
Collateral Impact of Public Health and Social Measures on Respiratory Virus Activity during the COVID-19 Pandemic 2020–2021




Abstract
:1. Introduction
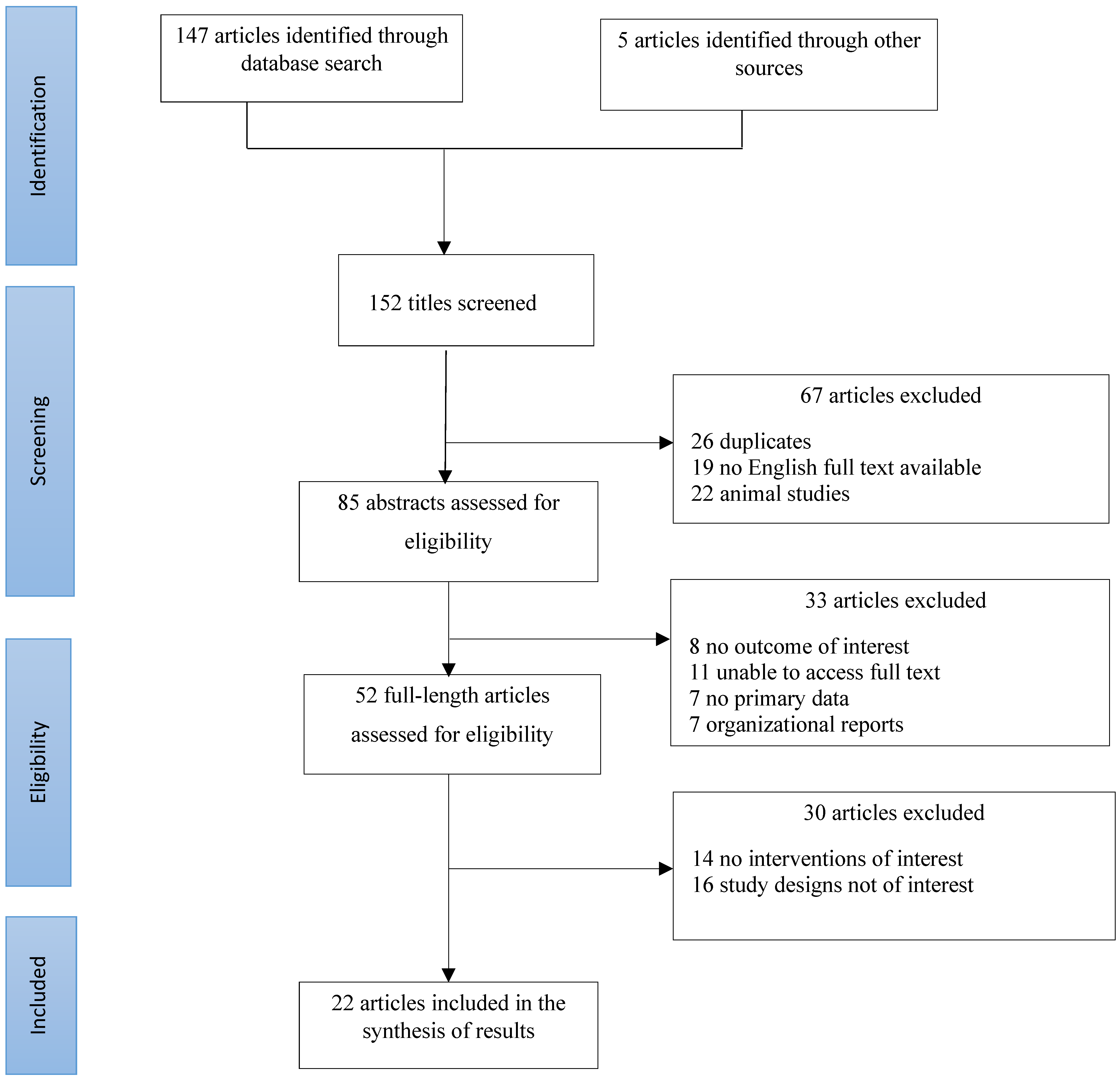
2. Materials and Methods
3. Results
3.1. Influenza

{kind=link}
| Author, Year, and Location of Study | Study Details | Main Findings |
|---|---|---|
| Cowling et al., 2020; China [29] | Using telephone surveys conducted on 20–23 January, 11–14 February, and 10–13 March 2020, data on 715 laboratory-confirmed COVID-19 cases were obtained from the Hong Kong Center for Health Protection. The authors estimated the daily effective reproduction number (Rt) for COVID-19 and influenza to estimate changes in transmissibility over time. | Influenza transmission declined after the implementation of PHSMs, with a 44% (95% CI: 34–53%) reduction in transmissibility in the community from an estimated Rt of 1.28 (95% CI: 1.26–1.30) before the start of school closure to 0.72 (0.70–0.74) during the closure weeks. |
| Soo et al., 2020; Singapore [27] | Indicators of influenza activity in 2020 before and after COVID-19 PHSMs with the corresponding indicators from 3 preceding years were compared. | The percentage of influenza positivity decreased by 64%, and the estimated daily number of influenza cases decreased by 76% in weeks 5–9 of 2020 compared with the preceding years. |
| Tempia et al., 2020; South Africa [25] | The authors assessed the detection of influenza and RSV through facility-based syndromic surveillance of adults and children with mild or severe respiratory illness (SRI) from January to October 2020 and compared this with surveillance data from 2013 to 2019. | A decrease in influenza-detection rate was recorded. From 2013 to 2019, there was a 12.7% and 5.2% influenza-detection rate for specimens from ILI and SRI patients, respectively. Meanwhile, in 2020, a corresponding detection rate of 4.4% and 0.8% influenza-detection rate of specimens from ILI and SRI cases was recorded, respectively. |
| Arellanos-Soto et al., 2021; Mexico [24] | Analysis of sentinel surveillance data on influenza-like illnesses (ILI) evaluating whether the influenza trends in the 2019–2020 season were different before and after the implementation of COVID-19 national control protocol. | The average number of influenza cases during the COVID-19 PHSM implementation was significantly different from that during the previous two influenza seasons (587 vs. 357). The percentage of influenza cases decreased by 64%, and the estimated daily number of influenza cases decreased by 76% in week 20 of season 2019–2020 compared with the preceding years. |
| Huang et al., 2021; New Zealand [23] | Using multiple surveillance systems from May to September 2020, the authors observed trends of influenza and other respiratory viral infections in 2020. | From 1 January to 31 July 2020, a total of 291 influenza hospitalizations were as follows: pre-lockdown 238 (81.8%), lockdown 33 (11.3%), and post-lockdown 15 (5.2%). |
| Kim et al., 2021; South Korea [30] | The authors analyzed changes in sample positivity by respiratory viruses after PHSMs. | Compared with the pre-PHSMs period, the positive rates of RSV and influenza decreased significantly to 19% and 6% and 23% and 6% of the predicted value. |
| Lee et al., 2021; South Korea [28] | National influenza surveillance data were compared over seven sequential seasons in April 2020. | A decrease in seasonal influenza cases, hospitalization, and activity was seen after the implementation of PHSMs. The peak activity was lower in 2019/2020, with 49.8 ILIs/1000 visits, than in other seasons showing values of 71.9 to 86.2 ILIs/1000 visits. ILI activity also decreased during weeks 9 to 17 (−12 ILIs/1000 visits on average; 95% CI: −18 ILIs/1000 visits to −6 ILIs/1000 visits). |
| Qi, et al., 2021; United States [26] | An absolute humidity-driven susceptible-infectious-recovered-susceptible (SIRS) model was used to quantify the reduction in influenza incidence and transmission after implementation of PHSMs in 2020. | The incidence of influenza, which circulated in early 2020, was reduced by more than 60% in the United States during the first 10 weeks following implementation of PHSMs. |
| El-Heneidy et al., 2022; Australia. [31] | Weekly counts of influenza and other respiratory diseases from a Queensland laboratory network were obtained for the year 2020 and compared with averaged counts from 2015 to 2019. | PHSMs were associated with a sharp and sustained decline in influenza, whereas during the typical annual influenza season (weeks 23–40), no cases were detected from 163,296 tests compared with an average of 26.1% (11,844/45,396) of tests positive in 2015–2019. |
3.2. Parainfluenza
| Author, Year, and Location of Study | Study Details | Main Findings |
|---|---|---|
| Liu et al., 2021; China [34] | Respiratory specimens were obtained from children with lower respiratory tract infections at Children’s Hospital of Fudan University, and data were analyzed and compared between the year 2020 (COVID-19 pandemic) and 2019 (before COVID-19 pandemic). | Parainfluenza viruses were detected in 460/2507 (18.35%) specimens in 2020, which was significantly lower than that in 2019 (1072/4600, 23.30%). |
| El-Heneidy et al., 2022; Australia [31] | Weekly counts of parainfluenza and other respiratory diseases from a Queensland laboratory network were obtained for the year 2020 and compared with averaged counts from 2015 to 2019. | The number of positive tests for influenza decreased to zero in 2020 compared to 1053 in 2015–2019 following the introduction of PHSMs. |
| Kuitunen et al., 2022; Finland [33] | A nationwide register-based retrospective epidemiologic surveillance study was conducted from January 2012 to December 2021. | The monthly parainfluenza incidence among children aged 0–4 years was six times higher than that in the previous years. As the restrictions were relaxed in September 2021, a high epidemic peak of parainfluenza was recorded after relatively low levels. |
3.3. Respiratory Syncytial Virus
| Author, Year, and Location of Study | Study Details | Findings |
|---|---|---|
| Groves et al., 2021; Canada [38] | Epidemiologic data were obtained from the Canadian Respiratory Virus Detection Surveillance System. Weekly data from the week ending 30 August 2014 until the week ending 13 March 2021 were analyzed. | The percent positive rates for RSV dropped by 0.02% in the post-pandemic period compared to that in the pre-pandemic levels. |
| Kim et al., 2021; South Korea [36] | The Korean influenza and respiratory virus-monitoring system database was used. From January 2016 through January 2021, the weekly positive rate of respiratory viruses and the weekly number of hospitalizations with acute respiratory infections were investigated. | Compared with the pre-PHSMs period, the positive rates of RSV decreased significantly from 19% to 6% in the PHSMs implemented period. |
| Wagatsuma et al., Japan 2021 [37] | The monthly number of RSV cases per sentinel site in 2020 was compared with the average of the corresponding period in the previous 6 years using a monthly paired t-test. | The average number of monthly RSV case notifications in 2020 decreased by approximately 85% compared to that in the preceding 6 years (2014–2019). |
| Yeoh et al., 2021; Australia [39] | Laboratory data were prospectively collected as part of routine regional public health surveillance and analyzed weekly from 1 January 2012 to 30 August 2020. | Overall, 98.0% reductions in RSV in children through winter 2020 compared to previous seasons (2012–2019). |
| Vittucci et al., 2021; Italy [40] | A retrospective analysis of nasopharyngeal samples of all patients (0–18 years old) admitted with respiratory symptoms in a large Italian tertiary hospital during the last three seasons from 2018 to 2021 was conducted. | There was a decrease in RSV cases from 726 in 2018–2019 to 689 in 2019–2020 during the COVID-19 pandemic. |
| El-Heneidy et al., 2022; Australia [31] | Weekly counts of RSV and other respiratory diseases from a Queensland laboratory network were obtained for the year 2020 and compared with averaged counts from 2015 to 2019. | RSV-detection rates decreased in weeks 39–47 after the implementation of PHSMs but increased to 5.6% (562/10,078) in weeks 48–52 in 2020 from 2.9% (150/5018) in 2015–2019. |
| Ye et al., 2022; China [34] | Epidemiologic characteristics of common childhood respiratory viruses in 2020 (after the pandemic) compared with 2019 (before the pandemic) were examined. | The positive rate of RSV in 2020 was higher than that in 2019 (9.35% vs. 6.31%). |
3.4. Rhinovirus
| Author, Year, and Location of Study | Study Details | Findings |
|---|---|---|
| Kuitunen et al., 2021; Finland [42] | Rhinovirus epidemiology in children during the pandemic was analyzed using data from the Finnish Infectious Disease Register. | There was a 22.6% decrease in rhinovirus incidence during the COVID-19 pandemic. The impact of the PHSMs was mostly seen among children aged 0–4 years of age in weeks 14–22 in 2020. |
| Park et al., 2021; South Korea [41] | National surveillance data were used to compare the incidence of respiratory viruses during 2016–2019 vs. 2020. | In South Korea, after social distancing measures were implemented, there was a significant decrease in monthly mean rhinovirus incidence rate relative to the pre-pandemic period (–60.4% to –93.8%). |
3.5. Adenovirus
| Author, Year, and Location of Study | Study Details | Findings |
|---|---|---|
| Li et al., 2021; China [43] | Data on tests of adenovirus from electronic healthcare records of Children’s Hospital of Zhejiang University School of Medicine were extracted during the COVID-19 pandemic (January–December 2020) and were compared with those in 2019 during the same period. | The positive detection rate of adenovirus in 2020 was 2.69% lower than the level in 2019. |
| Nagakubo et al., 2022; Japan [44] | Nasopharyngeal swab samples from 3249 patients who visited the Yamanashi Central Hospital in Japan from 1 March 2020 to 28 February 2021 were used to determine the adenovirus positive rate. | During the implementation of PHSMs, there was a 52% increase in sample positive rate for adenoviruses; a change in virus diversity was also observed. |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ryu, S.; Cowling, B.J. Human Influenza Epidemiology. Cold Spring Harb. Perspect. Med. 2021, 11, a038356. [Google Scholar] [CrossRef] [PubMed]
- Ryu, S.; Kim, S.; Kim, B.I.; Klein, E.Y.; Yoon, Y.K.; Chun, B.C. Temporal relationship between antibiotic use and respiratory virus activities in the Republic of Korea: A time-series analysis. Antimicrob. Resist. Infect. Control 2018, 7, 56. [Google Scholar] [CrossRef] [Green Version]
- McAllister, D.A.; Liu, L.; Shi, T.; Chu, Y.; Reed, C.; Burrows, J.; Adeloye, D.; Rudan, I.; Black, R.E.; Campbell, H.; et al. Global, regional, and national estimates of pneumonia morbidity and mortality in children younger than 5 years between 2000 and 2015: A systematic analysis. Lancet. Glob. Health 2019, 7, e47–e57. [Google Scholar] [CrossRef] [Green Version]
- Fong, M.W.; Gao, H.; Wong, J.Y.; Xiao, J.; Shiu, E.Y.C.; Ryu, S.; Cowling, B.J. Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings-Social Distancing Measures. Emerg. Infect. Dis. 2020, 26, 976–984. [Google Scholar] [CrossRef]
- Xiao, J.; Shiu, E.Y.C.; Gao, H.; Wong, J.Y.; Fong, M.W.; Ryu, S.; Cowling, B.J. Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings-Personal Protective and Environmental Measures. Emerg. Infect. Dis. 2020, 26, 967–975. [Google Scholar] [CrossRef]
- Ryu, S.; Gao, H.; Wong, J.Y.; Shiu, E.Y.C.; Xiao, J.; Fong, M.W.; Cowling, B.J. Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings-International Travel-Related Measures. Emerg. Infect. Dis. 2020, 26, 961–966. [Google Scholar] [CrossRef]
- Ryu, S.; Hwang, Y.; Ali, S.T.; Kim, D.S.; Klein, E.Y.; Lau, E.H.Y.; Cowling, B.J. Decreased Use of Broad-Spectrum Antibiotics During the Coronavirus Disease 2019 Epidemic in South Korea. J. Infect. Dis. 2021, 224, 949–955. [Google Scholar] [CrossRef]
- Pai, M.; Kasaeva, T.; Swaminathan, S. COVID-19’s Devastating Effect on Tuberculosis Care—A Path to Recovery. N. Engl. J. Med. 2022, 386, 1490–1493. [Google Scholar] [CrossRef]
- Brooker, S.J.; Ziumbe, K.; Negussu, N.; Crowley, S.; Hammami, M. Neglected tropical disease control in a world with COVID-19: An opportunity and a necessity for innovation. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 205–207. [Google Scholar] [CrossRef]
- Hwang, Y.; Kim, D.; Ryu, S. Decreased patient visits for ankle sprain during the COVID-19 pandemic in South Korea: A nationwide retrospective study. Prev. Med. Rep. 2022, 26, 101728. [Google Scholar] [CrossRef]
- Jang, S.; Weible, C.M.; Park, K. Policy processes in South Korea through the lens of the Advocacy Coalition Framework. J. Asian Public Policy 2016, 9, 274–290. [Google Scholar] [CrossRef]
- Chang, S.; Ryu, S.; Kim, D.; Chun, B.C. Decrease in the incidence of chlamydia infection during the COVID-19 pandemic in South Korea. Sex. Transm. Infect. 2022, 98, 155. [Google Scholar] [CrossRef] [PubMed]
- Chopra, V.; Toner, E.; Waldhorn, R.; Washer, L. How Should U.S. Hospitals Prepare for Coronavirus Disease 2019 (COVID-19)? Ann. Intern. Med. 2020, 172, 621–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, S.; Hill, E.M.; Tildesley, M.J.; Dyson, L.; Keeling, M.J. Vaccination and non-pharmaceutical interventions for COVID-19: A mathematical modelling study. Lancet. Infect. Dis. 2021, 21, 793–802. [Google Scholar] [CrossRef]
- Hwang, H.; Lim, J.S.; Song, S.A.; Achangwa, C.; Sim, W.; Kim, G.; Ryu, S. Transmission Dynamics of the Delta Variant of SARS-CoV-2 Infections in South Korea. J. Infect. Dis. 2022, 225, 793–799. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Ali, S.T.; Kim, S.; Jo, J.; Lim, J.S.; Lee, S.; Ryu, S. Estimation of Serial Interval and Reproduction Number to Quantify the Transmissibility of SARS-CoV-2 Omicron Variant in South Korea. Viruses 2022, 14, 533. [Google Scholar] [CrossRef]
- Ryu, S.; Ali, S.T.; Noh, E.; Kim, D.; Lau, E.H.Y.; Cowling, B.J. Transmission dynamics and control of two epidemic waves of SARS-CoV-2 in South Korea. BMC Infect. Dis. 2021, 21, 485. [Google Scholar] [CrossRef]
- Ryu, S.; Ali, S.T.; Jang, C.; Kim, B.; Cowling, B.J. Effect of Nonpharmaceutical Interventions on Transmission of Severe Acute Respiratory Syndrome Coronavirus 2, South Korea, 2020. Emerg. Infect. Dis. 2020, 26, 2406–2410. [Google Scholar] [CrossRef]
- Banatvala, J.E.; Anderson, T.B.; Reiss, B.B. Viruses in acute respiratory infection in a general community. Epidemiol. Infect. 1965, 63, 155–167. [Google Scholar] [CrossRef] [Green Version]
- Al-Harrasi, A.; Bhatia, S. Epidemiology Respiratory Infections: Types, Transmission, and Risks Associated with Co-Infections. Role Essent Oils Manag COVID-19. pp. 7–17. Available online: https://www.taylorfrancis.com/chapters/edit/10.1201/9781003175933-3/epidemiology-respiratory-infections-types-transmission-risks-associated-co-infections-ahmed-al-harrasi-saurabh-bhatia (accessed on 30 March 2022).
- Troeger, C.; Blacker, B.; Khalil, I.A.; Rao, P.C.; Cao, J.; Zimsen, S.R.M.; Albertson, S.B.; Deshpande, A.; Farag, T.; Abebe, Z.; et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.S.; Wood, T.; Jelley, L.; Jennings, T.; Jefferies, S.; Daniells, K.; Nesdale, A.; Dowell, T.; Turner, N.; Campbell-Stokes, P.; et al. Impact of the COVID-19 nonpharmaceutical interventions on influenza and other respiratory viral infections in New Zealand. Nat. Commun. 2021, 12, 1001. [Google Scholar] [CrossRef] [PubMed]
- Arellanos-Soto, D.; Padilla-Rivas, G.; Ramos-Jimenez, J.; Galan-Huerta, K.; Lozano-Sepulveda, S.; Martinez-Acuña, N.; Treviño-Garza, C.; Montes-de-Oca-Luna, R.; de-la-O-Cavazos, M.; Rivas-Estilla, A.M. Decline in influenza cases in Mexico after the implementation of public health measures for COVID-19. Sci. Rep. 2021, 11, 10730. [Google Scholar] [CrossRef]
- Tempia, S.; Walaza, S.; Bhiman, J.N.; McMorrow, M.L.; Moyes, J.; Mkhencele, T.; Meiring, S.; Quan, V.; Bishop, K.; McAnerney, J.M.; et al. Decline of influenza and respiratory syncytial virus detection in facility-based surveillance during the COVID-19 pandemic, South Africa, January to October 2020. Euro Surveill. 2021, 26, 2001600. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.; Shaman, J.; Pei, S. Quantifying the Impact of COVID-19 Nonpharmaceutical Interventions on Influenza Transmission in the United States. J. Infect. Dis. 2021, 224, 1500–1508. [Google Scholar] [CrossRef]
- Soo, R.J.J.; Chiew, C.J.; Ma, S.; Pung, R.; Lee, V.; Lee, V.J. Decreased Influenza Incidence under COVID-19 Control Measures, Singapore. Emerg. Infect. Dis. 2020, 26, 1933–1935. [Google Scholar] [CrossRef]
- Lee, H.-H.; Lin, S.-H. Effects of COVID-19 Prevention Measures on Other Common Infections, Taiwan. Emerg. Infect. Dis. 2020, 26, 2509. [Google Scholar] [CrossRef]
- Cowling, B.J.; Ali, S.T.; Ng, T.W.Y.; Tsang, T.K.; Li, J.C.M.; Fong, M.W.; Liao, Q.; Kwan, M.Y.; Lee, S.L.; Chiu, S.S.; et al. Impact assessment of non-pharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: An observational study. Lancet Public Health 2020, 5, e279–e288. [Google Scholar] [CrossRef]
- Lee, H.; Lee, H.; Song, K.H.; Kim, E.S.; Park, J.S.; Jung, J.; Ahn, S.; Jeong, E.K.; Park, H.; Kim, H.B. Impact of public health interventions on seasonal influenza activity during the COVID-19 outbreak in Korea. Clin. Infect. Dis. 2021, 73, e132–e140. [Google Scholar] [CrossRef]
- El-Heneidy, A.; Ware, R.S.; Robson, J.M.; Cherian, S.G.; Lambert, S.B.; Grimwood, K. Respiratory virus detection during the COVID-19 pandemic in Queensland, Australia. Aust. N. Z. J. Public Health 2022, 46, 10–15. [Google Scholar] [CrossRef]
- Chiu, S.S.; Cowling, B.J.; Peiris, J.S.M.; Chan, E.L.Y.; Wong, W.H.S.; Lee, K.P. Effects of Nonpharmaceutical COVID-19 Interventions on Pediatric Hospitalizations for Other Respiratory Virus Infections, Hong Kong. Emerg. Infect. Dis. 2022, 28, 62. [Google Scholar] [CrossRef] [PubMed]
- Kuitunen, I.; Artama, M.; Haapanen, M.; Renko, M. Record high parainfluenza season in children after relaxation of COVID-19 restrictions in fall 2021—A nationwide register study in Finland. Influenza Other Respi. Viruses 2022. [Google Scholar] [CrossRef]
- Ye, Q.; Liu, H. Impact of non-pharmaceutical interventions during the COVID-19 pandemic on common childhood respiratory viruses—An epidemiological study based on hospital data. Microbes Infect. 2022, 24, 104911. [Google Scholar] [CrossRef]
- Liu, P.; Xu, M.; Cao, L.; Su, L.; Lu, L.; Dong, N.; Jia, R.; Zhu, X.; Xu, J. Impact of COVID-19 pandemic on the prevalence of respiratory viruses in children with lower respiratory tract infections in China. Virol. J. 2021, 18, 159. [Google Scholar] [CrossRef]
- Kim, J.H.; Roh, Y.H.; Ahn, J.G.; Kim, M.Y.; Huh, K.; Jung, J.; Kang, J.M. Respiratory syncytial virus and influenza epidemics disappearance in Korea during the 2020-2021 season of COVID-19. Int. J. Infect. Dis. 2021, 110, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Wagatsuma, K.; Koolhof, I.S.; Shobugawa, Y.; Saito, R. Decreased human respiratory syncytial virus activity during the COVID-19 pandemic in Japan: An ecological time-series analysis. BMC Infect. Dis. 2021, 21, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Groves, H.E.; Piché-Renaud, P.-P.; Peci, A.; Farrar, D.S.; Buckrell, S.; Bancej, C.; Sevenhuysen, C.; Campigotto, A.; Gubbay, J.B.; Morris, S.K. The impact of the COVID-19 pandemic on influenza, respiratory syncytial virus, and other seasonal respiratory virus circulation in Canada: A population-based study. Lancet Reg. Health-Am. 2021, 1, 100015. [Google Scholar] [CrossRef]
- Yeoh, D.K.; Foley, D.A.; Minney-Smith, C.A.; Martin, A.C.; MacE, A.O.; Sikazwe, C.T.; Le, H.; Levy, A.; Blyth, C.C.; Moore, H.C. Impact of Coronavirus Disease 2019 Public Health Measures on Detections of Influenza and Respiratory Syncytial Virus in Children During the 2020 Australian Winter. Clin. Infect. Dis. 2021, 72, 2199–2202. [Google Scholar] [CrossRef]
- Vittucci, A.C.; Piccioni, L.; Coltella, L.; Ciarlitto, C.; Antilici, L.; Bozzola, E.; Midulla, F.; Palma, P.; Perno, C.F.; Villani, A. The Disappearance of Respiratory Viruses in Children during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 9550. [Google Scholar] [CrossRef]
- Park, S.; Michelow, I.C.; Choe, Y.J. Shifting Patterns of Respiratory Virus Activity Following Social Distancing Measures for Coronavirus Disease 2019 in South Korea. J. Infect. Dis. 2021, 224, 1900–1906. [Google Scholar] [CrossRef]
- Kuitunen, I.; Artama, M.; Haapanen, M.; Renko, M. Rhinovirus spread in children during the COVID-19 pandemic despite social restrictions—A nationwide register study in Finland. J. Med. Virol. 2021, 93, 6063–6067. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Zhu, Y.; Lou, J.; Chen, J.; Xie, X.; Mao, J. Rotavirus and adenovirus infections in children during COVID-19 outbreak in Hangzhou, China. Transl. Pediatr. 2021, 10, 2281–2286. [Google Scholar] [CrossRef]
- Nagakubo, Y.; Hirotsu, Y.; Maejima, M.; Shibusawa, M.; Hosaka, K.; Amemiya, K.; Sueki, H.; Hayakawa, M.; Mochizuki, H.; Tsutsui, T.; et al. Non-pharmaceutical interventions during the COVID-19 epidemic changed detection rates of other circulating respiratory pathogens in Japan. PLoS ONE 2022, 17, e0262874. [Google Scholar] [CrossRef]
- Chan, K.-S.; Liang, F.-W.; Tang, H.-J.; Toh, H.S.; Yu, W.-L. Collateral benefits on other respiratory infections during fighting COVID-19. Med. Clínica (Engl. Ed.) 2020, 155, 249–253. [Google Scholar] [CrossRef]
- Ryu, S.; Ali, S.T.; Cowling, B.J.; Lau, E.H.Y. Effects of School Holidays on Seasonal Influenza in South Korea, 2014–2016. J. Infect. Dis. 2020, 222, 832–835. [Google Scholar] [CrossRef] [PubMed]
- Hawryluck, L.; Gold, W.L.; Robinson, S.; Pogorski, S.; Galea, S.; Styra, R. SARS Control and Psychological Effects of Quarantine, Toronto, Canada. Emerg. Infect. Dis. 2004, 10, 1206. [Google Scholar] [CrossRef]
- Ali, S.T.; Lau, Y.C.; Shan, S.; Ryu, S.; Du, Z.; Wang, L.; Xu, X.-K.; Chen, D.; Xiong, J.; Tae, J.; et al. Prediction of Upcoming Global Infection Burden of Influenza Seasons after Relaxation of Public Health and Social Measures for COVID-19 Pandemic. SSRN Electron. J. 2022. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Achangwa, C.; Park, H.; Ryu, S.; Lee, M.-S. Collateral Impact of Public Health and Social Measures on Respiratory Virus Activity during the COVID-19 Pandemic 2020–2021. Viruses 2022, 14, 1071. https://doi.org/10.3390/v14051071
Achangwa C, Park H, Ryu S, Lee M-S. Collateral Impact of Public Health and Social Measures on Respiratory Virus Activity during the COVID-19 Pandemic 2020–2021. Viruses. 2022; 14(5):1071. https://doi.org/10.3390/v14051071
Chicago/Turabian StyleAchangwa, Chiara, Huikyung Park, Sukhyun Ryu, and Moo-Sik Lee. 2022. "Collateral Impact of Public Health and Social Measures on Respiratory Virus Activity during the COVID-19 Pandemic 2020–2021" Viruses 14, no. 5: 1071. https://doi.org/10.3390/v14051071