
Variability in the Clinical Course of COVID-19 in a Retrospective Analysis of a Large Real-World Database
 ,
,  , , , , , , , , , and
, , , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistical Analyses
3. Results
3.1. Demographic Characteristics of Patients Hospitalized during Different Periods of the Pandemic
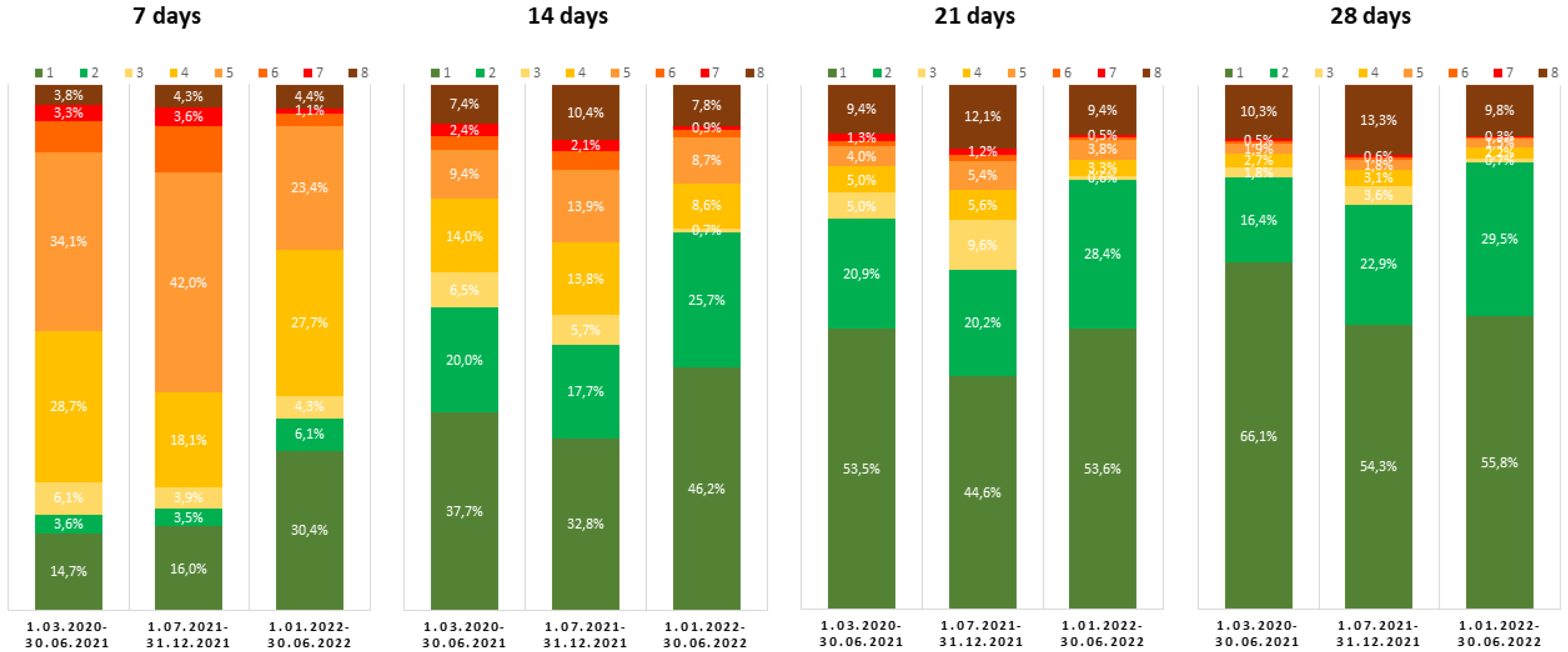
3.2. Clinical Features of Patients Hospitalized during Different Periods of the Pandemic
3.3. Mortality of Patients Hospitalized during Different Periods of the Pandemic
4. Discussion
4.1. Clinical Course of Disease during Periods Dominated by Different SARS-CoV-2 Variants
4.2. Potential Future Changes in Clinical Severity of SARS-CoV-2 Infections
4.3. Study Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 2 October 2022).
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 2 October 2022).
- Rochman, N.D.; Wolf, Y.I.; Faure, G.; Mutz, P.; Zhang, F.; Koonin, E.V. Ongoing Global and Regional Adaptive Evolution of SARS-CoV-2. Proc. Natl. Acad. Sci. USA 2021, 118, e2104241118. [Google Scholar] [CrossRef] [PubMed]
- Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants (accessed on 2 October 2022).
- Nagy, Á.; Pongor, S.; Győrffy, B. Different Mutations in SARS-CoV-2 Associate with Severe and Mild Outcome. Int. J. Antimicrob. Agents 2021, 57, 106272. [Google Scholar] [CrossRef] [PubMed]
- Twohig, K.A.; Nyberg, T.; Zaidi, A.; Thelwall, S.; Sinnathamby, M.A.; Aliabadi, S.; Seaman, S.R.; Harris, R.J.; Hope, R.; Lopez-Bernal, J.; et al. Hospital Admission and Emergency Care Attendance Risk for SARS-CoV-2 Delta (B.1.617.2) Compared with Alpha (B.1.1.7) Variants of Concern: A Cohort Study. Lancet Infect. Dis. 2022, 22, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Flisiak, R.; Rzymski, P.; Zarębska-Michaluk, D.; Rogalska, M.; Rorat, M.; Czupryna, P.; Lorenc, B.; Ciechanowski, P.; Kozielewicz, D.; Piekarska, A.; et al. Demographic and Clinical Overview of Hospitalized COVID-19 Patients during the First 17 Months of the Pandemic in Poland. J. Clin. Med. 2021, 11, 117. [Google Scholar] [CrossRef]
- Dobrowolska, K.; Brzdęk, M.; Zarębska-Michaluk, D.; Rzymski, P.; Rogalska, M.; Malinowska-Moniuszko, A.; Pasternak-Szymanek, A.; Jaroszewicz, J.; Dutkiewicz, E.; Kowalska, J.; et al. Differences between the course of SARS-CoV-2 infections in the periods of the Delta and Omicron variants dominance in Poland. Pol. Arch. Intern. Med. 2022; submitted. [Google Scholar]
- Cao, Y.; Wang, J.; Jian, F.; Xiao, T.; Song, W.; Yisimayi, A.; Huang, W.; Li, Q.; Wang, P.; An, R.; et al. Omicron Escapes the Majority of Existing SARS-CoV-2 Neutralizing Antibodies. Nature 2022, 602, 657–663. [Google Scholar] [CrossRef]
- Vangeel, L.; Chiu, W.; De Jonghe, S.; Maes, P.; Slechten, B.; Raymenants, J.; André, E.; Leyssen, P.; Neyts, J.; Jochmans, D. Remdesivir, Molnupiravir and Nirmatrelvir Remain Active against SARS-CoV-2 Omicron and Other Variants of Concern. Antivir. Res. 2022, 198, 105252. [Google Scholar] [CrossRef]
- Flisiak, R.; Zarębska-Michaluk, D.; Rogalska, M.; Kryńska, J.A.; Kowalska, J.; Dutkiewicz, E.; Dobrowolska, K.; Jaroszewicz, J.; Moniuszko-Malinowska, A.; Rorat, M.; et al. Real-World Experience with Molnupiravir during the Period of SARS-CoV-2 Omicron Variant Dominance. Pharmacol. Rep. 2022, 74, 1279–1285. [Google Scholar] [CrossRef]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. Public Health Scotland and the EAVE II Collaborators SARS-CoV-2 Delta VOC in Scotland: Demographics, Risk of Hospital Admission, and Vaccine Effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Saxena, S.K.; Kumar, S.; Ansari, S.; Paweska, J.T.; Maurya, V.K.; Tripathi, A.K.; Abdel-Moneim, A.S. Characterization of the Novel SARS-CoV-2 Omicron (B.1.1.529) Variant of Concern and Its Global Perspective. J. Med. Virol. 2022, 94, 1738–1744. [Google Scholar] [CrossRef]
- Classification of Omicron Variant. Available online: https://covariants.org/variants/21K.Omicron (accessed on 2 October 2022).
- Van Goethem, N.; Chung, P.; Meurisse, M.; Vandromme, M.; De Mot, L.; Brondeel, R.; Stouten, V.; Klamer, S.; Cuypers, L.; Braeye, T.; et al. Clinical Severity of SARS-CoV-2 Omicron Variant Compared with Delta among Hospitalized COVID-19 Patients in Belgium during Autumn and Winter Season 2021–2022. Viruses 2022, 14, 1297. [Google Scholar] [CrossRef]
- Khemiri, H.; Ayouni, K.; Triki, H.; Haddad-Boubaker, S. SARS-CoV-2 infection in pediatric population before and during the Delta (B.1.617.2) and Omicron (B.1.1.529) variants era. Virol. J. 2022, 19, 144. [Google Scholar] [CrossRef]
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Pawłowska, M.; Parczewski, M.; Piekarska, A.; Simon, K.; Tomasiewicz, K.; Zarębska-Michaluk, D. Management of SARS-CoV-2 Infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of March 31, 2020. Pol. Arch. Intern. Med. 2020, 130, 352–357. [Google Scholar] [CrossRef] [Green Version]
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Mastalerz-Migas, A.; Owczuk, R.; Parczewski, M.; Pawłowska, M.; Piekarska, A.; Simon, K.; et al. Management of SARS-CoV-2 Infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of April 26, 2021. Pol. Arch. Intern. Med. 2021, 131, 487–496. [Google Scholar] [CrossRef]
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Mastalerz-Migas, A.; Owczuk, R.; Parczewski, M.; Pawłowska, M.; Piekarska, A.; Simon, K.; et al. Management of SARS-CoV-2 Infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of February 23, 2022. Pol. Arch. Intern. Med. 2022, 132, 16230. [Google Scholar] [CrossRef]
- Genomic Epidemiology of SARS-CoV-2 with Subsampling Focused on Europe Since Pandemic Start. Available online: https://nextstrain.org/ncov/gisaid/europe/ (accessed on 14 October 2022).
- Hoang, V.-T.; Colson, P.; Levasseur, A.; Delerce, J.; Lagier, J.-C.; Parola, P.; Million, M.; Fournier, P.-E.; Raoult, D.; Gautret, P. Clinical Outcomes in Patients Infected with Different SARS-CoV-2 Variants at One Hospital during Three Phases of the COVID-19 Epidemic in Marseille, France. Infect. Genet. Evol. 2021, 95, 105092. [Google Scholar] [CrossRef]
- Zarębska-Michaluk, D.; Jaroszewicz, J.; Rogalska, M.; Lorenc, B.; Rorat, M.; Szymanek-Pasternak, A.; Piekarska, A.; Berkan-Kawińska, A.; Sikorska, K.; Tudrujek-Zdunek, M.; et al. Impact of Kidney Failure on the Severity of COVID-19. J. Clin. Med. 2021, 10, 2042. [Google Scholar] [CrossRef]
- Zarębska-Michaluk, D.; Jaroszewicz, J.; Rogalska, M.; Martonik, D.; Pabjan, P.; Berkan-Kawińska, A.; Bolewska, B.; Oczko-Grzesik, B.; Kozielewicz, D.; Tudrujek-Zdunek, M.; et al. Effectiveness of Tocilizumab with and without Dexamethasone in Patients with Severe COVID-19: A Retrospective Study. J. Inflamm. Res. 2021, 14, 3359–3366. [Google Scholar] [CrossRef]
- Consolazio, D.; Murtas, R.; Tunesi, S.; Lamberti, A.; Senatore, S.; Faccini, M.; Russo, A.G. A Comparison Between Omicron and Earlier COVID-19 Variants’ Disease Severity in the Milan Area, Italy. Front. Epidemiol. 2022, 2, 891162. [Google Scholar] [CrossRef]
- Wang, L.; Berger, N.A.; Kaelber, D.C.; Davis, P.B.; Volkow, N.D.; Xu, R. Comparison of Outcomes from COVID Infection in Pediatric and Adult Patients before and after the Emergence of Omicron. medRxiv, 2022; preprint. [Google Scholar] [CrossRef]
- Abdullah, F.; Myers, J.; Basu, D.; Tintinger, G.; Ueckermann, V.; Mathebula, M.; Ramlall, R.; Spoor, S.; de Villiers, T.; Van der Walt, Z.; et al. Decreased Severity of Disease during the First Global Omicron Variant COVID-19 Outbreak in a Large Hospital in Tshwane, South Africa. Int. J. Infect. Dis. 2022, 116, 38–42. [Google Scholar] [CrossRef]
- Bager, P.; Wohlfahrt, J.; Bhatt, S.; Stegger, M.; Legarth, R.; Møller, C.H.; Skov, R.L.; Valentiner-Branth, P.; Voldstedlund, M.; Fischer, T.K.; et al. Risk of Hospitalisation Associated with Infection with SARS-CoV-2 Omicron Variant versus Delta Variant in Denmark: An Observational Cohort Study. Lancet Infect. Dis. 2022, 22, 967–976. [Google Scholar] [CrossRef]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative Analysis of the Risks of Hospitalisation and Death Associated with SARS-CoV-2 Omicron (B.1.1.529) and Delta (B.1.617.2) Variants in England: A Cohort Study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- Pia, L.; Rowland-Jones, S. Omicron Entry Route. Nat. Rev. Immunol. 2022, 22, 144. [Google Scholar] [CrossRef] [PubMed]
- Taytard, J.; Prevost, B.; Schnuriger, A.; Aubertin, G.; Berdah, L.; Bitton, L.; Dupond-Athenor, A.; Thouvenin, G.; Nathan, N.; Corvol, H. SARS-CoV-2 B.1.1.529 (Omicron) Variant Causes an Unprecedented Surge in Children Hospitalizations and Distinct Clinical Presentation Compared to the SARS-CoV-2 B.1.617.2 (Delta) Variant. Front. Pediatr. 2022, 10, 932170. [Google Scholar] [CrossRef] [PubMed]
- Marks, K.J.; Whitaker, M.; Anglin, O.; Milucky, J.; Patel, K.; Pham, H.; Chai, S.J.; Kirley, P.D.; Armistead, I.; McLafferty, S.; et al. Hospitalizations of Children and Adolescents with Laboratory-Confirmed COVID-19-COVID-NET, 14 States, July 2021-January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Lauring, A.S.; Tenforde, M.W.; Chappell, J.D.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Clinical Severity of, and Effectiveness of MRNA Vaccines against, COVID-19 from Omicron, Delta, and Alpha SARS-CoV-2 Variants in the United States: Prospective Observational Study. Br. Med. J. 2022, 376, e069761. [Google Scholar] [CrossRef] [PubMed]
- ECDC COVID-19 Vaccine Tracker. Available online: https://vaccinetracker.ecdc.europa.eu/public/extensions/COVID-19/vaccine-tracker.html (accessed on 24 December 2022).
- Modes, M.E.; Directo, M.P.; Melgar, M.; Johnson, L.R.; Yang, H.; Chaudhary, P.; Bartolini, S.; Kho, N.; Noble, P.W.; Isonaka, S.; et al. Clinical Characteristics and Outcomes Among Adults Hospitalized with Laboratory-Confirmed SARS-CoV-2 Infection During Periods of B.1.617.2 (Delta) and B.1.1.529 (Omicron) Variant Predominance—One Hospital, California, July 15–September 23, 2021, and December 21, 2021–January 27, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 217–223. [Google Scholar] [CrossRef]
- Bhakta, S.; Sanghavi, D.K.; Johnson, P.W.; Kunze, K.L.; Neville, M.R.; Wadei, H.M.; Bosch, W.; Carter, R.E.; Shah, S.Z.; Pollock, B.D.; et al. Clinical and Laboratory Profiles of the SARS-CoV-2 Delta Variant Compared with Pre-Delta Variants. Int. J. Infect. Dis. 2022, 120, 88–95. [Google Scholar] [CrossRef]
- Lippi, G.; Nocini, R.; Henry, B.M. Analysis of Online Search Trends Suggests That SARS-CoV-2 Omicron (B.1.1.529) Variant Causes Different Symptoms. J. Infect. 2022, 84, e76–e77. [Google Scholar] [CrossRef]
- Taylor, C.A.; Whitaker, M.; Anglin, O.; Milucky, J.; Patel, K.; Pham, H.; Chai, S.J.; Alden, N.B.; Yousey-Hindes, K.; Anderson, E.J.; et al. COVID-19-Associated Hospitalizations Among Adults During SARS-CoV-2 Delta and Omicron Variant Predominance, by Race/Ethnicity and Vaccination Status-COVID-NET, 14 States, July 2021–January 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 466–473. [Google Scholar] [CrossRef]
- Yuasa, S.; Nakajima, J.; Takatsuki, Y.; Takahashi, Y.; Tani-Sassa, C.; Iwasaki, Y.; Nagano, K.; Sonobe, K.; Yoshimoto, T.; Nukui, Y.; et al. Viral Load of SARS-CoV-2 Omicron Is Not High despite Its High Infectivity. J. Med. Virol. 2022, 94, 5543–5546. [Google Scholar] [CrossRef]
- Laitman, A.M.; Lieberman, J.A.; Hoffman, N.G.; Roychoudhury, P.; Mathias, P.C.; Greninger, A.L. The SARS-CoV-2 Omicron Variant Does Not Have Higher Nasal Viral Loads Compared to the Delta Variant in Symptomatic and Asymptomatic Individuals. J. Clin. Microbiol. 2022, 60, e0013922. [Google Scholar] [CrossRef] [PubMed]
- Puhach, O.; Adea, K.; Hulo, N.; Sattonnet, P.; Genecand, C.; Iten, A.; Jacquérioz, F.; Kaiser, L.; Vetter, P.; Eckerle, I.; et al. Infectious Viral Load in Unvaccinated and Vaccinated Individuals Infected with Ancestral, Delta or Omicron SARS-CoV-2. Nat. Med. 2022, 28, 1491–1500. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Zhou, L.; Mo, M.; Liu, T.; Wu, C.; Gong, C.; Lu, K.; Gong, L.; Zhu, W.; Xu, Z. SARS-CoV-2 Omicron RBD Shows Weaker Binding Affinity than the Currently Dominant Delta Variant to Human ACE2. Signal Transduct. Target Ther. 2022, 7, 8. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, R.; Yamasoba, D.; Kimura, I.; Wang, L.; Kishimoto, M.; Ito, J.; Morioka, Y.; Nao, N.; Nasser, H.; Uriu, K.; et al. Attenuated Fusogenicity and Pathogenicity of SARS-CoV-2 Omicron Variant. Nature 2022, 603, 700–705. [Google Scholar] [CrossRef]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal Dynamics in Viral Shedding and Transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [Green Version]
- Peacock, T.P.; Brown, J.C.; Zhou, J.; Thakur, N.; Sukhova, K.; Newman, J.; Kugathasan, R.; Yan, A.W.C.; Furnon, W.; Lorenzo, G.D.; et al. The Altered Entry Pathway and Antigenic Distance of the SARS-CoV-2 Omicron Variant Map to Separate Domains of Spike Protein. bioRxiv 2022. [Google Scholar] [CrossRef]
- Meng, B.; Abdullahi, A.; Ferreira, I.A.T.M.; Goonawardane, N.; Saito, A.; Kimura, I.; Yamasoba, D.; Gerber, P.P.; Fatihi, S.; Rathore, S.; et al. Altered TMPRSS2 Usage by SARS-CoV-2 Omicron Impacts Infectivity and Fusogenicity. Nature 2022, 603, 706–714. [Google Scholar] [CrossRef]
- Oude Munnink, B.B.; Sikkema, R.S.; Nieuwenhuijse, D.F.; Molenaar, R.J.; Munger, E.; Molenkamp, R.; van der Spek, A.; Tolsma, P.; Rietveld, A.; Brouwer, M.; et al. Transmission of SARS-CoV-2 on Mink Farms between Humans and Mink and Back to Humans. Science 2021, 371, 172–177. [Google Scholar] [CrossRef]
- Hoffmann, M.; Zhang, L.; Krüger, N.; Graichen, L.; Kleine-Weber, H.; Hofmann-Winkler, H.; Kempf, A.; Nessler, S.; Riggert, J.; Winkler, M.S.; et al. SARS-CoV-2 Mutations Acquired in Mink Reduce Antibody-Mediated Neutralization. Cell Rep. 2021, 35, 109017. [Google Scholar] [CrossRef]
- Domańska-Blicharz, K.; Orłowska, A.; Smreczak, M.; Niemczuk, K.; Iwan, E.; Bomba, A.; Lisowska, A.; Opolska, J.; Trębas, P.; Potyrało, P.; et al. Mink SARS-CoV-2 Infection in Poland-Short Communication. J. Vet. Res. 2021, 65, 1–5. [Google Scholar] [CrossRef]
- Palmer, M.V.; Martins, M.; Falkenberg, S.; Buckley, A.; Caserta, L.C.; Mitchell, P.K.; Cassmann, E.D.; Rollins, A.; Zylich, N.C.; Renshaw, R.W.; et al. Susceptibility of White-Tailed Deer (Odocoileus virginianus) to SARS-CoV-2. J. Virol. 2021, 95, e00083-21. [Google Scholar] [CrossRef] [PubMed]
- Chandler, J.C.; Bevins, S.N.; Ellis, J.W.; Linder, T.J.; Tell, R.M.; Jenkins-Moore, M.; Root, J.J.; Lenoch, J.B.; Robbe-Austerman, S.; DeLiberto, T.J.; et al. SARS-CoV-2 Exposure in Wild White-Tailed Deer (Odocoileus virginianus). Proc. Natl. Acad. Sci. USA 2021, 118, e2114828118. [Google Scholar] [CrossRef] [PubMed]
- Kuchipudi, S.V.; Surendran-Nair, M.; Ruden, R.M.; Yon, M.; Nissly, R.H.; Vandegrift, K.J.; Nelli, R.K.; Li, L.; Jayarao, B.M.; Maranas, C.D.; et al. Multiple Spillovers from Humans and Onward Transmission of SARS-CoV-2 in White-Tailed Deer. Proc. Natl. Acad. Sci. USA 2022, 119, e2121644119. [Google Scholar] [CrossRef] [PubMed]
- Ellwanger, J.H.; Chies, J.A.B. Zoonotic Spillover: Understanding Basic Aspects for Better Prevention. Genet. Mol. Biol. 2021, 44, e20200355. [Google Scholar] [CrossRef] [PubMed]
- Halabowski, D.; Rzymski, P. Taking a Lesson from the COVID-19 Pandemic: Preventing the Future Outbreaks of Viral Zoonoses through a Multi-Faceted Approach. Sci. Total Environ. 2021, 757, 143723. [Google Scholar] [CrossRef] [PubMed]
- Iuliano, A.D.; Brunkard, J.M.; Boehmer, T.K.; Peterson, E.; Adjei, S.; Binder, A.M.; Cobb, S.; Graff, P.; Hidalgo, P.; Panaggio, M.J.; et al. Trends in Disease Severity and Health Care Utilization During the Early Omicron Variant Period Compared with Previous SARS-CoV-2 High Transmission Periods-United States, December 2020-January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 146–152. [Google Scholar] [CrossRef]
- Rzymski, P.; Poniedziałek, B.; Rosińska, J.; Rogalska, M.; Zarębska-Michaluk, D.; Rorat, M.; Moniuszko-Malinowska, A.; Lorenc, B.; Kozielewicz, D.; Piekarska, A.; et al. The Association of Airborne Particulate Matter and Benzo[a]Pyrene with the Clinical Course of COVID-19 in Patients Hospitalized in Poland. Environ. Pollut. 2022, 306, 119469. [Google Scholar] [CrossRef]
- Rzymski, P.; Poniedziałek, B.; Rosińska, J.; Ciechanowski, P.; Peregrym, M.; Pokorska-Śpiewak, M.; Talarek, E.; Zaleska, I.; Frańczak-Chmura, P.; Pilarczyk, M.; et al. Air Pollution Might Affect the Clinical Course of COVID-19 in Pediatric Patients. Ecotoxicol. Environ. Saf. 2022, 239, 113651. [Google Scholar] [CrossRef]


{kind=link}
| Pre-Delta 1 March 2020–30 June 2021 N = 7742 | Delta 1 July 2021–31 December 2021 N = 2929 | p Delta vs. Pre-Delta | Omicron 1 January 2022–30 June 2022 N = 1227 | p Omicron vs. Delta | |
|---|---|---|---|---|---|
| Females/males, n (%) | 3515/4227 (45.4/54.6) | 1455/1474 (49.7/50.3) | p < 0.001 (χ2 = 15.6) | 620/607 (50.5/49.5) | p > 0.05 (χ2 =0.25) |
| Age (years), mean (SD) | 56.7 (22.8) | 57.1 (26.0) | p > 0.05 (t = −0.87) | 53.1 (32.2) | p < 0.001 (t = −4.2) |
| Age of the deceased (years), mean (SD) | 75.2 (12.2) | 77.0 (13.0) | p = 0.03 (t = −2.2) | 78.0 (13.3) | p > 0.05 (t = 0.76) |
| Number and percentage of patients in age groups (years), n (%) | |||||
| <20 | 837 (10.8) | 376 (12.8) | p = 0.03 (χ2 = 8.7) | 296 (24.1) | p < 0.001 (χ2 = 81.3) |
| 20–40 | 723 (9.3) | 316 (10.8) | p = 0.02 (χ2 = 5.1) | 101 (8.2) | p = 0.01 (χ2 = 6.2) |
| 40–60 | 2 127 (27.5) | 607 (20.7) | p < 0.001 (χ2 = 50.8) | 135 (11.0) | p < 0.001 (χ2 = 55.7) |
| 60–80 | 3 090 (39.9) | 1072 (36.6) | p = 0.002 (χ2 = 9.8) | 405 (33.0) | p = 0.03 (χ2 = 4.9 |
| >80 | 965 (12.5) | 558 (19.1) | p < 0.001 (χ2 = 75.3) | 290 (23.6) | p < 0.001 (χ2 = 11.2) |
| Presence of comorbidities *, n (%) | |||||
| Among all patients | 5503 (71.1) | 2038 (68.6) | p < 0.001 (χ2 = 40.6) | 896 (73.0) | p = 0.03 (χ2 = 4.9) |
| Among the deceased | 718/760 (94.5) | 336/358 (93.9) | p > 0.05 (χ2 = 1.0) | 113/118 (95.8) | p > 0.05 (χ2 = 0.9) |
| Parameters | Pre-Delta 1 March 2020–30 June 2021 N = 7742 | Delta 1 July 2021–31 December 2021 N = 2929 | Delta vs. Pre-Delta | Omicron 1 January 2022–30 June 2022 N = 1227 | Omicron vs. Delta |
|---|---|---|---|---|---|
| Need for oxygen therapy, n (%) | 3849 (49.7) | 1675 (57.2) | p < 0.001 (χ2 = 47.5) | 451 (36.8) | p < 0.001 (χ2 = 144.5) |
| Need for mechanical ventilation, n (%) | 441 (5.7) | 197 (6.7) | p = 0.04 (χ2 = 4.0) | 29 (2.4) | p < 0.001 (χ2 = 32.0) |
| Baseline SpO2 * < 91% or ARDS **, n (%) | 2494 (32.2) | 1131 (38.6) | p < 0.001 (χ2 = 38.8) | 302 (24.6) | p < 0.001 (χ2 = 75.0) |
| Length of hospitalization, mean (SD) | 11.7 (8.5) | 11.2 (7.9) | p = 0.008 (t = 2.7) | 9.3 (8.7) | p < 0.001 (t = 6.8) |
| Clinical status at the admission to the hospital, n (%) | |||||
| Asymptomatic | 400 (5.2) | 53 (1.8) | p < 0.001 (χ2 = 143.1) | 54 (4.4) | p < 0.001 (χ2 = 23.2) |
| SpO2 1 > 95% | 2343 (30.3) | 724 (24.7) | p < 0.001 (χ2 = 31.9) | 552 (45.0) | p < 0.001 (χ2 = 167.0) |
| SpO2 1 91–95% | 2342 (30.3) | 946 (32.3) | p = 0.04 (χ2 = 3.9) | 300 (24.5) | p < 0.001 (χ2 = 25.3) |
| SpO2 1 < 91% | 2429 (31.4) | 1073 (36.7) | p < 0.001 (χ2 = 26.7) | 292 (23.8) | p < 0.001 (χ2 = 65.6) |
| ARDS 2 | 65 (0.8) | 57 (1.9) | p < 0.001 (χ2 = 23.0) | 10 (0.8) | p = 0.008 (χ2 = 7.0) |
| Unknown | 163 (2.1) | 76 (2.6) | p > 0.05 (χ2 = 2.3) | 19 (1.5) | p = 0.04 (χ2 = 4.2) |
| The most common symptoms, n (%) | |||||
| Cough | 4876 (63.0) | 2087 (71.3) | p < 0.001 (χ2 = 64.1) | 582 (47.4) | p < 0.001 (χ2 = 213.5) |
| Fever | 5441 (70.3) | 2026 (69.2) | p > 0.05 (χ2 = 1.2) | 677 (55.2) | p < 0.001 (χ2 = 74.5) |
| Dyspnoea | 3803 (49.1) | 1568 (53.5) | p < 0.001 (χ2 = 16.5) | 356 (29.0) | p < 0.001 (χ2 = 209.1) |
| Loss of smell and taste | 952 (12.3) | 214 (7.3) | p < 0.001 (χ2 = 54.4) | 28 (2.3) | p < 0.001 (χ2 = 39.8) |
| Diarhoea | 898 (11.6) | 400 (13.7) | p = 0.004 (χ2 = 8.4) | 159 (13.0) | p > 0.05 (χ2 = 0.3) |
| Headache | 1012 (13.1) | 347 (11.8) | p > 0.05 (χ2 = 2.9) | 93 (7.6) | p < 0.001 (χ2 = 16.6) |
| Nausea | 500 (6.5) | 217 (7.4) | p > 0.05 (χ2 = 3.1) | 80 (6.5) | p > 0.05 (χ2 = 1.0) |
| Vomiting | 410 (5.3) | 218 (7.4) | p < 0.001 (χ2 = 17.8) | 150 (12.2) | p < 0.001 (χ2 = 24.5) |
| Fatigue | 2880 (37.2) | 1441 (49.2) | p < 0.001 (χ2 = 127.0) | 330 (26.9) | p < 0.001 (χ2 = 175.0) |
| Pre-Delta 1 March 2020–30 June 2021 N = 7371 | Delta 1 July 2021–31 December 2021 N = 2699 | Delta vs. Pre-Delta | Omicron 1 January 2022–30 June 2022 N = 1220 | Omicron vs. Delta | |
|---|---|---|---|---|---|
| 7 days, n (%) | 1349 (18.3) | 526 (19.5) | p > 0.05 (χ2 = 1.8) | 446 (36.5) | p < 0.001 (χ2 = 131.2) |
| 14 days, n (%) | 4255 (57.7) | 1361 (50.5) | p < 0.001 (χ2 = 42.7) | 878 (71.9) | p < 0.001 (χ2 = 159.2) |
| 21 days, n (%) | 5487 (74.4) | 1747 (64.8) | p < 0.001 (χ2 = 92.1) | 1000 (82.0) | p < 0.001 (χ2 = 119.1) |
| 28 days, n (%) | 6079 (82.5) | 2083 (77.2) | p < 0.001 (χ2 = 36.1) | 1041 (85.3) | p < 0.001 (χ2 = 34.5) |
| Parameters | Pre-Delta 1 March 2020–30 June 2021 | Delta 1 July 2021–31 December 2021 | Delta vs. Pre-Delta | Omicron 1 January 2022–30 June 2022 | Omicron vs. Delta |
|---|---|---|---|---|---|
| Overall 28-day mortality 1, n (%) | 761/7371 (10.3) | 359/2699 (13.3) | p < 0.001 (χ2 = 14.0) | 119/1220 (9.8) | p = 0.005 (χ2 = 7.8) |
| Age-related mortality (years), n/N (%) | |||||
| <60 | 69/3542 (1.9) | 37/1260 (2.9) | p = 0.04 (χ2 = 4.0) | 9/512 (1.7) | p > 0.05 (χ2 = 1.9) |
| 60–80 | 426/3118 (13.7) | 199/1062 (18.7) | p < 0.001 (χ2 = 11.6) | 49/390 (12.6) | p = 0.02 (χ2 = 5.6) |
| >80 | 340/1082 (31.4) | 254/607 (41.8) | p < 0.001 (χ2 = 8.7) | 74/316 (23.4) | p < 0.001 (χ2 = 15.4) |
| Mortality in subpopulations most at risk of death, n/N (%) | |||||
| SpO2 < 91% | 561/2429 (23.1) | 333/1074 (31.0) | p < 0.001 (χ2 = 14.2) | 74/292 (25.3) | p > 0.05 (χ2 = 2.0) |
| Age >80 years +SpO2 < 91% +hypertension | 164/359 (45.7) | 131/221 (59.3) | p > 0.05 (χ2 = 3.2) | 26/82 (31.7) | p = 0.01 (χ2 = 6.4) |
| Age > 80 years +SpO2 < 91% +COPD 2 | 16/40 (40.0) | 17/31 (54.8) | p > 0.05 (χ2 = 0.6) | 7/17 (41.2) | p > 0.05 (χ2 = 0.3) |
| Age > 80 years +SpO2 < 91% +diabetes | 69/150 (46.0) | 70/96 (72.9) | p = 0.03 (χ2 = 4.7) | 19/40 (47.5) | p > 0.05 (χ2 = 1.8) |
| Age > 80 years +SpO2 < 91% +neoplasm | 24/41 (58.5) | 13/21 (61.9) | p > 0.05 (χ2 = 0.02) | 9/14 (64.3) | p > 0.05 (χ2 = 0.01) |
| Age > 80 years +SpO2 < 91% +CIHD 3 | 81/153 (52.9) | 53/82 (64.6) | p > 0.05 (χ2 = 0.8) | 13/31 (41.9) | p > 0.05 (χ2 = 1.3) |
| BA1 N = 812 | BA2 N = 408 | p | |
|---|---|---|---|
| Age (years), mean (SD) | 50.0 (32.0) | 59.1 (31.5) | p < 0.001 (t = 4.8) |
| SpO2 < 91% or ARDS, n (%) | 194 (23.9) | 106 (26.0) | p > 0.05 (χ2 = 0.6) |
| comorbidities, n (%) | 579 (71.3) | 315 (77.2) | p = 0.03 (χ2 = 4.8) |
| cough, n (%) | 382 (47.0) | 196 (48.0) | p > 0.05 (χ2 = 0.1) |
| fever, n (%) | 452 (55.7) | 224 (54.9) | p > 0.05 (χ2 = 0.1) |
| dyspnoea, n (%) | 212 (26.1) | 140 (34.3) | p = 0.003 (χ2 = 8.9) |
| need for oxygen therapy, n (%) | 301 (37.1) | 149 (36.5) | p > 0.05 (χ2 = 0.1) |
| need for mechanical ventilation, n (%) | 20 (2,5) | 9 (2,2) | p > 0.05 (χ2 = 0.1) |
| discharge within 7 days, n (%) | 318 (39.2) | 128 (31.4) | p = 0.008 (χ2 = 7.1) |
| discharge within 14 days, n (%) | 582 (71.7) | 296 (72.5) | p > 0.05 (χ2 = 0.1) |
| discharge within 21 days, n (%) | 667 (82.1) | 333 (81.6) | p > 0.05 (χ2 = 0.1) |
| discharge within 28 days, n (%) | 697 (85.8) | 344 (84.3) | p > 0.05 (χ2 = 0.5) |
| 28-day mortality, n (%) | 73 (9.0) | 46 (11.3) | p > 0.05 (χ2 = 1.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flisiak, R.; Rzymski, P.; Zarębska-Michaluk, D.; Ciechanowski, P.; Dobrowolska, K.; Rogalska, M.; Jaroszewicz, J.; Szymanek-Pasternak, A.; Rorat, M.; Kozielewicz, D.; et al. Variability in the Clinical Course of COVID-19 in a Retrospective Analysis of a Large Real-World Database. Viruses 2023, 15, 149. https://doi.org/10.3390/v15010149
Flisiak R, Rzymski P, Zarębska-Michaluk D, Ciechanowski P, Dobrowolska K, Rogalska M, Jaroszewicz J, Szymanek-Pasternak A, Rorat M, Kozielewicz D, et al. Variability in the Clinical Course of COVID-19 in a Retrospective Analysis of a Large Real-World Database. Viruses. 2023; 15(1):149. https://doi.org/10.3390/v15010149
Chicago/Turabian StyleFlisiak, Robert, Piotr Rzymski, Dorota Zarębska-Michaluk, Przemysław Ciechanowski, Krystyna Dobrowolska, Magdalena Rogalska, Jerzy Jaroszewicz, Anna Szymanek-Pasternak, Marta Rorat, Dorota Kozielewicz, and et al. 2023. "Variability in the Clinical Course of COVID-19 in a Retrospective Analysis of a Large Real-World Database" Viruses 15, no. 1: 149. https://doi.org/10.3390/v15010149