
A Cross-Sectional Comparative Characterization of Hematological Changes in Patients with COVID-19 Infection, Non-COVID Influenza-like Illnesses and Healthy Controls
 ,
,  ,
,
Abstract
:1. Introduction
2. Material and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hosseini, A.; Hashemi, V.; Shomali, N.; Asghari, F.; Gharibi, T.; Akbari, M.; Gholizadeh, S.; Jafari, A. Innate and adaptive immune responses against coronavirus. Biomed. Pharmacother. 2020, 132, 110859. [Google Scholar] [CrossRef] [PubMed]
- Lamers, M.M.; Haagmans, B.L. SARS-CoV-2 pathogenesis. Nat. Rev. Microbiol. 2022, 20, 270–284. [Google Scholar] [CrossRef] [PubMed]
- Liew, P.X.; Kubes, P. The Neutrophil’s Role During Health and Disease. Physiol. Rev. 2019, 99, 1223–1248. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Liu, S.; Goraya, M.U.; Maarouf, M.; Huang, S.; Chen, J.L. Host Immune Response to Influenza A Virus Infection. Front. Immunol. 2018, 9, 320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, A.P.; Liu, J.P.; Tao, W.Q.; Li, H.M. The diagnostic and predictive role of NLR, d-NLR and PLR in COVID-19 patients. Int. Immunopharmacol. 2020, 84, 106504. [Google Scholar] [CrossRef] [PubMed]
- Cui, S.N.; Tan, H.Y.; Fan, G.C. Immunopathological Roles of Neutrophils in Virus Infection and COVID-19. Shock 2021, 56, 345–351. [Google Scholar] [CrossRef]
- Payen, D.; Cravat, M.; Maadadi, H.; Didelot, C.; Prosic, L.; Dupuis, C.; Losser, M.-R.; Bittencourt, M.D.C. A Longitudinal Study of Immune Cells in Severe COVID-19 Patients. Front. Immunol. 2020, 11, 580250. [Google Scholar] [CrossRef]
- Knoll, R.; Schultze, J.L.; Schulte-Schrepping, J. Monocytes and Macrophages in COVID-19. Front. Immunol. 2021, 12, 720109. [Google Scholar] [CrossRef]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Invest. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- Tan, L.; Wang, Q.; Zhang, D.; Ding, J.; Huang, Q.; Tang, Y.-Q.; Wang, Q.; Miao, H. Lymphopenia predicts disease severity of COVID-19: A descriptive and predictive study. Signal Transduct. Target. Ther. 2020, 5, 33. [Google Scholar] [CrossRef]
- Delshad, M.; Tavakolinia, N.; Pourbagheri-Sigaroodi, A.; Safaroghli-Azar, A.; Bagheri, N.; Bashash, D. The contributory role of lymphocyte subsets, pathophysiology of lymphopenia and its implication as prognostic and therapeutic opportunity in COVID-19. Int. Immunopharmacol. 2021, 95, 107586. [Google Scholar] [CrossRef] [PubMed]
- Jayaram, A.; Mathews, N.S.; Nair, S.C.; Geevar, T.; Rose, W.; Verghese, V.P.; Mathuram, A.J.; Gunasekaran, K.; Abraham, A.M.; Mammen, J.J. High fluorescent lymphocyte cell count and scattergram patterns on the Sysmex XN series cell counters-Novel parameters in early and reliable diagnosis of dengue on a background of acute febrile illness. Int. J. Lab. Hematol. 2021, 43, O156–O160. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.-J.; Kim, J.-H.; Park, Y.-J.; Kahng, J.; Lee, H.; Lee, K.-Y.; Kim, M.Y.; Han, K.; Lee, W. Evaluation of cell population data on the UniCel DxH 800 Coulter Cellular Analysis system as a screening for viral infection in children. Int. J. Lab. Hematol. 2012, 34, 283–289. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Director-General’s Remarks at the Media Briefing on 2019-nCoV on 11 February 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020 (accessed on 21 July 2022).
- Brihn, A.; Chang, J.; OYong, K.; Balter, S.; Terashita, D.; Rubin, Z.; Yeganeh, N. Diagnostic Performance of an Antigen Test with RT-PCR for the Detection of SARS-CoV-2 in a Hospital Setting—Los Angeles County, California, June–August 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 702–706. [Google Scholar] [CrossRef]
- Di Mitri, C.; Arcoleo, G.; Mazzuca, E.; Camarda, G.; Farinella, E.M.; Soresi, M.; Carroccio, A.; IMUSG. COVID-19 and non-COVID-19 pneumonia: A comparison. Ann. Med. 2021, 53, 2321–2331. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; The Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Selim, S. Leukocyte count in COVID-19: An important consideration. Egypt J. Bronchol. 2020, 14, 43. [Google Scholar] [CrossRef]
- Urrechaga, E.; Ponga, C.; Fernández, M.; España, P.P.; Haider, R.Z.; Aguirre, U. Diagnostic potential of leukocyte differential and cell population data in prediction of COVID-19 among related viral and bacterial infections at Emergency Department. Clin. Chem. Lab. Med. 2022, 60, e104–e107. [Google Scholar] [CrossRef]
- Van Elden, L.J.; van Essen, G.A.; Boucher, C.A.; van Loon, A.M.; Nijhuis, M.; Schipper, P.; Verheij, T.J.; Hoepelman, I.M. Clinical diagnosis of influenza virus infection: Evaluation of diagnostic tools in general practice. Br. J. Gen. Pract. 2001, 51, 630–634. [Google Scholar]
- Sahu, K.K.; Mishra, A.K.; Raturi, M.; Lal, A. Current Perspectives of convalescent plasma therapy in COVID-19. Acta Biomed. 2020, 91, e2020175. [Google Scholar]
- Marionneaux, S. Nonmalignant leukocyte disorders. Rodaks Hematol. 2020, 445–465. [Google Scholar] [CrossRef]
- Tanni, F.; Akker, E.; Zaman, M.M.; Figueroa, N.; Tharian, B.; Hupart, K.H. Eosinopenia and COVID-19. J. Am. Osteopath. Assoc. 2020; accepted. [Google Scholar] [CrossRef] [PubMed]
- Arora, P.; Gupta, P.K.; Lingaiah, R.; Mukhopadhyay, A.K. Volume, conductivity, and scatter parameters of leukocytes as early markers of sepsis and treatment response. J. Lab. Physicians 2019, 11, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Manley, H.R.; Keightley, M.C.; Lieschke, G.J. The Neutrophil Nucleus: An Important Influence on Neutrophil Migration and Function. Front. Immunol. 2018, 9, 2867. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Zhang, Z.; Prajapati, M.; Li, Y. Lymphopenia Caused by Virus Infections and the Mechanisms Beyond. Viruses 2021, 13, 1876. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Liao, D.; Jiang, J.; Sun, T.; Deng, S. The VCS Parameters of Lymphocytes may Improve Discrimination between Bacterial Infection and Viral Infection. Clin. Lab. 2021, 67, 11. [Google Scholar] [CrossRef] [PubMed]
- Seyit, M.; Avci, E.; Nar, R.; Senol, H.; Yilmaz, A.; Ozen, M.; Oskay, A.; Aybek, H. Neutrophil to lymphocyte ratio, lymphocyte to monocyte ratio and platelet to lymphocyte ratio to predict the severity of COVID-19. Am. J. Emerg. Med. 2021, 40, 110–114. [Google Scholar] [CrossRef]
- Liu, J.; Liu, Y.; Xiang, P.; Pu, L.; Xiong, H.; Li, C.; Zhang, M.; Tan, J.; Xu, Y.; Song, R.; et al. Neutrophil-to-lymphocyte ratio predicts critical illness patients with 2019 coronavirus disease in the early stage. J. Transl. Med. 2020, 18, 206. [Google Scholar] [CrossRef]
- Carbonell-Sahuquillo, S.; LAzaro-Carreno, M.I.; Camacho, J.; Barres-Fernandez, A.; Albert, E.; Torres, I.; Bretón-Martínez, J.R.; Martínez-Costa, C.; Navarro, D. Evaluation of a Rapid Antigen Detection test (Panbio COVID-19 Ag Rapid test device) as a point-of-care diagnostic tool for COVID-19 in a pediatric emergency department. J. Med. Virol. 2021, 93, 6803–6807. [Google Scholar] [CrossRef]
- Villarreal, A.; Rangel, G.; Zhang, X.; Wong, D.; Britton, G.; Fernandez, P.L.; Perez, A.; Oviedo, D.; Restrepo, C.; Carreirra, M.B.; et al. Performance of a Point of Care Test for Detecting IgM and IgG Antibodies Against SARS-CoV-2 and Seroprevalence in Blood Donors and Health Care Workers in Panama. Front. Med. 2021, 8, 616106. [Google Scholar] [CrossRef]
- Ozaras, R.; Cirpin, R.; Duran, A.; Duman, H.; Arslan, O.; Bakcan, Y.; Kaya, M.; Mutlu, H.; Isayeva, L.; Kebanli, F.; et al. Influenza and COVID-19 coinfection: Report of six cases and review of the literature. J. Med. Virol. 2020, 92, 2657–2665. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameters | COVID-19 (N = 169) | Control (N = 140) | Non-COVID-19 Influenza-like Illnesses (N = 113) | Pa | Pb |
|---|---|---|---|---|---|
| Age, Y | 55 ± 14.6 | 38.14 ± 8.7 | 50.19 ± 16.5 | 0 | 0.009 |
| Male, n (%) | 134(70.9) | 92(65.7) | 79(69.9) | 0.31 | 0.85 |
| WBC (×109) | 9.9 ± 6.1 | 6.8 ± 1.4 | 9.06 ± 4.5 | 0 | 0.197 |
| RBC (×1012/L) | 4.1 ± 0.8 | 4.5 ± 0.5 | 4.1 ± 0.767 | 0 | 0.67 |
| HB (g/L) | 12.01 ± 2.2 | 13.8 ± 1.6 | 12.1 ± 2.21 | 0 | 0.85 |
| PLT (×109/L) | 207.2 ± 121.5 | 195 ± 75.7 | 233.5 ± 136 | 0.32 | 0.084 |
| NE % | 75.8 ± 15.2 | 56.7 ± 8.05 | 71.5 ± 11.3 | 0 | 0.014 |
| LY % | 13.1(7.1–21.2) | 30.9(26.7–36.7) | 17.7(12.1–23.7) | 0 | 0.001 |
| MO % | 6.7(4.5–8.8) | 7.3(6.4–8.8) | 7.9(5.3–10.2) | 0.005 | 0.001 |
| EO % | 0.19(0.0–0.8) | 2.6(1.6–4.2) | 0.37(0.09–1.5) | 0 | 0.01 |
| BA % | 0.3(0.2–0.5) | 0.6(0.4–0.8) | 0.35(0.29–0.52) | 0 | 0.02 |
| NE # (×109/L) | 6.4(4.7–10.5) | 3.7(3.1–4.5) | 6.09(3.67–8.1) | 0 | 0.06 |
| LY # (×109/L) | 1.08(0.7–1.57) | 2.0(1.7–2.4) | 1.2(0.93–1.8) | 0 | 0.011 |
| MO # (×109/L) | 0.5(0.4–0.74) | 0.5(0.4–0.6) | 0.6(0.4–0.86) | 0.109 | 0.012 |
| EO # (×109/L) | 0.007(0.0–0.1) | 0.2(0.1–0.3) | 0.15(0.0–0.13) | 0 | 0.123 |
| BA # (×109/L) | 0.015(0.0–0.04) | 0.0(0.0–0.1) | 0.02(0.0–0.04) | 0.003 | 0.305 |
| MN-V-NE | 152(146–158) | 149(146–153.7) | 148(143.5–156) | 0.002 | 0.009 |
| MN-C-NE | 145(141–147) | 145(143–149) | 145(143–146) | 0.004 | 0.667 |
| MN-MALS-NE | 141(136–145) | 141(137–144) | 138(131–144) | 0.965 | 0.017 |
| MN-UMALS-NE | 142(136–145) | 141(139–144) | 141(134–145) | 0.449 | 0.024 |
| MN-LMALS-NE | 136(129–141) | 136(131–140) | 133(124–140) | 0.688 | 0.023 |
| MN-LALS-NE | 196(146–208) | 157(144–204.7) | 176(141–205) | 0.062 | 0.015 |
| MN-AL2-NE | 138(133.5–143) | 136(134–140) | 137(133–140) | 0.006 | 0.042 |
| MN-V-LY | 90(86–94) | 89(87–90.7) | 89(85–92) | 0.051 | 0.434 |
| MN-C-LY | 118(114–120) | 113(111–118) | 118(115–121) | 0 | 0.73 |
| MN-MALS-LY | 75(67.5–79) | 70(67–75) | 76(72.5–78) | 0 | 0.344 |
| MN-UMALS-LY | 80(69–86) | 73(69–79) | 80(77–85) | 0 | 0.176 |
| MN-LMALS-LY | 65(60–70) | 61(58–66) | 66(61–68) | 0 | 0.942 |
| MN-LALS-LY | 40(34–43.5) | 36(35–43) | 37(33.5–42) | 0.577 | 0.036 |
| MN-AL2-LY | 65(61–69) | 65(63–70) | 64(62–68) | 0.126 | 0.13 |
| MN-V-MO | 182(175–188) | 170(167–175) | 179(172–185) | 0 | 0.047 |
| MN-C-MO | 124(121–127) | 123(121–127) | 124(122–126) | 0.284 | 0.517 |
| MN-MALS-MO | 94(88–97) | 90(87–94) | 93(87–960 | 0 | 0.411 |
| MN-UMALS-MO | 105(98–109) | 100(96–103) | 104(98.5–107) | 0 | 0.579 |
| MN-LMALS-MO | 79(72–84) | 78(74–80.7) | 78(72–82) | 0.05 | 0.209 |
| MN-LALS-MO | 92(73–115) | 95(90–123.5) | 85(72.5–102.5) | 0 | 0.77 |
| MN-AL2-MO | 122(115–127) | 119(115.2–125.7) | 118(113–125) | 0.122 | 0.009 |
| NLR | 6.00(3.27–12.30) | 1.87(1.39–2.26) | 4.02(2.82–6.48) | 0 | 0.001 |
| PLR | 14.17(7.84–30.71) | 6.19(4.07–7.99) | 12.55(7.17–26.47) | 0 | 0.173 |
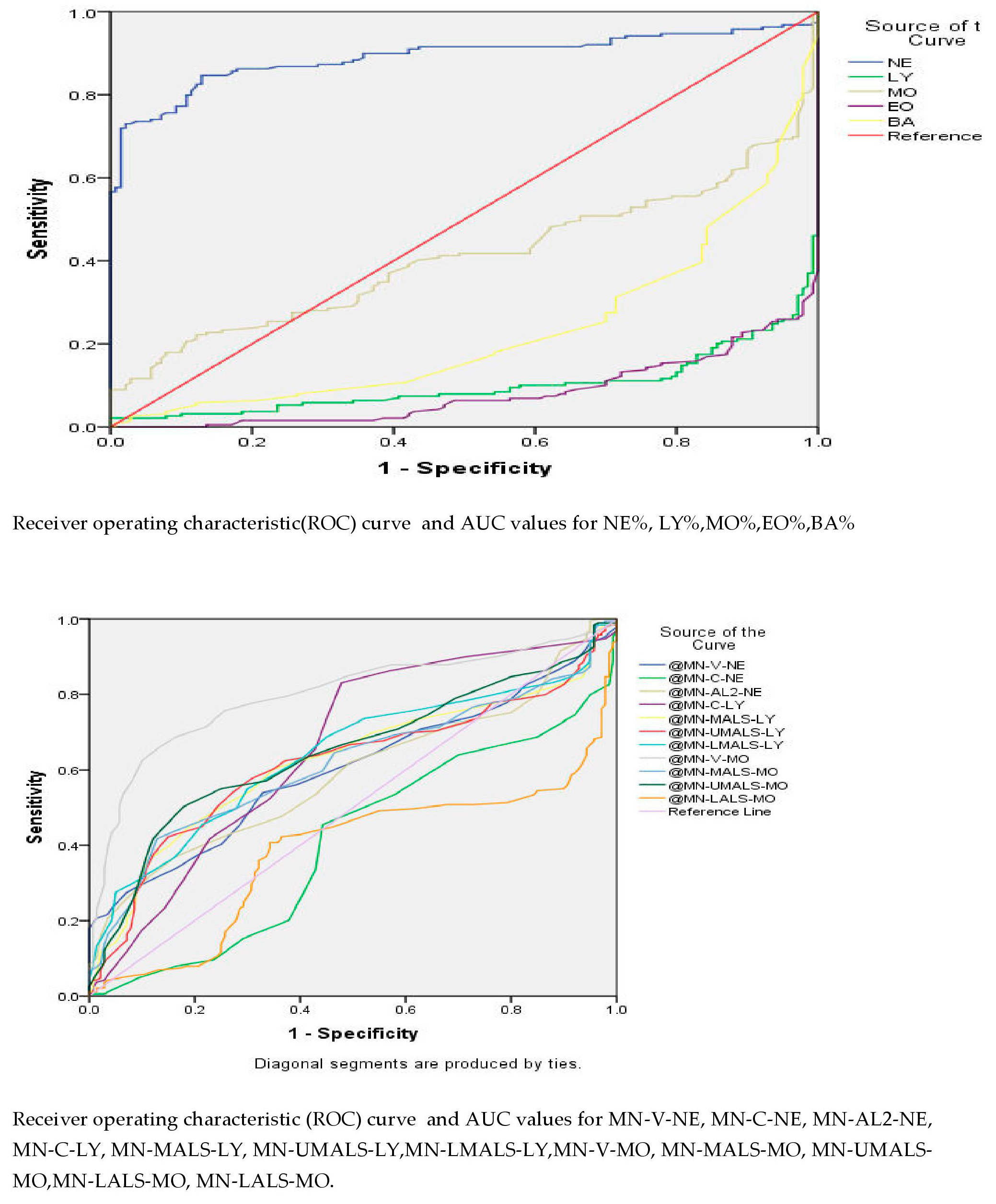
| Test Result Variable(s) | Area Under Curve | Sensitivity | Specificity | Cutoff | CI | p Value | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| NE # | 0.816 | 76% | 70% | 4.35 | 0.769 | 0.863 | 0 |
| MO # | 0.553 | 62% | 42% | 0.44 | 0.491 | 0.615 | 0.109 |
| BA # | 0.587 | 48% | 67% | 0.016 | 0.522 | 0.652 | 0.003 |
| NE % | 0.890 | 86% | 82% | 63.34 | 0.853 | 0.928 | 0 |
| MN-V-NE | 0.600 | 59% | 55% | 149.5 | 0.539 | 0.660 | 0.002 |
| MN-AL2-NE | 0.589 | 53% | 57% | 137.5 | 0.529 | 0.651 | 0.006 |
| MN-C-LY | 0.659 | 59% | 61% | 46.5 | 0598 | 0.720 | 0 |
| MN-MALS-LY | 0.625 | 62% | 60% | 71.5 | 0.565 | 0.686 | 0 |
| MN-UMALS-LY | 0.618 | 62% | 63% | 75.5 | 0.557 | 0.679 | 0 |
| MN-LMALS-LY | 0.641 | 59% | 64% | 63.5 | 0.582 | 0.701 | 0 |
| MN-V-MO | 0.798 | 75% | 74% | 174.5 | 0.749 | 0.846 | 0 |
| MN-MALS-MO | 0.614 | 64% | 53% | 90.5 | 0.554 | 0.675 | 0 |
| MN-UMALS-MO | 0.648 | 63% | 58% | 101.5 | 0.589 | 0.708 | 0 |
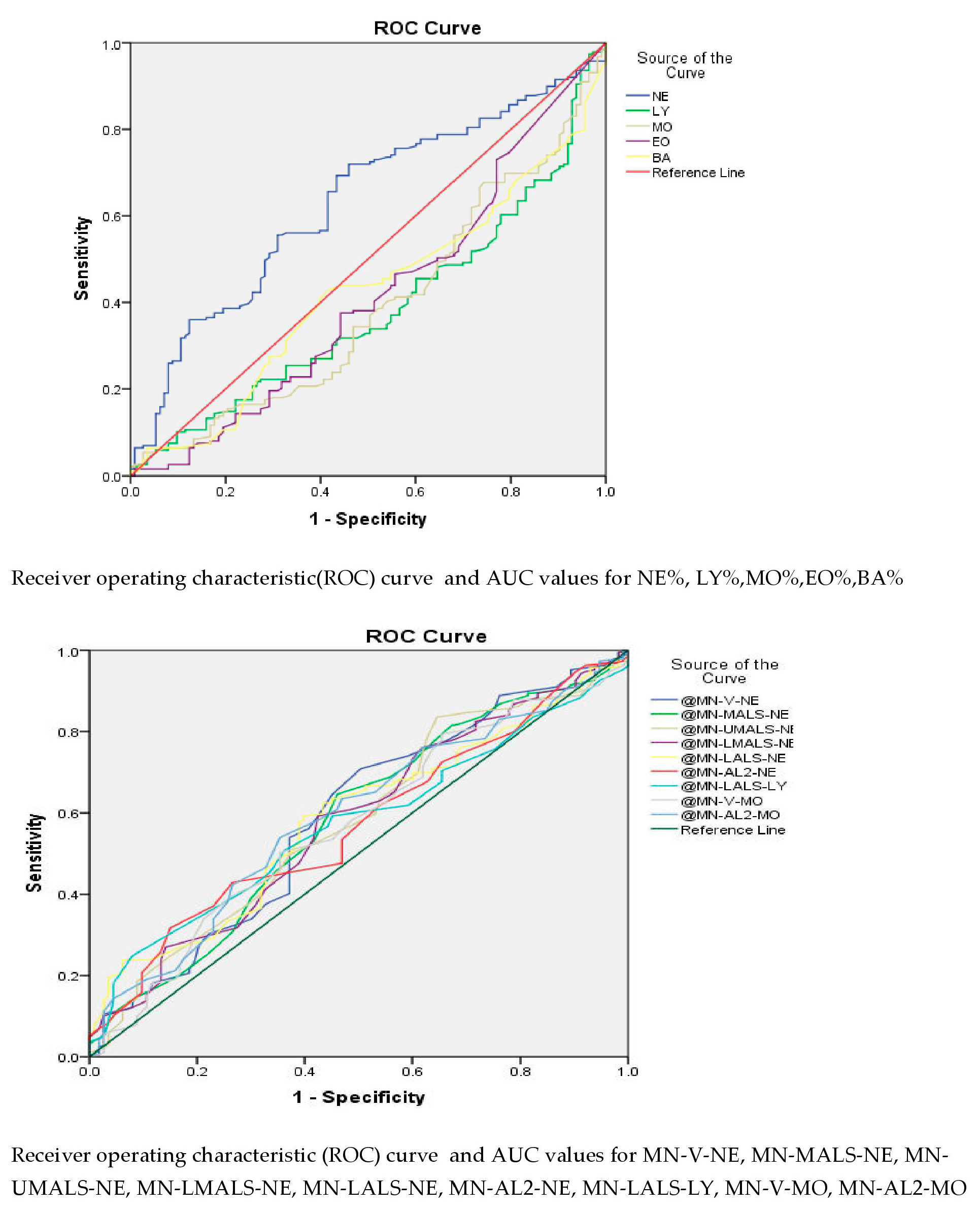
| Test Result Variable(s) | Area Under Curve | Sensitivity | Specificity | Cutoff | CI | p Value | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| NE % | 0.630 | 72% | 54% | 72.1 | 0.566 | 0694 | 0.014 |
| NE # | 0.565 | 67% | 44% | 5.14 | 0.497 | 0.631 | 0.060 |
| MN-V-NE | 0.589 | 64% | 54% | 148.5 | 0.657 | 0.522 | 0.009 |
| MN-MALS-NE | 0.582 | 64% | 54% | 138.5 | 0.515 | 0.649 | 0.017 |
| MN-UMALS-NE | 0.578 | 52% | 57% | 141.5 | 0.511 | 0644 | 0.024 |
| MN-LMALS-NE | 0.578 | 59% | 57% | 134.5 | 0.512 | 0.645 | 0.023 |
| MN-LALS-NE | 0.584 | 62% | 56% | 184.5 | 0.519 | 0.649 | 0.015 |
| MN-AL2-NE | 0.570 | 53% | 53% | 137.5 | 0.505 | 0.635 | 0.042 |
| MN-LALS-LY | 0.572 | 59% | 54% | 37.5 | 0.507 | 0.636 | 0.036 |
| MN-V-MO | 0.568 | 53% | 54% | 180.5 | 0.502 | 0.635 | 0.047 |
| MN-AL2-MO | 0.590 | 60% | 54% | 119.5 | 0.524 | 0.655 | 0.009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kala, M.; Ahmad, S.; Dhebane, M.; Das, K.; Raturi, M.; Tyagi, M.; Kusum, A. A Cross-Sectional Comparative Characterization of Hematological Changes in Patients with COVID-19 Infection, Non-COVID Influenza-like Illnesses and Healthy Controls. Viruses 2023, 15, 134. https://doi.org/10.3390/v15010134
Kala M, Ahmad S, Dhebane M, Das K, Raturi M, Tyagi M, Kusum A. A Cross-Sectional Comparative Characterization of Hematological Changes in Patients with COVID-19 Infection, Non-COVID Influenza-like Illnesses and Healthy Controls. Viruses. 2023; 15(1):134. https://doi.org/10.3390/v15010134
Chicago/Turabian StyleKala, Mansi, Sohaib Ahmad, Meghali Dhebane, Kunal Das, Manish Raturi, Meghna Tyagi, and Anuradha Kusum. 2023. "A Cross-Sectional Comparative Characterization of Hematological Changes in Patients with COVID-19 Infection, Non-COVID Influenza-like Illnesses and Healthy Controls" Viruses 15, no. 1: 134. https://doi.org/10.3390/v15010134