
Prevalence and Predictors of Liver Fibrosis in People Living with Hepatitis B in Senegal

Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Characteristics of Study Population
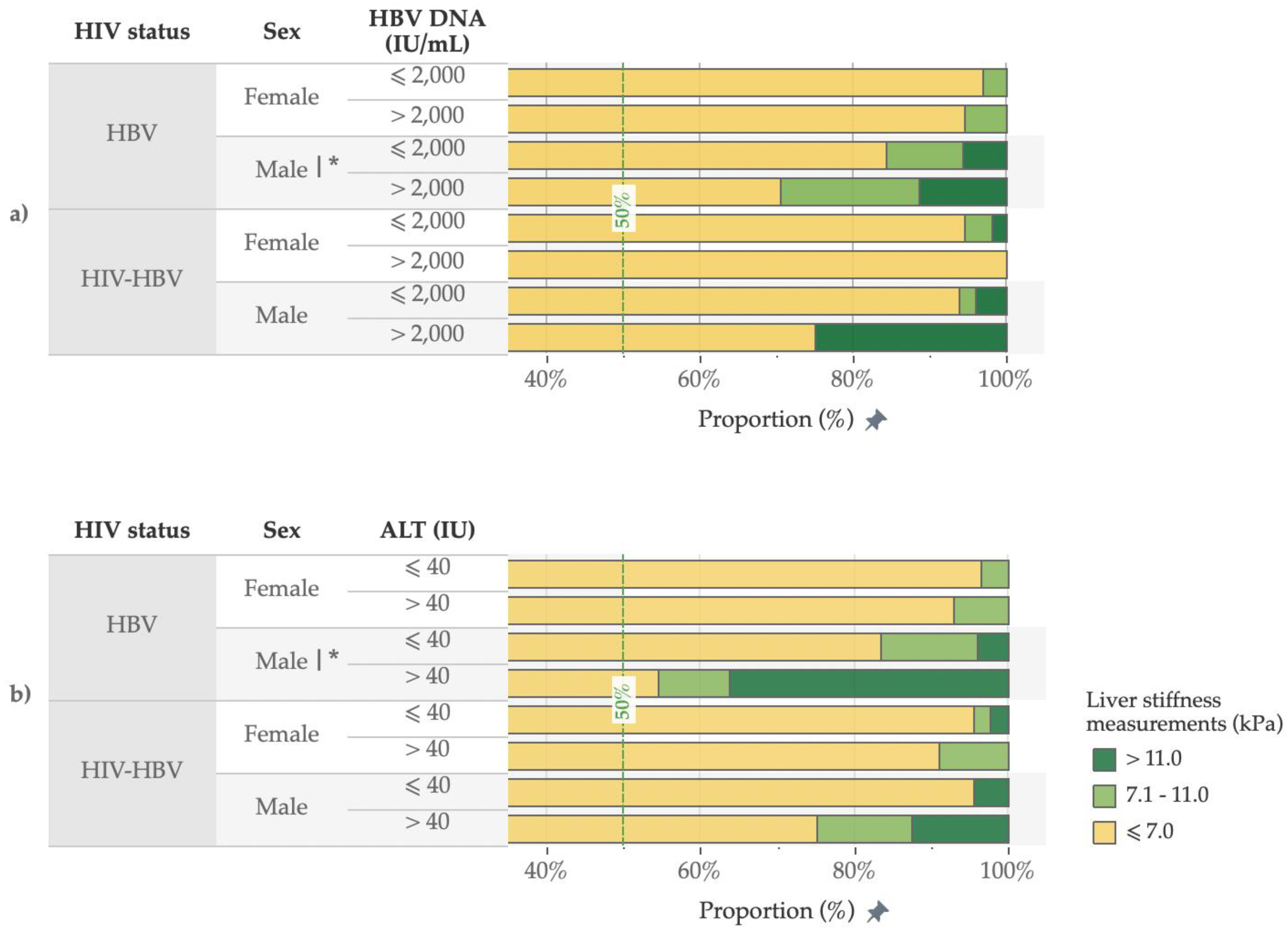
3.2. Prevalence of Significant Liver Fibrosis and Cirrhosis
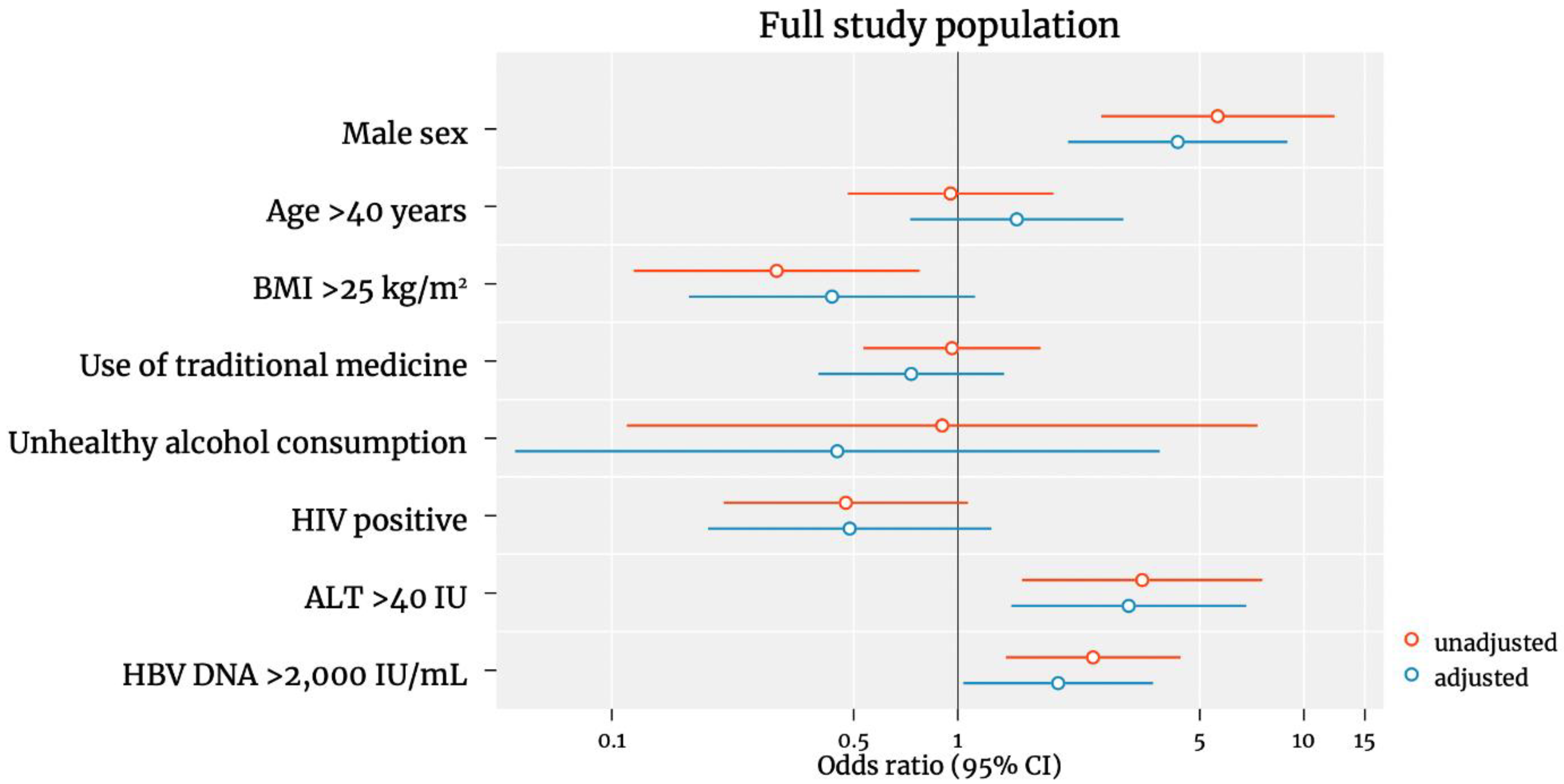
3.3. Risk Factors for Significant Fibrosis and Cirrhosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2017 Cirrhosis Collaborators. The Global, Regional, and National Burden of Cirrhosis by Cause in 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 245–266. [Google Scholar] [CrossRef] [Green Version]
- Mc Naughton, A.L.; Lourenço, J.; Bester, P.A.; Mokaya, J.; Lumley, S.F.; Obolski, U.; Forde, D.; Maponga, T.G.; Katumba, K.R.; Goedhals, D.; et al. Hepatitis B Virus Seroepidemiology Data for Africa: Modelling Intervention Strategies Based on a Systematic Review and Meta-Analysis. PLoS Med. 2020, 17, e1003068. [Google Scholar] [CrossRef] [Green Version]
- Surial, B.; Wyser, D.; Béguelin, C.; Ramírez-Mena, A.; Rauch, A.; Wandeler, G. Prevalence of Liver Cirrhosis in Individuals with Hepatitis B Virus Infection in Sub-Saharan Africa: Systematic Review and Meta-Analysis. Liver Int. 2021, 41, 710–719. [Google Scholar] [CrossRef] [PubMed]
- Kamal, H.; Fornes, R.; Simin, J.; Stål, P.; Duberg, A.-S.; Brusselaers, N.; Aleman, S. Risk of Hepatocellular Carcinoma in Hepatitis B and D Virus Co-Infected Patients: A Systematic Review and Meta-Analysis of Longitudinal Studies. J. Viral Hepat. 2021, 28, 1431–1442. [Google Scholar] [CrossRef]
- Kew, M.C. Aflatoxins as a Cause of Hepatocellular Carcinoma. J. Gastrointestin. Liver Dis. 2013, 22, 305–310. [Google Scholar] [PubMed]
- Khatami, A.; Bahadory, S.; Ghorbani, S.; Saadati, H.; Zarei, M.; Soleimani, A.; Zibaei, M. Two Rivals or Colleagues in the Liver? Hepatit B Virus and Schistosoma Mansoni Co-Infections: A Systematic Review and Meta-Analysis. Microb. Pathog. 2021, 154, 104828. [Google Scholar] [CrossRef]
- McNaughton, A.L.; Lemoine, M.; van Rensburg, C.; Matthews, P.C. Extending Treatment Eligibility for Chronic Hepatitis B Virus Infection. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 146–147. [Google Scholar] [CrossRef]
- Jeng, W.-J.; Lok, A.S. Should Treatment Indications for Chronic Hepatitis B Be Expanded? Clin. Gastroenterol. Hepatol. 2021, 19, 2006–2014. [Google Scholar] [CrossRef]
- Global Hepatitis Report. 2017. Available online: https://www.who.int/publications-detail-redirect/9789241565455 (accessed on 30 May 2022).
- Chen, C.-J.; Yang, H.-I.; Su, J.; Jen, C.-L.; You, S.-L.; Lu, S.-N.; Huang, G.-T.; Iloeje, U.H.; REVEAL-HBV Study Group. Risk of Hepatocellular Carcinoma across a Biological Gradient of Serum Hepatitis B Virus DNA Level. JAMA 2006, 295, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Iloeje, U.H.; Yang, H.-I.; Su, J.; Jen, C.-L.; You, S.-L.; Chen, C.-J.; Risk Evaluation of Viral Load Elevation and Associated Liver Disease/Cancer-In HBV (the REVEAL-HBV) Study Group. Predicting Cirrhosis Risk Based on the Level of Circulating Hepatitis B Viral Load. Gastroenterology 2006, 130, 678–686. [Google Scholar] [CrossRef]
- Ramírez Mena, A.; Tine, J.M.; Fortes, L.; Ndiaye, O.; Ka, D.; Ngom, N.F.; Ramette, A.; Bittel, P.; Seydi, M.; Wandeler, G. Hepatitis B Screening Practices and Viral Control among Persons Living with HIV in Urban Senegal. J. Viral Hepat. 2021, 29, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Boursier, J.; Zarski, J.-P.; de Ledinghen, V.; Rousselet, M.-C.; Sturm, N.; Lebail, B.; Fouchard-Hubert, I.; Gallois, Y.; Oberti, F.; Bertrais, S.; et al. Determination of Reliability Criteria for Liver Stiffness Evaluation by Transient Elastography. Hepatology 2013, 57, 1182–1191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Guidelines for the Prevention, Care and Treatment of Persons with Chronic Hepatitis B Infection. Available online: http://www.who.int/hepatitis/publications/hepatitis-b-guidelines/en/ (accessed on 24 August 2020).
- Bradley, K.A.; DeBenedetti, A.F.; Volk, R.J.; Williams, E.C.; Frank, D.; Kivlahan, D.R. AUDIT-C as a Brief Screen for Alcohol Misuse in Primary Care. Alcohol. Clin. Exp. Res. 2007, 31, 1208–1217. [Google Scholar] [CrossRef] [PubMed]
- Bush, K.; Kivlahan, D.R.; McDonell, M.B.; Fihn, S.D.; Bradley, K.A. The AUDIT Alcohol Consumption Questions (AUDIT-C): An Effective Brief Screening Test for Problem Drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch. Intern. Med. 1998, 158, 1789–1795. [Google Scholar] [CrossRef] [Green Version]
- Chan, H.L.-Y.; Wong, G.L.-H.; Choi, P.C.-L.; Chan, A.W.-H.; Chim, A.M.-L.; Yiu, K.K.-L.; Chan, F.K.-L.; Sung, J.J.-Y.; Wong, V.W.-S. Alanine Aminotransferase-Based Algorithms of Liver Stiffness Measurement by Transient Elastography (Fibroscan) for Liver Fibrosis in Chronic Hepatitis B. J. Viral Hepat. 2009, 16, 36–44. [Google Scholar] [CrossRef]
- Jann, B. Plotting Regression Coefficients and Other Estimates. Stata J. 2014, 14, 708–737. [Google Scholar] [CrossRef] [Green Version]
- Jann, B. Customizing Stata Graphs Made Easy (Part 2). Stata J. 2018, 18, 786–802. [Google Scholar] [CrossRef]
- Aberra, H.; Desalegn, H.; Berhe, N.; Mekasha, B.; Medhin, G.; Gundersen, S.G.; Johannessen, A. The WHO Guidelines for Chronic Hepatitis B Fail to Detect Half of the Patients in Need of Treatment in Ethiopia. J. Hepatol. 2019, 70, 1065–1071. [Google Scholar] [CrossRef] [PubMed]
- Mendy, M.E.; Welzel, T.; Lesi, O.A.; Hainaut, P.; Hall, A.J.; Kuniholm, M.H.; McConkey, S.; Goedert, J.J.; Kaye, S.; Rowland-Jones, S.; et al. Hepatitis B Viral Load and Risk for Liver Cirrhosis and Hepatocellular Carcinoma in The Gambia, West Africa. J. Viral Hepat 2010, 17, 115–122. [Google Scholar] [CrossRef] [Green Version]
- Wong, R.J.; Kaufman, H.W.; Niles, J.K.; Kapoor, H.; Gish, R.G. Simplifying Treatment Criteria in Chronic Hepatitis B: Reducing Barriers to Elimination. Clin. Infect. Dis. 2022, ciac385. [Google Scholar] [CrossRef]
- Wang, D.; Zhang, P.; Zhang, M. Predictors for Advanced Liver Fibrosis in Chronic Hepatitis B Virus Infection with Persistently Normal or Mildly Elevated Alanine Aminotransferase. Exp. Med. 2017, 14, 5363–5370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.-F.; Song, S.-H.; Lee, C.-S.; Chen, H.-L.; Ni, Y.-H.; Hsu, H.-Y.; Wu, T.-C.; Chang, M.-H. Clinical Predictors of Liver Fibrosis in Patients With Chronic Hepatitis B Virus Infection From Children to Adults. J. Infect. Dis. 2018, 217, 1408–1416. [Google Scholar] [CrossRef] [PubMed]
- Xiong, M.; Li, J.; Yang, S.; Zeng, F.; Ji, Y.; Liu, J.; Wu, Q.; He, Q.; Jiang, R.; Zhou, F.; et al. Influence of Gender and Reproductive Factors on Liver Fibrosis in Patients With Chronic Hepatitis B Infection. Clin. Transl. Gastroenterol. 2019, 10, e00085. [Google Scholar] [CrossRef]
- Hawkins, C.; Agbaji, O.; Ugoagwu, P.; Thio, C.L.; Auwal, M.M.; Ani, C.; Okafo, C.; Wallender, E.; Murphy, R.L. Assessment of Liver Fibrosis by Transient Elastography in Patients with HIV and Hepatitis B Virus Coinfection in Nigeria. Clin. Infect. Dis. 2013, 57, e189–e192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinikoor, M.J.; Sinkala, E.; Chilengi, R.; Mulenga, L.B.; Chi, B.H.; Zyambo, Z.; Hoffmann, C.J.; Saag, M.S.; Davies, M.-A.; Egger, M.; et al. Impact of Antiretroviral Therapy on Liver Fibrosis Among Human Immunodeficiency Virus-Infected Adults With and Without HBV Coinfection in Zambia. Clin. Infect. Dis. 2017, 64, 1343–1349. [Google Scholar] [CrossRef] [Green Version]
- Jaquet, A.; Wandeler, G.; Nouaman, M.; Ekouevi, D.K.; Tine, J.; Patassi, A.; Coffie, P.A.; Tanon, A.; Seydi, M.; Attia, A.; et al. Alcohol Use, Viral Hepatitis and Liver Fibrosis among HIV-Positive Persons in West Africa: A Cross-Sectional Study. J. Int. AIDS Soc. 2017, 19, 21424. [Google Scholar] [CrossRef]
- Stockdale, A.J.; Phillips, R.O.; Beloukas, A.; Appiah, L.T.; Chadwick, D.; Bhagani, S.; Bonnett, L.; Sarfo, F.S.; Dusheiko, G.; Geretti, A.M. Liver Fibrosis by Transient Elastography and Virologic Outcomes After Introduction of Tenofovir in Lamivudine-Experienced Adults With HIV and Hepatitis B Virus Coinfection in Ghana. Clin. Infect. Dis. 2015, 61, 883–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, J.L.; Agaba, P.; Ugoagwu, P.; Muazu, A.; Okpokwu, J.; Akpa, S.; Machenry, S.; Imade, G.; Agbaji, O.; Thio, C.L.; et al. Changes in Liver Stiffness after ART Initiation in HIV-Infected Nigerian Adults with and without Chronic HBV. J. Antimicrob. Chemother. 2019, 74, 2003–2008. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Huang, Y.-S.; Wang, Z.-Z.; Yang, Z.-R.; Sun, F.; Zhan, S.-Y.; Liu, X.-E.; Zhuang, H. Systematic Review with Meta-Analysis: The Diagnostic Accuracy of Transient Elastography for the Staging of Liver Fibrosis in Patients with Chronic Hepatitis B. Aliment. Pharm. 2016, 43, 458–469. [Google Scholar] [CrossRef]
- Abruzzi, A.; Fried, B.; Alikhan, S.B. Coinfection of Schistosoma Species with Hepatitis B or Hepatitis C Viruses. Adv. Parasitol. 2016, 91, 111–231. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Persons Living with HBV (n = 471) | Persons Living with HIV/HBV (n = 110) |
|---|---|---|
| Male sex, n (%) | 256 (54.4) | 52 (47.7) |
| Median age in years (IQR) * | 31 (25–39) | 46 (38–54) |
| BMI > 25 kg/m2, n (%) | 109 (24.4) | 24 (23.5) |
| Use of traditional medicine, n (%) * | 173 (36.7) | 28 (25.7) |
| Any alcohol consumption, n (%) | 23 (4.9) | 6 (5.5) |
| Unhealthy alcohol consumption, n (%) | 9 (1.9) | 3 (2.7) |
| Smoker, n (%) * | 9 (1.9) | 8 (7.3) |
| HCV Ab-positive, n (%) | 2 (0.8) | 0 (0) |
| HDV Ab-positive 1, n (%) | 1 (0.6) | 2 (2) |
| TDF-experienced, n (%) | 22 (4.7) | 100 (100) |
| Median ALT in IU (IQR) * | 17 (12–24) | 19 (13–34) |
| ALT > 40 (IU), n (%) * | 36 (7.8) | 19 (17.3) |
| Median HBV DNA in IU/mL (IQR) * | 547.5 (92–2600) | 0 (0) |
| HBV DNA undetectable, n (%) * | 76 (16.2) | 89 (83.2) |
| HBV DNA > 2000 (IU/mL), n (%) * | 133 (28.3) | 5 (4.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramírez Mena, A.; Ngom, N.F.; Tine, J.; Ndiaye, K.; Fortes, L.; Ndiaye, O.; Fall, M.; Gaye, A.; Ka, D.; Seydi, M.; et al. Prevalence and Predictors of Liver Fibrosis in People Living with Hepatitis B in Senegal. Viruses 2022, 14, 1614. https://doi.org/10.3390/v14081614
Ramírez Mena A, Ngom NF, Tine J, Ndiaye K, Fortes L, Ndiaye O, Fall M, Gaye A, Ka D, Seydi M, et al. Prevalence and Predictors of Liver Fibrosis in People Living with Hepatitis B in Senegal. Viruses. 2022; 14(8):1614. https://doi.org/10.3390/v14081614
Chicago/Turabian StyleRamírez Mena, Adrià, Ndeye Fatou Ngom, Judicaël Tine, Kine Ndiaye, Louise Fortes, Ousseynou Ndiaye, Maguette Fall, Assietou Gaye, Daye Ka, Moussa Seydi, and et al. 2022. "Prevalence and Predictors of Liver Fibrosis in People Living with Hepatitis B in Senegal" Viruses 14, no. 8: 1614. https://doi.org/10.3390/v14081614