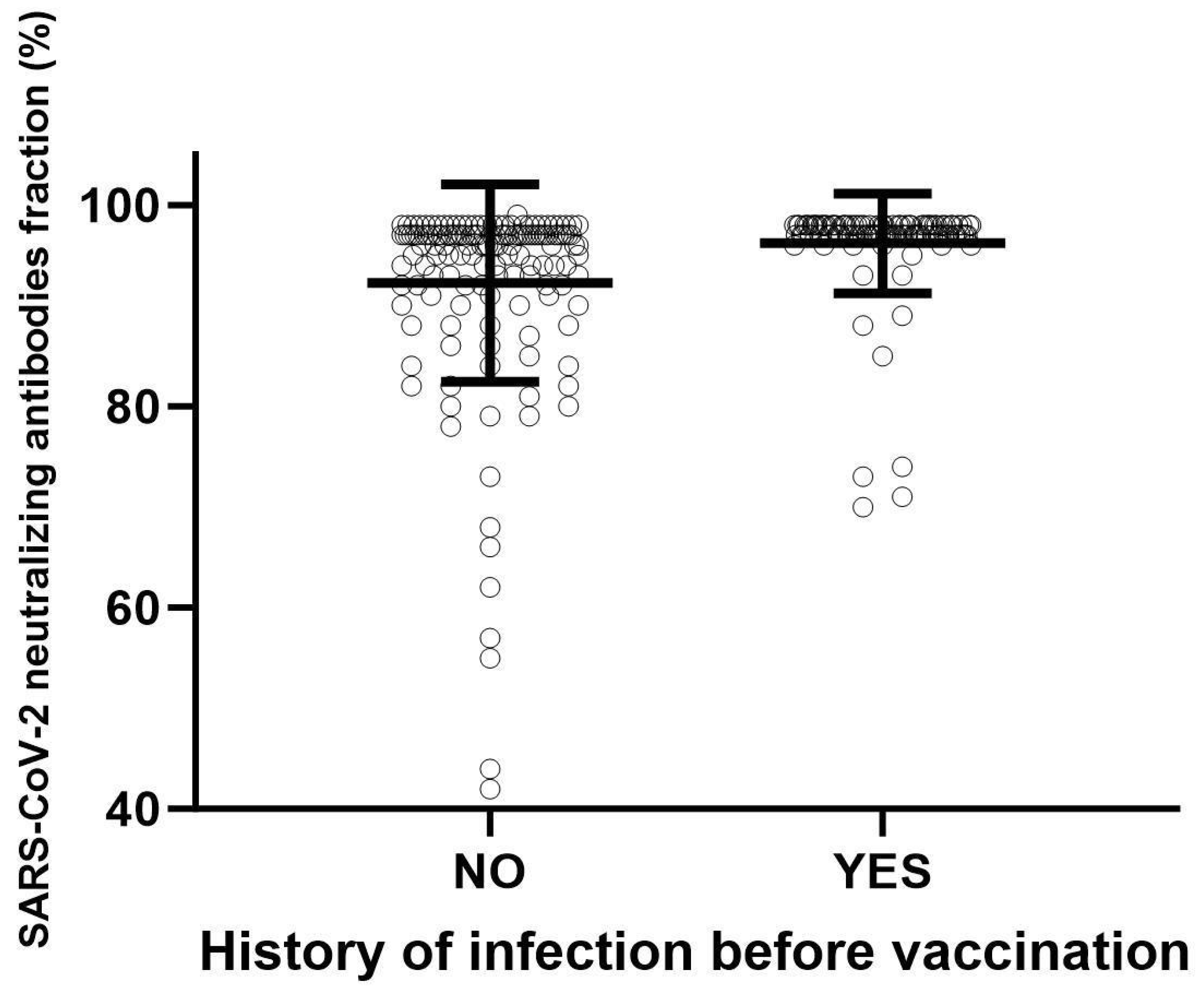
| History of Infection before Vaccination | |||||
|---|---|---|---|---|---|
| Proportion of SARS-CoV-2 neutralizing antibodies fraction | Present n = 115 | Absent n = 147 | p-Value | ||
| Mean (SD) | Min, Median, Max | Mean (SD) | Min, Median, Max | ||
| 0.961 (0.049) | 0.700, 0.970, 0.980 | 0.922 (0.097) | 0.420, 0.960, 0.990 | <0.001 * | |
| Clinical Characteristics | Saturated Model * | Minimal Model ** | ||||||
|---|---|---|---|---|---|---|---|---|
| B | 95% IC | p-Value | B | 95% IC | p-Value | |||
| LL | LU | LL | LU | |||||
| Intercept | 5.135 | 3.099 | 7.170 | <0.001 | 4.18 | 3.53 | 4.83 | <0.001 |
| Age (Years) | −0.026 | −0.068 | 0.016 | 0.224 | ||||
| Sex (Male) | 0.562 | −0.468 | 1.59 | 0.285 | ||||
| Diabetes | −1.65 | −2.97 | −0.319 | 0.015 | −1.73 | −3.04 | −0.417 | 0.009 |
| Obesity | 1.06 | −1.12 | 3.24 | 0.342 | ||||
| Hypertension | 0.395 | −0.878 | 1.67 | 0.543 | ||||
| Alcoholism | −1.29 | −2.46 | −0.124 | 0.030 | −1.06 | −2.08 | −0.048 | 0.040 |
| Smoking | −0.022 | −1.26 | 1.21 | 0.971 | ||||
| COVID-19 infection history | 4.28 | 3.07 | 5.50 | <0.001 | 4.37 | 3.16 | 5.58 | <0.001 |
| Phi coefficients (Dispersion) | ||||||||
| Phi (Intercept) | 2.66 | 2.41 | 2.91 | <0.001 | 2.65 | 2.41 | 2.90 | <0.001 |
| Phi (Diabetes) | −0.800 | −1.46 | −0.137 | 0.018 | −0.893 | −1.56 | −0.228 | 0.008 |
| Phi (Obesity) | 1.04 | 0.164 | 1.93 | 0.020 | 0.846 | 0.029 | 1.66 | 0.042 |
| Phi (COVID-19 infection history) | 1.27 | 0.906 | 1.63 | <0.001 | 1.29 | 0.932 | 1.65 | <0.001 |
| History of Infection before Vaccination | |||||
|---|---|---|---|---|---|
| Present | Absent | ||||
| Diabetes | Present | Alcoholism | Present | 94.5% | 80.1% |
| Absent | 95.4% | 87.7% | |||
| Absent | Alcoholism | Present | 95.8% | 90.1% | |
| Absent | 96.3% | 92.5% | |||
| Clinical Characteristics | Reinfection with Omicron after Vaccination | Bootstrap p-Value | |
|---|---|---|---|
| Present n = 8 | Absent n = 254 | ||
| Age (Years) * | 43.1 (9.28) | 44.2 (10.5) | 0.747 § |
| Age (40 years and more) | 6 (75.0%) | 172 (67.7%) | 0.667 † |
| Sex (Male) ** | 0 (0.0%) | 69 (27.2%) | 0.232 † |
| Diabetes ** | 0 (0.0%) | 19 (7.5%) | 0.885 † |
| Obesity ** | 1 (12.5%) | 10 (3.9%) | 0.879 † |
| Hypertension ** | 0 (0.0%) | 39 (15.4%) | 0.558 † |
| Alcoholism ** | 0 (0.0%) | 28 (11.0%) | 0.832 † |
| Smoking ** | 1 (12.5%) | 22 (8.7%) | 0.962 † |
| Clinical Characteristics | OR | 95% BCa Bootstrap IC | |
|---|---|---|---|
| LL | LU | ||
| Age (Years) | 1.000 | 0.907 | 1.09 |
| Sex (Male) | 0.172 | 0.047 | 0.433 |
| Diabetes | 0.952 | 0.010 | 3.67 |
| Obesity | 6.41 | 1.15 | 105.0 |
| Hypertension | 0.399 | 0.122 | 1.34 |
| Alcoholism | 0.634 | 0.167 | 2.024 |
| Smoking | 3.25 | 0.571 | 33.8 |
| Percentage of SARS-CoV-2 antibodies | 1.03 | 0.970 | 1.75 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vargas-De-León, C.; Cureño-Díaz, M.A.; Salazar, M.I.; Cruz-Cruz, C.; Loyola-Cruz, M.Á.; Durán-Manuel, E.M.; Zamora-Pacheco, E.R.; Bravata-Alcántara, J.C.; Lugo-Zamudio, G.E.; Fernández-Sánchez, V.; et al. Neutralizing Antibodies against SARS-CoV-2: Importance of Comorbidities in Health Personnel against Reinfections. Viruses 2023, 15, 2354. https://doi.org/10.3390/v15122354
Vargas-De-León C, Cureño-Díaz MA, Salazar MI, Cruz-Cruz C, Loyola-Cruz MÁ, Durán-Manuel EM, Zamora-Pacheco ER, Bravata-Alcántara JC, Lugo-Zamudio GE, Fernández-Sánchez V, et al. Neutralizing Antibodies against SARS-CoV-2: Importance of Comorbidities in Health Personnel against Reinfections. Viruses. 2023; 15(12):2354. https://doi.org/10.3390/v15122354
Chicago/Turabian StyleVargas-De-León, Cruz, Mónica Alethia Cureño-Díaz, Ma. Isabel Salazar, Clemente Cruz-Cruz, Miguel Ángel Loyola-Cruz, Emilio Mariano Durán-Manuel, Edwin Rodrigo Zamora-Pacheco, Juan Carlos Bravata-Alcántara, Gustavo Esteban Lugo-Zamudio, Verónica Fernández-Sánchez, and et al. 2023. "Neutralizing Antibodies against SARS-CoV-2: Importance of Comorbidities in Health Personnel against Reinfections" Viruses 15, no. 12: 2354. https://doi.org/10.3390/v15122354