
Hepatitis B Virus Genotype H: Epidemiological, Molecular, and Clinical Characteristics in Mexico

Abstract
:1. Introduction
2. Methods
3. An Overview of the Major Milestones of Viral Hepatitis
4. Epidemiology of HBV Infections in Mexico from Serology to Molecular Biology
4.1. The Early Seroepidemiological Diagnostic Studies in Mexico
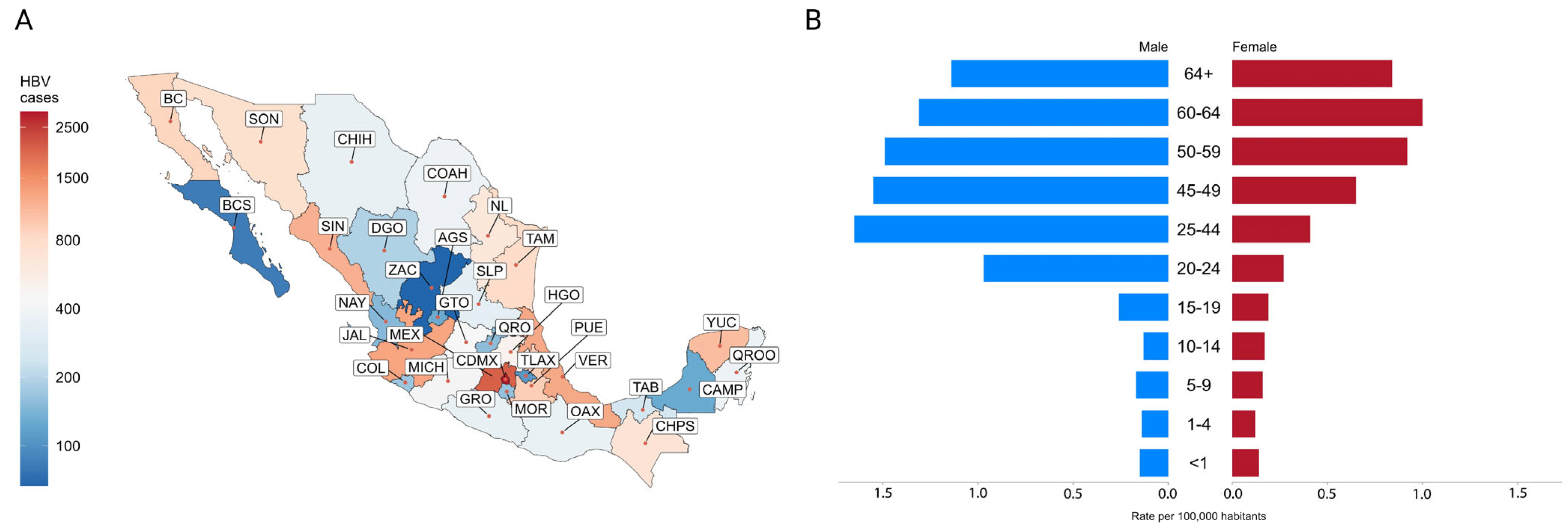
4.2. Incidence and Prevalence of HBV Infection in Mexico
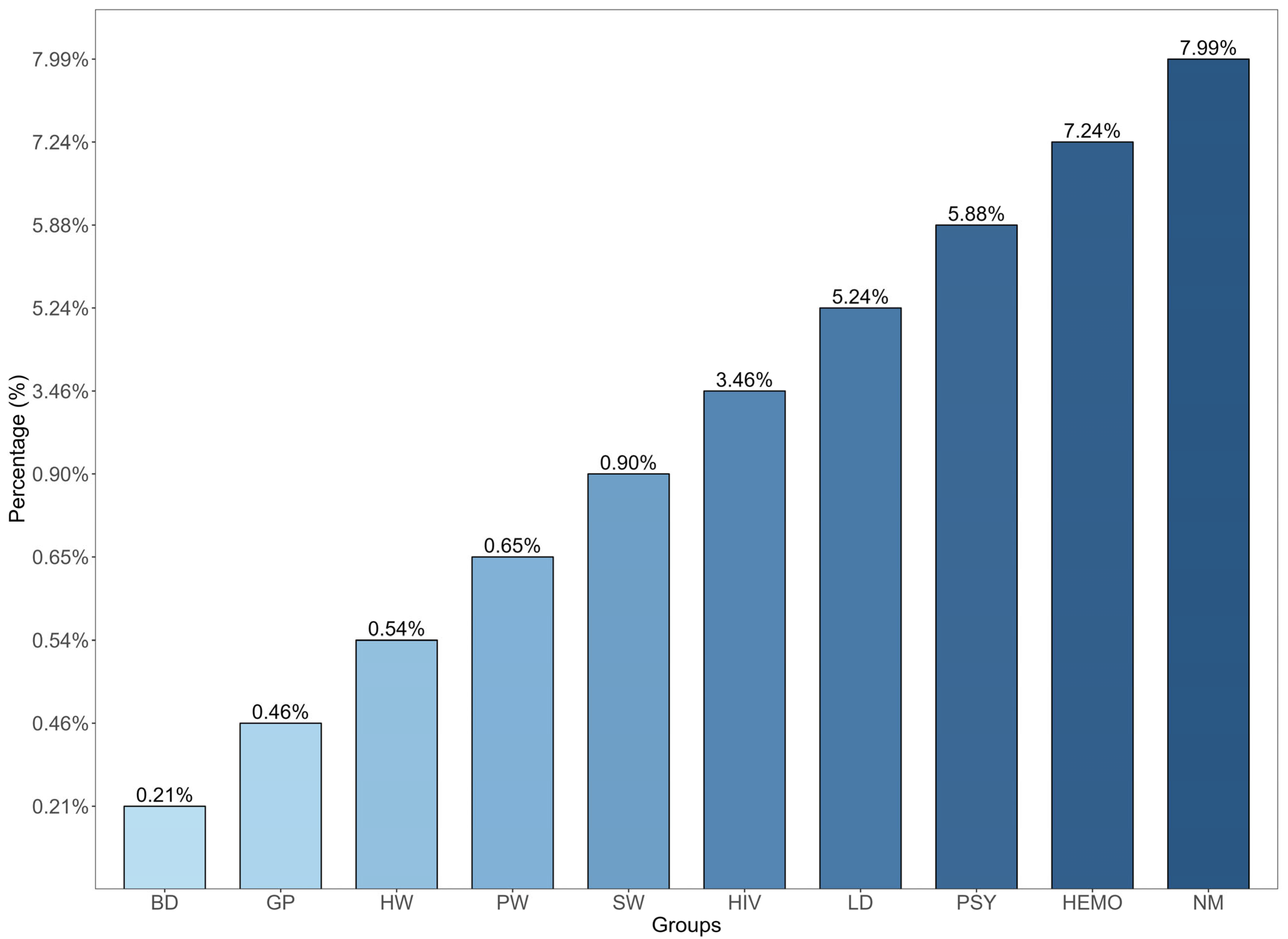
4.2.1. Low-Risk Groups
4.2.2. Intermediate-to-High-Risk Group
4.3. Occult Hepatitis B and Misdiagnosis of HBV Infection
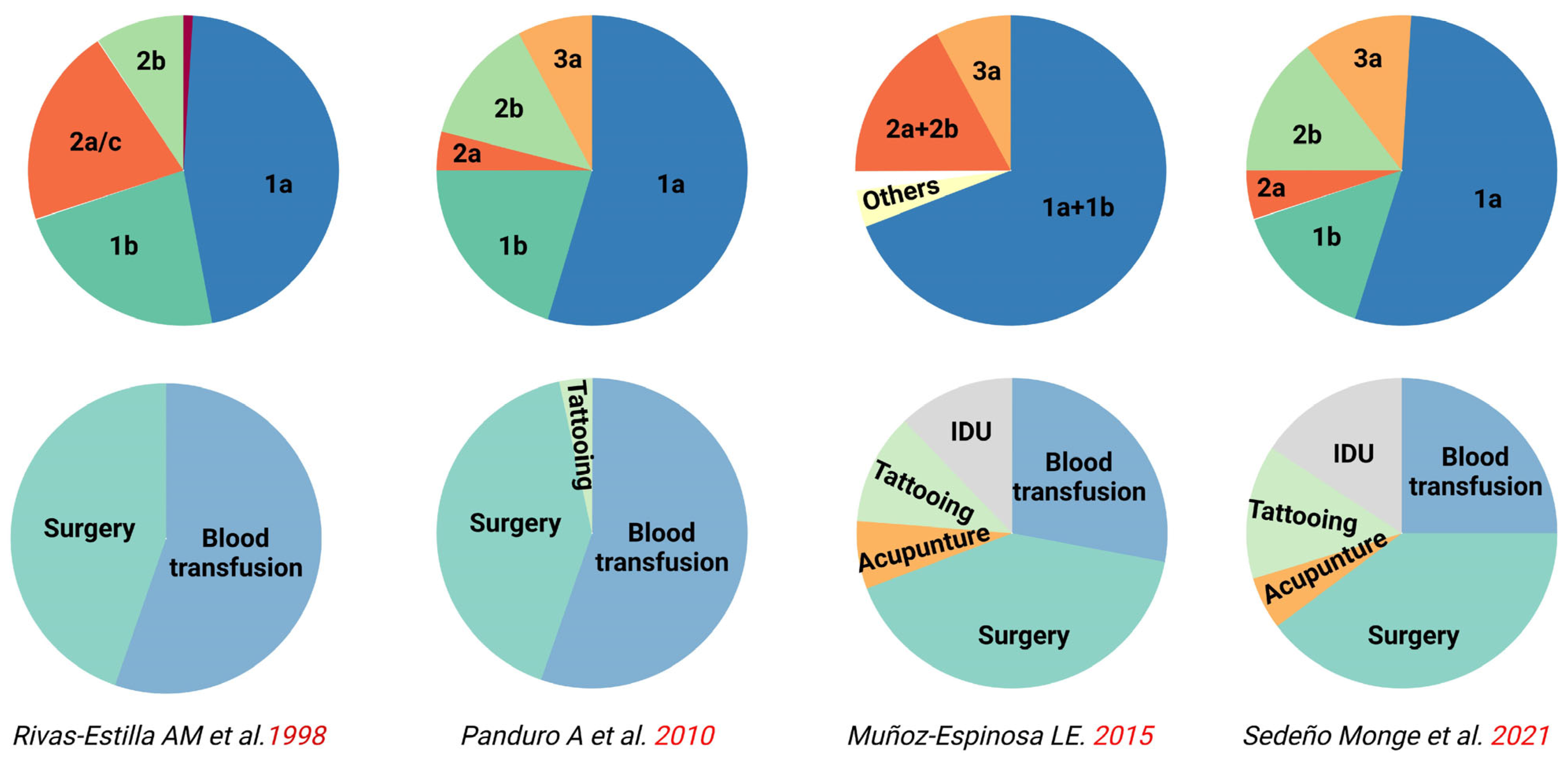
4.4. Major Routes of Transmission and Risk Factors
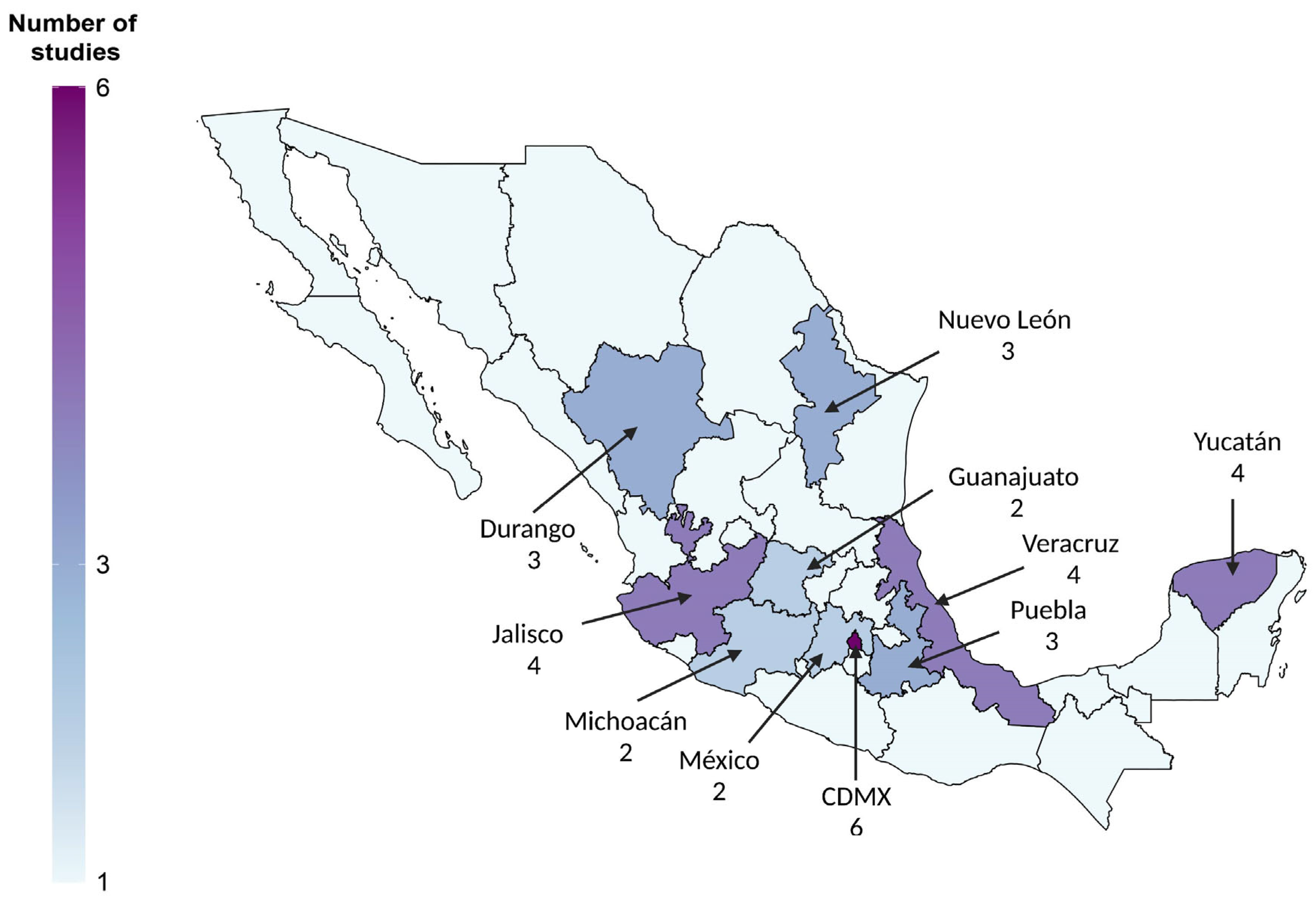
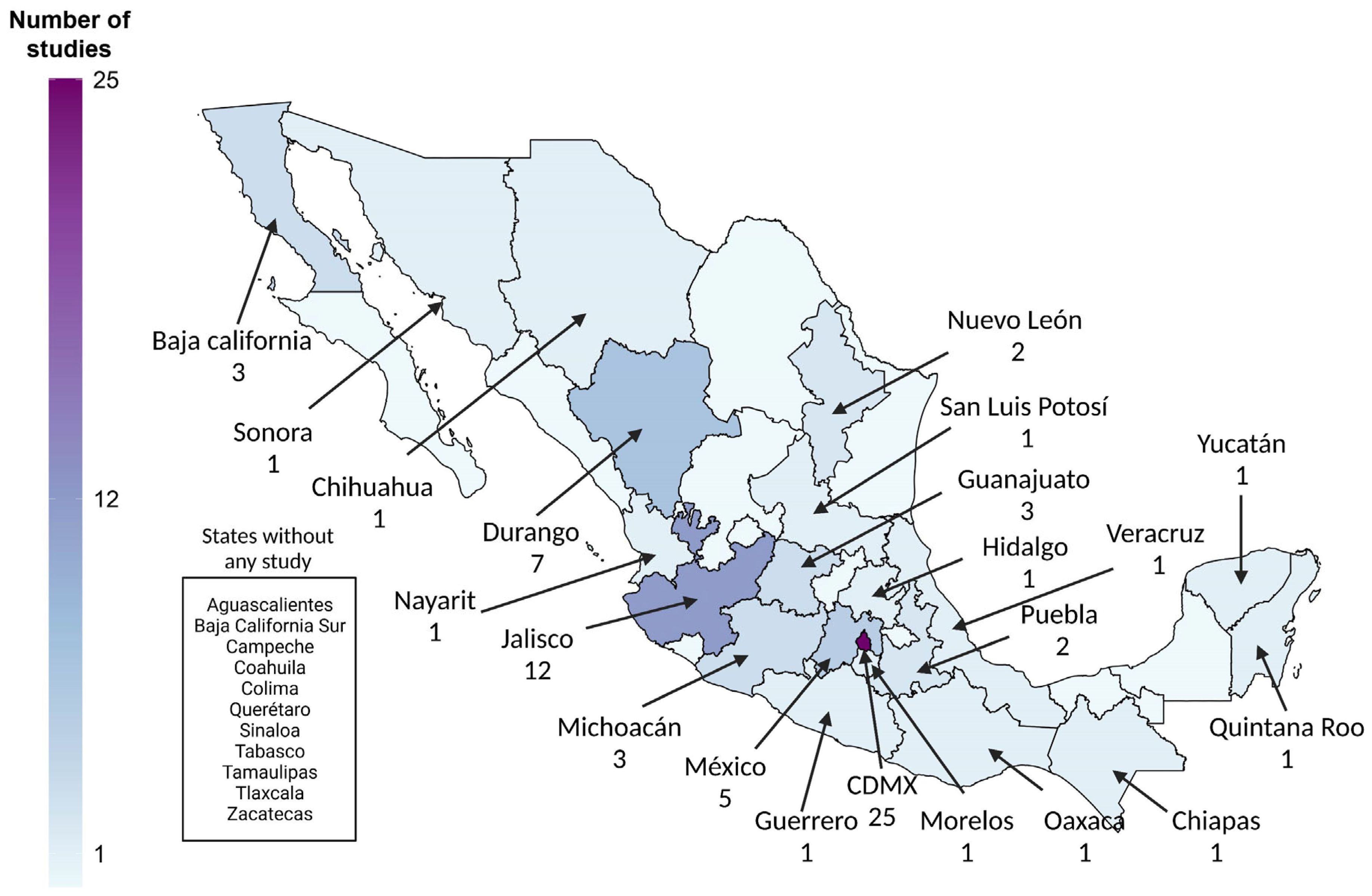
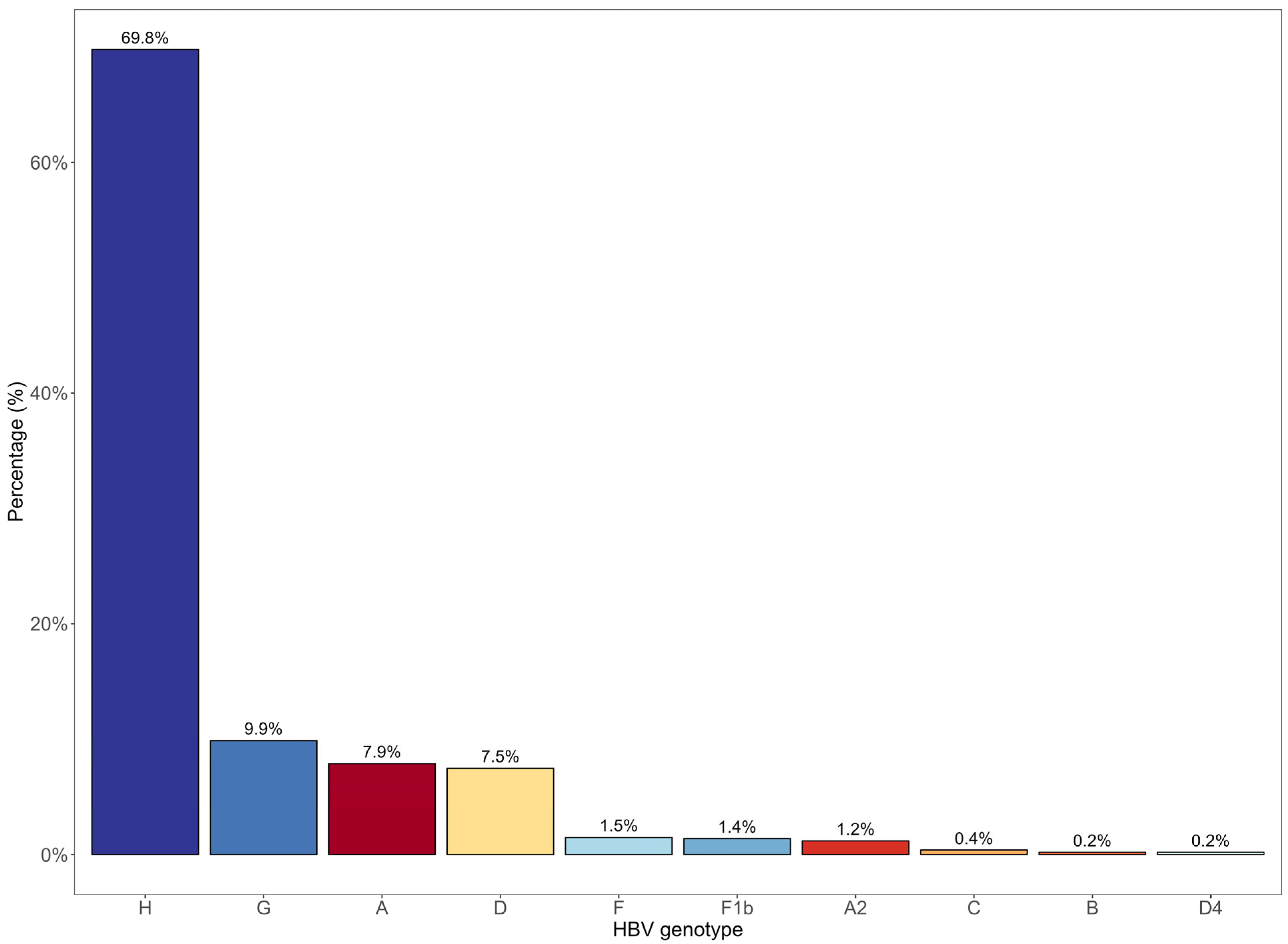
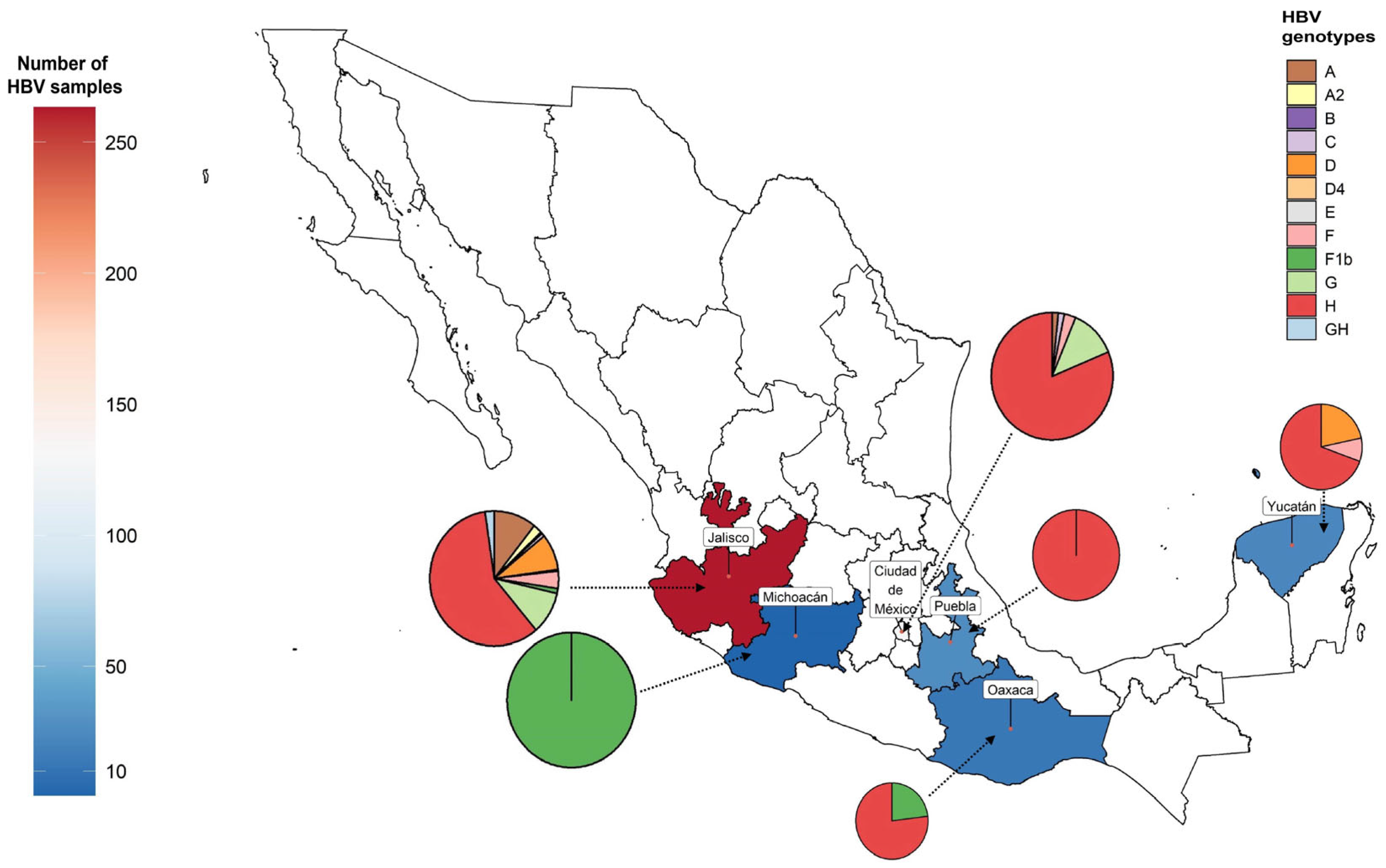
4.5. Molecular Epidemiology of HBV in Mexico
4.6. Reconstruction of HBV/H Infections in the Americas
4.7. Genetic Variability of HBV/H: Antiviral Resistance and Immune Escape Mutations
5. Clinical Aspects of HBV Infections in Mexico
5.1. HBV Infections in Cirrhosis and HCC
5.2. Mixed HBV Infections
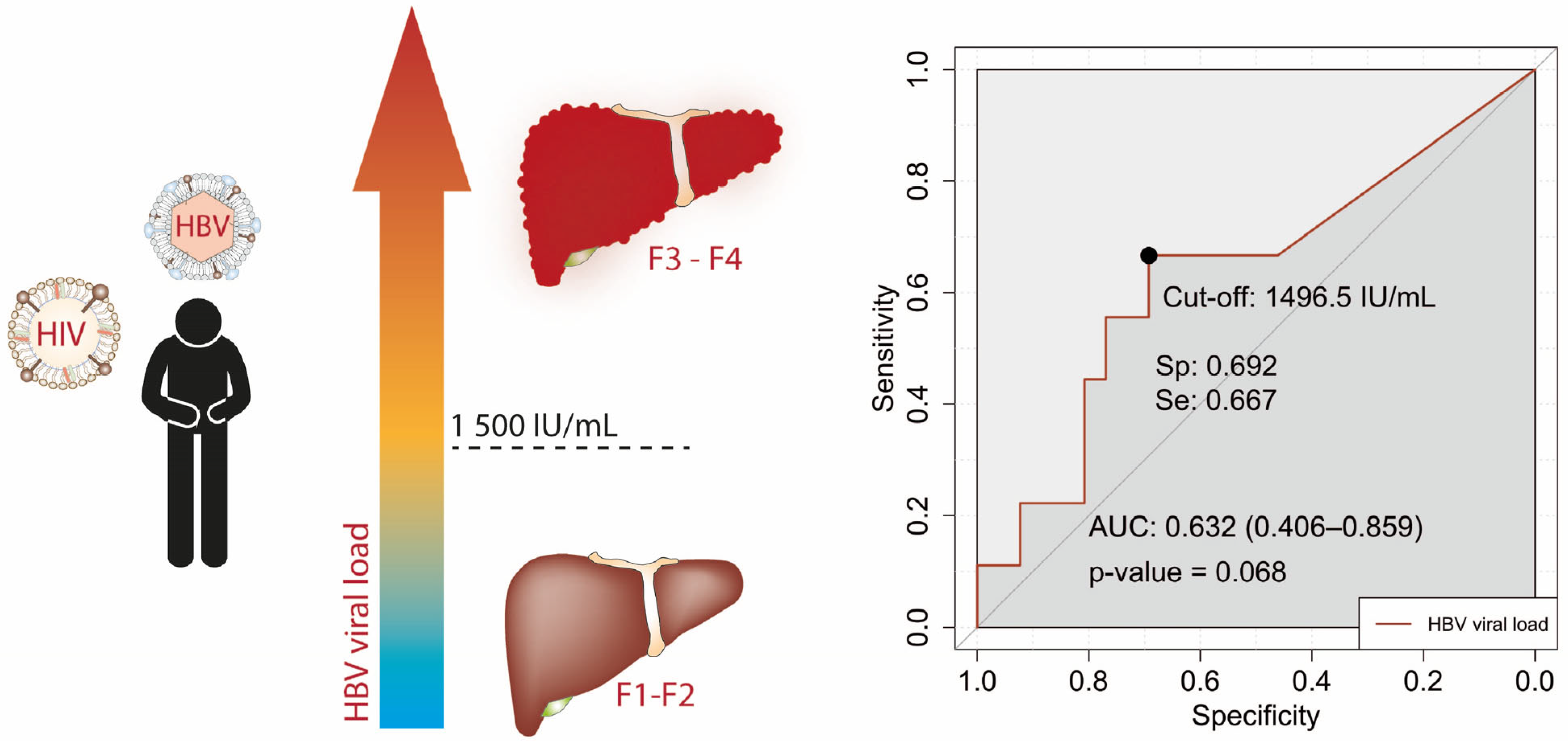
5.3. The Clinical Characteristics of HBV Infections in Mexico Do Not Match International Criteria for Treatment
6. HBV Vaccine
7. Discussion and Future Directions
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| State | Total Number | State | Total Number | ||
|---|---|---|---|---|---|
| Mexico City | CDMX | 2915 | Quintana Roo | QROO | 368 |
| México State | MEX | 2012 | Oaxaca | OAX | 358 |
| Jalisco | JAL | 1264 | Chihuahua | CHIH | 348 |
| Veracruz | VER | 1227 | Guerrero | GRO | 346 |
| Sinaloa | SIN | 1157 | San Luis Potosí | SLP | 320 |
| Yucatán | YUC | 1044 | Tabasco | TAB | 247 |
| Puebla | PUE | 920 | Durango | DGO | 191 |
| Baja California | BC | 864 | Colima | COL | 171 |
| Tamaulipas | TAM | 803 | Morelos | MOR | 163 |
| Sonora | SON | 742 | Querétaro | QRO | 156 |
| Chiapas | CHPS | 676 | Nayarit | NAY | 149 |
| Nuevo León | NL | 640 | Aguascalientes | AGS | 128 |
| Hidalgo | HGO | 505 | Campeche | CAMP | 127 |
| Guanajuato | GTO | 438 | Tlaxcala | TLAX | 107 |
| Michoacán | MICH | 418 | Baja California Sur | BCS | 83 |
| Coahuila | COAH | 375 | Zacatecas | ZAC | 67 |
| Study Groups | Diagnostic Marker | Prevalence %(95% CI) | Articles (N) | References |
|---|---|---|---|---|
| Low Risk | ||||
| University students | HBsAg | 0.29 (0.08–1.0) | 3 | [55,152,153] |
| General population | HBsAg | 0.46 (0.16–1.32) | 6 | [50,53,54,55,56,57] |
| Blood donors | HBsAg | 0.21 (0.15–0.29) | 20 | [47,55,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75] |
| Anti-HBc | 1.43 (1.05–1.95) | 5 | [60,66,67,74,75] | |
| High Risk | ||||
| HCV patients | HBsAg | 0 (0.01–2.98) | 1 | [78] |
| Lupus erythematosus patients | HBsAg | 0 (0.03–6.46) | 1 | [154] |
| Healthcare workers | HBsAg | 0.54 (0.19–1.52) | 4 | [81,155,156,157] |
| Pregnant women | HBsAg | 0.65 (0.37–1.12) | 6 | [55,106,107,108,109,110] |
| Anti-HBc | 1.75 (1.50–2.04) | 3 | [106,107,108] | |
| Sexual Workers | HBsAg | 0.90 (0.32–2.50) | 8 | [55,158,159,160,161,162,163,164] |
| Low income/Rural | HBsAg | 1.03 (0.83–1.27) | 2 | [134,165] |
| Anti-HBc | 20.89 (1.83–78.92) | 2 | [165,166] | |
| Children | HBsAg | 3.02 (1.40–6.36) | 2 | [167,168] |
| HIV/AIDS patients | HBsAg | 3.46 (1.30–8.88) | 7 | [78,90,91,92,93,94,95] |
| Drug addicts | HBsAg | 4.44 (2.24–8.63) | 1 | [55] |
| Deferred blood donors | HBsAg | 4.82 (1.82–12.15) | 1 | [78] |
| Liver-diseased patients | HBsAg | 5.24 (3.08–8.80) | 6 | [48,59,86,87,88,89] |
| Psychiatric patients | HBsAg | 5.88 (2.89–11.58) | 2 | [84,85] |
| Emergency-room attendees | HBsAg | 6.93 (5.45–8.77) | 1 | [169] |
| Hemodialysis/transfusion | HBsAg | 7.24 (5.66–9.21) | 4 | [80,81,82,83] |
| Native Mexicans | HBsAg | 7.99 (5.49–11.49) | 2 | [78,79] |
| Anti-HBc | 13.88 (6.23–28.08) | 3 | [78,79,166] | |
| Occult hepatitis B | HBV DNA | 8.27 (2.88–21.53) | 10 | [67,74,75,79,91,93,95,98,99,100] |
References
- Kocher, A.; Papac, L.; Barquera, R.; Key, F.M.; Spyrou, M.A.; Hübler, R.; Rohrlach, A.B.; Aron, F.; Stahl, R.; Wissgott, A. Ten Millennia of Hepatitis B Virus Evolution. Science 2021, 374, 182–188. [Google Scholar] [CrossRef]
- Nevola, R.; Beccia, D.; Rosato, V.; Ruocco, R.; Mastrocinque, D.; Villani, A.; Perillo, P.; Imbriani, S.; Delle Femine, A.; Criscuolo, L.; et al. HBV Infection and Host Interactions: The Role in Viral Persistence and Oncogenesis. Int. J. Mol. Sci. 2023, 24, 7651. [Google Scholar] [CrossRef]
- Velkov, S.; Ott, J.J.; Protzer, U.; Michler, T. The Global Hepatitis B Virus Genotype Distribution Approximated from Available Genotyping Data. Genes 2018, 9, 495. [Google Scholar] [CrossRef]
- Mühlemann, B.; Jones, T.C.; Damgaard, P.d.B.; Allentoft, M.E.; Shevnina, I.; Logvin, A.; Usmanova, E.; Panyushkina, I.P.; Boldgiv, B.; Bazartseren, T.; et al. Ancient Hepatitis B Viruses from the Bronze Age to the Medieval Period. Nature 2018, 557, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Kramvis, A. Genotypes and Genetic Variability of Hepatitis B Virus. Intervirology 2014, 57, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Sunbul, M. Hepatitis B Virus Genotypes: Global Distribution and Clinical Importance. World J. Gastroenterol. WJG 2014, 20, 5427–5434. [Google Scholar] [CrossRef] [PubMed]
- Revill, P.A.; Tu, T.; Netter, H.J.; Yuen, L.K.W.; Locarnini, S.A.; Littlejohn, M. The Evolution and Clinical Impact of Hepatitis B Virus Genome Diversity. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 618–634. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.-H.; Wu, C.-C.; Chen, X.-W.; Li, X.; Li, J.; Lu, M.-J. Genetic Variation of Hepatitis B Virus and Its Significance for Pathogenesis. World J. Gastroenterol. 2016, 22, 126–144. [Google Scholar] [CrossRef]
- Kramvis, A.; Kew, M.C. Relationship of Genotypes of Hepatitis B Virus to Mutations, Disease Progression and Response to Antiviral Therapy. J. Viral Hepat. 2005, 12, 456–464. [Google Scholar] [CrossRef]
- Tatematsu, K.; Tanaka, Y.; Kurbanov, F.; Sugauchi, F.; Mano, S.; Maeshiro, T.; Nakayoshi, T.; Wakuta, M.; Miyakawa, Y.; Mizokami, M. A Genetic Variant of Hepatitis B Virus Divergent from Known Human and Ape Genotypes Isolated from a Japanese Patient and Provisionally Assigned to New Genotype J. J. Virol. 2009, 83, 10538–10547. [Google Scholar] [CrossRef]
- Yu, H.; Yuan, Q.; Ge, S.-X.; Wang, H.-Y.; Zhang, Y.-L.; Chen, Q.-R.; Zhang, J.; Chen, P.-J.; Xia, N.-S. Molecular and Phylogenetic Analyses Suggest an Additional Hepatitis B Virus Genotype “I”. PLoS ONE 2010, 5, e9297. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-L.; Kao, J.-H. Hepatitis B Virus Genotypes and Variants. Cold Spring Harb. Perspect. Med. 2015, 5, a021436. [Google Scholar] [CrossRef]
- Panduro, A.; Maldonado-Gonzalez, M.; Fierro, N.A.; Roman, S. Distribution of HBV Genotypes F and H in Mexico and Central America. Antivir. Ther. 2013, 18, 475–484. [Google Scholar] [CrossRef]
- Araujo, N.M.; Osiowy, C. Hepatitis B Virus Genotype G: The Odd Cousin of the Family. Front. Microbiol. 2022, 13, 872766. [Google Scholar] [CrossRef]
- Roman, S.; Panduro, A. HBV Endemicity in Mexico Is Associated with HBV Genotypes H and G. World J. Gastroenterol. 2013, 19, 5446–5453. [Google Scholar] [CrossRef]
- World Health Organization WHO. Hepatitis B Factsheet 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 30 August 2023).
- World Health Organization Global Health Sector Strategy on Viral Hepatitis 2016–2021. Towards Ending Viral Hepatitis. Available online: https://www.who.int/publications-detail-redirect/WHO-HIV-2016.06 (accessed on 8 August 2023).
- Hiebert, L.; Ward, J.W. Strategic Information to Guide Elimination of Viral Hepatitis. Lancet Gastroenterol. Hepatol. 2023, 8, 291–292. [Google Scholar] [CrossRef] [PubMed]
- Polaris Observatory Collaborators. Global Prevalence, Cascade of Care, and Prophylaxis Coverage of Hepatitis B in 2022: A Modelling Study. Lancet Gastroenterol. Hepatol. 2023, 8, 879–907. [Google Scholar] [CrossRef] [PubMed]
- Revill, P.A.; Chisari, F.V.; Block, J.M.; Dandri, M.; Gehring, A.J.; Guo, H.; Hu, J.; Kramvis, A.; Lampertico, P.; Janssen, H.L.A.; et al. A Global Scientific Strategy to Cure Hepatitis B. Lancet Gastroenterol. Hepatol. 2019, 4, 545–558. [Google Scholar] [CrossRef]
- Revill, P.; Testoni, B.; Locarnini, S.; Zoulim, F. Global Strategies Are Required to Cure and Eliminate HBV Infection. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Latin America Roundtable Synthesis.Pdf. Available online: https://www.globalhep.org/sites/default/files/content/webinar/files/2022-03/Latin%20America%20Roundtable%20Synthesis.pdf (accessed on 16 October 2023).
- Roblero, J.P.; Arab, J.P.; Mezzano, G.; Mendizabal, M. Hepatitis C Virus Infection: What Are We Currently Doing in Latin America about WHO’s Proposals for 2030? Clin. Liver Dis. 2021, 18, 72–75. [Google Scholar] [CrossRef]
- Ridruejo, E.; Soza, A. Which Strategies Should Be Implemented in Latin America to Eradicate Hepatitis C Virus by 2030? Clin. Liver Dis. 2019, 13, 43–45. [Google Scholar] [CrossRef]
- De la Torre Rosas, A.; Kershenobich, D.; Svarch, A.E.; López-Gatell, H. Eliminating Hepatitis C in Mexico: A Primary Health Care Approach. Clin. Liver Dis. 2021, 18, 219–224. [Google Scholar] [CrossRef]
- Wolpert Barraza, E.; Kershenobich Stalnikowitz, D.; Guerrero Guerrero, J.E.; de la Torre Rosas, A. Micro-Elimination of Hepatitis C in Low- and Middle-Income Settings: Challenges and Windows of Opportunity. Clin. Liver Dis. 2022, 19, 38–40. [Google Scholar] [CrossRef] [PubMed]
- García-Sepúlveda, C.A.; Laguna-Meraz, S.; Panduro, A. How Far Is Mexico from Viral Hepatitis Global Health Sector Strategy 2030 Targets. Ann. Hepatol. 2020, 19, 123–125. [Google Scholar] [CrossRef]
- Campollo, O.; Roman, S. Consensus and Clinical Practice Guidelines in Latin America: Who, Where, When and How. Ann. Hepatol. 2019, 18, 281–284. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting Meta-Analyses in R with the Metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Jose-Abrego, A.; Roman, S.; Rebello Pinho, J.R.; de Castro, V.F.D.; Panduro, A. Hepatitis B Virus (HBV) Genotype Mixtures, Viral Load, and Liver Damage in HBV Patients Co-Infected With Human Immunodeficiency Virus. Front. Microbiol. 2021, 12, 640889. [Google Scholar] [CrossRef]
- Pappas, G.; Kiriaze, I.J.; Falagas, M.E. Insights into Infectious Disease in the Era of Hippocrates. Int. J. Infect. Dis. 2008, 12, 347–350. [Google Scholar] [CrossRef]
- Cuthbert, J.A. Hepatitis A: Old and New. Clin. Microbiol. Rev. 2001, 14, 38–58. [Google Scholar] [CrossRef]
- MacCallum, F.O. Homologous Serum Hepatitis. Proc. R. Soc. Med. 1946, 39, 655–657. [Google Scholar] [CrossRef]
- Blumberg, B.S. A “New” Antigen in Leukemia Sera. JAMA J. Am. Med. Assoc. 1965, 191, 541. [Google Scholar] [CrossRef]
- Blumberg, B.S.; Gerstley, B.J.; Hungerford, D.A.; London, W.T.; Sutnick, A.I. A Serum Antigen (Australia Antigen) in Down’s Syndrome, Leukemia, and Hepatitis. Ann. Intern. Med. 1967, 66, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Prince, A.M. An Antigen Detected in the Blood during the Incubation Period of Serum Hepatitis. Proc. Natl. Acad. Sci. USA 1968, 60, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Okochi, K.; Murakami, S. Observations on Australia Antigen in Japanese. Vox Sang. 1968, 15, 374–385. [Google Scholar] [CrossRef]
- Shulman, N.R.; Hirschman, R.J.; Barker, L.F. Viral Hepatitis. Ann. Intern. Med. 1970, 72, 257–269. [Google Scholar] [CrossRef]
- Galibert, F.; Mandart, E.; Fitoussi, F.; Tiollais, P.; Charnay, P. Nucleotide Sequence of the Hepatitis B Virus Genome (Subtype Ayw) Cloned in E. Coli | Nature. Nature 1979, 281, 646–650. [Google Scholar] [CrossRef]
- Charnay, P.; Pourcel, C.; Louise, A.; Fritsch, A.; Tiollais, P. Cloning in Escherichia Coli and Physical Structure of Hepatitis B Virion DNA. Proc. Natl. Acad. Sci. USA 1979, 76, 2222–2226. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, P.R.; Ruiz-Opazo, N.; Shouval, D.; Shafritz, D.A. Identification of Integrated Hepatitis B Virus DNA and Expression of Viral RNA in an HBsAg-Producing Human Hepatocellular Carcinoma Cell Line. Nature 1980, 286, 531–533. [Google Scholar] [CrossRef]
- Miyakawa, Y.; Mizokami, M. Classifying Hepatitis B Virus Genotypes. Intervirology 2003, 46, 329–338. [Google Scholar] [CrossRef]
- Kay, A.; Zoulim, F. Hepatitis B Virus Genetic Variability and Evolution. Virus Res. 2007, 127, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, H.; Tsuda, F.; Sakugawa, H.; Sastrosoewignjo, R.I.; Imai, M.; Miyakawa, Y.; Mayumi, M. Typing Hepatitis B Virus by Homology in Nucleotide Sequence: Comparison of Surface Antigen Subtypes. J. Gen. Virol. 1988, 69 Pt 10, 2575–2583. [Google Scholar] [CrossRef]
- Norder, H.; Couroucé, A.-M.; Magnius, L.O. Complete Genomes, Phylogenetic Relatedness, and Structural Proteins of Six Strains of the Hepatitis B Virus, Four of Which Represent Two New Genotypes. Virology 1994, 198, 489–503. [Google Scholar] [CrossRef]
- Stuyver, L.; De Gendt, S.; Van Geyt, C.; Zoulim, F.; Fried, M.; Schinazi, R.F.; Rossau, R. A New Genotype of Hepatitis B Virus: Complete Genome and Phylogenetic Relatedness. Microbiology 2000, 81, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda, B.; Landa, L.; Aubanel, M.; Rodriguez-Moyado, H. Investigación Del Antígeno Asociado a La Hepatitis (Australia) En Donadores “Profesionales” de Sangre. Gac. Med. Mex. 1971, 102, 615–627. [Google Scholar] [PubMed]
- Sepulveda, B.N.; Rattoni, M.; Stoppen, L. Landa El Analisis Radioinmunologico Del Antigeno de La Hepatitis B. Gac. Med. Mex. 1973, 106, 123–130. [Google Scholar] [PubMed]
- Bustamante-Calvillo, M.E.; Ruiz-Gómez, J.; Ruíz Rodríguez, A.J.; Gutiérrez, G. Encuesta Serológica En Niños de La Ciudad de Mexico. X. Frecuencia de Antígeno Australia En Una Población Hospitalaria. Rev. Mex. Pediatr. 1972, 41, 623. [Google Scholar]
- Landa, L. Seroepidemiologia de La Hepatitis B. Gac. Med. Mex. 1976, 111, 85. [Google Scholar]
- Barriga Angulo, G.; Yxcapa, S.; Ruiz Sanchez, D.; Lopez Velarde, M.A. Exposicion Ocupacional a La Hepatitis Viral Del Tipo B En Un Centro Medico. Rev. Méd IMSS 1984, 22, 169–175. [Google Scholar]
- Bustamante-Calvillo, M.E.; Correa Bucio, M.E.; Alvarez-Muñoz, M.T.; Ruiz-Gómez, J.; Muñoz, O. Etiologia de La Hepatitis En La Ciudad de Mexico. Bol. Med. Hosp. Infant. Mex. 1986, 44, 5–10. [Google Scholar]
- López-Gatell, H.; García-García, L.; Echániz-Avilés, G.; Cruz-Hervert, P.; Olamendi-Portugal, M.; Sanchez-Alemán, M.Á.; Romero-Martínez, M.; DeAntonio, R.; Cervantes-Apolinar, M.Y.; Cortes-Alcalá, R.; et al. Hepatitis B Seroprevalence in 10-25-Year-Olds in Mexico-the 2012 National Health and Nutrition Survey (ENSANUT) Results. Hum. Vaccines Immunother. 2019, 15, 433–439. [Google Scholar] [CrossRef]
- Alvarez-Muñoz, M.T.; Bustamante-Calvillo, E.; Martínez-García, C.; Moreno-Altamirando, L.; Guiscafre-Gallardo, H.; Guiscafre, J.P.; Muñoz, O. Seroepidemiology of the Hepatitis B and Delta in the Southeast of Chiapas, Mexico. Arch. Investig. Med. 1989, 20, 189–195. [Google Scholar]
- Alvarez-Esquivel, C.; Sifuentes-Alvarez, A.; Perez-Ochoa, J.F.; Garcia-Corral, N.; Rodriguez-Briones, A.; Gonzalez-Castañeda, J.L.; Alonso-Muñoz, M.T.; Bracho-Huemoeller, A. Serorreactividad al antígeno de superficie del virus de la hepatitis B en diversos grupos de población de la ciudad de Durango, México. Gac. Med. Mex. 2008, 144, 481–484. [Google Scholar]
- Carnalla, M.; Vidaña-Pérez, D.; Alpuche-Aranda, C.; Chávez-Tapia, N.C.; Romero-Martínez, M.; Shamah-Levy, T.; Barrientos-Gutiérrez, T. Hepatitis B Infection in Mexican Adults: Results of a Nationally Representative Survey. Ann. Hepatol. 2022, 27 (Suppl. S1), 100583. [Google Scholar] [CrossRef] [PubMed]
- Valdespino, J.L.; Conde-González, C.J.; Olaiz-Fernández, G.; Palma, O.; Sepúlveda, J. Prevalencia en México de la infección y el estado de portador de la hepatitis B en adultos. Salud Pública México 2007, 49, s404–s411. [Google Scholar] [CrossRef]
- Alvarez-Muñoz, M.T.; Bustamante-Calvillo, M.E.; Guiscafre-Gallardo, J.P.; Munoz, O. Hepatitis B y Delta: Prevalencia de Marcadores Seroepidemiologicos En Donadores de Sangre Voluntarios y Su Grupo Familiar. Gac. Med. Mex. 1991, 127, 399–404. [Google Scholar]
- Souto, C.A.; Simón, J.; Pulido, M.d.l.A.; Hernández, A.; García, I.C.; del Río, C.A. Prevalencia de marcadores para hepatitis A, B y C en un hospital de México. Salud Pública México 1994, 36, 257–262. [Google Scholar]
- Ayala Gaytan, J.J.; Guerra Avalos, F.J.; Mora Brondo, P.; Casillas Romo, A. Prevalencia de Marcadores Virales Para Hepatitis B, C y Virus de La Inmunodeficiencia Humana En Donadores de Sangre Voluntarios En El Noreste de Mexico. Gastroenterol. México 1997, 62, 250–253. [Google Scholar]
- Tristán Rojas, C.M.; Najera Tobias, E.; Cázares Taméz, R.; Flores Aréchiga, A. Estudio Comparativo de La Seroprevalencia Observada En Diferentes Bancos de Sangre de La Republica Mexicana. Rev. Mex. Patol. Clínica 1999, 46, 34. [Google Scholar]
- Barragán, J.R.; Muñoz-Valle, J.F.; Navarro-Hernández, R.E. Frecuencia de anticuerpos contra el HIV, HCV y HBsAg en donadores familiares en el Hospital del Carmen de la Ciudad de Guadalajara, Jalisco. Rev. Mex. Patol. Clin. 1999, 46, 243–248. [Google Scholar]
- Méndez-Sánchez, N.; Baptista-González, H.; Sánchez-Gómez, R.H.; Bordes-Aznar, J.; Uribe-Esquivel, M. Prevalencia de hepatitis B y C en donadores de sangre en un hospital de tercer nivel de la ciudad de México. Salud Pública México 1999, 41, 475–478. [Google Scholar] [CrossRef]
- Carreto-Vélez, M.A.; Carrada-Bravo, T.; Martínez-Magdaleno, A. Seroprevalencia de VHB, VHC y VIH En Donadores de Sangre En Irapuato, México. Salud Pública México 2003, 45, 690–693. [Google Scholar] [CrossRef]
- Rivera-López, M.R.F. Prevalencia de seropositividad para VIH, hepatitis B y C en donadores de sangre. Gac. Médica México 2004, 140, 657–660. [Google Scholar]
- Monteón, V.M.; Reyes-López, P.A.; Sosa-Palacio, A.; León-Tello, G.; Martínez-Murguía, J.; Sosa-Jurado, F. Distribución heterogénea de la prevalencia de anticuerpos contra Trypanosoma cruzi en donadores de sangre en Puebla, México. Salud Pública México 2005, 47, 116–125. [Google Scholar] [CrossRef]
- García-Montalvo, B.M.; Farfán-Ale, J.A.; Acosta-Viana, K.Y.; Puerto-Manzano, F.I. Hepatitis B Virus DNA in Blood Donors with Anti-HBc as a Possible Indicator of Active Hepatitis B Virus Infection in Yucatan, Mexico. Transfus. Med. 2005, 15, 371–378. [Google Scholar] [CrossRef]
- Chiquete, E.; Sánchez, L.V.; Becerra, G.; Quintero, A.; Maldonado, M.; Panduro, A. Performance of the Serologic and Molecular Screening of Blood Donations for the Hepatitis B and C Viruses in a Mexican Transfusion Center. Ann. Hepatol. 2005, 4, 275–278. [Google Scholar] [CrossRef]
- Vázquez-Flores, J.A.; Valiente-Banuet, L.; Marín y López, R.A.; Sánchez-Guerrero, S.A. La seguridad de las reservas sanguíneas en la República Mexicana durante los años 1999 a 2003. Rev. Investig. Clínica 2006, 58, 101–108. [Google Scholar]
- García-Montalvo, B.M. Seropositivity of HIV, HBV, HCV and Treponema pallidum in blood donors in southeast Mexico. Rev. Investig. Clin. Organo Hosp. Enfermedades Nutr. 2006, 58, 567–572. [Google Scholar]
- Valerio-Ureña, J.; Vásquez-Fernández, F.; Pérez-Sosa, J.A.; Cortazar-Benítez, L.F.; Chávez-Tapia, N.C.; Ruvalcaba-Rojas, O.A.; Torres-Medina, V. Prevalencia de marcadores serológicos de VHB y VHC en donadores de sangre de la ciudad de Veracruz. Gac. Médica México 2009, 145, 183–187. [Google Scholar]
- Contreras, A.M.; Reta, C.B.; Torres, O.; Celis, A.; Domínguez, J. Sangre segura en ausencia de infecciones virales por VHB, VHC y VIH en período de ventana serológica de donadores. Salud Pública México 2011, 53, S13–S18. [Google Scholar]
- Lopez-Balderas, N.; Bravo, E.; Camara, M.; Hernandez-Romano, P. Seroprevalence of Hepatitis Viruses and Risk Factors in Blood Donors of Veracruz, Mexico. J. Infect. Dev. Ctries. 2015, 9, 274–282. [Google Scholar] [CrossRef]
- Sosa-Jurado, F.; Hilda Rosas-Murrieta, N.; Guzman-Flores, B.; Perez Zempoaltecalt, C.; Patricia Sanchez Torres, A.; Ramirez Rosete, L.; Bernal-Soto, M.; Marquez-Dominguez, L.; Melendez-Mena, D.; Angel Mendoza Torres, M.; et al. Prevalence of Serologic Hepatitis B Markers in Blood Donors From Puebla, Mexico: The Association of Relatively High Levels of Anti-Core Antibodies With the Detection of Surface Antigen and Genomic DNA. Hepat. Mon. 2016, 16, e36942. [Google Scholar] [CrossRef]
- Hernández-Romano, P.; Hernández-Romano, J.; Torres-Hernández, R.M.; González-Jiménez, B.; López-Balderas, N. Occult Hepatitis B Infections and Anti-HBc Prevalence at a Resource-Limited Blood Bank in Mexico. Transfus. Med. Oxf. Engl. 2020, 30, 396–400. [Google Scholar] [CrossRef]
- Roman, S.; Panduro, A.; Aguilar-Gutierrez, Y.; Maldonado, M.; Vazquez-Vandyck, M.; Martinez-Lopez, E.; Ruiz-Madrigal, B.; Hernandez-Nazara, Z. A Low Steady HBsAg Seroprevalence Is Associated with a Low Incidence of HBV-Related Liver Cirrhosis and Hepatocellular Carcinoma in Mexico: A Systematic Review. Hepatol. Int. 2009, 3, 343–355. [Google Scholar] [CrossRef] [PubMed]
- Sosa-Jurado, F.; Palencia-Lara, R.; Xicoténcatl-Grijalva, C.; Bernal-Soto, M.; Montiel-Jarquin, Á.; Ibarra-Pichardo, Y.; Rosas-Murrieta, N.H.; Lira, R.; Cortes-Hernandez, P.; Santos-López, G. Donated Blood Screening for HIV, HCV and HBV by ID-NAT and the Residual Risk of Iatrogenic Transmission in a Tertiary Care Hospital Blood Bank in Puebla, Mexico. Viruses 2023, 15, 1331. [Google Scholar] [CrossRef] [PubMed]
- Jose-Abrego, A.; Panduro, A.; Fierro, N.A.; Roman, S. High Prevalence of HBV Infection, Detection of Subgenotypes F1b, A2, and D4, and Differential Risk Factors among Mexican Risk Populations with Low Socioeconomic Status. J. Med. Virol. 2017, 89, 2149–2157. [Google Scholar] [CrossRef] [PubMed]
- Roman, S.; Tanaka, Y.; Khan, A.; Kurbanov, F.; Kato, H.; Mizokami, M.; Panduro, A. Occult Hepatitis B in the Genotype H-Infected Nahuas and Huichol Native Mexican Population. J. Med. Virol. 2010, 82, 1527–1536. [Google Scholar] [CrossRef] [PubMed]
- Porras Nuñez, L.O.; Balderas Avila, R.; Leija Guzmán, M.; Mattar Olivo, C. Core M marcador útil de hepatitis B en pacientes de hemodiálisis. Rev. Mex. Patol. Clínica Med. Lab. 2002, 49, 148–152. [Google Scholar]
- Treviño Hernández, R.; Pérez Ramírez, J.L.; Cruz Valdez, J.; Ramírez, B.; Ortiz, R.; Bosques Padilla, F. Prevalencia de hepatitis C y B en pacientes con insuficiencia renal crónica en programa de hemodiálisis en el Hospital Universitario y Centro Renal de Monterrey. Med. Univ. 2003, 5, 228–232. [Google Scholar]
- Calderon, G.M.; Gonzalez-Velázquez, F.; Gonzalez-Bonilla, C.R.; Novelo-Garza, B.; Terrazas, J.J.; Martínez-Rodríguez, M.L.; Cortés-Márquez, S.R.; Blanco-Flores, J.P.; Rodríguez-Rodríguez, A.; del Campo, M.A.; et al. Prevalence and Risk Factors of Hepatitis C Virus, Hepatitis B Virus, and Human Immunodeficiency Virus in Multiply Transfused Recipients in Mexico. Transfusion 2009, 49, 2200–2207. [Google Scholar] [CrossRef]
- Paniagua, R.; Villasís-Keever, A.; Prado-Uribe, M.D.C.; Ventura-García, M.-J.; Alcántara-Ortega, G.; Ponce de Leon, S.R.; Cure-Bolt, N.; Rangel-Frausto, S. Elevated Prevalence of Hepatitis B in Mexican Hemodialysis Patients. A Multicentric Survey. Arch. Med. Res. 2010, 41, 251–254. [Google Scholar] [CrossRef]
- Alvarado Esquivel, C.; Arreola Valenzuela, M.A.; Mercado Suárez, M.F.; Espinoza Andrade, F. Hepatitis B Virus Infection among Inpatients of a Psychiatric Hospital of Mexico. Clin. Pract. Epidemiol. Ment. Health 2005, 1, 10. [Google Scholar] [CrossRef] [PubMed]
- Alvarado-Esquivel, C.; Arreola-Valenzuela, M.A.; Rodríguez-Briones, A.; Alanís-Quiñones, O.P.; Estrada-Martínez, S.; Luevanos-Becerra, C.; Martínez-Saenz, L.F.; Martínez-García, S.A.; Ramírez-Valles, E.G.; Ibarra-Torres, I.; et al. Seroprevalence of Selected Viral, Bacterial and Parasitic Infections among Inpatients of a Public Psychiatric Hospital of Mexico. Rev. Inst. Med. Trop. Sao Paulo 2008, 50, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Aguirre-Garcia, J.; Velasco-Aviles, F.; Stoopen, M.-; Landa, L.; Sepulveda, B. Lesiones Hepáticas En Portadores Asintomticos al Antígeno Superficial Del Virus de La Hepatitis V (VHB). Gac. Med. Mex. 1976, 112, 375–381. [Google Scholar] [PubMed]
- Góngora-Biachi, R.A.; Castro-Sansores, C.J.; González-Martínez, P.; Lara-Perera, D.M.; Garrido-Palma, J.; Lara-Perera, V. Frequency of Antibodies against the Hepatitis C Virus in Patients with Hepatic Cirrhosis in Yucatan, Mexico. Salud Pública México 2003, 45, 346–350. [Google Scholar] [CrossRef]
- Méndez-Sánchez, N.; Aguilar-Ramírez, J.R.; Reyes, A.; Dehesa, M.; Juárez, A.; Castañeda, B.; Sánchez-Avila, F.; Poo, J.L.; Guevara González, L.; Lizardi, J.; et al. Etiology of Liver Cirrhosis in Mexico. Ann. Hepatol. 2004, 3, 30–33. [Google Scholar] [CrossRef]
- Abdo-Francis, M.; Torre, A.; Tenorio, C.; Ornelas, E.; Villasis, A. Prevalencia de La Hepatitis Por Virus B En Pacientes Con Cirrosis En México. Rev. Medica Hosp. Gen. Mex. 2011, 74, 16–20. [Google Scholar]
- Juárez-Figueroa, L.A.; Uribe-Salas, F.J.; Conde-Glez, C.J.; Hernández-Avila, M.; Hernández-Nevárez, P.; Uribe-Zúñiga, P.; Del Río-Chiriboga, C. Hepatitis B Markers in Men Seeking Human Immunodeficiency Virus Antibody Testing in Mexico City. Sex. Transm. Dis. 1997, 24, 211. [Google Scholar] [CrossRef]
- Torres-Baranda, R.; Bastidas-Ramírez, B.E.; Maldonado-González, M.; Sánchez-Orozco, L.V.; Vázquez-Vals, E.; Rodríguez-Noriega, E.; Panduro, A. Occult Hepatitis B in Mexican Patients with HIV, an Analysis Using Nested Polymerase Chain Reaction. Ann. Hepatol. 2006, 5, 34–40. [Google Scholar] [CrossRef]
- Segoviano-Mendoza, G.; Torres-Erazo, D.S.; Tovar-Serrano, A. Coinfección con virus de hepatitis B o C en pacientes infectados por VIH. Med. Interna México 2014, 30, 365–372. [Google Scholar]
- Alvarez-Muñoz, M.T.; Maldonado-Rodriguez, A.; Rojas-Montes, O.; Torres-Ibarra, R.; Gutierrez-Escolano, F.; Vazquez-Rosales, G.; Gomez, A.; Muñoz, O.; Torres, J.; Lira, R. Occult Hepatitis B Virus Infection among Mexican Human Immunodeficiency Virus-1-Infected Patients. World J. Gastroenterol. 2014, 20, 13530–13537. [Google Scholar] [CrossRef]
- Juárez-Figueroa, L.A.; Uribe-Salas, F.J.; González-Rodríguez, A.; Iracheta-Hernández, P.; Ruiz-González, V.; Medina-Islas, Y. Evaluation of HIV, STI and CD4 Results among Voluntary Attendees at the HIV/AIDS Program of Mexico City. Salud Publica Mex. 2017, 59, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Enriquez-Navarro, K.; Maldonado-Rodriguez, A.; Rojas-Montes, O.; Torres-Ibarra, R.; Bucio-Ortiz, L.; De la Cruz, M.A.; Torres-Flores, J.; Xoconostle-Cazares, B.; Lira, R. Identification of Mutations in the S Gene of Hepatitis B Virus in HIV Positive Mexican Patients with Occult Hepatitis B Virus Infection. Ann. Hepatol. 2020, 19, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Saitta, C.; Pollicino, T.; Raimondo, G. Occult Hepatitis B Virus Infection: An Update. Viruses 2022, 14, 1504. [Google Scholar] [CrossRef] [PubMed]
- Yip, T.C.-F.; Wong, G.L.-H. Current Knowledge of Occult Hepatitis B Infection and Clinical Implications. Semin. Liver Dis. 2019, 39, 249–260. [Google Scholar] [CrossRef]
- García-Montalvo, B.M.; Ventura-Zapata, L.P. Molecular and Serological Characterization of Occult Hepatitis B Infection in Blood Donors from Mexico. Ann. Hepatol. 2011, 10, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Escobedo-Melendez, G.; Panduro, A.; Fierro, N.A.; Roman, S. High Prevalence of Occult Hepatitis B Virus Genotype H Infection among Children with Clinical Hepatitis in West Mexico. Mem. Inst. Oswaldo Cruz 2014, 109, 728–737. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Galindo, D.A.; Galván-Ramírez, M.D.l.L.; Andrade-Sierra, J.; González-Espinoza, E.; Evangelista-Carrillo, L.A.; Mendoza-Cabrera, S.; Rodríguez-Pérez, L.R.; Chiquete, E.; Armendáriz-Borunda, J.; Sánchez-Orozco, L.V. Occult Hepatitis B in Kidney Transplants Recipients and Donors from Western Mexico. Int. J. Infect. Dis. 2020, 91, 17–21. [Google Scholar] [CrossRef]
- Conners, E.E. Screening and Testing for Hepatitis B Virus Infection: CDC Recommendations—United States, 2023. MMWR Recomm. Rep. 2023, 72, 1–25. [Google Scholar] [CrossRef]
- Sepulveda Amor, J.; Garcia Garcia, M.L.D.L.; Dominguez Torix, J.L.; Valdespino Gomez, J.L. Prevencion de la Transmisión Sanguínea del VIH. La Experiencia Mexicana. Bol. Sanit. Panam. 1988, 105, 605–614. [Google Scholar]
- Rojo Medina, J. El Centro Nacional de La Transfusión Sanguínea. Rev. Med. Hosp. Gen. Mex. 2010, 73, 209–210. [Google Scholar]
- DOF-Diario Oficial de La Federación. Available online: https://dof.gob.mx/nota_detalle.php?codigo=4810828&fecha=08/12/1993#gsc.tab=0 (accessed on 11 September 2023).
- Escobedo-Melendez, G.; Panduro, A.; Celis, A.; Roman, S. Risk Factors Associated with Horizontal Transmission of Hepatitis B Viral Infection from Parents to Children in Mexico. J. Infect. Dev. Ctries. 2019, 13, 44–49. [Google Scholar] [CrossRef]
- Alvarez-Muñoz, M.T.; Vázquez-Rosales, J.G.; Bustamante-Calvillo, M.E.; Del Rey-Pineda, G.; Arredondo-Garcia, J.L.; Muñoz, O. Prevalencia de marcadores serológicos para los virus B y C de la hepatitis en una cohorte de mujeres embarazadas del Valle de México. Bol. Med. Hosp. Infant. Mex. 1995, 52, 143–147. [Google Scholar]
- Ortiz, F.J.; Figueroa, R.; Lara, J.; Arredondo, J.L.; Ahued, J.R. Prevalencia de marcadores serológicosde los virus de la hepatitis A B C y D. Salud Pública México 1996, 38, 317–322. [Google Scholar]
- Hernández Arriaga, J.L.; Ramirez-Crespo, A.; de Anda-Gómez, M.; Castellanos-Martinez, J. Marcadores serológicos de hepátitis B en la etapa perinatal. Bol. Med. Hosp. Infant. Mex. 2000, 57, 682–685. [Google Scholar]
- Vázquez-Martínez, J.L.; Coreño-Juárez, M.O.; Montaño-Estrada, L.F.; Attlan, M.; Gómez-Dantés, H. Seroprevalence of Hepatitis B in Pregnant Women in Mexico. Salud Publica Mex. 2003, 45, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Berrones, M.Á. Detección de la prevalencia de antígeno de superficie para hepatitis B en mujeres embarazadas. Rev. Espec. Médico-Quirúrgicas 2015, 20, 54–59. [Google Scholar]
- Rivas-Estilla, A.M.; Sanchez, L.V.; Matsui, O.; Campollo, O.; Armendariz-Borunda, J.; Segura-Ortega, J.E.; Panduro, A. Identification of Hepatitis C Virus (HCV) Genotypes Patients from West of Mexico. Hepatol. Res. 1998, 12, 121130. [Google Scholar]
- Rivas-Estilla, A.M.; Cordero-Pérez, P.; del Carmen Trujillo-Murillo, K.; Ramos-Jiménez, J.; Chen-López, C.; de L. Garza-Rodríguez, M.; Ramírez-Gutiérrez, Á.; Muñoz-Espinosa, L. Genotyping of Hepatitis C Virus (HCV) in Infected Patients from Northeast Mexico: Original Article. Ann. Hepatol. 2008, 7, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Panduro, A.; Roman, S.; Khan, A.; Tanaka, Y.; Kurbanov, F.; Martinez-Lopez, E.; Campollo, O.; Hernandez-Nazara, Z.; Mizokami, M. Molecular Epidemiology of Hepatitis C Virus Genotypes in West Mexico. Virus Res. 2010, 151, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Espinosa, L.E.; Trujillo-Trujillo, M.E.; Martínez-Macías, R.F.; Panduro, A.; Rivas-Estilla, A.M.; Fierro, N.A.; Silvera-Linares, A.L.; Torres-Valadez, R.; Cordero-Pérez, P.; González-Aldaco, K.; et al. Increase of Drug Use and Genotype 3 in HCV-Infected Patients from Central West and Northeast Mexico. Ann. Hepatol. 2015, 14, 642–651. [Google Scholar] [CrossRef]
- Sedeño-Monge, V.; Laguna-Meraz, S.; Santos-López, G.; Panduro, A.; Sosa-Jurado, F.; Jose-Abrego, A.; Meléndez-Mena, D.; Muñoz-Ramírez, M.A.; Cosme-Chávez, M.; Roman, S. A Comprehensive Update of the Status of Hepatitis C Virus (HCV) Infection in Mexico—A Systematic Review and Meta-Analysis (2008–2019). Ann. Hepatol. 2021, 20, 100292. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, L.V.; Maldonado, M.; Bastidas-Ramírez, B.E.; Norder, H.; Panduro, A. Genotypes and S-Gene Variability of Mexican Hepatitis B Virus Strains: Mexican Hepatitis B Virus Strains. J. Med. Virol. 2002, 68, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Arauz-Ruiz, P.; Norder, H.; Robertson, B.H.; Magnius, L.O. Genotype H: A New Amerindian Genotype of Hepatitis B Virus Revealed in Central America. J. Gen. Virol. 2002, 83, 2059–2073. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Gish, R.G.; Bzowej, N.; Newsom, M.; Sugauchi, F.; Tanaka, Y.; Kato, T.; Orito, E.; Usuda, S.; Ueda, R.; et al. Eight Genotypes (A-H) of Hepatitis B Virus Infecting Patients from San Francisco and Their Demographic, Clinical, and Virological Characteristics. J. Med. Virol. 2004, 73, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Fujiwara, K.; Gish, R.G.; Sakugawa, H.; Yoshizawa, H.; Sugauchi, F.; Orito, E.; Ueda, R.; Tanaka, Y.; Kato, T.; et al. Classifying Genotype F of Hepatitis B Virus into F1 and F2 Subtypes. World J. Gastroenterol. WJG 2005, 11, 6295–6304. [Google Scholar] [CrossRef] [PubMed]
- Alvarado-Esquivel, C.; Sablon, E.; Conde-González, C.J.; Juárez-Figueroa, L.; Ruiz-Maya, L.; Aguilar-Benavides, S. Molecular Analysis of Hepatitis B Virus Isolates in Mexico: Predominant Circulation of Hepatitis B Virus Genotype H. World J. Gastroenterol. WJG 2006, 12, 6540–6545. [Google Scholar] [CrossRef]
- Nakajima, A.; Usui, M.; Huy, T.T.T.; Hlaing, N.K.T.; Masaki, N.; Sata, T.; Abe, K. Full-Length Sequence of Hepatitis B Virus Belonging to Genotype H Identified in a Japanese Patient with Chronic Hepatitis. Jpn. J. Infect. Dis. 2005, 58, 244–246. [Google Scholar]
- Ohnuma, H.; Yoshikawa, A.; Mizoguchi, H.; Okamoto, H.; The Jrc Nat Screening Research Group. Characterization of Genotype H Hepatitis B Virus Strain Identified for the First Time from a Japanese Blood Donor by Nucleic Acid Amplification Test. J. Gen. Virol. 2005, 86, 595–599. [Google Scholar] [CrossRef]
- Kumagai, I.; Abe, K.; Oikawa, T.; Sato, A.; Sato, S.; Endo, R.; Takikawa, Y.; Suzuki, K.; Masuda, T.; Sainokami, S.; et al. A Male Patient with Severe Acute Hepatitis Who Was Domestically Infected with a Genotype H Hepatitis B Virus in Iwate, Japan. J. Gastroenterol. 2007, 42, 168–175. [Google Scholar] [CrossRef]
- Sánchez, L.V.; Tanaka, Y.; Maldonado, M.; Mizokami, M.; Panduro, A. Difference of Hepatitis B Virus Genotype Distribution in Two Groups of Mexican Patients with Different Risk Factors: High Prevalence of Genotype H and G. Intervirology 2006, 50, 9–15. [Google Scholar] [CrossRef]
- Roman, S.; Jose-Abrego, A.; Fierro, N.A.; Escobedo-Melendez, G.; Ojeda-Granados, C.; Martinez-Lopez, E.; Panduro, A. Hepatitis B Virus Infection in Latin America: A Genomic Medicine Approach. World J. Gastroenterol. 2014, 20, 7181–7196. [Google Scholar] [CrossRef] [PubMed]
- Glebe, D.; Goldmann, N.; Lauber, C.; Seitz, S. HBV Evolution and Genetic Variability: Impact on Prevention, Treatment and Development of Antivirals. Antiviral Res. 2021, 186, 104973. [Google Scholar] [CrossRef]
- Wolf, J.M.; Pereira, V.R.Z.B.; Simon, D.; Lunge, V.R. Evolutionary History of Hepatitis B Virus Genotype H. J. Med. Virol. 2021, 93, 4004–4009. [Google Scholar] [CrossRef] [PubMed]
- Jose-Abrego, A.; Roman, S.; Laguna-Meraz, S.; Rebello-Pinho, J.R.; Justo Arevalo, S.; Panduro, A. Tracing the Evolutionary History of Hepatitis B Virus Genotype H Endemic to Mexico. Front. Microbiol. 2023, 14, 1180931. [Google Scholar] [CrossRef] [PubMed]
- Jose-Abrego, A.; Roman, S.; Laguna-Meraz, S.; Panduro, A. Host and HBV Interactions and Their Potential Impact on Clinical Outcomes. Pathogens 2023, 12, 1146. [Google Scholar] [CrossRef]
- Fernández-Galindo, D.A.; Sánchez-Ávila, F.; Bobadilla-Morales, L.; Gómez-Quiróz, P.; Bueno-Topete, M.; Armendáriz-Borunda, J.; Sánchez-Orozco, L.V. New Amino Acid Changes in Drug Resistance Sites and HBsAg in Hepatitis B Virus Genotype H: RT and HBsAg Mutations in HBV Genotype H. J. Med. Virol. 2015, 87, 985–992. [Google Scholar] [CrossRef]
- Jose-Abrego, A.; Roman, S.; Pinho, J.R.R.; Gomes-Gouvêa, M.S.; Panduro, A. High Frequency of Antiviral Resistance Mutations in HBV Genotypes A2 and H: Multidrug Resistance Strains in Mexico. J. Clin. Transl. Hepatol. 2023, 11, 1023–1034. [Google Scholar] [CrossRef]
- Servin-Rojas, M.; Olivas-Martinez, A.; Toapanta-Yanchapaxi, L.; García-Juárez, I. Liver Transplantation in Mexico. Clin. Liver Dis. 2022, 19, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Torres-Valadez, R.; Roman, S.; Jose-Abrego, A.; Sepulveda-Villegas, M.; Ojeda-Granados, C.; Rivera-Iñiguez, I.; Panduro, A. Early Detection of Liver Damage in Mexican Patients with Chronic Liver Disease. J. Transl. Intern. Med. 2017, 5, 49–57. [Google Scholar] [CrossRef]
- Laguna-Meraz, S.; Roman, S.; Jose-Abrego, A.; Sigala-Arellano, R.; Panduro, A. A Hospital-Based Study of the Prevalence of HBV, HCV, HIV, and Liver Disease among a Low-Income Population in West Mexico. Ann. Hepatol. 2022, 27, 100579. [Google Scholar] [CrossRef]
- Gomez-Quiroz, L.E.; Roman, S. Influence of Genetic and Environmental Risk Factors in the Development of Hepatocellular Carcinoma in Mexico. Ann. Hepatol. 2022, 27, 100649. [Google Scholar] [CrossRef]
- Cisneros-Garza, L.E.; González-Huezo, M.S.; López-Cossio, J.A.; Kuljacha-Gastelum, A.L. Caracterización del carcinoma hepatocelular en México. Rev. Gastroenterol. México 2018, 83, 223–227. [Google Scholar] [CrossRef]
- Oba, U.; Koga, Y.; Hoshina, T.; Suminoe, A.; Abe, K.; Hayashida, M.; Taguchi, T.; Hara, T. An Adolescent Female Having Hepatocellular Carcinoma Associated with Hepatitis B Virus Genotype H with a Deletion Mutation in the Pre-S2 Region. J. Infect. Chemother. 2015, 21, 302–304. [Google Scholar] [CrossRef]
- Pattyn, J.; Hendrickx, G.; Vorsters, A.; Van Damme, P. Hepatitis B Vaccines. J. Infect. Dis. 2021, 224, S343–S351. [Google Scholar] [CrossRef] [PubMed]
- Shepard, C.W.; Simard, E.P.; Finelli, L.; Fiore, A.E.; Bell, B.P. Hepatitis B Virus Infection: Epidemiology and Vaccination. Epidemiol. Rev. 2006, 28, 112–125. [Google Scholar] [CrossRef]
- Historia y avances de la vacunación en Mexico. Available online: https://www.gob.mx/cms/uploads/attachment/file/400159/Varios_-_Historia_y_avances_de_la_vacunaci_n_en_M_xico.pdf (accessed on 20 October 2023).
- Flores-Sánchez, L.; Paredes-Solís, S.; Balanzar-Martínez, A.; Flores-Moreno, M.; Legorreta-Soberanis, J.; Andersson, N. Hepatitis B vaccination coverage and associated factor for vaccine acceptance: A cross-sectional study in health workers of the Acapulco General Hospital, Mexico. Gac. Med. Mex. 2014, 150, 395–402. [Google Scholar]
- Mongua-Rodríguez, N.; Huberttuber, C.; Ferreira-Guerrero, E.; de Castro, F.; Ferreyra-Reyes, L.; Villalobos-Hernández, A.; Cruz-Hervert, P.; Delgado-Sánchez, G.; Díaz-Ortega, J.L.; Romero-Martínez, M.; et al. Trends in vaccination coverage among children aged 12–23 and 24–35 months in Mexico. Ensanut 2012 and Ensanut 100k. Salud Publica Mex. 2019, 61, 809–820. [Google Scholar] [CrossRef]
- Mongua-Rodríguez, N.; Delgado-Sánchez, G.; Ferreira-Guerrero, E.; Ferreyra-Reyes, L.; Martínez-Hernández, M.; Canizales-Quintero, S.; Téllez-Vázquez, N.A.; García-García, L. Cobertura de vacunación en niños, niñas y adolescentes en México. Salud Pública México 2023, 65, s23–s33. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Tanaka, Y. Cross-Protection of Hepatitis B Vaccination among Different Genotypes. Vaccines 2020, 8, 456. [Google Scholar] [CrossRef]
- Cassidy, A.; Mossman, S.; Olivieri, A.; De Ridder, M.; Leroux-Roels, G. Hepatitis B Vaccine Effectiveness in the Face of Global HBV Genotype Diversity. Expert Rev. Vaccines 2011, 10, 1709–1715. [Google Scholar] [CrossRef] [PubMed]
- A Roadmap for Serum Biomarkers for Hepatitis B Virus: Current Status and Future Outlook | Nature Reviews Gastroenterology & Hepatology. Available online: https://www.nature.com/articles/s41575-022-00649-z (accessed on 23 October 2023).
- Programa de Vacunacion Universal, Secretaria de Salud, Mexico. Lineamientos Generales. Available online: https://www.gob.mx/cms/uploads/attachment/file/790120/LineamientosGeneralesPVU_2023.pdf (accessed on 20 October 2023).
- Fierro, N.A.; Roman, S.; Realpe, M.; Hernandez-Nazara, Z.; Zepeda-Carrillo, E.A.; Panduro, A. Multiple Cytokine Expression Profiles Reveal Immune-Based Differences in Occult Hepatitis B Genotype H-Infected Mexican Nahua Patients. Mem. Inst. Oswaldo Cruz 2011, 106, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- Scheiblauer, H.; El-Nageh, M.; Diaz, S.; Nick, S.; Zeichhardt, H.; Grunert, H.-P.; Prince, A. Performance Evaluation of 70 Hepatitis B Virus (HBV) Surface Antigen (HBsAg) Assays from around the World by a Geographically Diverse Panel with an Array of HBV Genotypes and HBsAg Subtypes. Vox Sang. 2010, 98, 403–414. [Google Scholar] [CrossRef]
- Lou, S.; Taylor, R.; Pearce, S.; Kuhns, M.; Leary, T. An Ultra-Sensitive Abbott ARCHITECT® Assay for the Detection of Hepatitis B Virus Surface Antigen (HBsAg). J. Clin. Virol. 2018, 105, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, D.E.; Seiz, P.L.; Schüttler, C.G.; Gerlich, W.H.; Glebe, D.; Scheiblauer, H.; Nick, S.; Chudy, M.; Dougall, T.; Stone, L.; et al. International Collaborative Study on the 3rd WHO International Standard for Hepatitis B Surface Antigen. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2016, 82, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Cárdenas-Perea, M.E.; Gómez-Conde, E.; Santos-López, G.; Pérez-Contreras, I.; Díaz-Orea, M.A.; Gándara-Ramírez, J.L.; Cruz Y López, O.R.; Márquez-Domínguez, L.; Sosa-Jurado, F. Hepatitis B Surface Antibodies in Medical Students from a Public University in Puebla, Mexico. Hum. Vaccines Immunother. 2016, 12, 1857–1862. [Google Scholar] [CrossRef]
- Flores-Castañeda, M.S.; Garcia-Méndez, B.L.; Tijerina-Menchaca, R. Seropositividad de La Infección Por HVC y HVB En Estudiantes Universitarios Del Estado de Nuevo León, México. Rev. Gastroenterol. Mex. 1996, 61, 327–331. [Google Scholar]
- Mercado, U.; Avendaño-Reyes, M.; Araiza-Casillas, R.; Díaz-Molina, R. Prevalencia de anticuerpos contra virus de hepatitis C y B en pacientes con lupus eritematoso sistémico. Rev. Gastroenterol. México 2005, 70, 399–401. [Google Scholar]
- Villasís-Keever, M.A.; Peña, L.A.; Miranda-Novales, G.; Alvarez y Muñoz, T.; Damasio-Santana, L.; López-Fuentes, G.; Girón-Carrillo, J.L. Prevalence of Serological Markers against Measles, Rubella, Varicella, Hepatitis B, Hepatitis C, and Human Immunodeficiency Virus among Medical Residents in Mexico. Prev. Med. 2001, 32, 424–428. [Google Scholar] [CrossRef]
- Méndez-Sánchez, N.; Motola-Kuba, D.; Zamora-Valdés, D.; Sánchez-Lara, K.; Ponciano-Rodríguez, G.; Uribe-Ramos, M.H.; Vásquez-Fernández, F.; Lezama-Mora, J.; Pérez-Sosa, J.A.; Baptista-González, H.A.; et al. Risk Factors and Prevalence of Hepatitis Virus B and C Serum Markers among Nurses at a Tertiary-Care Hospital in Mexico City, Mexico: A Descriptive Study. Ann. Hepatol. 2006, 5, 276–280. [Google Scholar] [CrossRef]
- González Huezo, M.S.; Sánchez-Hernández, E.; Camacho, M.C.; Rebollo-Vargas, J. Prevalencia de marcadores positivos para hepatitis B (Ags-VHB) y hepatitis C (Anti-VHC) en personal de salud del ISSEMYM. Rev. Gastroenterol. Mex. 2010, 75, 293–298. [Google Scholar] [PubMed]
- Hyams, K.C.; Escamilla, J.; Romero, R.L.; Alvarado, E.M.; Giraldo, N.B.; Papadimos, T.J.; Martinez, C.R.; Gonzalez, P.G. Hepatitis B Infection in a Non-Drug Abusing Prostitute Population in Mexico. Scand. J. Infect. Dis. 1990, 22, 527–531. [Google Scholar] [CrossRef] [PubMed]
- Gomez, J.L.V.; Garcia, M.D.L.G.; del Rio Chiribo, C.; Palacio, C.C.; Loo-Mendez, E.; Sotelo, A.L. Las Enfermedades de Trasmision Sexual y La Epidemia de VIH/SIDA. Salud Publica Mex. 1995, 37, 549–555. [Google Scholar]
- Hernández-Girón, C.; Uribe-Salas, F.; Conde-González, C.; Cruz Valdez, J.; Juarez-Figueroa, L.; Uribe-Zuñiga, P.; del Río-Chiriboga, C.; Hernández-Avila, M. Seroprevalencias a diversos virus y características sociodemográficas en mujeres que buscan detectarse VIH. Rev. Investig. Clin. 1997, 49, 5–13. [Google Scholar]
- Juárez-Figueroa, L.; Uribe-Salas, F.; Conde-Glez, C.; Hernández-Avila, M.; Olamendi-Portugal, M.; Uribe-Zúñiga, P.; Calderón, E. Low Prevalence of Hepatitis B Markers among Mexican Female Sex Workers. Sex. Transm. Infect. 1998, 74, 448–450. [Google Scholar] [CrossRef] [PubMed]
- Uribe-Salas, F.; Conde-Glez, C.J.; Juárez-Figueroa, L.; Hernández-Castellanos, A. Sociodemographic Dynamics and Sexually Transmitted Infections in Female Sex Workers at the Mexican–Guatemalan Border. Sex. Transm. Dis. 2003, 30, 266–271. [Google Scholar] [CrossRef]
- Ganley, K.Y.; Wilson-Barthes, M.; Zullo, A.R.; Sosa-Rubí, S.G.; Conde-Glez, C.J.; García-Cisneros, S.; Lurie, M.N.; Marshall, B.D.L.; Operario, D.; Mayer, K.H.; et al. Incidence and Time-Varying Predictors of HIV and Sexually Transmitted Infections among Male Sex Workers in Mexico City. Infect. Dis. Poverty 2021, 10, 7. [Google Scholar] [CrossRef]
- Uribe-Salas, F.; Hernández-Avila, M.; Juarez-Figueroa, L.; Conde-Glez, C.J.; Uribe-Zuñiga, P. Risk Factors for Herpes Simplex Virus Type 2 Infection among Female Commercial Sex Workers in Mexico City. Int. J. STD AIDS 1999, 10, 105–111. [Google Scholar] [CrossRef]
- Juárez-Figueroa, L.A.; Uribe-Salas, F.J.; Conde-González, C.J.; Sánchez-Alemán, M.Á. Marcadores serológicos de hepatitis B y C, y VIH en La Calera y Cuambio, Guerrero, México. Salud Pública México 2011, 53, S32–S36. [Google Scholar]
- Cisneros-Castolo, M.; Hernández-Ruiz, L.; Ibarra-Robles, I.E.; Fernández-Gárate, R.H.; Escobedo-De La Peña, J. Prevalence of Hepatitis B Virus Infection and Related Risk Factors in a Rural Community of Mexico. Am. J. Trop. Med. Hyg. 2001, 65, 759–763. [Google Scholar] [CrossRef]
- Baptista-González, H.A.; Kourchenko-Raab, H.; Rosenfeld-Mann, F.; Rizo-Almenara, S.; Peñuela-Olaya, M.A. Estudio de infecciones virales en el lactante menor transfundido en la etapa neonatal. Bol. Med. Hosp. Infant. Mex. 1998, 55, 385–392. [Google Scholar]
- Escobedo-Meléndez, G.; Fierro, N.A.; Roman, S.; Maldonado-González, M.; Zepeda-Carrillo, E.; Panduro, A. Prevalence of Hepatitis A, B and C Serological Markers in Children from Western Mexico. Ann. Hepatol. 2012, 11, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Kato-Maeda, M.; Ponce-de-León, S.; Sifuentes-Osornio, J.; Rangel-Frausto, M.S.; Calva-Mercado, J.; Infante-Surez, L.; Villareal, F.M.; Ponce-de-León, S. Bloodborne Viral Infections in Patients Attending an Emergency Room in Mexico City: Estimate of Seroconversion Probability in Healthcare Workers after an Occupational Exposure. Infect. Control Hosp. Epidemiol. 2000, 21, 600–602. [Google Scholar] [CrossRef] [PubMed]








| Study Population |
Subjects (N) |
Antigen + n (%) |
Antibody + n (%) |
Diagnostic Technique | Year/Ref. |
|---|---|---|---|---|---|
| Professional blood donors | 4196 | 28 (0.66) (AAH) | 7 (0.16) | IEP | 1971/[47] |
| Professional blood donors Voluntary blood donors | 551 594 | 11 (2.0) 0 (0.0) | - - | CF | 1971/[47,48] |
| Children with high values of liver function tests Children with lymphomas/ Leukemias | - - | 5.7% 11.7% | - - | ID | 1972/[49] |
| General population Netzahualcoyotl City, Mexico State San Angel, Mexico City | 19,249 | 0.29% - - | 6.38% 7.48% 3.91% | IEP | 1976/[50] |
| Healthcare workers Non-healthcare workers | 545 500 | 143 (26.4) 72 (14.4) | - | RIA | 1984/[51] |
| Patients with acute hepatitis | 222 | 11(5.0) | - | RIA | 1987/[52] |
| Subpopulations * |
Inhabitants (N) | HBsAg Prevalence ** (%) |
Inhabitants (N) |
Anti-HBc Prevalence ** (%) |
Inhabitants (N) |
|---|---|---|---|---|---|
| Middle/High Income | 51,782,209 | 0.46 | 238,198 | 1.43 | 740,485 |
| Low income | 51,717,710 | 1.03 | 532,692 | 20.89 | 10,803,829 |
| Native Mexicans | 23,200,000 | 7.99 | 1,853,680 | 13.88 | 3,220,160 |
| Total | 126,699,919 | 2,624,570 | 14,764,474 |
| Study Groups |
Studies (N) |
Prevalence OBI % (95% CI) |
Prevalence Anti-HBc % (95% Cl) | Reference |
|---|---|---|---|---|
| HIV/AIDS | 3 | 34.30 (19.76–52.52) | 22.26 (15.67–30.61) | [91,93,95] |
| Native population | 1 | 14.19 (10.62–18.70) | 32.67 (27.66–38.13) | [79] |
| Children | 1 | 11.16 (2.30–22.0) | 9.5 (6.08–13.98) | [99] |
| Transplanted patients | 1 | 2.74 (0.69–10.30) | 0 (0.04–9.89) | [100] |
| Blood Donors | 4 | 2.50 (2.30–22.0) | 1.45 (1.10–1.91) | [67,74,75,98] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panduro, A.; Roman, S.; Laguna-Meraz, S.; Jose-Abrego, A. Hepatitis B Virus Genotype H: Epidemiological, Molecular, and Clinical Characteristics in Mexico. Viruses 2023, 15, 2186. https://doi.org/10.3390/v15112186
Panduro A, Roman S, Laguna-Meraz S, Jose-Abrego A. Hepatitis B Virus Genotype H: Epidemiological, Molecular, and Clinical Characteristics in Mexico. Viruses. 2023; 15(11):2186. https://doi.org/10.3390/v15112186
Chicago/Turabian StylePanduro, Arturo, Sonia Roman, Saul Laguna-Meraz, and Alexis Jose-Abrego. 2023. "Hepatitis B Virus Genotype H: Epidemiological, Molecular, and Clinical Characteristics in Mexico" Viruses 15, no. 11: 2186. https://doi.org/10.3390/v15112186