
Clinical Severity in Different Waves of SARS-CoV-2 Infection in Sicily: A Model of Smith’s “Law of Declining Virulence” from Real-World Data

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
- Received the first dose of a COVID-19 vaccine before contracting SARS-CoV-2.
- Developed SARS-CoV-2 infection in the weeks where the predominance of a VOC was less than 80%.
2.2. Statistical Analysis
3. Results
3.1. Socio-Demographic and Clinical Characteristics
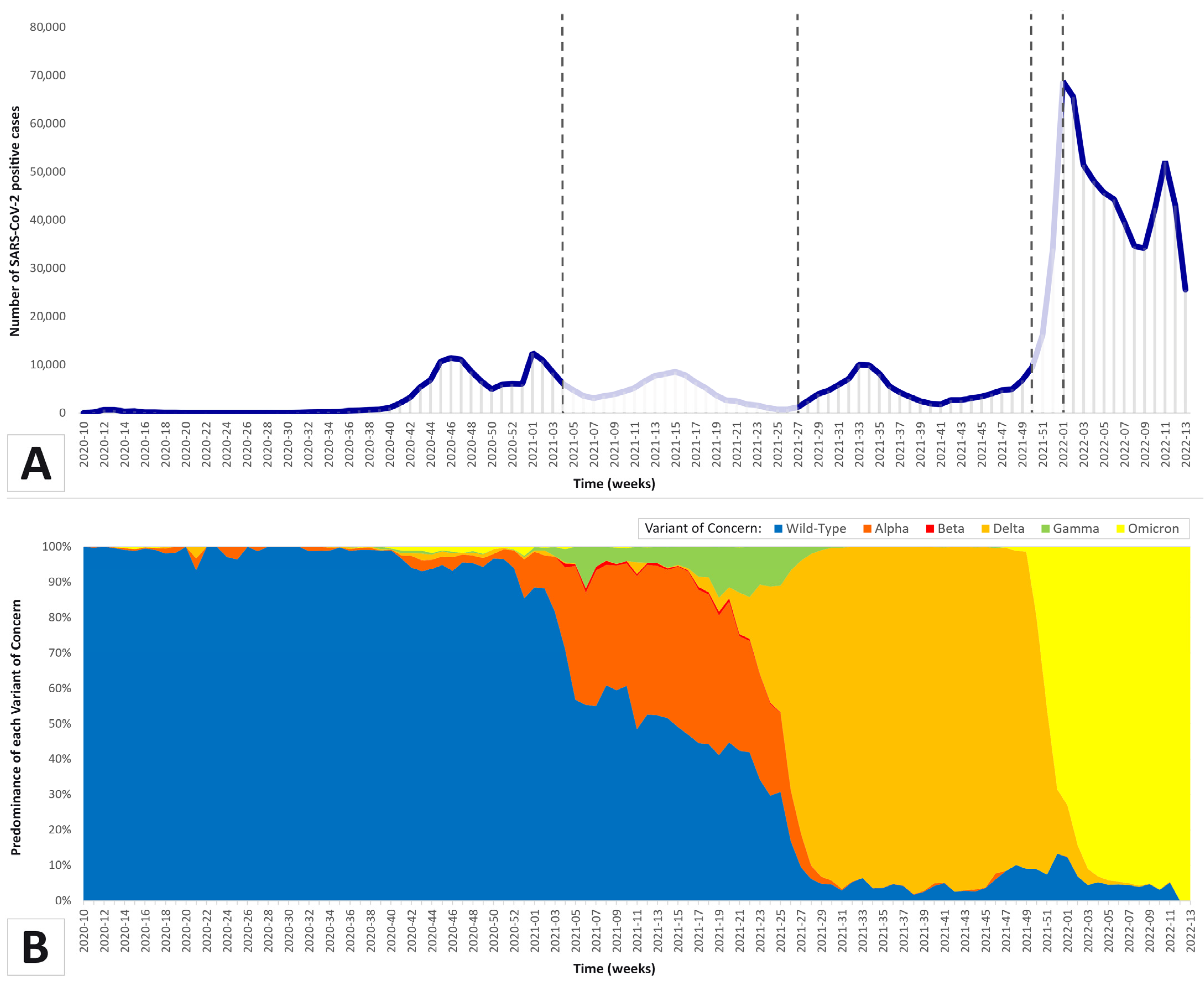
3.2. Predominance of SARS-CoV-2 VOCs and Number of Positive Cases per Week
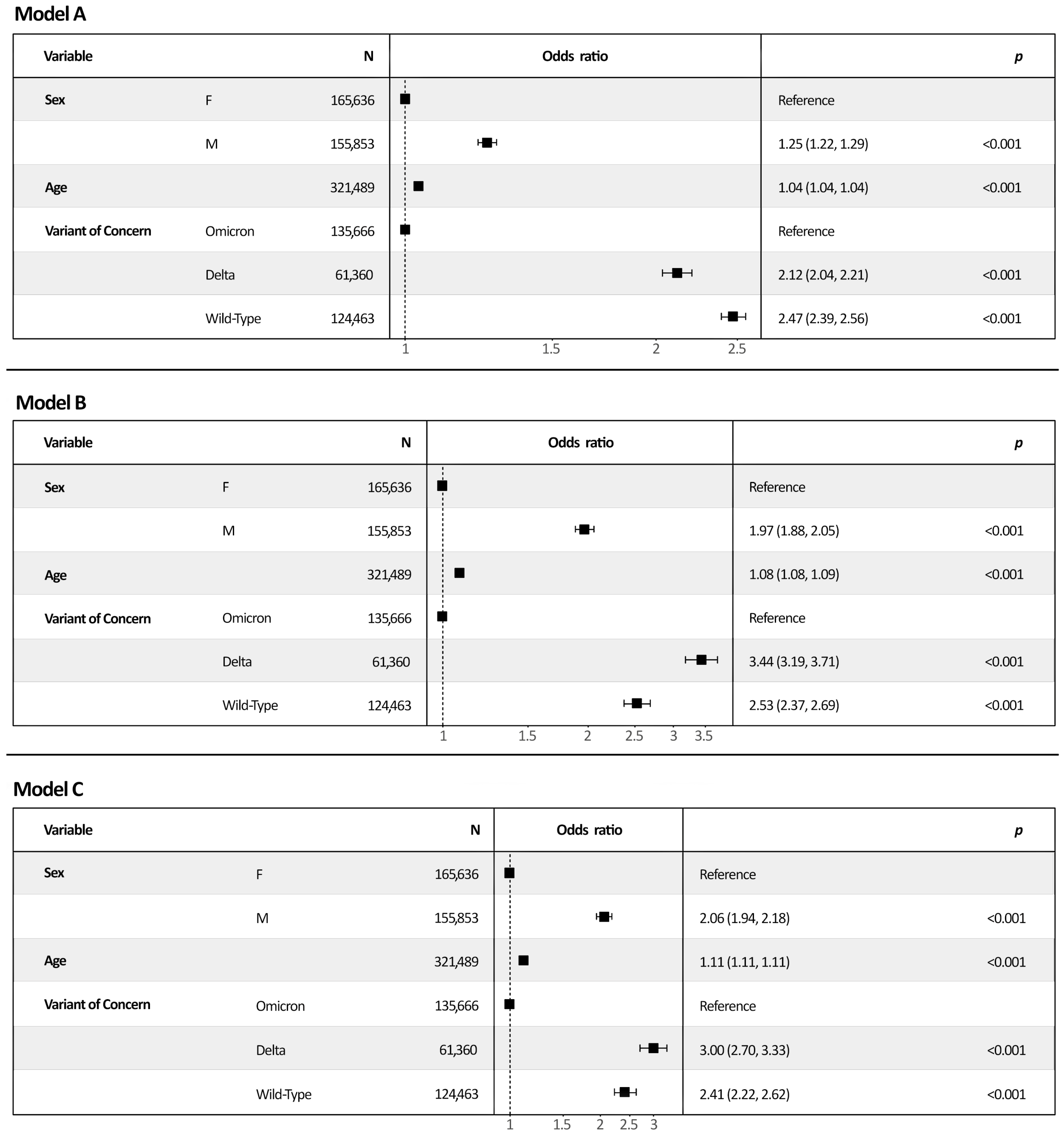
3.3. Multivariable Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Amodio, E.; Vitale, F.; Cimino, L.; Casuccio, A.; Tramuto, F. Outbreak of novel coronavirus (SARS-Cov-2): First evidences from international scientific literature and pending questions. Healthcare 2020, 8, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 28 October 2022).
- Istituto Superiore di Sanità. Available online: https://www.epicentro.iss.it/coronavirus (accessed on 28 October 2022).
- Open Data. Available online: https://opendatadpc.maps.arcgis.com/apps/dashboards/b0c68bce2cce478eaac82fe38d4138b1 (accessed on 28 October 2022).
- Ministero della Salute. Monitoraggio Covid-19 Numero 82-Regione Sicilia. Available online: https://www.salute.gov.it/portale/nuovocoronavirus/dettaglioMonitoraggioNuovoCoronavirus.jsp?lingua=italiano&menu=monitoraggi&id=91 (accessed on 23 December 2022).
- Ministero della Salute. Monitoraggio Covid-19 Numero 98-Regione Sicilia. Available online: https://www.salute.gov.it/portale/nuovocoronavirus/dettaglioMonitoraggioNuovoCoronavirus.jsp?lingua=italiano&menu=monitoraggi&id=108 (accessed on 23 December 2022).
- Istituto Superiore di Sanità. Monitoraggio Delle Varianti Del Virus SARS-CoV-2 Di Interesse in Sanità Pubblica in Italia-“Prevalenza e Distribuzione Delle Varianti Di SARS-CoV-2 Di Interesse per La Sanità Pubblica in Italia-Rapporton. 15 Del 10 Dicembre 2021”. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-monitoraggio-varianti-rapporti-periodici (accessed on 23 December 2022).
- Al Maqbali, M.; Al Badi, K.; Al Sinani, M.; Madkhali, N.; Dickens, G.L. Clinical features of COVID-19 patients in the first year of pandemic: A systematic review and meta-analysis. Biol. Res. Nurs. 2022, 24, 172–185. [Google Scholar] [CrossRef] [PubMed]
- Timelli, L.; Liuzzi, G. Association of COVID-19 case fatality rate with disease burden: An ecological analysis in Italy during the first wave. Int. J. Infect. Dis. 2021, 111, 186–189. [Google Scholar] [CrossRef]
- Chavda, V.P.; Prajapati, R.; Lathigara, D.; Nagar, B.; Kukadiya, J.; Redwan, E.M.; Uversky, V.N.; Kher, M.N.; Patel, R. Therapeutic monoclonal antibodies for COVID-19 management: An update. Expert Opin. Biol. Ther. 2022, 22, 763–780. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, R.L.; Nirula, A.; Chen, P.; Boscia, J.; Heller, B.; Morris, J.; Huhn, G.; Cardona, J.; Mocherla, B.; Stosor, V.; et al. Effect of Bamlanivimab as monotherapy or in combination with etesevimab on viral load in patients with mild to moderate COVID-19: A randomized clinical trial. JAMA 2021, 325, 632–644. [Google Scholar] [CrossRef]
- Cohen, M.S.; Nirula, A.; Mulligan, M.J.; Novak, R.M.; Marovich, M.; Yen, C.; Stemer, A.; Mayer, S.M.; Wohl, D.; Brengle, B.; et al. Effect of Bamlanivimab vs Placebo on incidence of COVID-19 among residents and staff of skilled nursing and assisted living facilities: A randomized clinical trial. JAMA 2021, 326, 46–55. [Google Scholar] [CrossRef]
- Simonovich, V.A.; Burgos Pratx, L.D.; Scibona, P.; Beruto, M.V.; Vallone, M.G.; Vázquez, C.; Savoy, N.; Giunta, D.H.; Pérez, L.G.; Sánchez, M.D.L.; et al. A randomized trial of convalescent plasma in COVID-19 severe pneumonia. N. Engl. J. Med. 2021, 384, 619–629. [Google Scholar] [CrossRef]
- Salian, V.S.; Wright, J.A.; Vedell, P.T.; Nair, S.; Li, C.; Kandimalla, M.; Tang, X.; Carmona Porquera, E.M.; Kalari, K.R.; Kandimalla, K.K. COVID-19 transmission, current treatment, and future therapeutic strategies. Mol. Pharm. 2021, 18, 754–771. [Google Scholar] [CrossRef]
- Italian Medicines Agency (AIFA). Determina n. 154/2020-Determinazione uso Umano Comirnaty. Available online: https://www.aifa.gov.it/en/comirnaty (accessed on 28 October 2022).
- Ministry of Health. Anti COVID-19 Vaccines Report. Available online: https://www.governo.it/it/cscovid19/report-vaccini (accessed on 28 October 2022).
- Italian Medicines Agency (AIFA). Determina n. 73/2021-Estensione Indicazioni Terapeutiche Comirnaty. Available online: https://www.aifa.gov.it/en/comirnaty (accessed on 28 October 2022).
- Epicentro, Comirnaty (BNT162b2), the First Vaccine Against COVID-19 Approved in Europe and Italy. Available online: https://www.epicentro.iss.it/vaccini/covid-19-vaccino-pfizer-biontech (accessed on 28 October 2022).
- Amicone, M.; Borges, V.; Alves, M.J.; Isidro, J.; Zé-Zé, L.; Duarte, S.; Vieira, L.; Guiomar, R.; Gomes, J.P.; Gordo, I. Mutation rate of SARS-CoV-2 and emergence of mutators during experimental evolution. Evol. Med. Public Health 2022, 10, 142–155. [Google Scholar] [CrossRef]
- Aleem, A.; Akbar Samad, A.B.; Slenker, A.K. Emerging Variants of SARS-CoV-2 and Novel Therapeutics against Coronavirus (COVID-19); StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Bonura, F.; Genovese, D.; Amodio, E.; Calamusa, G.; Sanfilippo, G.L.; Cacioppo, F.; Giammanco, G.M.; De Grazia, S.; Ferraro, D. Neutralizing antibodies response against SARS-CoV-2 variants of concern elicited by prior infection or mRNA BNT162b2 vaccination. Vaccines 2022, 10, 874. [Google Scholar] [CrossRef]
- World Health Organization. Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants (accessed on 28 October 2022).
- Méthot, P.O. Why do parasites harm their host? On the origin and legacy of Theobald Smith’s “law of declining virulence”—1900–1980. Hist. Philos. Life Sci. 2012, 34, 561–601. [Google Scholar]
- Alizon, S. A visionary pioneer of parasite ecology and evolution. Am. Nat. 2016, 187, ii–iii. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavine, J.S.; Bjornstad, O.N.; Antia, R. Immunological characteristics govern the transition of COVID-19 to endemicity. Science 2021, 371, 741–745. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). Data on SARS-CoV-2 Variants in the EU/EEA. Available online: https://www.ecdc.europa.eu/en/publications-data/data-virus-variants-covid-19-eueea (accessed on 28 October 2022).
- Istituto Superiore di Sanità. Sorveglianza Integrata COVID-19: I Principali Dati Nazionali. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-sorveglianza-dati (accessed on 23 December 2022).
- RStudio Team. RStudio: Integrated Development for R. RStudio; PBC: Boston, MA, USA, 2020. [Google Scholar]
- Asselah, T.; Durantel, D.; Pasmant, E.; Lau, G.; Schinazi, R.F. COVID-19: Discovery, diagnostics and drug development. J. Hepatol. 2021, 74, 168–184. [Google Scholar] [CrossRef] [PubMed]
- Callaway, E.; Ledford, H. How bad is Omicron? What scientists know so far. Nature 2021, 600, 197–199. [Google Scholar] [CrossRef]
- Liu, Y.; Yu, Y.; Zhao, Y.; He, D. Reduction in the infection fatality rate of Omicron variant compared with previous variants in South Africa. Int. J. Infect. Dis. 2022, 120, 146–149. [Google Scholar] [CrossRef]
- Xue, L.; Jing, S.; Zhang, K.; Milne, R.; Wang, H. Infectivity versus fatality of SARS-CoV-2 mutations and influenza. Int. J. Infect. Dis. 2022, 121, 195–202. [Google Scholar] [CrossRef]
- Mohiuddin, M.; Kasahara, K. Cellular senescence is a potential severity factor for COVID-19: Suitable targets required to eliminate cellular senescence. Respir. Med. 2021, 186, 106517. [Google Scholar] [CrossRef]
- Nehme, J.; Borghesan, M.; Mackedenski, S.; Bird, T.G.; Demaria, M. Cellular senescence as a potential mediator of COVID-19 severity in the elderly. Aging Cell 2020, 19, e13237. [Google Scholar] [CrossRef]
- Beaney, T.; Neves, A.L.; Alboksmaty, A.; Ashrafian, H.; Flott, K.; Fowler, A.; Benger, J.R.; Aylin, P.; Elkin, S.; Darzi, A.; et al. Trends and associated factors for Covid-19 hospitalisation and fatality risk in 2.3 million adults in England. Nat. Commun. 2022, 13, 2356. [Google Scholar] [CrossRef]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef] [PubMed]
- Diani, S.; Leonardi, E.; Cavezzi, A.; Ferrari, S.; Iacono, O.; Limoli, A.; Bouslenko, Z.; Natalini, D.; Conti, S.; Mantovani, M.; et al. SARS-CoV-2—The role of natural immunity: A narrative review. J. Clin. Med. 2022, 11, 6272. [Google Scholar] [CrossRef] [PubMed]
- Wolter, N.; Jassat, W.; Walaza, S.; Welch, R.; Moultrie, H.; Groome, M.; Amoako, D.G.; Everatt, J.; Bhiman, J.N.; Scheepers, C.; et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: A data linkage study. Lancet 2022, 399, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Nordström, P.; Ballin, M.; Nordström, A. Risk of SARS-CoV-2 reinfection and COVID-19 hospitalisation in individuals with natural and hybrid immunity: A retrospective, total population cohort study in Sweden. Lancet Infect. Dis. 2022, 22, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Lauring, A.S.; Tenforde, M.W.; Chappell, J.D.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Clinical severity of, and effectiveness of mRNA vaccines against, COVID-19 from omicron, delta, and alpha SARS-CoV-2 variants in the United States: Prospective observational study. BMJ 2022, 376, e069761. [Google Scholar] [CrossRef]
- Wang, L.; Berger, N.A.; Kaelber, D.C.; Davis, P.B.; Volkow, N.D.; Xu, R. Incidence Rates and Clinical Outcomes of SARS-CoV-2 Infection with the Omicron and Delta Variants in Children Younger Than 5 Years in the US. JAMA Pediatr. 2022, 176, 811–813. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Unvaccinated Population (n = 321,490) | |
|---|---|
Sex, n (%)
| 165,636 (51.5%) 155,854 (48.5%) |
| Age, Median (IQR) | 32 (11–52) |
Worst clinical outcome, n (%)
| 292,062 (90.9%) 19,044 (5.9%) 4502 (1.4%) 5882 (1.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amodio, E.; Genovese, D.; Fallucca, A.; Ferro, P.; Sparacia, B.; D’Azzo, L.; Fertitta, A.; Maida, C.M.; Vitale, F. Clinical Severity in Different Waves of SARS-CoV-2 Infection in Sicily: A Model of Smith’s “Law of Declining Virulence” from Real-World Data. Viruses 2023, 15, 125. https://doi.org/10.3390/v15010125
Amodio E, Genovese D, Fallucca A, Ferro P, Sparacia B, D’Azzo L, Fertitta A, Maida CM, Vitale F. Clinical Severity in Different Waves of SARS-CoV-2 Infection in Sicily: A Model of Smith’s “Law of Declining Virulence” from Real-World Data. Viruses. 2023; 15(1):125. https://doi.org/10.3390/v15010125
Chicago/Turabian StyleAmodio, Emanuele, Dario Genovese, Alessandra Fallucca, Patrizia Ferro, Benedetta Sparacia, Luciano D’Azzo, Angelo Fertitta, Carmelo Massimo Maida, and Francesco Vitale. 2023. "Clinical Severity in Different Waves of SARS-CoV-2 Infection in Sicily: A Model of Smith’s “Law of Declining Virulence” from Real-World Data" Viruses 15, no. 1: 125. https://doi.org/10.3390/v15010125