
Serum Angiopoietin-2 Predicts the Occurrence and Recurrence of Hepatocellular Carcinoma after Direct-Acting Antiviral Therapy for Hepatitis C
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analyses
3. Results
3.1. Baseline Patient Characteristics
3.2. Baseline Factors Associated with HCC Occurrence after Successful HCV Eradication by DAAs
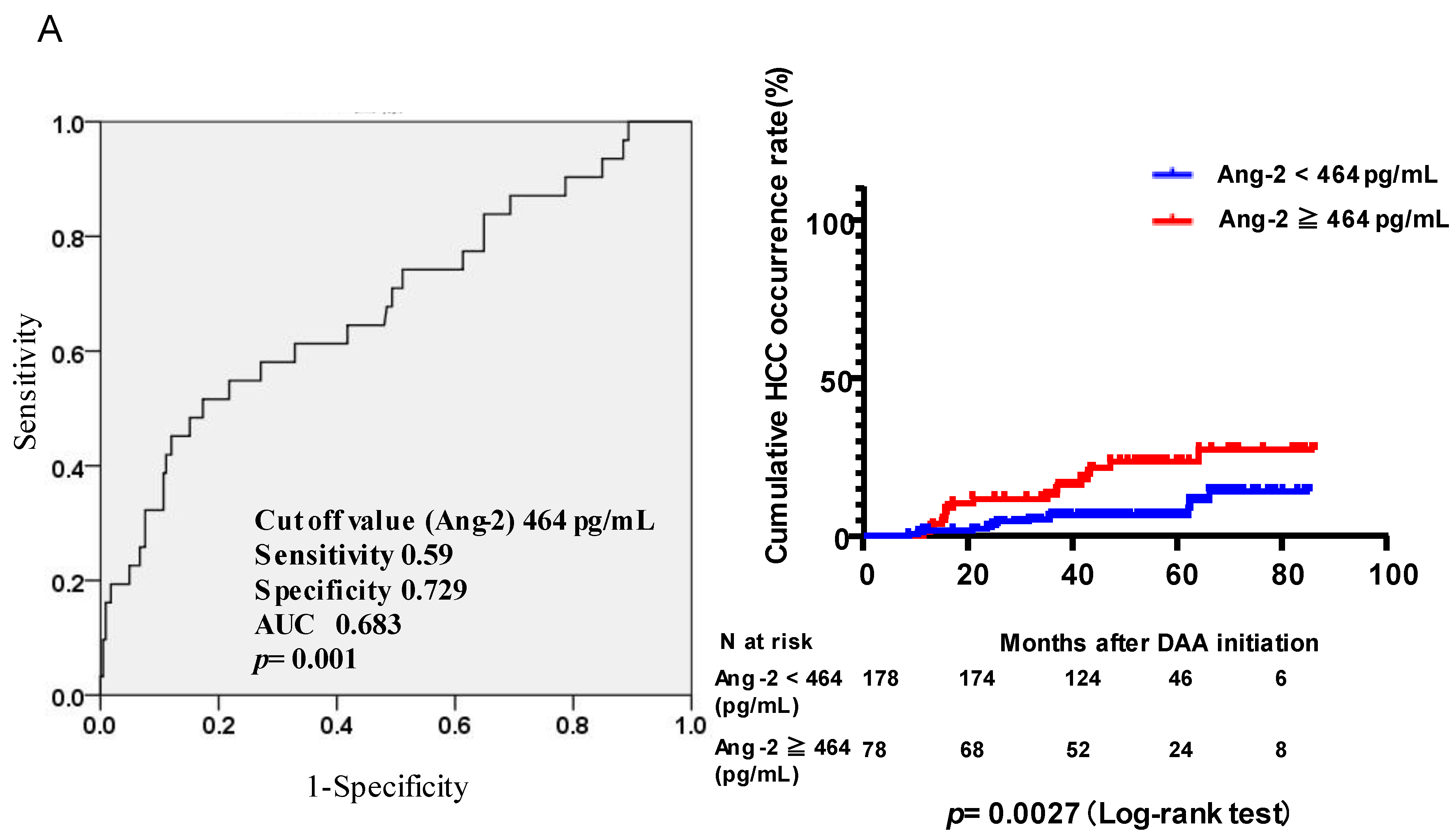
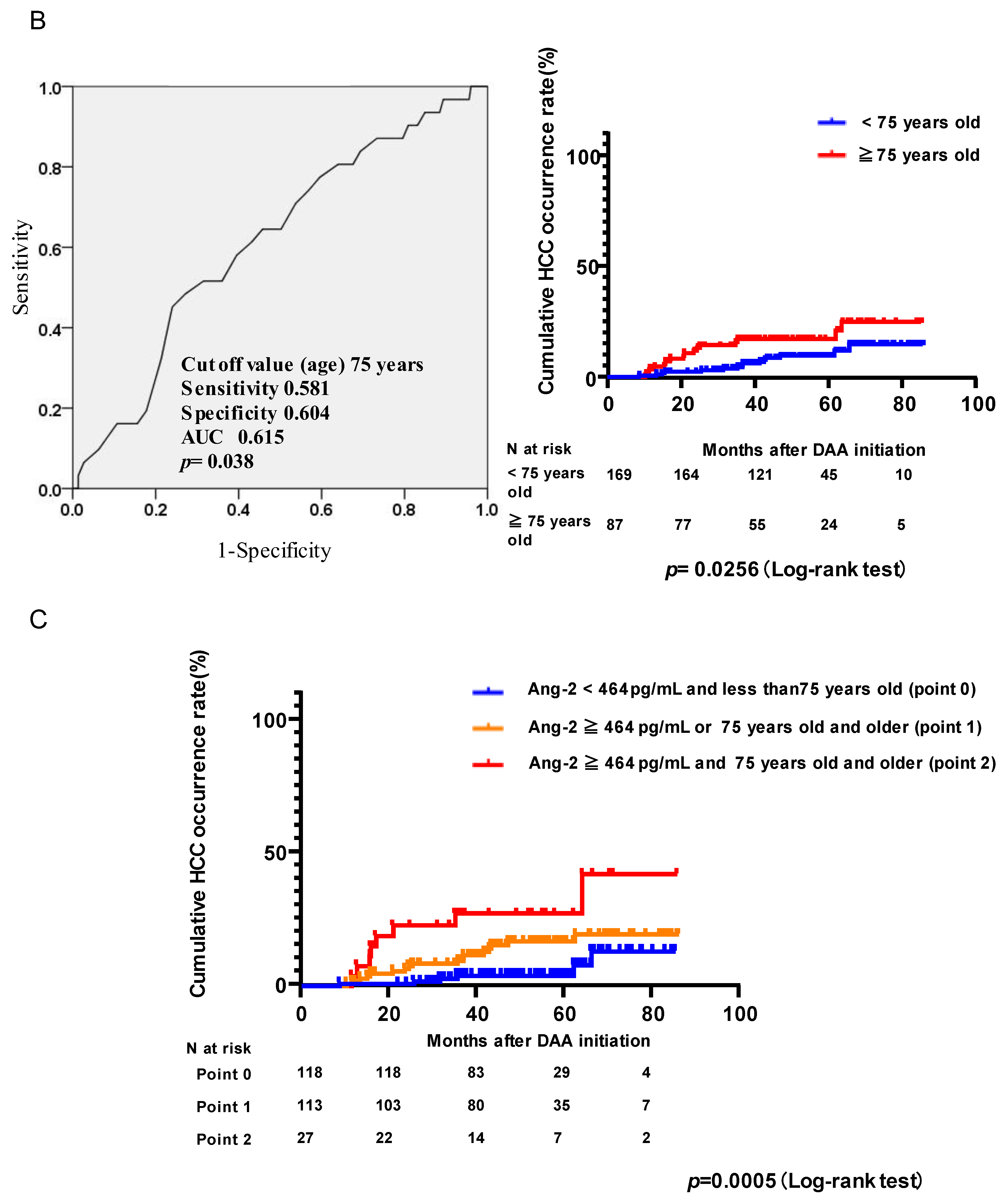
3.3. Risk of HCC Occurrence after Successful HCV Eradication by DAAs According to Serum Ang2 Levels and Age
3.4. Factors at the End of Treatment Associated with HCC Occurrence after Successful HCV Eradication by DAAs
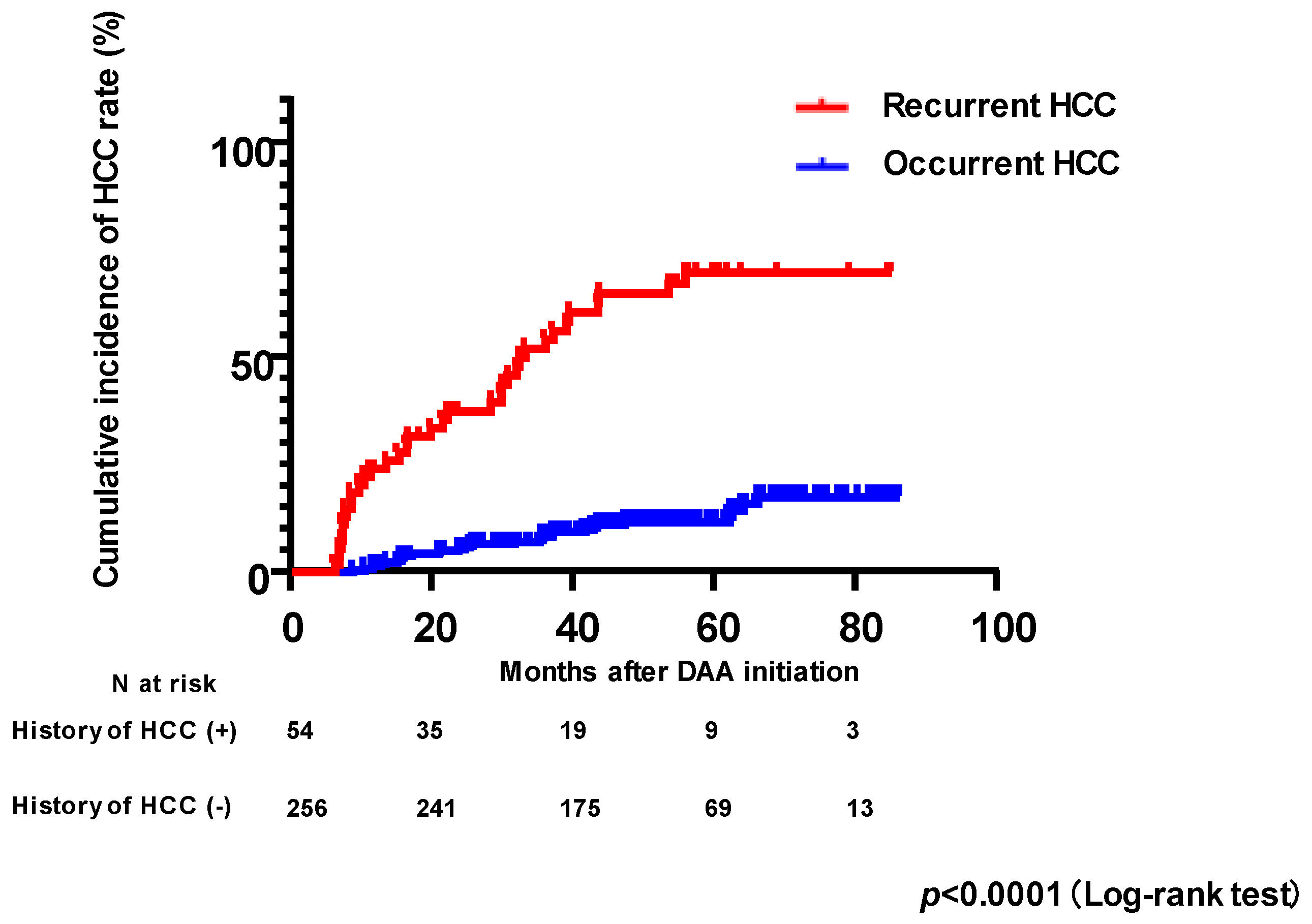
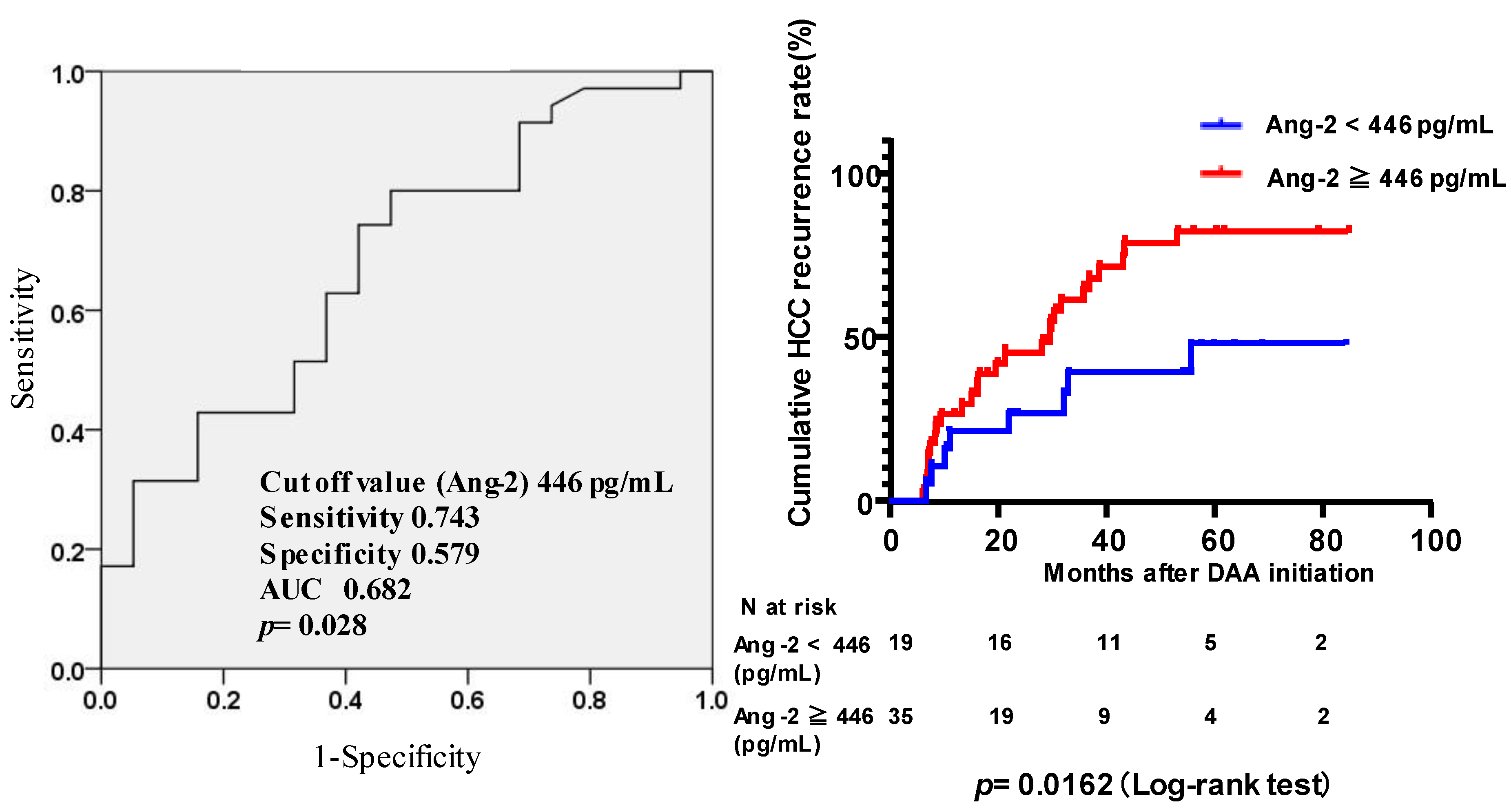
3.5. Factors Associated with HCC Recurrence after Successful HCV Eradication by DAAs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Suda, G.; Ogawa, K.; Yamamoto, Y.; Katagiri, M.; Furuya, K.; Kumagai, K.; Konno, J.; Kimura, M.; Kawagishi, N.; Ohara, M.; et al. Retreatment with sofosbuvir, ledipasvir, and add-on ribavirin for patients who failed daclatasvir and asunaprevir combination therapy. J. Gastroenterol. 2017, 52, 1122–1129. [Google Scholar] [CrossRef] [PubMed]
- Suda, G.; Ogawa, K.; Morikawa, K.; Sakamoto, N. Treatment of hepatitis C in special populations. J. Gastroenterol. 2018, 53, 591–605. [Google Scholar] [CrossRef] [Green Version]
- Suda, G.; Kurosaki, M.; Itakura, J.; Izumi, N.; Uchida, Y.; Mochida, S.; Hasebe, C.; Abe, M.; Haga, H.; Ueno, Y.; et al. Safety and efficacy of elbasvir and grazoprevir in Japanese hemodialysis patients with genotype 1b hepatitis C virus infection. J. Gastroenterol. 2019, 54, 78–86. [Google Scholar] [CrossRef]
- Suda, G.; Kudo, M.; Nagasaka, A.; Furuya, K.; Yamamoto, Y.; Kobayashi, T.; Shinada, K.; Tateyama, M.; Konno, J.; Tsukuda, Y.; et al. Efficacy and safety of daclatasvir and asunaprevir combination therapy in chronic hemodialysis patients with chronic hepatitis C. J. Gastroenterol. 2016, 51, 733–740. [Google Scholar] [CrossRef] [Green Version]
- Suda, G.; Hasebe, C.; Abe, M.; Kurosaki, M.; Itakura, J.; Izumi, N.; Uchida, Y.; Mochida, S.; Haga, H.; Ueno, Y.; et al. Safety and efficacy of glecaprevir and pibrentasvir in Japanese hemodialysis patients with genotype 2 hepatitis C virus infection. J. Gastroenterol. 2019, 54, 641–649. [Google Scholar] [CrossRef]
- Suda, G.; Furusyo, N.; Toyoda, H.; Kawakami, Y.; Ikeda, H.; Suzuki, M.; Arataki, K.; Mori, N.; Tsuji, K.; Katamura, Y.; et al. Daclatasvir and asunaprevir in hemodialysis patients with hepatitis C virus infection: A nationwide retrospective study in Japan. J. Gastroenterol. 2018, 53, 119–128. [Google Scholar] [CrossRef]
- Suda, G.; Sakamoto, N. Recent advances in the treatment of hepatitis C virus infection for special populations and remaining problems. J. Gastroenterol. Hepatol. 2020. [Google Scholar] [CrossRef]
- Rockstroh, J.K.; Lacombe, K.; Viani, R.M.; Orkin, C.; Wyles, D.; Luetkemeyer, A.F.; Soto-Malave, R.; Flisiak, R.; Bhagani, S.; Sherman, K.E.; et al. Efficacy and Safety of Glecaprevir/Pibrentasvir in Patients Coinfected With Hepatitis C Virus and Human Immunodeficiency Virus Type 1: The EXPEDITION-2 Study. Clin. Infect. Dis. 2018, 67, 1010–1017. [Google Scholar] [CrossRef] [Green Version]
- Naggie, S.; Cooper, C.; Saag, M.; Workowski, K.; Ruane, P.; Towner, W.J.; Marks, K.; Luetkemeyer, A.; Baden, R.P.; Sax, P.E.; et al. Ledipasvir and Sofosbuvir for HCV in Patients Coinfected with HIV-1. N. Engl. J. Med. 2015, 373, 705–713. [Google Scholar] [CrossRef]
- Agarwal, K.; Castells, L.; Mullhaupt, B.; Rosenberg, W.M.C.; McNabb, B.; Arterburn, S.; Camus, G.; McNally, J.; Stamm, L.M.; Brainard, D.M.; et al. Sofosbuvir/velpatasvir for 12weeks in genotype 1-4 HCV-infected liver transplant recipients. J. Hepatol. 2018, 69, 603–607. [Google Scholar] [CrossRef]
- Tahata, Y.; Hikita, H.; Mochida, S.; Kawada, N.; Enomoto, N.; Ido, A.; Yoshiji, H.; Miki, D.; Hiasa, Y.; Takikawa, Y.; et al. Sofosbuvir plus velpatasvir treatment for hepatitis C virus in patients with decompensated cirrhosis: A Japanese real-world multicenter study. J. Gastroenterol. 2021, 56, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Esteban, R.; Pineda, J.A.; Calleja, J.L.; Casado, M.; Rodriguez, M.; Turnes, J.; Morano Amado, L.E.; Morillas, R.M.; Forns, X.; Pascasio Acevedo, J.M.; et al. Efficacy of Sofosbuvir and Velpatasvir, With and Without Ribavirin, in Patients With Hepatitis C Virus Genotype 3 Infection and Cirrhosis. Gastroenterology 2018, 155, 1120–1127.e1124. [Google Scholar] [CrossRef] [Green Version]
- Ioannou, G.N.; Green, P.K.; Berry, K. HCV eradication induced by direct-acting antiviral agents reduces the risk of hepatocellular carcinoma. J. Hepatol. 2017, 68, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Tachi, Y.; Hirai, T.; Miyata, A.; Ohara, K.; Iida, T.; Ishizu, Y.; Honda, T.; Kuzuya, T.; Hayashi, K.; Ishigami, M.; et al. Progressive fibrosis significantly correlates with hepatocellular carcinoma in patients with a sustained virological response. Hepatol. Res. 2015, 45, 238–246. [Google Scholar] [CrossRef]
- Shiratori, Y.; Imazeki, F.; Moriyama, M.; Yano, M.; Arakawa, Y.; Yokosuka, O.; Kuroki, T.; Nishiguchi, S.; Sata, M.; Yamada, G.; et al. Histologic improvement of fibrosis in patients with hepatitis C who have sustained response to interferon therapy. Ann. Intern. Med. 2000, 132, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Kawagishi, N.; Suda, G.; Kimura, M.; Maehara, O.; Shimazaki, T.; Yamada, R.; Kitagataya, T.; Shigesawa, T.; Suzuki, K.; Nakamura, A.; et al. High serum angiopoietin-2 level predicts non-regression of liver stiffness measurement-based liver fibrosis stage after direct-acting antiviral therapy for hepatitis C. Hepatol. Res. 2020, 50, 671–681. [Google Scholar] [CrossRef]
- Mauro, E.; Crespo, G.; Montironi, C.; Londono, M.C.; Hernandez-Gea, V.; Ruiz, P.; Sastre, L.; Lombardo, J.; Marino, Z.; Diaz, A.; et al. Portal pressure and liver stiffness measurements in the prediction of fibrosis regression after sustained virological response in recurrent hepatitis C. Hepatology 2018, 67, 1683–1694. [Google Scholar] [CrossRef] [Green Version]
- Kawagishi, N.; Suda, G.; Kimura, M.; Maehara, O.; Yamada, R.; Tokuchi, Y.; Kubo, A.; Kitagataya, T.; Shigesawa, T.; Suzuki, K.; et al. Baseline elevated serum angiopoietin-2 predicts long-term non-regression of liver fibrosis after direct-acting antiviral therapy for hepatitis C. Sci. Rep. 2021, 11, 9207. [Google Scholar] [CrossRef]
- Souma, T.; Thomson, B.R.; Heinen, S.; Carota, I.A.; Yamaguchi, S.; Onay, T.; Liu, P.; Ghosh, A.K.; Li, C.; Eremina, V.; et al. Context-dependent functions of angiopoietin 2 are determined by the endothelial phosphatase VEPTP. Proc. Natl. Acad. Sci. USA 2018, 115, 1298–1303. [Google Scholar] [CrossRef] [Green Version]
- Benest, A.V.; Kruse, K.; Savant, S.; Thomas, M.; Laib, A.M.; Loos, E.K.; Fiedler, U.; Augustin, H.G. Angiopoietin-2 is critical for cytokine-induced vascular leakage. PLoS ONE 2013, 8, e70459. [Google Scholar] [CrossRef]
- Saharinen, P.; Eklund, L.; Alitalo, K. Therapeutic targeting of the angiopoietin-TIE pathway. Nat. Rev. Drug Discov. 2017, 16, 635–661. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, S.; Suda, G.; Ohara, M.; Fu, Q.; Yang, Z.; Hosoda, S.; Kimura, M.; Akinori, K.; Tokuchi, Y.; Yamada, R.; et al. Frequency and Characteristics of Overestimated Renal Function in Japanese Patients with Chronic Liver Disease and Its Relation to Sarcopenia. Nutrients 2021, 13, 2415. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, S.; Suda, G.; Ohara, M.; Kimura, M.; Yang, Z.; Maehara, O.; Fu, Q.; Hosoda, S.; Akinori, K.; Tokuchi, Y.; et al. Overestimated renal function in patients with liver cirrhosis predicts poor prognosis. Hepatol. Res. 2022, 52, 603–613. [Google Scholar] [CrossRef] [PubMed]
- Ohara, M.; Suda, G.; Kimura, M.; Maehara, O.; Shimazaki, T.; Shigesawa, T.; Suzuki, K.; Nakamura, A.; Kawagishi, N.; Nakai, M.; et al. Analysis of the optimal psoas muscle mass index cut-off values, as measured by computed tomography, for the diagnosis of loss of skeletal muscle mass in Japanese people. Hepatol. Res. 2020, 50, 715–725. [Google Scholar] [CrossRef]
- Shigesawa, T.; Suda, G.; Kimura, M.; Maehara, O.; Tokuchi, Y.; Kubo, A.; Yamada, R.; Furuya, K.; Baba, M.; Kitagataya, T.; et al. Baseline serum angiopoietin-2 and VEGF levels predict the deterioration of the liver functional reserve during lenvatinib treatment for hepatocellular carcinoma. PLoS ONE 2021, 16, e0247728. [Google Scholar] [CrossRef]
- Shigesawa, T.; Suda, G.; Kimura, M.; Shimazaki, T.; Maehara, O.; Yamada, R.; Kitagataya, T.; Suzuki, K.; Nakamura, A.; Ohara, M.; et al. Baseline angiopoietin-2 and FGF19 levels predict treatment response in patients receiving multikinase inhibitors for hepatocellular carcinoma. JGH Open 2020, 4, 880–888. [Google Scholar] [CrossRef] [Green Version]
- Alberts, C.J.; Clifford, G.M.; Georges, D.; Negro, F.; Lesi, O.A.; Hutin, Y.J.; de Martel, C. Worldwide prevalence of hepatitis B virus and hepatitis C virus among patients with cirrhosis at country, region, and global levels: A systematic review. Lancet Gastroenterol. Hepatol. 2022, 7, 724–735. [Google Scholar] [CrossRef]
- Akuta, N.; Suzuki, F.; Sezaki, H.; Kobayashi, M.; Fujiyama, S.; Kawamura, Y.; Hosaka, T.; Kobayashi, M.; Saitoh, S.; Suzuki, Y.; et al. Complex Association of Virus- and Host-Related Factors with Hepatocellular Carcinoma Rate following Hepatitis C Virus Clearance. J. Clin. Microbiol. 2019, 57, e01463-18. [Google Scholar] [CrossRef] [Green Version]
- Nagata, H.; Nakagawa, M.; Asahina, Y.; Sato, A.; Asano, Y.; Tsunoda, T.; Miyoshi, M.; Kaneko, S.; Otani, S.; Kawai-Kitahata, F.; et al. Effect of interferon-based and -free therapy on early occurrence and recurrence of hepatocellular carcinoma in chronic hepatitis C. J. Hepatol. 2017, 67, 933–939. [Google Scholar] [CrossRef]
- Ogawa, E.; Furusyo, N.; Nomura, H.; Dohmen, K.; Higashi, N.; Takahashi, K.; Kawano, A.; Azuma, K.; Satoh, T.; Nakamuta, M.; et al. Short-term risk of hepatocellular carcinoma after hepatitis C virus eradication following direct-acting anti-viral treatment. Aliment. Pharmacol. Ther. 2018, 47, 104–113. [Google Scholar] [CrossRef]
- Watanabe, T.; Tokumoto, Y.; Joko, K.; Michitaka, K.; Horiike, N.; Tanaka, Y.; Tada, F.; Kisaka, Y.; Nakanishi, S.; Yamauchi, K.; et al. Predictors of hepatocellular carcinoma occurrence after direct-acting antiviral therapy in patients with hepatitis C virus infection. Hepatol. Res. 2019, 49, 136–146. [Google Scholar] [CrossRef]
- Nakai, M.; Yamamoto, Y.; Baba, M.; Suda, G.; Kubo, A.; Tokuchi, Y.; Kitagataya, T.; Yamada, R.; Shigesawa, T.; Suzuki, K.; et al. Prediction of hepatocellular carcinoma using age and liver stiffness on transient elastography after hepatitis C virus eradication. Sci. Rep. 2022, 12, 1449. [Google Scholar] [CrossRef] [PubMed]
- Goettsch, W.; Gryczka, C.; Korff, T.; Ernst, E.; Goettsch, C.; Seebach, J.; Schnittler, H.J.; Augustin, H.G.; Morawietz, H. Flow-dependent regulation of angiopoietin-2. J. Cell Physiol. 2008, 214, 491–503. [Google Scholar] [CrossRef] [PubMed]
- Faillaci, F.; Marzi, L.; Critelli, R.; Milosa, F.; Schepis, F.; Turola, E.; Andreani, S.; Vandelli, G.; Bernabucci, V.; Lei, B.; et al. Liver Angiopoietin-2 Is a Key Predictor of De Novo or Recurrent Hepatocellular Cancer After Hepatitis C Virus Direct-Acting Antivirals. Hepatology 2018, 68, 1010–1024. [Google Scholar] [CrossRef] [Green Version]
- Lefere, S.; Van de Velde, F.; Hoorens, A.; Raevens, S.; Van Campenhout, S.; Vandierendonck, A.; Neyt, S.; Vandeghinste, B.; Vanhove, C.; Debbaut, C.; et al. Angiopoietin-2 Promotes Pathological Angiogenesis and Is a Therapeutic Target in Murine Nonalcoholic Fatty Liver Disease. Hepatology 2019, 69, 1087–1104. [Google Scholar] [CrossRef]
- Allegretti, A.S.; Vela Parada, X.; Ortiz, G.A.; Long, J.; Krinsky, S.; Zhao, S.; Fuchs, B.C.; Sojoodi, M.; Zhang, D.; Karumanchi, S.A.; et al. Serum Angiopoietin-2 Predicts Mortality and Kidney Outcomes in Decompensated Cirrhosis. Hepatology 2019, 69, 729–741. [Google Scholar] [CrossRef] [Green Version]
- Sahni, J.; Patel, S.S.; Dugel, P.U.; Khanani, A.M.; Jhaveri, C.D.; Wykoff, C.C.; Hershberger, V.S.; Pauly-Evers, M.; Sadikhov, S.; Szczesny, P.; et al. Simultaneous Inhibition of Angiopoietin-2 and Vascular Endothelial Growth Factor-A with Faricimab in Diabetic Macular Edema: BOULEVARD Phase 2 Randomized Trial. Ophthalmology 2019, 126, 1155–1170. [Google Scholar] [CrossRef] [Green Version]
- Meyer, T.; Ledin, E.; Kim, D.-W.; Ghiringhelli, F.; Serwatowski, P.; Voskoboynik, M.; Landsteiner, H.T.; Chen, V.; Jayadeva, G.; Macarulla, T. Phase Ib study of BI 836880 (VEGF/Ang2 inhibitor) plus ezabenlimab (BI 754091; anti-PD-1 antibody) in patients (pts) with advanced hepatocellular carcinoma (HCC). J. Clin. Oncol. 2022, 40, 434. [Google Scholar] [CrossRef]
- Pauta, M.; Ribera, J.; Melgar-Lesmes, P.; Casals, G.; Rodriguez-Vita, J.; Reichenbach, V.; Fernandez-Varo, G.; Morales-Romero, B.; Bataller, R.; Michelena, J.; et al. Overexpression of angiopoietin-2 in rats and patients with liver fibrosis. Therapeutic consequences of its inhibition. Liver Int. 2015, 35, 1383–1392. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No History of HCC | History of HCC | |
|---|---|---|
| Number | 256 | 54 |
| Age (years) a | 70 (22–86) | 73 (50–86) |
| Sex (male/female) | 102/154 | 29/25 |
| HCV genotype (1/2/unknown) | 183/71/2 | 49/5/0 |
| Platelet count (104/μL) a | 13.3 (2.2–37.3) | 11.9 (1.9–38.8) |
| Albumin (g/dL) a | 4.0 (2.5–4.9) | 3.7 (2.6–4.4) |
| AST (IU/L) a | 47 (16–342) | 47.5 (15–176) |
| ALT (IU/L) a | 42 (6–379) | 37 (14–128) |
| FIB-4 index a | 3.99 (0.54–23.55) | 5.87 (1.36–39.35) |
| Liver cirrhosis (LC)/non-LC | 123/133 | 36/18 |
| M2BPGi a | 2.69 (0.28–17.76) | 5.31 (0.67–20.01) |
| AFP (ng/mL) a | 5.4 (1.1–250.8) | 8.6 (2.2–83.9) |
| Angiopoietin-2 (pg/mL) a | 367.9 (131.9–1489) | 483.8 (178.2–1598.6) |
| Diabetes, n (%) | 50 (19.5%) | 14 (25.9%) |
| Duration from the start date of DAA treatment (months) a,b | 49.3 (12.3–86) | 57.4 (12.1–85.1) |
| History of HCC, n (%) | 0 (0%) | 54 (100%) |
| Previous HCC characteristics | ||
| HCC stage (1/2/3/4) | - | 30/23/1/0 |
| Treatment (RFA/TACE/operation/others) | - | 30/9/14/1 |
| Treatment (curative/non-curative) | - | 54/0 |
| Duration from the last HCC treatment to the initiation of DAA therapy (months) a | - | 5.9 (1–95.2) |
| Cut-off Value | Univariate p-Values | Multivariate | |||
|---|---|---|---|---|---|
| Factors | HR | 95% CI | p-Values | ||
| Age (years) | ≥75 | * 0.026 | 2.92 | 1.34–6.33 | * 0.007 |
| Sex (male/female) | Male | 0.459 | |||
| HCV genotype | 1 | 0.436 | |||
| Platelet count (104/μL) | ≥13.8 | 0.5 | |||
| Albumin (g/dL) | ≥4.0 | 0.393 | |||
| AST (IU/L) | ≥47 | 0.079 | |||
| ALT (IU/L) | ≥42 | 0.829 | |||
| FIB-4 index | ≥4.55 | 0.093 | |||
| M2BPGi | ≥4.23 | * <0.001 | 2.13 | 0.82–5.52 | 0.12 |
| AFP (ng/mL) | ≥7.7 | * 0.006 | 1.61 | 0.66–3.89 | 0.292 |
| Angiopoietin-2 (pg/mL) | ≥464 | * 0.003 | 2.75 | 1.18–6.37 | * 0.019 |
| Delta Angiopoietin-2 between baseline and end of treatment | ≥−13 | 0.258 | |||
| Diabetes, n (%) | Yes | * 0.03 | 2.05 | 0.89–4.69 | 0.091 |
| Cut-off Value | Univariate p-Values | Multivariate | |||
|---|---|---|---|---|---|
| Factors | HR | 95% CI | p-Values | ||
| Age (years) | ≥75 | * 0.026 | 1.85 | 0.8–4.29 | 0.151 |
| Sex (male/female) | Male | 0.459 | |||
| HCV genotype | 1 | 0.436 | |||
| Platelet count (104/μL) at EOT | ≥15.8 | 0.765 | |||
| Albumin (g/dL) at EOT | ≥4.3 | 0.404 | |||
| AST (IU/L) at EOT | ≥24 | 0.194 | |||
| ALT (IU/L) at EOT | ≥18 | 0.757 | |||
| FIB-4 index at EOT | ≥3.67 | * 0.046 | 1.42 | 0.57–3.51 | 0.448 |
| M2BPGi at EOT | ≥1.89 | * 0.001 | 1.37 | 0.5–3.79 | 0.542 |
| AFP (ng/mL) at EOT | ≥4.6 | * 0.037 | 1.38 | 0.57–3.34 | 0.48 |
| Angiopoietin-2 (pg/mL) at EOT | ≥402 | * <0.001 | 3.68 | 1.37–9.9 | * 0.01 |
| Diabetes, n (%) | Yes | * 0.03 | 2.05 | 0.85–4.93 | 0.109 |
| Cut-off Value | Univariate p-Values | Multivariate | |||
|---|---|---|---|---|---|
| Factors | HR | 95% CI | p-Values | ||
| Age (years) | ≥71 | 0.605 | |||
| Sex (male/female) | Male | 0.407 | |||
| HCV genotype | 1 | 0.255 | |||
| Platelet count (104/μL) | ≥13.4 | 0.936 | |||
| Albumin (g/dL) | ≥3.7 | 0.517 | |||
| AST (IU/L) | ≥45 | * <0.001 | 1.81 | 0.67–4.93 | 0.244 |
| ALT (IU/L) | ≥37 | * <0.001 | 2.61 | 0.9–7.58 | 0.077 |
| FIB-4 index | ≥6.4 | 0.872 | |||
| M2BPGi | ≥5.22 | * 0.025 | 1.332 | 0.751–1.492 | 0.213 |
| AFP (ng/mL) | ≥8.6 | 0.053 | |||
| Angiopoietin-2 (pg/mL) | ≥446 | * 0.017 | 2.659 | 1.209–5.847 | * 0.015 |
| Delta Angiopoietin-2 (pg/mL) between baseline and end of treatment | ≥−31 | 0.197 | |||
| Diabetes, n (%) | Yes | 0.409 | |||
| Previous HCC characteristics | |||||
| HCC stage | >1 | 0.509 | |||
| Treatment | RFA or operation | 0.685 | |||
| Duration from HCC treatment to DAA (months) | ≥7.62 | 0.494 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawagishi, N.; Suda, G.; Yamamoto, Y.; Baba, M.; Furuya, K.; Maehara, O.; Ohnishi, S.; Yoshida, S.; Fu, Q.; Yang, Z.; et al. Serum Angiopoietin-2 Predicts the Occurrence and Recurrence of Hepatocellular Carcinoma after Direct-Acting Antiviral Therapy for Hepatitis C. Viruses 2023, 15, 181. https://doi.org/10.3390/v15010181
Kawagishi N, Suda G, Yamamoto Y, Baba M, Furuya K, Maehara O, Ohnishi S, Yoshida S, Fu Q, Yang Z, et al. Serum Angiopoietin-2 Predicts the Occurrence and Recurrence of Hepatocellular Carcinoma after Direct-Acting Antiviral Therapy for Hepatitis C. Viruses. 2023; 15(1):181. https://doi.org/10.3390/v15010181
Chicago/Turabian StyleKawagishi, Naoki, Goki Suda, Yoshiya Yamamoto, Masaru Baba, Ken Furuya, Osamu Maehara, Shunsuke Ohnishi, Sonoe Yoshida, Qingjie Fu, Zijian Yang, and et al. 2023. "Serum Angiopoietin-2 Predicts the Occurrence and Recurrence of Hepatocellular Carcinoma after Direct-Acting Antiviral Therapy for Hepatitis C" Viruses 15, no. 1: 181. https://doi.org/10.3390/v15010181