
BK Virus Nephropathy in Kidney Transplantation: A State-of-the-Art Review


Abstract
:1. Introduction
2. History of the BK Virus
3. Virology
4. Epidemiology
- Intensity of immunosuppression: This is considered as the most significant factor associated with BK viral replication. This is based on the finding that the incidence of BK viremia is highest in the early post-transplant period given the magnitude of immunosuppression. Some but not all studies have demonstrated that tacrolimus may portend a higher risk of BK virus infection than cyclosporine, but this is confounded by the fact that cyclosporine inhibits enterohepatic recirculation of MMF and results in lower mycophenolic acid area under the curve [31,33,34,35], while mammalian target of rapamycin (mTOR) inhibitors may be associated with lower risk by virtue of being less immunosuppressive than tacrolimus or cyclosporine [36,37,38]. It is pertinent to note the presence of BK viremia reflects a higher level of immunosuppression and its occurrence with or without BKVAN is in the setting of all maintenance immunosuppressive agents/combinations [18,39,40,41,42,43,44,45].
5. Cellular Immune Response and Pathogenesis
6. Clinical Manifestations
7. Screening and Diagnosis
7.1. Urine BK PCR
7.2. Plasma BK PCR
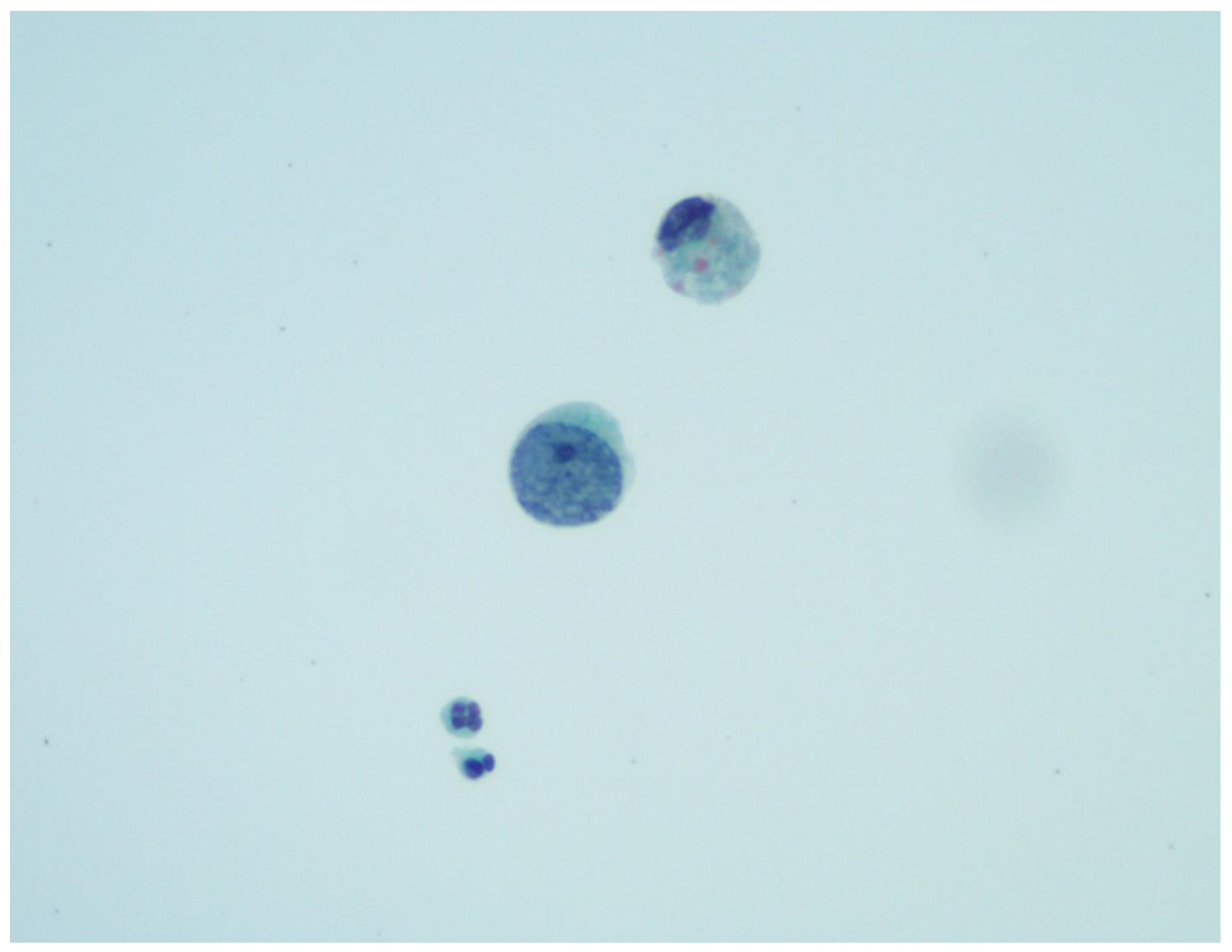
7.3. Urine Cytology
7.4. Donor-Derived Cell-Free DNA (dd-cfDNA)
7.5. Transplant Kidney Biopsy
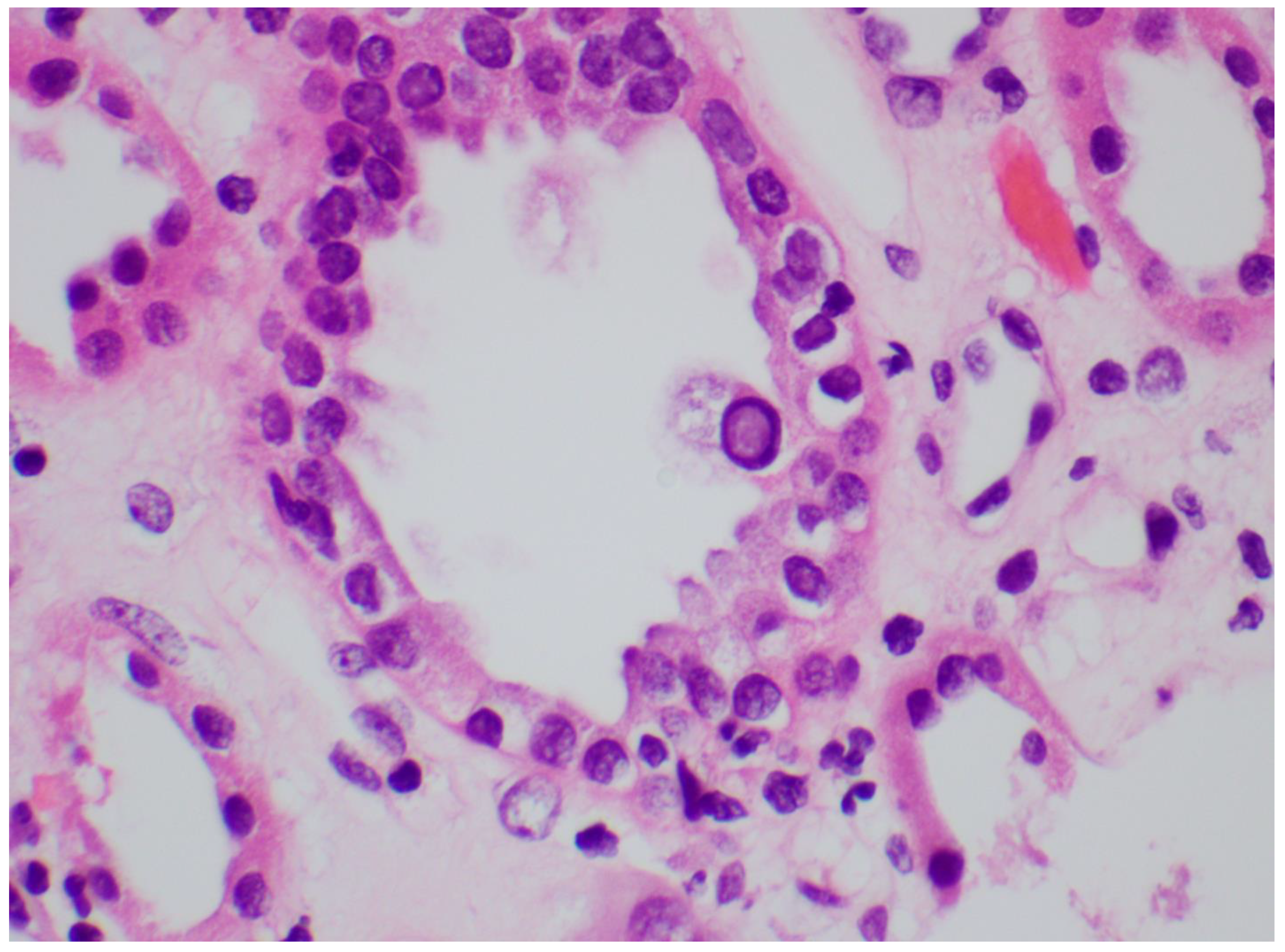
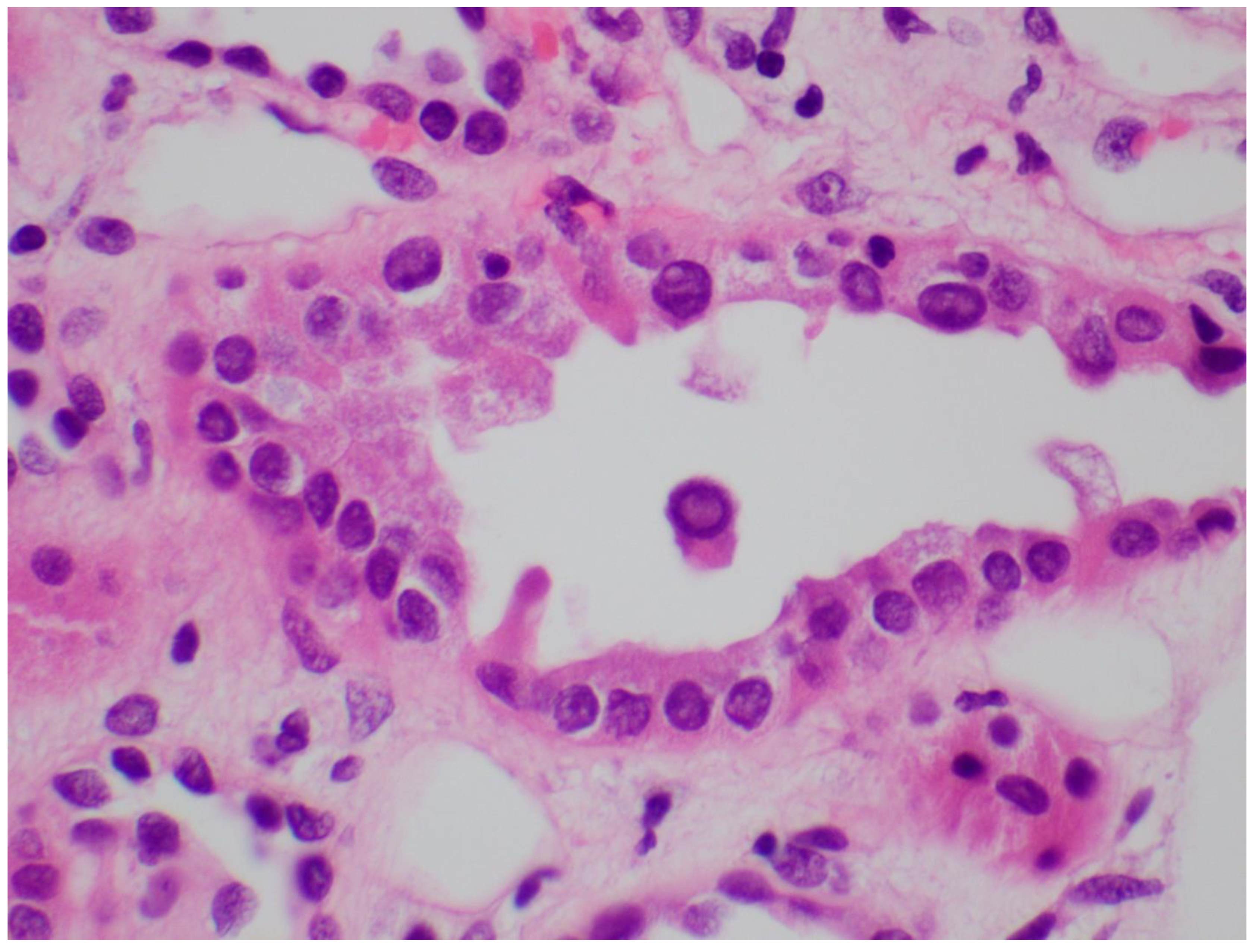
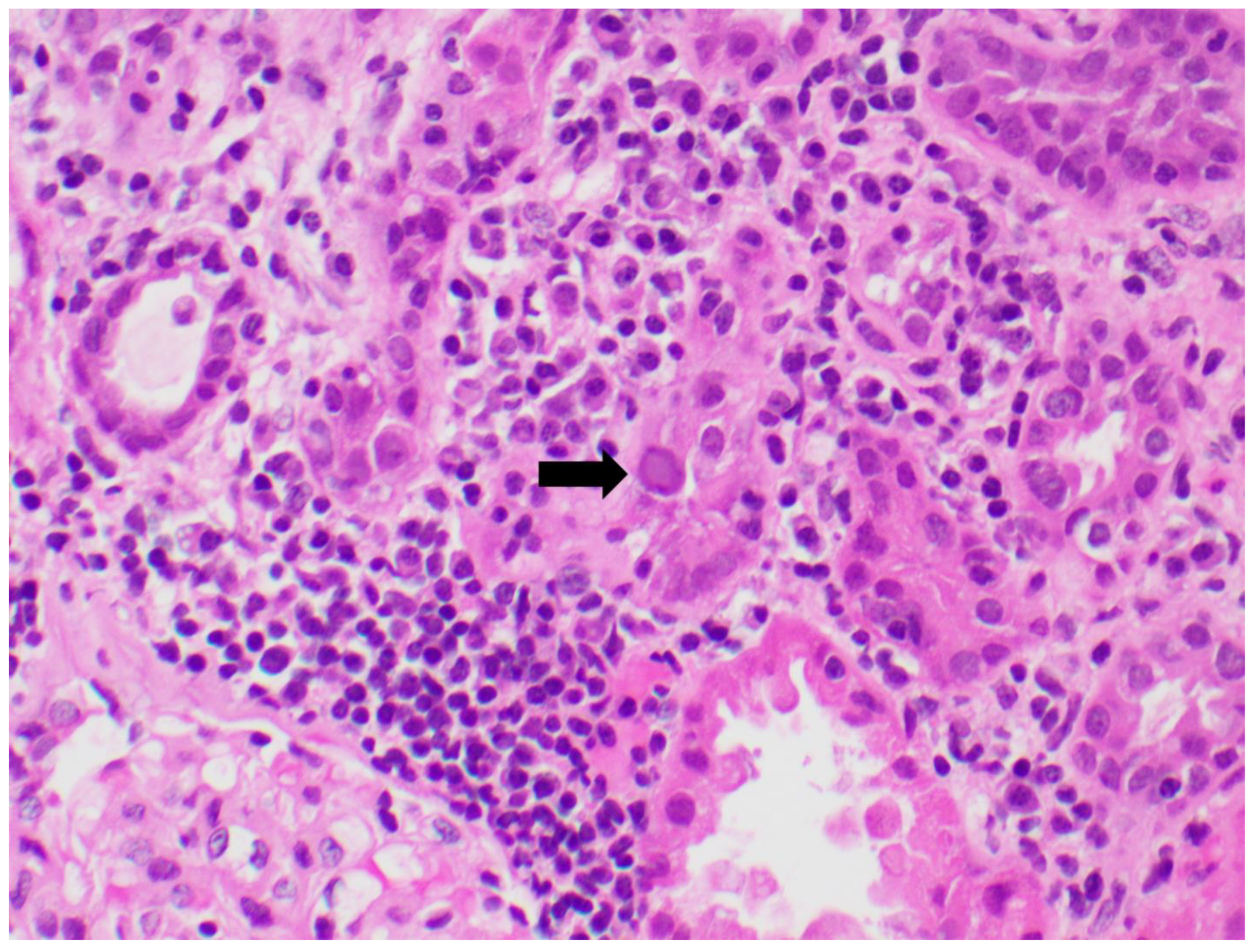
- Characteristic cytopathic changes (described further in Histology below).
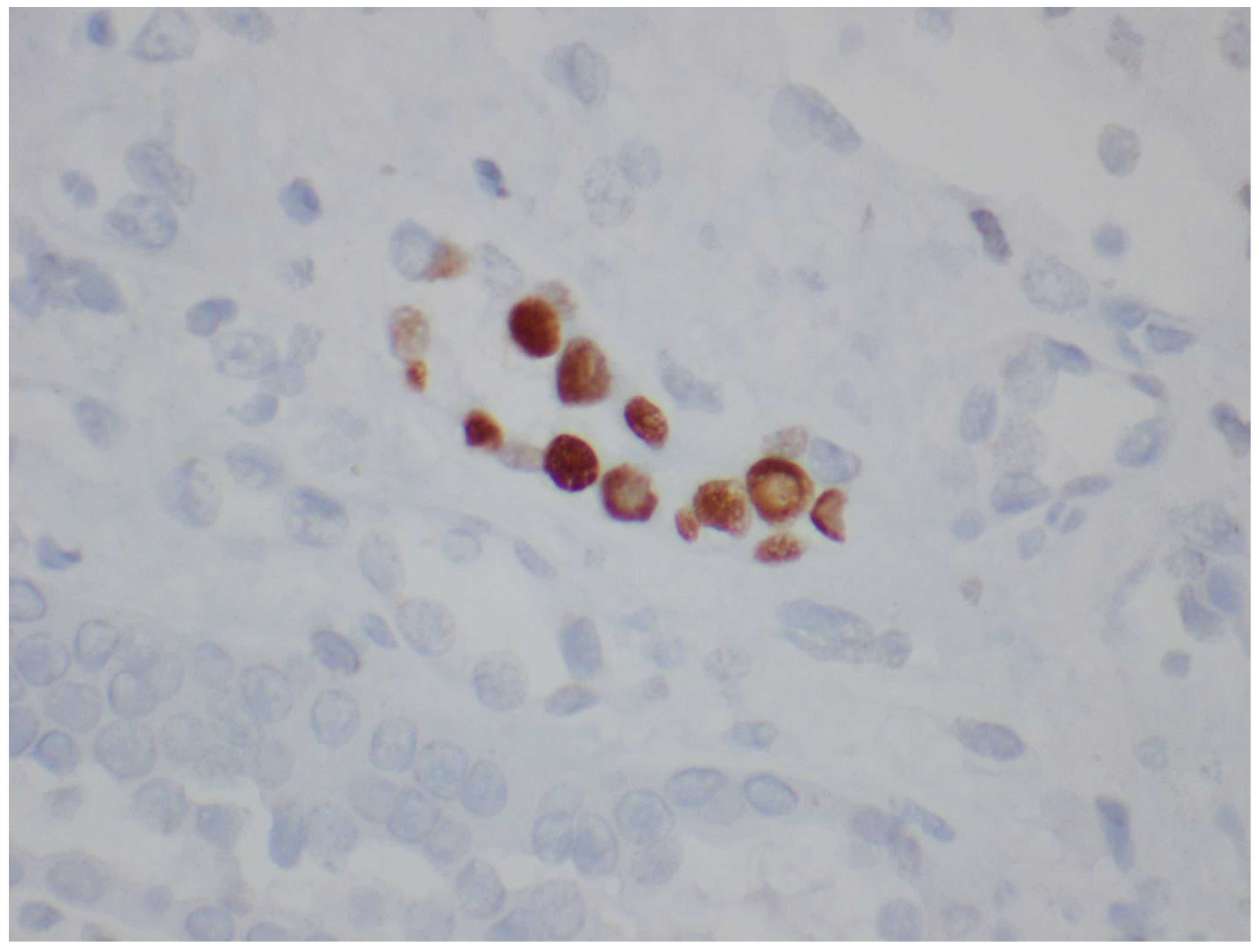
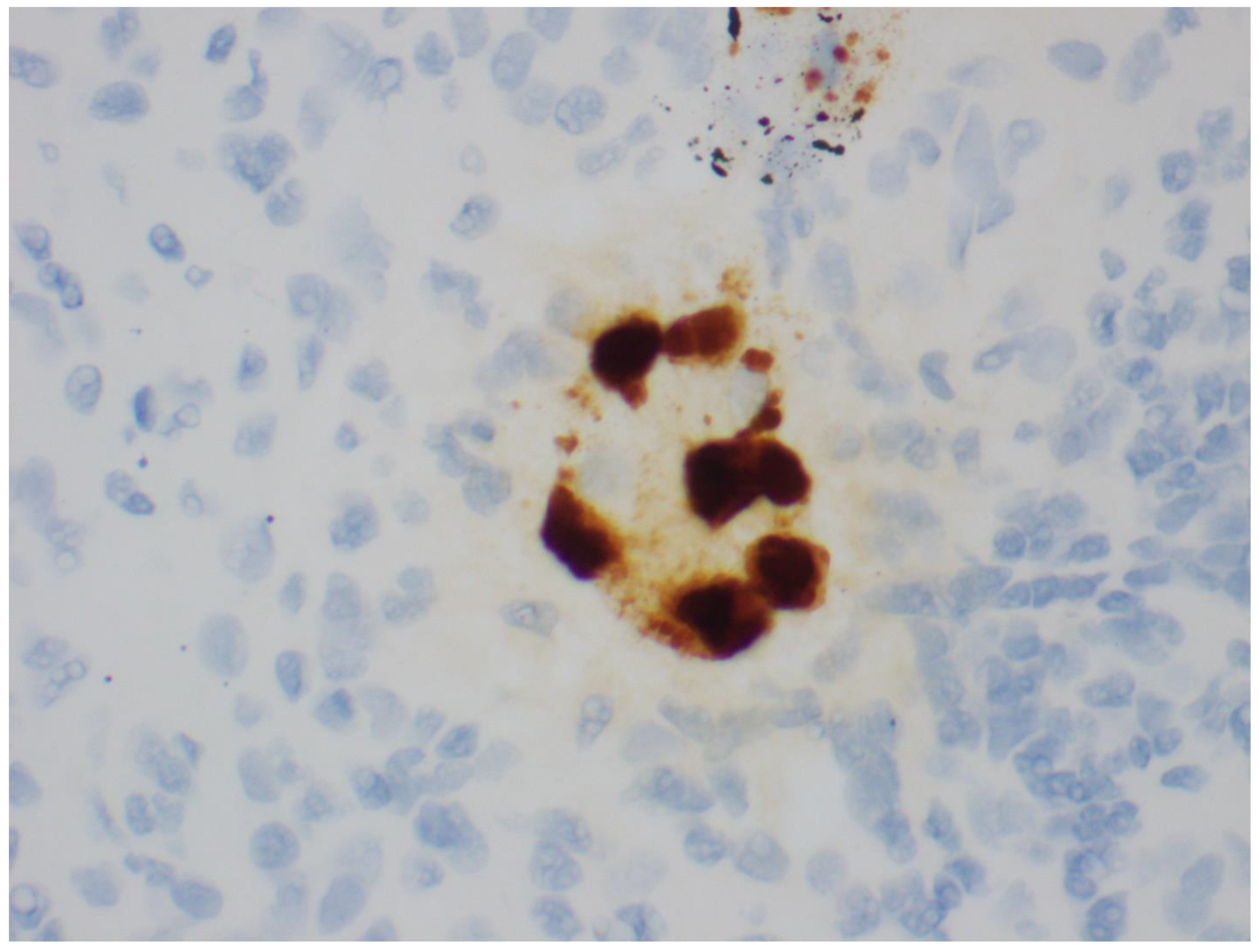
- Positive immunohistochemistry tests using antibodies directed specifically against BKV or against the cross-reacting SV40 large T antigen. Positive SV40 staining is useful as it is associated with a specificity of almost 100 percent for polyomavirus nephropathy (PVN); although, it does not distinguish between BKV and JC virus (JCV).
7.6. Histology
8. Treatment
- Reduce dose of antimetabolite by half while continuing on the same doses of calcineurin inhibitor and/or prednisone. It is imperative to monitor serum creatinine and serial plasma BK PCR levels from the same laboratory (to reduce inter-assay variability) every 2 weeks in the interim.
- If viral loads continue to be at similar levels or increase, proceed with complete cessation of anti-metabolite.
- The next step is to reduce calcineurin-inhibitor trough goals if viral loads do not reduce over 4 weeks despite cessation of anti-metabolite (4–6 ng/mL for tacrolimus and 50–100 ng/L for cyclosporine).
- IVIG: It is utilized in the setting of non-response to a maximal reduction in immunosuppression (balancing with risk of rejection). The rationale for use is the presence of BK-neutralizing antibodies in IVIG preparations. Data from five observational studies have demonstrated a reduction in BK viral loads; however, other anti-viral agents were administered at the same time as well [106,107,108,109,110].
- Quinolones: Despite demonstrating anti-viral properties in vitro, randomized trials failed to show efficacy as prophylaxis in the immediate post-transplant period or treatment for BK viremia [111,112,113]. In the levofloxacin prophylaxis trial, a higher incidence of resistant bacterial infection was seen in the quinolone group [112].
- Cidofovir: A nucleotide analog of cytosine has demonstrated activity against Polyomaviridae in-vitro [114]. Studies have shown no benefit with cidofovir use, notwithstanding that a significant risk of kidney dysfunction was noted [115,116]. Cidofovir has already been shown to be associated with proteinuria, proximal tubular dysfunction, and kidney disease [114,117].
- Leflunomide: A prodrug that converts to an active metabolite, A77 1726, which has demonstrated both immunosuppressive and anti-viral properties [118,119]. While there was initial enthusiasm for its use in BK virus infection based on a case series, a pharmacodynamic and prospective open-label study showed no benefit [119,120,121]. Another metabolite, FK778, did not demonstrate efficacy in a phase 2, proof-of-concept, randomized, open-label, parallel-group, 6-month study in kidney transplant patients when compared with a reduction in immunosuppression [122].
Upcoming Therapeutic Trials
- A randomized, double-blind, placebo-controlled study to assess the safety, pharmacokinetics, and efficacy of MAU868—a human monoclonal antibody (IgG1) that binds the viral capsid protein, VP1, which is responsible for binding to the surface of host cells (ClinicalTrials.gov identifier: NCT04294472).
- A phase 2 multicenter, randomized, double-blind, study of the safety, tolerability, and effectiveness of adoptively transferred posoleuccel (ALVR105) multivirus-specific T Cells in kidney transplant recipients with either high or low levels of BK viremia (ClinicalTrials.gov identifier: NCT04605484).
9. Kidney Re-Transplantation
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Hirsch, H.H.; Randhawa, P.S.; AST Infectious Diseases Community of Practice. BK polyomavirus in solid organ transplantation—Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13528. [Google Scholar] [CrossRef] [PubMed]
- Randhawa, P.; Vats, A.; Shapiro, R.; Weck, K.; Scantlebury, V. BK Virus: Discovery, Epidemiology, and Biology. Graft 2002, 5, S19–S27. [Google Scholar] [CrossRef]
- Randhawa, P.; Ramos, E. BK viral nephropathy: An overview. Transplant. Rev. 2007, 21, 77–85. [Google Scholar] [CrossRef]
- Wadei, H.M.; Rule, A.D.; Lewin, M.; Mahale, A.S.; Khamash, H.A.; Schwab, T.R.; Gloor, J.M.; Textor, S.C.; Fidler, M.E.; Lager, D.J.; et al. Kidney Transplant Function and Histological Clearance of Virus Following Diagnosis of Polyomavirus-Associated Nephropathy (PVAN). Am. J. Transplant. 2006, 6, 1025–1032. [Google Scholar] [CrossRef]
- Helle, F.; Brochot, E.; Handala, L.; Martin, E.; Castelain, S.; Francois, C.; Duverlie, G. Biology of the BKPyV: An Update. Viruses 2017, 9, 327. [Google Scholar] [CrossRef] [Green Version]
- Olsen, G.-H.; Andresen, P.A.; Hilmarsen, H.T.; Bjørang, O.; Scott, H.; Midtvedt, K.; Rinaldo, C.H. Genetic variability in BK Virus regulatory regions in urine and kidney biopsies from renal-transplant patients. J. Med. Virol. 2006, 78, 384–393. [Google Scholar] [CrossRef]
- Gosert, R.; Rinaldo, C.H.; Funk, G.A.; Egli, A.; Ramos, E.; Drachenberg, C.B.; Hirsch, H.H. Polyomavirus BK with rearranged noncoding control region emerge in vivo in renal transplant patients and increase viral replication and cytopathology. J. Exp. Med. 2008, 205, 841–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Funk, G.A.; Steiger, J.; Hirsch, H.H. Rapid Dynamics of Polyomavirus Type BK in Renal Transplant Recipients. J. Infect. Dis. 2006, 193, 80–87. [Google Scholar] [CrossRef]
- Saribas, A.S.; Coric, P.; Hamazaspyan, A.; Davis, W.; Axman, R.; White, M.K.; Abou-Gharbia, M.; Childers, W.; Condra, J.H.; Bouaziz, S.; et al. Emerging from the Unknown: Structural and Functional Features of Agnoprotein of Polyomaviruses. J. Cell. Physiol. 2016, 231, 2115–2127. [Google Scholar] [CrossRef] [Green Version]
- Baksh, F.K.; Finkelstein, S.D.; Swalsky, P.A.; Stoner, G.L.; Ryschkewitsch, C.F.; Randhawa, P. Molecular genotyping of BK and JC viruses in human polyomavirus[ndash ]associated interstitial nephritis after renal transplantation. Am. J. Kidney Dis. 2001, 38, 354–365. [Google Scholar] [CrossRef]
- Pastrana, D.V.; Ray, U.; Magaldi, T.G.; Schowalter, R.M.; Çuburu, N.; Buck, C.B. BK Polyomavirus Genotypes Represent Distinct Serotypes with Distinct Entry Tropism. J. Virol. 2013, 87, 10105–10113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prelog, M.; Egli, A.; Zlamy, M.; Hirsch, H.H. JC and BK polyomavirus-specific immunoglobulin G responses in patients thymectomized in early childhood. J. Clin. Virol. 2013, 58, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Laskin, B.L.; Sullivan, K.E.; Hester, J.; Goebel, J.; Davies, S.M.; Jodele, S. Antibodies to BK virus in children prior to allogeneic hematopoietic cell transplant. Pediatr. Blood Cancer 2015, 62, 1670–1673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knowles, W.A.; Pipkin, P.; Andrews, N.; Vyse, A.; Minor, P.; Brown, D.W.; Miller, E. Population-based study of antibody to the human polyomaviruses BKV and JCV and the simian polyomavirus SV40. J. Med Virol. 2003, 71, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Chong, S.; Antoni, M.; Macdonald, A.; Reeves, M.; Harber, M.; Magee, C.N. BK virus: Current understanding of pathogenicity and clinical disease in transplantation. Rev. Med. Virol. 2019, 29, e2044. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Miller, F.; Nord, E.; Wadhwa, N. Delayed renal allograft dysfunction and cystitis associated with human polyomavirus (BK) infection in a renal transplant recipient: A case report and review of literature. Clin. Nephrol. 2003, 60, 405–414. [Google Scholar] [CrossRef]
- Sánchez, D.M.; García, L.J.; Jiménez, I.L.; Luján, I.S.; Soriano, M.G.; Viñas, S.L.; Gil Muñoz, M.; Mateo, T.C. Renal Function Impairment in Kidney Transplantation: Importance of Early BK Virus Detection. Transplant. Proc. 2018, 51, 350–352. [Google Scholar] [CrossRef]
- Brennan, D.C.; Agha, I.; Bohl, D.L.; Schnitzler, M.A.; Hardinger, K.L.; Lockwood, M.; Torrence, S.; Schuessler, R.; Roby, T.; Gaudreault-Keener, M.; et al. Incidence of BK with Tacrolimus Versus Cyclosporine and Impact of Preemptive Immunosuppression Reduction. Am. J. Transplant. 2005, 5, 582–594. [Google Scholar] [CrossRef]
- Schwarz, A.; Linnenweber-Held, S.; Heim, A.; Framke, T.; Haller, H.; Schmitt, C. Viral Origin, Clinical Course, and Renal Outcomes in Patients with BK Virus Infection After Living-Donor Renal Transplantation. Transplantation 2016, 100, 844–853. [Google Scholar] [CrossRef]
- Hirsch, H.H.; Knowles, W.; Dickenmann, M.; Passweg, J.; Klimkait, T.; Mihatsch, M.J.; Steiger, J. Prospective Study of Polyomavirus Type BK Replication and Nephropathy in Renal-Transplant Recipients. N. Engl. J. Med. 2002, 347, 488–496. [Google Scholar] [CrossRef]
- Babel, N.; Fendt, J.; Karaivanov, S.; Bold, G.; Arnold, S.; Sefrin, A.; Lieske, E.; Hoffzimmer, M.; Dziubianau, M.; Bethke, N.; et al. Sustained BK Viruria as an Early Marker for the Development of BKV-Associated Nephropathy: Analysis of 4128 Urine and Serum Samples. Transplantation 2009, 88, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Höcker, B.; Schneble, L.; Murer, L.; Carraro, A.; Pape, L.; Kranz, B.; Oh, J.; Zirngibl, M.; Strologo, L.D.; Büscher, A.; et al. Epidemiology of and Risk Factors for BK Polyomavirus Replication and Nephropathy in Pediatric Renal Transplant Recipients: An International CERTAIN Registry Study. Transplantation 2019, 103, 1224–1233. [Google Scholar] [CrossRef] [PubMed]
- Pollara, C.P.; Corbellini, S.; Chiappini, S.; Sandrini, S.; De Tomasi, D.; Bonfanti, C.; Manca, N. Quantitative viral load measurement for BKV infection in renal transplant recipients as a predictive tool for BKVAN. New Microbiol. 2011, 34, 165–171. [Google Scholar] [PubMed]
- Sood, P.; Senanayake, S.; Sujeet, K.; Medipalli, R.; Zhu, Y.R.; Johnson, C.P.; Hariharan, S. Management and Outcome of BK Viremia in Renal Transplant Recipients. Transplantation 2012, 94, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Bicalho, C.S.; Oliveira, R.D.R.; David, D.R.; Fink, M.C.D.S.; Agena, F.; Castro, M.C.; Panutti, C.; David-Neto, E.; Pierrotti, L.C. Determination of viremia cut-off for risk to develop BKPyV-associated nephropathy among kidney transplant recipients. Transpl. Infect. Dis. 2018, 20, e12969. [Google Scholar] [CrossRef]
- Randhawa, P.; Ho, A.; Shapiro, R.; Vats, A.; Swalsky, P.; Finkelstein, S.; Uhrmacher, J.; Weck, K. Correlates of Quantitative Measurement of BK Polyomavirus (BKV) DNA with Clinical Course of BKV Infection in Renal Transplant Patients. J. Clin. Microbiol. 2004, 42, 1176–1180. [Google Scholar] [CrossRef] [Green Version]
- Viscount, H.B.; Eid, A.J.; Espy, M.J.; Griffin, M.; Thomsen, K.M.; Harmsen, W.S.; Razonable, R.R.; Smith, T.F. Polyomavirus Polymerase Chain Reaction as a Surrogate Marker of Polyomavirus-Associated Nephropathy. Transplantation 2007, 84, 340–345. [Google Scholar] [CrossRef]
- Drachenberg, C.B.; Papadimitriou, J.C.; Hirsch, H.H.; Wali, R.; Crowder, C.; Nogueira, J.; Cangro, C.B.; Mendley, S.; Mian, A.; Ramos, E. Histological Patterns of Polyomavirus Nephropathy: Correlation with Graft Outcome and Viral Load. Am. J. Transplant. 2004, 4, 2082–2092. [Google Scholar] [CrossRef]
- Van Aalderen, M.C.; Heutinck, K.M.; Huisman, C.; Ten Berge, I.J. BK virus infection in transplant recipients: Clinical manifestations, treatment options and the immune response. Neth. J. Med. 2012, 70, 172–183. [Google Scholar]
- Schold, J.D.; Rehman, S.; Kayler, L.K.; Magliocca, J.; Srinivas, T.R.; Meier-Kriesche, H.-U. Treatment for BK virus: Incidence, risk factors and outcomes for kidney transplant recipients in the United States. Transpl. Int. 2009, 22, 626–634. [Google Scholar] [CrossRef]
- Dharnidharka, V.R.; Cherikh, W.S.; Abbott, K. An OPTN Analysis of National Registry Data on Treatment of BK Virus Allograft Nephropathy in the United States. Transplantation 2009, 87, 1019–1026. [Google Scholar] [CrossRef] [PubMed]
- Nickeleit, V.; Hirsch, H.H.; Zeiler, M.; Gudat, F.; Prince, O.; Thiel, G.; Mihatsch, M.J. BK-virus nephropathy in renal transplants—tubular necrosis, MHC-class II expression and rejection in a puzzling game. Nephrol. Dial. Transplant. 2000, 15, 324–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demey, B.; Tinez, C.; François, C.; Helle, F.; Choukroun, G.; Duverlie, G.; Castelain, S.; Brochot, E. Risk factors for BK virus viremia and nephropathy after kidney transplantation: A systematic review. J. Clin. Virol. 2018, 109, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, H.H.; Vincenti, F.; Friman, S.; Tuncer, M.; Citterio, F.; Wiecek, A.; Scheuermann, E.H.; Klinger, M.; Russ, G.; Pescovitz, M.D.; et al. Polyomavirus BK Replication in De Novo Kidney Transplant Patients Receiving Tacrolimus or Cyclosporine: A Prospective, Randomized, Multicenter Study. Am. J. Transplant. 2012, 13, 136–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Gelder, T. How cyclosporine reduces mycophenolic acid exposure by 40% while other calcineurin inhibitors do not. Kidney Int. 2021, 100, 1185–1189. [Google Scholar] [CrossRef]
- Wojciechowski, D.; Chandran, S.; Webber, A.; Hirose, R.; Vincenti, F. Mycophenolate Mofetil Withdrawal with Conversion to Everolimus to Treat BK Virus Infection in Kidney Transplant Recipients. Transplant. Proc. 2017, 49, 1773–1778. [Google Scholar] [CrossRef] [PubMed]
- Tohme, F.; Kalil, R.; Thomas, C. Conversion to a sirolimus-based regimen is associated with lower incidence of BK viremia in low-risk kidney transplant recipients. Transpl. Infect. Dis. 2015, 17, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Moscarelli, L.; Caroti, L.; Antognoli, G.; Zanazzi, M.; Di Maria, L.; Carta, P.; Minetti, E. Everolimus leads to a lower risk of BKV viremia than mycophenolic acid inde novorenal transplantation patients: A single-center experience. Clin. Transplant. 2013, 27, 546–554. [Google Scholar] [CrossRef]
- Hirsch, H.H.; Brennan, D.C.; Drachenberg, C.B.; Ginevri, F.; Gordon, J.; Limaye, A.P.; Mihatsch, M.J.; Nickeleit, V.; Ramos, E.; Randhawa, P.; et al. Polyomavirus-Associated Nephropathy in Renal Transplantation: Interdisciplinary Analyses and Recommendations. Transplantation 2005, 79, 1277–1286. [Google Scholar] [CrossRef]
- Hardinger, K.L.; Koch, M.J.; Bohl, D.J.; Storch, G.A.; Brennan, D.C. BK-Virus and the Impact of Pre-Emptive Immunosuppression Reduction: 5-Year Results. Am. J. Transplant. 2010, 10, 407–415. [Google Scholar] [CrossRef] [Green Version]
- Nickeleit, V.; Klimkait, T.; Binet, I.F.; Dalquen, P.; Del Zenero, V.; Thiel, G.; Mihatsch, M.J.; Hirsch, H.H. Testing for Polyomavirus Type BK DNA in Plasma to Identify Renal-Allograft Recipients with Viral Nephropathy. N. Engl. J. Med. 2000, 342, 1309–1315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bressollette-Bodin, C.; Coste-Burel, M.; Hourmant, M.; Sebille, V.; Andre-Garnier, E.; Imbert-Marcille, B.M. A Prospective Longitudinal Study of BK Virus Infection in 104 Renal Transplant Recipients. Am. J. Transplant. 2005, 5, 1926–1933. [Google Scholar] [CrossRef]
- Mengel, M.; Marwedel, M.; Radermacher, J.; Eden, G.; Schwarz, A.; Haller, H.; Kreipe, H. Incidence of polyomavirus-nephropathy in renal allografts: Influence of modern immunosuppressive drugs. Nephrol. Dial. Transplant. 2003, 18, 1190–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dadhania, D.; Snopkowski, C.; Ding, R.; Muthukumar, T.; Chang, C.; Aull, M.J.; Lee, J.; Sharma, V.K.; Kapur, S.; Suthanthiran, M. Epidemiology of BK Virus in Renal Allograft Recipients: Independent Risk Factors for BK Virus Replication. Transplantation 2008, 86, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Van Doesum, W.B.; Gard, L.; Bemelman, F.J.; De Fijter, J.W.; Van Der Heide, J.J.H.; Niesters, H.G.; Van Son, W.J.; Stegeman, C.A.; Groen, H.; Riezebos-Brilman, A.; et al. Incidence and outcome of BK polyomavirus infection in a multicenter randomized controlled trial with renal transplant patients receiving cyclosporine-, mycophenolate sodium-, or everolimus-based low-dose immunosuppressive therapy. Transpl. Infect. Dis. 2017, 19, e12687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, S.; Zheng, H.-Y.; Suzuki, M.; Chen, Q.; Ikegaya, H.; Aoki, N.; Usuku, S.; Kobayashi, N.; Nukuzuma, S.; Yasuda, Y.; et al. Age-Related Urinary Excretion of BK Polyomavirus by Nonimmunocompromised Individuals. J. Clin. Microbiol. 2007, 45, 193–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohl, D.L.; Storch, G.A.; Ryschkewitsch, C.; Gaudreault-Keener, M.; Schnitzler, M.A.; Major, E.O.; Brennan, D.C. Donor Origin of BK Virus in Renal Transplantation and Role of HLA C7 in Susceptibility to Sustained BK Viremia. Am. J. Transplant. 2005, 5, 2213–2221. [Google Scholar] [CrossRef]
- Abend, J.R.; Changala, M.; Sathe, A.; Casey, F.; Kistler, A.; Chandran, S.; Howard, A.; Wojciechowski, D. Correlation of BK Virus Neutralizing Serostatus with the Incidence of BK Viremia in Kidney Transplant Recipients. Transplantation 2017, 101, 1495–1505. [Google Scholar] [CrossRef]
- Sood, P.; Senanayake, S.; Sujeet, K.; Medipalli, R.; Van-Why, S.K.; Cronin, D.C.; Johnson, C.P.; Hariharan, S. Donor and Recipient BKV-Specific IgG Antibody and Posttransplantation BKV Infection. Transplantation 2013, 95, 896–902. [Google Scholar] [CrossRef]
- Sharif, A.; Alachkar, N.; Bagnasco, S.; Geetha, D.; Gupta, G.; Womer, K.; Arend, L.; Racusen, L.; Montgomery, R.; Kraus, E. Incidence and Outcomes of BK Virus Allograft Nephropathy among ABO- and HLA-Incompatible Kidney Transplant Recipients. Clin. J. Am. Soc. Nephrol. 2012, 7, 1320–1327. [Google Scholar] [CrossRef]
- Bohl, D.L.; Brennan, D.C. BK Virus Nephropathy and Kidney Transplantation. Clin. J. Am. Soc. Nephrol. 2007, 2, S36–S46. [Google Scholar] [CrossRef] [PubMed]
- Wunderink, H.F.; van der Meijden, E.; van der Blij-de Brouwer, C.S.; Mallat, M.J.; Haasnoot, G.W.; van Zwet, E.W.; Claas, E.C.J.; de Fijter, J.W.; Kroes, A.C.M.; Arnold, F.; et al. Pretransplantation Donor-Recipient Pair Seroreactivity Against BK Polyomavirus Predicts Viremia and Nephropathy After Kidney Transplantation. Am. J. Transplant. 2016, 17, 161–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, S.K.; Huang, C.; Sahoo, M.K.; Weber, J.; Kurzer, J.; Stedman, M.R.; Concepcion, W.; Gallo, A.E.; Alonso, D.; Srinivas, T.; et al. Impact of Pretransplant Donor BK Viruria in Kidney Transplant Recipients. J. Infect. Dis. 2019, 220, 370–376. [Google Scholar] [CrossRef]
- Verghese, P.S.; Schmeling, D.O.; Knight, J.A.; Matas, A.J.; Balfour, H.H. The Impact of Donor Viral Replication at Transplant on Recipient Infections Posttransplant. Transplantation 2015, 99, 602–608. [Google Scholar] [CrossRef]
- Wunderink, H.F.; Haasnoot, G.W.; de Brouwer, C.S.; van Zwet, E.W.; Kroes, A.C.M.; de Fijter, J.W.; Rotmans, J.I.; Claas, F.H.J.; Feltkamp, M.C.W. Reduced Risk of BK Polyomavirus Infection in HLA-B51–positive Kidney Transplant Recipients. Transplantation 2019, 103, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Plafkin, C.; Singh, T.; Astor, B.C.; Parajuli, S.; Bhutani, G.; Safdar, N.; Panzer, S.E. Kidney transplant recipients with polycystic kidney disease have a lower risk of post-transplant BK infection than those with end-stage renal disease due to other causes. Transpl. Infect. Dis. 2018, 20, e12974. [Google Scholar] [CrossRef]
- Sawinski, D.; Goral, S. BK virus infection: An update on diagnosis and treatment. Nephrol. Dial. Transplant. 2014, 30, 209–217. [Google Scholar] [CrossRef] [Green Version]
- Prosser, S.E.; Orentas, R.J.; Jurgens, L.; Cohen, E.P.; Hariharan, S. Recovery of BK Virus Large T-Antigen–Specific Cellular Immune Response Correlates with Resolution of BK Virus Nephritis. Transplantation 2008, 85, 185–192. [Google Scholar] [CrossRef]
- Schachtner, T.; Müller, K.; Stein, M.; Diezemann, C.; Sefrin, A.; Babel, N.; Reinke, P. BK Virus-Specific Immunity Kinetics: A Predictor of Recovery from Polyomavirus BK-Associated Nephropathy. Am. J. Transplant. 2011, 11, 2443–2452. [Google Scholar] [CrossRef]
- Trydzenskaya, H.; Sattler, A.; Müller, K.; Schachtner, T.; Dang-Heine, C.; Friedrich, P.; Nickel, P.; Hoerstrup, J.; Schindler, R.; Thiel, A.; et al. Novel Approach for Improved Assessment of Phenotypic and Functional Characteristics of BKV-Specific T-Cell Immunity. Transplantation 2011, 92, 1269–1277. [Google Scholar] [CrossRef]
- Chesters, P.M.; Heritage, J.; McCance, D.J. Persistence of DNA Sequences of BK Virus and JC Virus in Normal Human Tissues and in Diseased Tissues. J. Infect. Dis. 1983, 147, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.V. Human polyomavirus BKV and renal disease. Nephrol. Dial. Transplant. 2000, 15, 754–755. [Google Scholar] [CrossRef] [PubMed]
- Drachenberg, C.B.; Beskow, C.O.; Cangro, C.B.; Bourquin, P.M.; Simsir, A.; Fink, J.; Weir, M.R.; Klassen, D.K.; Bartlett, S.T.; Papadimitriou, J.C. Human polyoma virus in renal allograft biopsies: Morphological findings and correlation with urine cytology. Hum. Pathol. 1999, 30, 970–977. [Google Scholar] [CrossRef]
- Grinde, B.; Gayorfar, M.; Rinaldo, C.H. Impact of a polyomavirus (BKV) infection on mRNA expression in human endothelial cells. Virus Res. 2007, 123, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Randhawa, P.; Shapiro, R. Conceptual Problems in the Diagnosis and Therapy of Acute Rejection in Patients with Polyomavirus Nephropathy. Am. J. Transplant. 2004, 4, 840. [Google Scholar] [CrossRef]
- Nankivell, B.J.; Renthawa, J.; Sharma, R.N.; Kable, K.; O’Connell, P.J.; Chapman, J.R. BK Virus Nephropathy: Histological Evolution by Sequential Pathology. Am. J. Transplant. 2017, 17, 2065–2077. [Google Scholar] [CrossRef] [Green Version]
- Elfadawy, N.; Yamada, M.; Sarabu, N. Management of BK Polyomavirus Infection in Kidney and Kidney-Pancreas Transplant Recipients. Infect. Dis. Clin. N. Am. 2018, 32, 599–613. [Google Scholar] [CrossRef]
- McClure, G.B.; Gardner, J.S.; Williams, J.T.; Copeland, C.M.; Sylvester, S.K.; Garcea, R.L.; Meinerz, N.M.; Groome, L.J.; Vanchiere, J.A. Dynamics of pregnancy-associated polyomavirus urinary excretion: A prospective longitudinal study. J. Med. Virol. 2012, 84, 1312–1322. [Google Scholar] [CrossRef]
- Madden, K.; Janitell, C.; Sower, D.; Yang, S. Prediction of BK viremia by urine viral load in renal transplant patients: An analysis of BK viral load results in paired urine and plasma samples. Transpl. Infect. Dis. 2018, 20, e12952. [Google Scholar] [CrossRef]
- Imlay, H.; Whitaker, K.; Fisher, C.E.; Limaye, A.P. Clinical characteristics and outcomes of late-onset BK virus nephropathy in kidney and kidney-pancreas transplant recipients. Transpl. Infect. Dis. 2018, 20, e12928. [Google Scholar] [CrossRef]
- Gupta, G.; Kuppachi, S.; Kalil, R.S.; Buck, C.B.; Lynch, C.F.; Engels, E.A. Treatment for presumed BK polyomavirus nephropathy and risk of urinary tract cancers among kidney transplant recipients in the United States. Am. J. Transplant. 2017, 18, 245–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geetha, D.; Tong, B.C.; Racusen, L.; Markowitz, J.S.; Westra, W.H. Bladder carcinoma in a transplant recipient: Evidence to implicate the BK human polyomavirus as a causal transforming agent. Transplantation 2002, 73, 1933–1936. [Google Scholar] [CrossRef] [PubMed]
- Abend, J.R.; Jiang, M.; Imperiale, M.J. BK virus and human cancer: Innocent until proven guilty. Semin. Cancer Biol. 2009, 19, 252–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sirohi, D.; Vaske, C.; Sanborn, Z.; Smith, S.C.; Don, M.D.; Lindsey, K.G.; Federman, S.; Vankalakunti, M.; Koo, J.; Bose, S.; et al. Polyoma virus-associated carcinomas of the urologic tract: A clinicopathologic and molecular study. Mod. Pathol. 2018, 31, 1429–1441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bialasiewicz, S.; Cho, Y.; Rockett, R.; Preston, J.; Wood, S.; Fleming, S.; Shepherd, B.; Barraclough, K.; Sloots, T.; Isbel, N. Association of micropapillary urothelial carcinoma of the bladder and BK viruria in kidney transplant recipients. Transpl. Infect. Dis. 2013, 15, 283–289. [Google Scholar] [CrossRef]
- Bechert, C.J.; Schnadig, V.J.; Payne, D.A.; Dong, J. Monitoring of BK Viral Load in Renal Allograft Recipients by Real-Time PCR Assays. Am. J. Clin. Pathol. 2010, 133, 242–250. [Google Scholar] [CrossRef]
- Schaub, S.; Hirsch, H.H.; Dickenmann, M.; Steiger, J.; Mihatsch, M.J.; Hopfer, H.; Mayr, M. Reducing Immunosuppression Preserves Allograft Function in Presumptive and Definitive Polyomavirus-Associated Nephropathy. Am. J. Transplant. 2010, 10, 2615–2623. [Google Scholar] [CrossRef]
- Petrov, R.; Elbahloul, O.; Gallichio, M.H.; Stellrecht, K.; Conti, D.J. Monthly Screening for Polyoma Virus Eliminates BK Nephropathy and Preserves Renal Function. Surg. Infect. 2009, 10, 85–90. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO clinical practice guideline for the care of kidney transplant recipients. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2009, 9, S1–S155. [Google Scholar] [CrossRef]
- Laskin, B.L.; Goebel, J. Cost-efficient screening for BK virus in pediatric kidney transplantation: A single-center experience and review of the literature. Pediatr. Transplant. 2010, 14, 589–595. [Google Scholar] [CrossRef]
- World Health Organization. First World Health Organization International Standard for BK Virus DNA; NIBSC code, 14/212; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Govind, S.; Hockley, J.; Morris, C.; Almond, N. The development and establishment of the 1st WHO BKV International Standard for nucleic acid based techniques. Biologicals 2019, 60, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.; Milligan, S.; Sahoo, M.K.; Taylor, N.; Pinsky, B.A. Calibration of BK Virus Nucleic Acid Amplification Testing to the 1st WHO International Standard for BK Virus. J. Clin. Microbiol. 2017, 55, 923–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bateman, A.C.; Greninger, A.L.; Atienza, E.E.; Limaye, A.P.; Jerome, K.R.; Cook, L. Quantification of BK Virus Standards by Quantitative Real-Time PCR and Droplet Digital PCR Is Confounded by Multiple Virus Populations in the WHO BKV International Standard. Clin. Chem. 2017, 63, 761–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Randhawa, P.; Kant, J.; Shapiro, R.; Tan, H.; Basu, A.; Luo, C. Impact of Genomic Sequence Variability on Quantitative PCR Assays for Diagnosis of Polyomavirus BK Infection. J. Clin. Microbiol. 2011, 49, 4072–4076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, N.G.; Cook, L.; Atienza, E.E.; Limaye, A.P.; Jerome, K.R. Marked Variability of BK Virus Load Measurement Using Quantitative Real-Time PCR among Commonly Used Assays. J. Clin. Microbiol. 2008, 46, 2671–2680. [Google Scholar] [CrossRef] [Green Version]
- Nankivell, B.J.; Renthawa, J.; Jeoffreys, N.; Kable, K.; O’Connell, P.J.; Chapman, J.R.; Wong, G.; Sharma, R.N. Clinical Utility of Urinary Cytology to Detect BK Viral Nephropathy. Transplantation 2015, 99, 1715–1722. [Google Scholar] [CrossRef]
- Nickeleit, V.; Hirsch, H.H.; Binet, I.F.; Gudat, F.; Prince, O.; Dalquen, P.; Thiel, G.; Mihatsch, M.J. Polyomavirus infection of renal allograft recipients: From latent infection to manifest disease. J. Am. Soc. Nephrol. 1999, 10, 1080–1089. [Google Scholar] [CrossRef]
- Singh, H.K.; Andreoni, K.A.; Madden, V.; True, K.; Detwiler, R.; Weck, K.; Nickeleit, V. Presence of Urinary Haufen Accurately Predicts Polyomavirus Nephropathy. J. Am. Soc. Nephrol. 2009, 20, 416–427. [Google Scholar] [CrossRef] [Green Version]
- Singh, H.K.; Reisner, H.; Derebail, V.K.; Kozlowski, T.; Nickeleit, V. Polyomavirus Nephropathy. Transplantation 2015, 99, 609–615. [Google Scholar] [CrossRef] [Green Version]
- Kant, S.; Bromberg, J.; Haas, M.; Brennan, D. Donor-derived Cell-free DNA and the Prediction of BK Virus-associated Nephropathy. Transplant. Direct 2020, 6, e622. [Google Scholar] [CrossRef]
- Kant, S.; Brennan, D.C. Donor Derived Cell Free DNA in Kidney Transplantation: The Circa 2020–2021 Update. Transpl. Int. 2022, 35, 115. [Google Scholar] [CrossRef] [PubMed]
- Kant, S.; Brennan, D. Donor-Derived Cell-Free DNA in Kidney Transplantation: Origins, Present and a Look to the Future. Medicina 2021, 57, 482. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, A.C. Polyomavirus Nephropathy: A Current Perspective and Clinical Considerations. Am. J. Kidney Dis. 2009, 54, 131–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drachenberg, C.; Papadimitriou, J. Polyomavirus-associated nephropathy: Update in diagnosis. Transpl. Infect. Dis. 2006, 8, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Drachenberg, C.B.; Papadimitriou, J.C.; Wali, R.; Cubitt, C.L.; Ramos, E. BK Polyoma Virus Allograft Nephropathy: Ultrastructural Features from Viral Cell Entry to Lysis. Am. J. Transplant. 2003, 3, 1383–1392. [Google Scholar] [CrossRef] [PubMed]
- Jennette, J.C.; Jennette, J.C.; Olson, J.L.; Schwartz, M.M.; Melvin, M.; Silva, F.G. Heptinstall’s Pathology of the Kidney, 6th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2006. [Google Scholar]
- Nankivell, B.J.; Renthawa, J.; Shingde, M.; Khan, A. The Importance of Kidney Medullary Tissue for the Accurate Diagnosis of BK Virus Allograft Nephropathy. Clin. J. Am. Soc. Nephrol. 2020, 15, 1015–1023. [Google Scholar] [CrossRef]
- Nickeleit, V.; Singh, H.K.; Randhawa, P.; Drachenberg, C.B.; Bhatnagar, R.; Bracamonte, E.; Chang, A.; Chon, W.J.; Dadhania, D.; Davis, V.G.; et al. The Banff Working Group Classification of Definitive Polyomavirus Nephropathy: Morphologic Definitions and Clinical Correlations. J. Am. Soc. Nephrol. 2018, 29, 680–693. [Google Scholar] [CrossRef] [Green Version]
- Randhawa, P.S.; Vats, A.; Zygmunt, D.; Swalsky, P.; Scantlebury, V.; Shapiro, R.; Finkelstein, S. Quantitation of viral DNA in renal allograft tissue from patients with BK virus nephropathy. Transplantation 2002, 74, 485–488. [Google Scholar] [CrossRef] [Green Version]
- Nickeleit, V.; Mihatsch, M.J. Polyomavirus Allograft Nephropathy and Concurrent Acute Rejection: A Diagnostic and Therapeutic Challenge. Am. J. Transplant. 2004, 4, 838–839. [Google Scholar] [CrossRef]
- Haas, M.; Loupy, A.; Lefaucheur, C.; Roufosse, C.; Glotz, D.; Seron, D.; Nankivell, B.J.; Halloran, P.F.; Colvin, R.B.; Akalin, E.; et al. The Banff 2017 Kidney Meeting Report: Revised diagnostic criteria for chronic active T cell–mediated rejection, antibody-mediated rejection, and prospects for integrative endpoints for next-generation clinical trials. Am. J. Transplant. 2018, 18, 293–307. [Google Scholar] [CrossRef] [Green Version]
- Colvin, R.B.; Chang, A. Diagnostic Pathology: Kidney Diseases, 2nd ed.; Elsevier: Philadelphia, PA, USA, 2016. [Google Scholar]
- Ginevri, F.; Azzi, A.; Hirsch, H.H.; Basso, S.; Fontana, I.; Cioni, M.; Bodaghi, S.; Salotti, V.; Rinieri, A.; Botti, G.; et al. Prospective Monitoring of Polyomavirus BK Replication and Impact of Pre-Emptive Intervention in Pediatric Kidney Recipients. Am. J. Transplant. 2007, 7, 2727–2735. [Google Scholar] [CrossRef] [PubMed]
- Johnston, O.; Jaswal, D.; Gill, J.S.; Doucette, S.; Fergusson, D.; Knoll, G. Treatment of Polyomavirus Infection in Kidney Transplant Recipients: A Systematic Review. Transplantation 2010, 89, 1057–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benotmane, I.; Solis, M.; Velay, A.; Cognard, N.; Olagne, J.; Vargas, G.G.; Perrin, P.; Marx, D.; Soulier, E.; Gallais, F.; et al. Intravenous immunoglobulin as a preventive strategy against BK virus viremia and BKV-associated nephropathy in kidney transplant recipients—Results from a proof-of-concept study. Am. J. Transplant. 2021, 21, 329–337. [Google Scholar] [CrossRef]
- Vu, D.; Shah, T.; Ansari, J.; Naraghi, R.; Min, D. Efficacy of Intravenous Immunoglobulin in the Treatment of Persistent BK Viremia and BK Virus Nephropathy in Renal Transplant Recipients. Transplant. Proc. 2015, 47, 394–398. [Google Scholar] [CrossRef]
- Sharma, A.P.; Moussa, M.; Casier, S.; Rehman, F.; Filler, G.; Grimmer, J. Intravenous immunoglobulin as rescue therapy for BK virus nephropathy. Pediatr. Transplant. 2009, 13, 123–129. [Google Scholar] [CrossRef]
- Kable, K.; Davies, C.D.; O’Connell, P.J.; Chapman, J.R.; Nankivell, B.J. Clearance of BK Virus Nephropathy by Combination Antiviral Therapy with Intravenous Immunoglobulin. Transplant. Direct 2017, 3, e142. [Google Scholar] [CrossRef] [PubMed]
- Sener, A.; House, A.A.; Jevnikar, A.M.; Boudville, N.; McAlister, V.; Muirhead, N.; Rehman, F.; Luke, P.P.W. Intravenous Immunoglobulin as a Treatment for BK Virus Associated Nephropathy: One-Year Follow-Up of Renal Allograft Recipients. Transplantation 2006, 81, 117–120. [Google Scholar] [CrossRef]
- Patel, S.J.; Knight, R.J.; Kuten, S.A.; Graviss, E.A.; Nguyen, D.T.; Moore, L.W.; Musick, W.L.; Gaber, A.O. Ciprofloxacin for BK viremia prophylaxis in kidney transplant recipients: Results of a prospective, double-blind, randomized, placebo-controlled trial. Am. J. Transplant. 2019, 19, 1831–1837. [Google Scholar] [CrossRef]
- Knoll, G.; Humar, A.; Fergusson, D.; Johnston, O.; House, A.A.; Kim, S.J.; Ramsay, T.; Chassé, M.; Pang, X.; Zaltzman, J.; et al. Levofloxacin for BK Virus Prophylaxis Following Kidney Transplantation. JAMA 2014, 312, 2106–2114. [Google Scholar] [CrossRef]
- Lee, B.T.; Gabardi, S.; Grafals, M.; Hofmann, R.M.; Akalin, E.; Aljanabi, A.; Mandelbrot, D.A.; Adey, D.B.; Heher, E.; Fan, P.-Y.; et al. Efficacy of Levofloxacin in the Treatment of BK Viremia: A Multicenter, Double-Blinded, Randomized, Placebo-Controlled Trial. Clin. J. Am. Soc. Nephrol. 2014, 9, 583–589. [Google Scholar] [CrossRef] [Green Version]
- Meier, P.; Dautheville-Guibal, S.; Ronco, P.M.; Rossert, J. Cidofovir-induced end-stage renal failure. Nephrol. Dial. Transplant. 2002, 17, 148–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vats, A.; Shapiro, R.; Randhawa, P.S.; Scantlebury, V.; Tuzuner, A.; Saxena, M.; Moritz, M.L.; Beattie, T.J.; Gonwa, T.; Green, M.D.; et al. Quantitative viral load monitoring and cidofovir therapy for the management of BK virus-associated nephropathy in children and adults. Transplantation 2003, 75, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Kuypers, D.R.; Vandooren, A.-K.; Lerut, E.; Evenepoel, P.; Claes, K.; Snoeck, R.; Naesens, L.; Vanrenterghem, Y. Adjuvant Low-Dose Cidofovir Therapy for BK Polyomavirus Interstitial Nephritis in Renal Transplant Recipients. Am. J. Transplant. 2005, 5, 1997–2004. [Google Scholar] [CrossRef] [PubMed]
- Bagnis, C.; Izzdine, H.; Deray, G. Renal tolerance of cidofovir. Therapie 1999, 54, 689–691. [Google Scholar]
- Chong, A.; Zeng, H.; Knight, D.; Shen, J.; Meister, G.; Williams, J.; Waldman, W. Concurrent Antiviral and Immunosuppressive Activities of Leflunomide In Vivo. Am. J. Transplant. 2006, 6, 69–75. [Google Scholar] [CrossRef]
- Josephson, M.A.; Gillen, D.; Javaid, B.; Kadambi, P.; Meehan, S.; Foster, P.; Harland, R.; Thistlethwaite, R.J.; Garfinkel, M.; Atwood, W.; et al. Treatment of Renal Allograft Polyoma BK Virus Infection with Leflunomide. Transplantation 2006, 81, 704–710. [Google Scholar] [CrossRef]
- Faguer, S.; Hirsch, H.H.; Kamar, N.; Guilbeau-Frugier, C.; Ribes, D.; Guitard, J.; Esposito, L.; Cointault, O.; Modesto, A.; Lavit, M.; et al. Leflunomide treatment for polyomavirus BK-associated nephropathy after kidney transplantation. Transpl. Int. 2007, 20, 962–969. [Google Scholar] [CrossRef]
- Krisl, J.C.; Taber, D.J.; Pilch, N.; Chavin, K.; Bratton, C.; Thomas, B.; McGillicuddy, J.; Baliga, P. Leflunomide Efficacy and Pharmacodynamics for the Treatment of BK Viral Infection. Clin. J. Am. Soc. Nephrol. 2012, 7, 1003–1009. [Google Scholar] [CrossRef] [Green Version]
- Guasch, A.; Roy-Chaudhury, P.; Woodle, E.S.; Fitzsimmons, W.; Holman, J.; First, M.R. Assessment of Efficacy and Safety of FK778 in Comparison with Standard Care in Renal Transplant Recipients With Untreated BK Nephropathy. Transplantation 2010, 90, 891–897. [Google Scholar] [CrossRef]
- Leeaphorn, N.; Thongprayoon, C.; Chon, W.J.; Cummings, L.S.; Mao, M.A.; Cheungpasitporn, W. Outcomes of kidney retransplantation after graft loss as a result of BK virus nephropathy in the era of newer immunosuppressant agents. Am. J. Transplant. 2019, 20, 1334–1340. [Google Scholar] [CrossRef]
- Ginevri, F.; Pastorino, N.; de Santis, R.; Fontana, I.; Sementa, A.; Losurdo, G.; Santopietro, A.; Perfumo, F.; Locatelli, F.; Maccario, R.; et al. Retransplantation after kidney graft loss due to polyoma BK virus nephropathy: Successful outcome without original allograft nephrectomy. Am. J. Kidney Dis. 2003, 42, 821–825. [Google Scholar] [CrossRef]
- Boucek, P.; Voska, L.; Saudek, F. Successful retransplantation after renal allograft loss to polyoma virus interstitial nephritis. Transplantation 2002, 74, 1478. [Google Scholar] [CrossRef]
- Huang, J.; Danovitch, G.; Pham, P.-T.; Bunnapradist, S.; Huang, E. Kidney retransplantation for BK virus nephropathy with active viremia without allograft nephrectomy. J. Nephrol. 2015, 28, 773–777. [Google Scholar] [CrossRef] [PubMed]
- Geetha, D.; Sozio, S.; Ghanta, M.; Josephson, M.; Shapiro, R.; Dadhania, D.; Hariharan, S. Results of Repeat Renal Transplantation After Graft Loss from BK Virus Nephropathy. Transplantation 2011, 92, 781–786. [Google Scholar] [CrossRef] [PubMed]
- Dharnidharka, V.R.; Cherikh, W.S.; Neff, R.; Cheng, Y.; Abbott, K. Retransplantation After BK Virus Nephropathy in Prior Kidney Transplant: An OPTN Database Analysis. Am. J. Transplant. 2010, 10, 1312–1315. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biopsy-Proven PVN Class 1 | Biopsy-Proven PVN Class 2 | Biopsy-Proven PVN Class 3 | |||
|---|---|---|---|---|---|
| pvl | Banff Ci Score | Pvl | Banff Ci Score | Pvl | Banff Ci Score |
| 1 | 0–1 | 1 | 2–3 | - | - |
| - | - | 2 | 0–3 | - | - |
| - | - | 3 | 0–1 | 3 | 2–3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kant, S.; Dasgupta, A.; Bagnasco, S.; Brennan, D.C. BK Virus Nephropathy in Kidney Transplantation: A State-of-the-Art Review. Viruses 2022, 14, 1616. https://doi.org/10.3390/v14081616
Kant S, Dasgupta A, Bagnasco S, Brennan DC. BK Virus Nephropathy in Kidney Transplantation: A State-of-the-Art Review. Viruses. 2022; 14(8):1616. https://doi.org/10.3390/v14081616
Chicago/Turabian StyleKant, Sam, Alana Dasgupta, Serena Bagnasco, and Daniel C. Brennan. 2022. "BK Virus Nephropathy in Kidney Transplantation: A State-of-the-Art Review" Viruses 14, no. 8: 1616. https://doi.org/10.3390/v14081616