
The Effect of HIV and Antiretroviral Therapy on Drug-Resistant Tuberculosis Treatment Outcomes in Eastern Cape, South Africa: A Cohort Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Demographics
2.2. Setting
2.3. Data Sources and Study Measures
2.4. Statistical Analysis
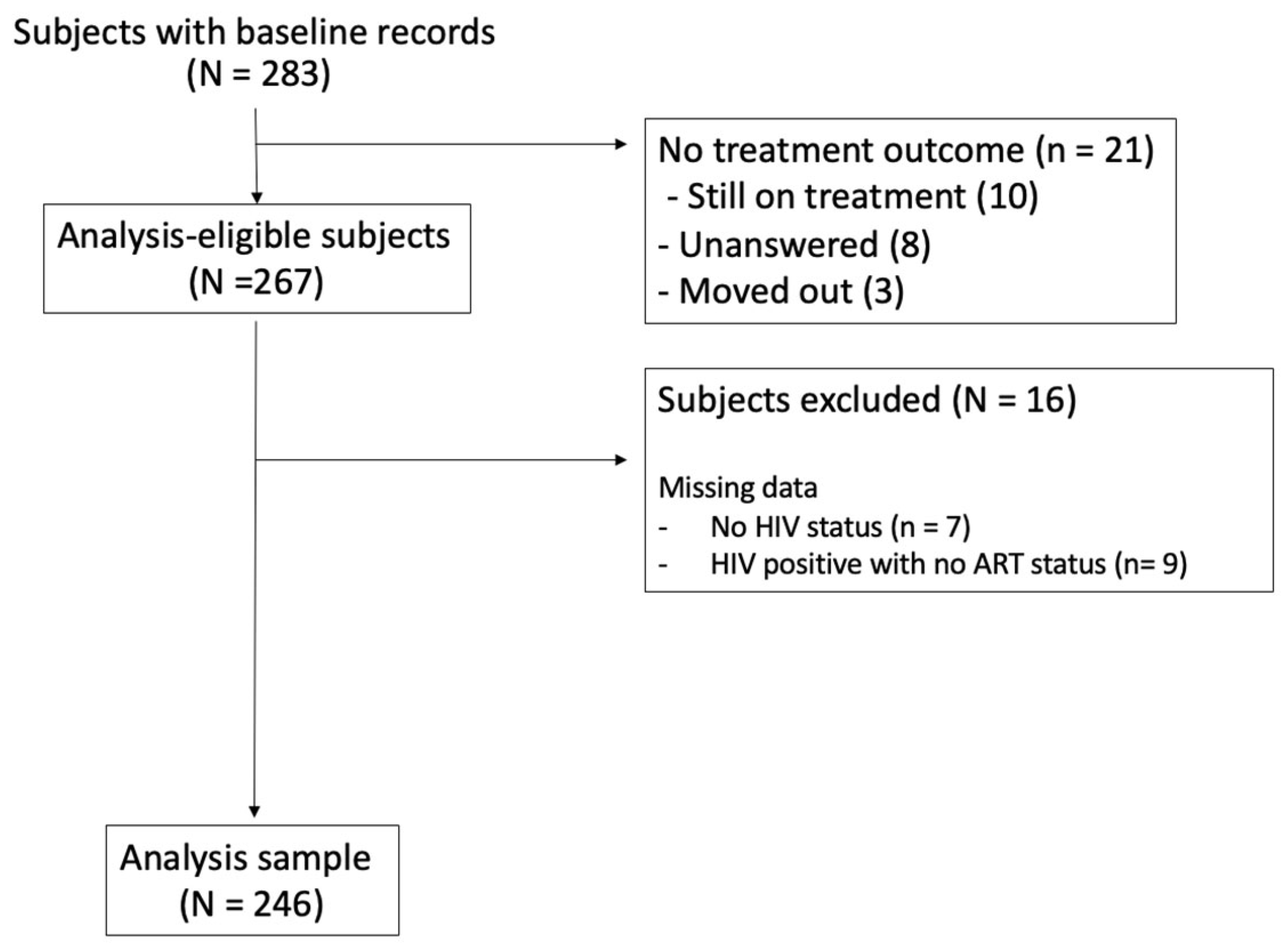
3. Results
3.1. Demographics
3.2. Treatment Outcomes
3.3. Regression Analysis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2021; World Health Organization: Geneva, Switzerland, 2021. Available online: https://apps.who.int/iris/handle/10665/346387 (accessed on 27 May 2022).
- Tackling the Drug-Resistant TB Crisis. Available online: https://www.who.int/activities/tackling-the-drug-resistant-tb-crisis (accessed on 23 April 2023).
- Ismail, N.; Ismail, F.; Omar, S.V.; Blows, L.; Gardee, Y.; Koornhof, H.; Onyebujoh, P.C. Drug resistant tuberculosis in Africa: Current status, gaps and opportunities. Afr. J. Lab. Med. 2018, 7, 781. [Google Scholar] [CrossRef] [PubMed]
- Shamu, S.; Kuwanda, L.; Farirai, T.; Guloba, G.; Slabbert, J.; Nkhwashu, N. Study on knowledge about associated factors of Tuberculosis (TB) and TB/HIV co-infection among young adults in two districts of South Africa. PLoS ONE 2019, 14, e0217836. [Google Scholar] [CrossRef] [PubMed]
- Abay, S.M.; Deribe, K.; Reda, A.A.; Biadgilign, S.; Datiko, D.; Assefa, T.; Todd, M.; Deribew, A. The Effect of Early Initiation of Antiretroviral Therapy in TB/HIV Coinfected Patients: A Systematic Review and Meta-Analysis. J. Int. Assoc. Provid. AIDS Care (JIAPAC) 2015, 14, 560–570. [Google Scholar] [CrossRef]
- van de Water, B.J.; Prvu Bettger, J.; Silva, S.; Humphreys, J.; Cunningham, C.K.; Farley, J.E. Time to Drug-Resistant Tuberculosis Treatment in a Prospective South African Cohort. Glob. Pediatr. Health 2017, 4, 2333794X17744140. [Google Scholar] [CrossRef] [PubMed]
- South African National Department of Health TB Programme. The First National TB Prevalence Survey. 2018. Available online: https://www.nicd.ac.za/wp-content/uploads/2021/02/TB-Prevalence-survey-report_A4_SA_TPS-Short_Feb-2021.pdf (accessed on 2 October 2023).
- Sarah Baartman District Municipality-Demographic. Available online: https://municipalities.co.za/demographic/103/sarah-baartman-district-municipality (accessed on 6 July 2023).
- Nelson Mandela Bay Metropolitan Municipality-Demographic. Available online: https://municipalities.co.za/demographic/1/nelson-mandela-bay-metropolitan-municipality (accessed on 6 July 2023).
- Statistics South Africa. Census 2011: Fact Sheet; Statistics South Africa: Pretoria, South Africa, 2012; p. 12.
- Eastern Cape Labour Market. Available online: https://www.ecsecc.org/datarepository/documents/ecsecc-q3-labourfeb-22-3_MNovg.pdf (accessed on 15 September 2023).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inf. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Definitions and Reporting Framework for Tuberculosis-2013 Revision; World Health Organization: Geneva, Switzerland, 2020; p. 47.
- Hicks, R.M.; Padayatchi, N.; Shah, N.S.; Wolf, A.; Werner, L.; Sunkari, V.B.; O’Donnell, M.R. Malnutrition associated with unfavorable outcome and death among South African MDR-TB and HIV co-infected children. Int. J. Tuberc. Lung Dis. Off. J. Int. Union. Tuberc. Lung Dis. 2014, 18, 1074–1083. [Google Scholar] [CrossRef]
- Lohiya, S.; Tripathy, J.P.; Sagili, K.; Khanna, V.; Kumar, R.; Ojha, A.; Bhatnagar, A.; Khanna, A. Does Drug-Resistant Extrapulmonary Tuberculosis Hinder TB Elimination Plans? A Case from Delhi, India. Trop. Med. Infect. Dis. 2020, 5, 109. [Google Scholar] [CrossRef]
- Pai, M.; Behr, M.A.; Dowdy, D.; Dheda, K.; Divangahi, M.; Boehme, C.C.; Ginsberg, A.; Swaminathan, S.; Spigelman, M.; Getahun, H.; et al. Tuberculosis. Nat. Rev. Primer. 2016, 2, 16076. [Google Scholar] [CrossRef]
- Verdecchia, M.; Keus, K.; Blankley, S.; Vambe, D.; Ssonko, C.; Piening, T.; Casas, E.C. Model of care and risk factors for poor outcomes in patients on multi-drug resistant tuberculosis treatment at two facilities in eSwatini (formerly Swaziland), 2011–2013. PLoS ONE 2018, 13, e0205601. [Google Scholar] [CrossRef]
- Nicholson, T.J.; Hoddinott, G.; Seddon, J.A.; Claassens, M.M.; van der Zalm, M.M.; Lopez, E.; Bock, P.; Caldwell, J.; Da Costa, D.; de Vaal, C.; et al. A systematic review of risk factors for mortality among tuberculosis patients in South Africa. Syst. Rev. 2023, 12, 23. [Google Scholar] [CrossRef]
- Masuku, S.D.; Berhanu, R.; Van Rensburg, C.; Ndjeka, N.; Rosen, S.; Long, L.; Evans, D.; Nichols, B.E. Managing multidrug-resistant tuberculosis in South Africa: A budget impact analysis. Int. J. Tuberc. Lung Dis. 2020, 24, 376–382. [Google Scholar] [CrossRef] [PubMed]
- van de Water, B.J.; Fulcher, I.; Cilliers, S.; Meyer, N.; Wilson, M.; Young, C.; Gaunt, B.; le Roux, K. Association of HIV infection and antiretroviral therapy with the occurrence of an unfavorable TB treatment outcome in a rural district hospital in Eastern Cape, South Africa: A retrospective cohort study. PLoS ONE 2022, 17, e0266082. [Google Scholar] [CrossRef] [PubMed]
- Chem, E.D.; Van Hout, M.C.; Hope, V. Treatment outcomes and antiretroviral uptake in multidrug-resistant tuberculosis and HIV co-infected patients in Sub Saharan Africa: A systematic review and meta-analysis. BMC Infect. Dis. 2019, 19, 723. [Google Scholar] [CrossRef] [PubMed]
- Nglazi, M.D.; Bekker, L.G.; Wood, R.; Kaplan, R. The impact of HIV status and antiretroviral treatment on TB treatment outcomes of new tuberculosis patients attending co-located TB and ART services in South Africa: A retrospective cohort study. BMC Infect. Dis. 2015, 15, 536. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S.; Chughtai, A.A.; Banu, S.; Seale, H. Context matters: Examining the factors impacting the implementation of tuberculosis infection prevention and control guidelines in health settings in seven high tuberculosis burden countries. J. Infect. Public Health 2021, 14, 588–597. [Google Scholar] [CrossRef]
- Murdoch, J.; Curran, R.; van Rensburg, A.J.; Awotiwon, A.; Dube, A.; Bachmann, M.; Petersen, I.; Fairall, L. Identifying contextual determinants of problems in tuberculosis care provision in South Africa: A theory-generating case study. Infect. Poverty. 2021, 10, 67. [Google Scholar] [CrossRef]
- Loveday, M.; Wallengren, K.; Reddy, T.; Besada, D.; Brust, J.C.M.; Voce, A.; Desai, H.; Ngozo, J.; Radebe, Z.; Master, I.; et al. MDR-TB patients in KwaZulu-Natal, South Africa: Cost-effectiveness of 5 models of care. PLoS ONE 2018, 13, e0196003. [Google Scholar] [CrossRef]
- Loveday, M.; Wallengren, K.; Voce, A.; Margot, B.; Reddy, T.; Master, I.; Brust, J.; Chaiyachati, K.; Padayatchi, N. Comparing early treatment outcomes of MDR-TB in decentralised and centralised settings in KwaZulu-Natal, South Africa. Int. J. Tuberc. Lung Dis. Off. J. Int. Union. Tuberc. Lung Dis. 2012, 16, 209–215. [Google Scholar] [CrossRef]
- Statistics South Africa. South Africa Demographic and Health Survey 2016; Statistics South Africa: Pretoria, South Africa, 2016; p. 76.
- Wen, S.; Yin, J.; Sun, Q. Impacts of social support on the treatment outcomes of drug-resistant tuberculosis: A systematic review and meta-analysis. BMJ Open. 2020, 10, e036985. [Google Scholar] [CrossRef]
- Darnton-Hill, I.; Mandal, P.P.; de Silva, A.; Bhatia, V.; Sharma, M. Opportunities to prevent and manage undernutrition to amplify efforts to end TB. Int. J. Tuberc. Lung Dis. Off. J. Int. Union. Tuberc. Lung Dis. 2022, 26, 6–11. [Google Scholar] [CrossRef]
- Smith, J.P.; Gandhi, N.R.; Shah, N.S.; Mlisana, K.; Moodley, P.; Johnson, B.A.; Allana, S.; Campbell, A.; Nelson, K.N.; Master, I.; et al. The Impact of Concurrent Antiretroviral Therapy and MDR-TB Treatment on Adverse Events. J. Acquir. Immune Defic. Syndr. 2020, 83, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, G.; Tjoa, K.; Iskandar, A.W.B.; Louisa, M.; Sagwa, E.L.; Padayatchi, N.; Soetikno, V. The effect of human immunodeficiency virus infection on adverse events during treatment of drug-resistant tuberculosis: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0248017. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, N.; Ahuja, S.D.; Akkerman, O.W.; Alffenaar, J.C.; Anderson, L.F.; Baghaei, P.; Bang, D.; Barry, P.M.; Bastos, M.L.; Behera, D.; et al. Treatment correlates of successful outcomes in pulmonary multidrug resistant tuberculosis: An individual patient data meta-analysis. Lancet 2018, 392, 821–834. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total (N = 246) | HIV− Patients (N = 89) | HIV+ on ART (N = 137) | HIV+ Not on ART (N = 20) | p-Value | |
|---|---|---|---|---|---|
| Age, mean (SD) | 36.0 (13.4) | 35.2 (17.6) | 36.1 (10.1) | 38.5 (11.4) | 0.43 |
| Age | <0.01 | ||||
| 0–15 | 9 (3.7%) | 8 (9.0%) | 1 (0.7%) | 0 (0.0%) | |
| 16–35 | 123 (50.0%) | 44 (49.4%) | 70 (51.1%) | 9 (45.0%) | |
| 36–50 | 81 (32.9%) | 19 (21.4%) | 55 (40.2%) | 7 (35.0%) | |
| >50 | 33 (13.4%) | 18 (20.2%) | 11 (8.0%) | 4 (20.0%) | |
| Sex | 0.12 | ||||
| Male | 134 (54.5%) | 56 (62.9%) | 69 (50.4%) | 9 (45.0%) | |
| Female | 112 (45.5%) | 33 (37.1%) | 68 (49.6%) | 11 (55.0%) | |
| Type of DR-TB | 0.13 | ||||
| Rif resistant | 95 (38.6%) | 38 (42.7%) | 45 (32.9%) | 12 (60.0%) | |
| Mono or poly resistant | 2 (0.8%) | 0 (0%) | 1 (0.7%) | 1 (5.0%) | |
| MDR (confirmed and not confirmed) | 79 (28.5%) | 25 (28.1%) | 41 (29.9%) | 4 (20.0%) | |
| Pre-XDR | 22 (8.9%)) | 11 (12.4%) | 11 (8.0%) | 0 (0.0%) | |
| XDR | 55 (22.4%) | 15 (16.9%) | 37 (27.0%) | 3 (15.0%) | |
| Unanswered | 2 (0.8%) | 0 (0%) | 2 (1.5%) | 0 (0.0%) | |
| Previous TB drug history | 0.11 | ||||
| New patient (no previous history) | 115 (46.8%) | 49 (55.1%) | 54 (39.4%) | 12 (60.0%) | |
| Previous treatment with 1st-line drugs | 105 (42.7%) | 31 (34.8%) | 67 (48.9%) | 7 (35.0%) | |
| Previous treatment with 2nd-line drugs | 1 (5.0%) | 8 (9.0%) | 9 (6.6%) | 1 (5.0%) | |
| Unanswered | 8 (3.3%) | 1 (1.1%) | 7 (5.1%) | 0 (0.0%) | |
| Classification of disease | 0.20 | ||||
| Pulmonary | 198 (80.5%) | 73 (82.0%) | 105 (76.6%) | 20 (100.0%) | |
| Extrapulmonary | 1 (0.4%) | 0 (0%) | 1 (0.7%) | 0 (0.0%) | |
| HTN | 0.09 | ||||
| Yes | 32 (13.0%) | 18 (20.2%) | 12 (8.8%) | 2 (10.0%) | |
| No | 210 (85.4%) | 70 (78.7%) | 123 (89.8%) | 17 (85.0%) | |
| Diabetes | 0.01 | ||||
| Yes | 18 (7.3%) | 12 (13.5%) | 4 (2.9%) | 2 (10.0%) | |
| No | 228 (92.7%) | 77 (86.5%) | 133 (97.1%) | 18 (90.0%) | |
| Hearing loss | 0.49 | ||||
| Yes | 18 (7.3%) | 8 (9.0%) | 10 (7.3%) | 0 (0.0%) | |
| No | 172 (69.9%) | 61 (68.5%) | 98 (71.5%) | 13 (65.0%) | |
| Of those who are HIV-positive, on cotrimoxazole | <0.01 | ||||
| Yes | 118 (75.6%) | 0 (0%) | 108 (79.4%) | 10 (50.0%) | |
| No | 24 (15.4%) | 0 (0%) | 16 (11.8%) | 8 (40.0%) | |
| Baseline BMI (mean, STD) | 19.6 (4.5) | 19.5 (4.0) | 19.5 (4.8) | 20.0 (4.6) | 0.58 |
| Pregnant | 0.26 | ||||
| Yes | 2 (1.8%) | 0 (0%) | 1 (1.5%) | 1 (9.1%) | |
| No | 88 (79.3%) | 28 (87.5%) | 52 (76.5%) | 8 (72.7%) | |
| GeneXpert completed | 0.04 | ||||
| Yes | 117 (47.6%) | 54 (60.7%) | 55 (40.2%) | 8 (40.0%) | |
| No | 55 (22.4%) | 16 (18.0%) | 33 (24.1%) | 6 (30.0%) | |
| TB microscopy completed | <0.01 | ||||
| Yes | 169 (68.7%) | 62 (69.7%) | 98 (71.5%) | 9 (45.0%) | |
| No | 34 (13.8%) | 19 (21.4%) | 12 (8.8%) | 3 (15.0%) | |
| First-line LPA completed | 0.091 | ||||
| Yes | 95 (38.6%) | 40 (44.9%) | 51 (37.2%) | 4 (20.0%) | |
| No | 79 (32.1%) | 31 (34.8%) | 41 (29.9%) | 7 (35.0%) | |
| Unanswered | 72 (29.3%) | 18 (20.2%) | 45 (32.9%) | 9 (45.0%) | |
| Second-line LPA completed | 0.15 | ||||
| Yes | 88 (35.8%) | 34 (38.2%) | 50 (36.5%) | 4 (20.0%) | |
| No | 86 (35.0%) | 36 (40.5%) | 43 (31.4%) | 7 (35.0%) | |
| Unanswered | 72 (29.3%) | 19 (21.4%) | 44 (32.1%) | 9 (45.0%) | |
| TB culture | <0.01 | ||||
| Yes | 151 (61.4%) | 56 (62.9%) | 89 (65.0%) | 6 (30.0%) | |
| No | 48 (19.5%) | 23 (25.8%) | 20 (14.6%) | 5 (25.0%) | |
| First-line drug sensitivity test (DST) | 0.04 | ||||
| Yes | 54 (22.0%) | 23 (25.8%) | 29 (21.2%) | 2 (10.0%) | |
| No | 134 (54.5%) | 53 (59.6%) | 72 (52.6%) | 9 (45.0%) | |
| Unanswered | 58 (23.6%) | 13 (14.6% | 36 (26.3%) | 9 (45.0%) | |
| Second-line drug sensitivity test (DST) | 0.05 | ||||
| Yes | 56 (22.8%) | 20 (22.5%) | 33 (24.1%) | 3 (15.0%) | |
| No | 131 (53.3%) | 55 (61.8%) | 68 (49.6%) | 8 (40.0%) | |
| Unanswered | 59 (24.0%) | 14 (15.7%) | 36 (26.3%) | 9 (45.0%) | |
| Regimen type | |||||
| Short regimen * | 96 (39%) | 45 (18.29%) | 46 (18.7%) | 5 (2.0%) | 0.04 |
| Long regimen * | 118 (48.16%) | 32 (13.06%) | 74 (30.20%) | 12 (4.90%) | 0.03 |
| Hospital | <0.01 | ||||
| Urban | 141 (57.3%) | 64 (71.9%) | 77 (56.2%) | 0 (0%) | |
| Suburban | 105 (42.7%) | 25 (28.1%) | 60 (43.8%) | 20 (100.0%) | |
| Education | 0.03 | ||||
| No school | 15 (6.1%) | 6 (6.7%) | 5 (3.7%) | 4 (20.0%) | |
| Some school | 210 (85.4%) | 74 (83.2%) | 123 (89.8%) | 13 (65.0%) | |
| Unanswered | 21 (8.5%) | 9 (10.1%) | 9 (6.6%) | 3 (15.0%) | |
| Mean number years of school (STD) | 8.9 (3.1) | 8.6 (3.2) | 9.2 (2.9) | 7.5 (4.3) | 0.25 |
| Income | |||||
| Salary wages | 26 (10.6%) | 6 (6.7%) | 18 (13.1%) | 2 (10.0%) | 0.31 |
| Casual wages | 14 (5.7%) | 4 (4.5%) | 8 (5.8%) | 2 (10.0%) | 0.66 |
| UIF (grant) | 2 (0.8%) | 2 (2.3%) | 0 (0.0%) | 0 (0.0%) | 0.17 |
| No income | 135 (54.9%) | 45 (50.6%) | 79 (57.7%) | 11 (55.0%) | 0.58 |
| Self-employed | 2 (0.8%) | 1 (1.1%) | 1 (0.7%) | 0 (0.0%) | 0.87 |
| Number of dependents living at home (mean, STD) | 1.73 (1.62) | 1.78 (1.94) | 1.75 (1.36) | 1.2 (1.69) | 0.51 |
| Any household contacts | 0.03 | ||||
| Yes | 236 (95.9%) | 87 (97.8%) | 132 (96.4%) | 17 (85.0%) | |
| No | 10 (4.1%) | 2 (2.3%) | 5 (3.7%) | 3 (15.0%) | |
| Smoker | 0.01 | ||||
| Yes | 86 (35.0%) | 41 (46.1%) | 40 (29.2%) | 5 (25.0%) | |
| No | 148 (60.2%) | 44 (49.4%) | 92 (67.2%) | 12 (60.0%) | |
| Alcohol use | 0.39 | ||||
| Non-drinker | 126 (51.6%) | 47 (53.4%) | 67 (49.3%) | 12 (60.0%) | |
| Light (1× month) | 46 (18.9%) | 14 (15.9%) | 28 (20.6%) | 4 (20.0%) | |
| Moderate (1× week) | 32 (13.1%) | 10 (11.4%) | 19 (14.0%) | 3 (15.0%) | |
| Heavy (daily) | 14 (5.7%) | 3 (3.4%) | 11 (8.1%) | 0 (0.0%) |
| Everyone (N = 246) | HIV− (N = 89) | HIV+ on ART (N = 137) | HIV+ Not on ART (N = 20) | |
|---|---|---|---|---|
| Success | 144 (58.5%) | 64 (71.9%) | 75 (54.7%) | 5 (25.0%) |
| Cure | 118 | 49 | 64 | 5 |
| Completed treatment | 26 | 15 | 11 | 0 |
| Non-success | 51 (20.7%) | 10 (11.2%) | 33 (24.1%) | 8 (40.0%) |
| Failed | 1 | 0 | 1 | 0 |
| Died | 39 | 6 | 25 | 8 |
| Lost to follow-up | 11 | 4 | 7 | 0 |
| Transferred out | 51 (20.7%) | 15 (16.9%) | 29 (21.2%) | 7 (35.0%) |
| Censored | 21 | 6 | 12 | 3 |
| Still on treatment | 10 | 1 | 8 | 1 |
| Missing | 8 | 5 | 3 | 0 |
| Moved out | 3 | 0 | 1 | 2 |
| Estimated OR for Success vs. Non-Success of DR-TB Treatment Outcomes | ||
|---|---|---|
| Characteristic | OR (95% CI) | p-Value |
| Age (years) (continuous) | 0.99 (0.97, 1.02) | 0.57 |
| 0–35 (versus >35) | 0.80 (0.42, 1.54) | 0.51 |
| Female sex | 1.08 (0.57, 2.07) | 0.82 |
| HIV status | ||
| HIV-negative | 10.24 (2.79, 37.61) | <0.01 |
| HIV+, on ART | 3.64 (1.11, 11.95) | <0.05 |
| HIV+, not on ART | Ref | – |
| Urban hospital—JPH (vs. suburban hospital—MPH) | 6.97 (3.46, 14.04) | <0.001 |
| Number of years of education (continuous) | 1.02 (0.92, 1.14) | 0.68 |
| BMI (continuous) | 1.05 (0.96, 1.16) | 0.26 |
| Smoker (vs. non-smoker) | 0.87 (0.44, 1.71) | 0.68 |
| Alcohol use | ||
| Non-drinker | Ref | |
| Drinker (mild/mod/heavy) | 0.69 (0.37, 1.32) | 0.26 |
| Income | ||
| Any income (salary, casual wages, grant, disability) | 0.55 (0.23, 1.30) | 0.17 |
| No income | Ref | |
| Estimated OR for Success vs. Death of DR-TB Treatment Outcomes | ||
|---|---|---|
| Characteristic | OR (95% CI) | p-Value |
| HIV status | ||
| HIV-negative | 13.06 (3.21, 53.11) | 0.0003 |
| HIV+, on ART | 4.10 (1.22, 13.72) | 0.0223 |
| HIV+, not on ART | Ref | – |
| Estimated OR for Transfer Out vs. Non-Success of DR-TB Treatment Outcomes | ||
|---|---|---|
| Characteristic | OR (95% CI) | p-Value |
| Age (years) (continuous) | 1.00 (0.98, 1.04) | 0.57 |
| 0–35 (versus >35) | 0.67 (0.31, 1.47) | 0.32 |
| Female sex | 1.88 (0.86, 4.13) | 0.11 |
| HIV status | ||
| HIV-negative | 1.71 (0.47, 6.24) | 0.41 |
| HIV+, on ART | 1.00 (0.32, 3.11) | 0.99 |
| HIV+, not on ART | Ref | – |
| Urban hospital (versus suburban hospital) | 0.39 (0.16, 0.99) | 0.047 |
| Number of years of education (continuous) | 1.04 (0.91, 1.20) | 0.56 |
| BMI (continuous) | 1.09 (1.00, 1.19) | 0.061 |
| Smoker (vs. non-smoker) | 0.47 (0.19, 1.14) | 0.093 |
| Alcohol use | ||
| Non-drinker | Ref | |
| Drinker (mild/mod/heavy) | 0.79 (0.36, 1.72) | 0.55 |
| Income | ||
| Any income (salary, casual wages, grant, disability) | 0.93 (0.34, 2.51) | 0.88 |
| No income | Ref | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van de Water, B.; Abuelezam, N.; Hotchkiss, J.; Botha, M.; Ramangoaela, L. The Effect of HIV and Antiretroviral Therapy on Drug-Resistant Tuberculosis Treatment Outcomes in Eastern Cape, South Africa: A Cohort Study. Viruses 2023, 15, 2242. https://doi.org/10.3390/v15112242
van de Water B, Abuelezam N, Hotchkiss J, Botha M, Ramangoaela L. The Effect of HIV and Antiretroviral Therapy on Drug-Resistant Tuberculosis Treatment Outcomes in Eastern Cape, South Africa: A Cohort Study. Viruses. 2023; 15(11):2242. https://doi.org/10.3390/v15112242
Chicago/Turabian Stylevan de Water, Brittney, Nadia Abuelezam, Jenny Hotchkiss, Mandla Botha, and Limpho Ramangoaela. 2023. "The Effect of HIV and Antiretroviral Therapy on Drug-Resistant Tuberculosis Treatment Outcomes in Eastern Cape, South Africa: A Cohort Study" Viruses 15, no. 11: 2242. https://doi.org/10.3390/v15112242