
Indirect Protection from Vaccinating Children against Influenza A Virus Infection in Households
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Laboratory Methods
2.3. Model Details and Inference
2.4. Model Specification
2.5. Model Adequacy and Comparison
2.6. Model Prediction
2.7. Sensitivity Analysis
3. Results
3.1. Study Participants
3.2. Household Transmission Dynamics
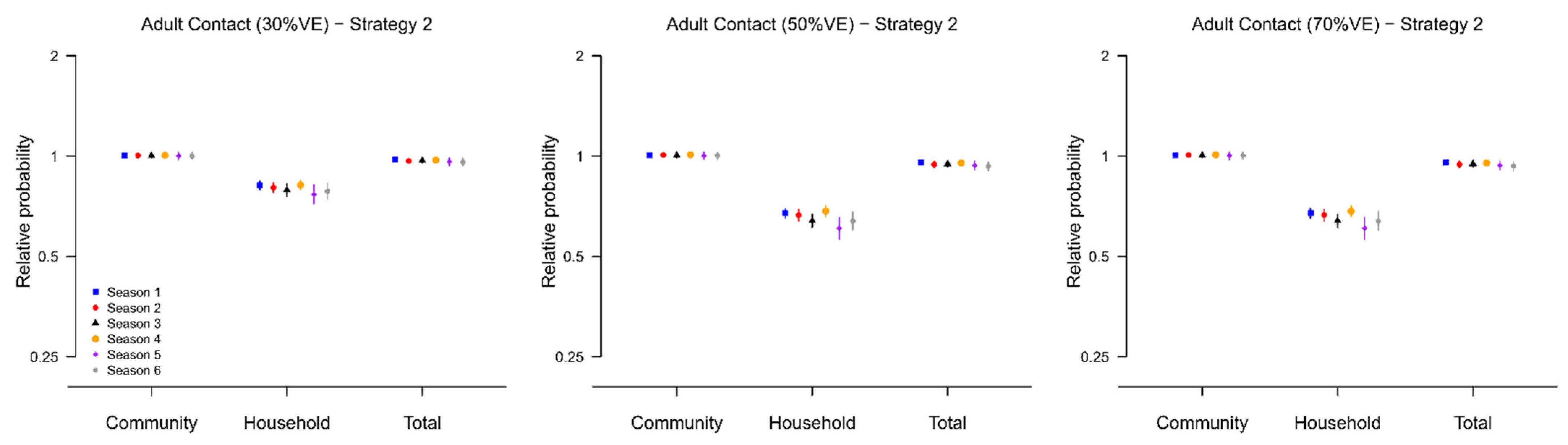
3.3. Indirect Effect of Vaccination
3.4. Model Adequacy
3.5. Sensitivity Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef]
- Dawood, F.S.; Iuliano, A.D.; Reed, C.; Meltzer, M.I.; Shay, D.K.; Cheng, P.Y.; Bandaranayake, D.; Breiman, R.F.; Brooks, W.A.; Buchy, P.; et al. Estimated global mortality associated with the first 12 months of 2009 pandemic influenza A H1N1 virus circulation: A modelling study. Lancet Infect. Dis. 2012, 12, 687–695. [Google Scholar] [CrossRef]
- Simonsen, L.; Reichert, T.A.; Viboud, C.; Blackwelder, W.C.; Taylor, R.J.; Miller, M.A. Impact of influenza vaccination on seasonal mortality in the US elderly population. Arch. Intern. Med. 2005, 165, 265–272. [Google Scholar] [PubMed]
- Jefferson, T.; Rivetti, A.; Harnden, A.; Di Pietrantonj, C.; Demicheli, V. Vaccines for preventing influenza in healthy children. Cochrane Database Syst Rev. 2008, 2, CD004879. [Google Scholar]
- Khanna, M.; Kumar, P.; Choudhary, K.; Kumar, B.; Vijayan, V.K. Emerging influenza virus: A global threat. J. Biosci. 2008, 33, 475–482. [Google Scholar] [CrossRef]
- Monto, A.S. Influenza: Quantifying morbidity and mortality. Am. J. Med. 1987, 82, 20–25. [Google Scholar] [CrossRef]
- Calatayud, L.; Kurkela, S.; Neave, P.E.; Brock, A.; Perkins, S.; Zuckerman, M.; Sudhanva, M.; Bermingham, A.; Ellis, J.; Pebody, R.; et al. Pandemic (H1N1) 2009 virus outbreak in a school in London, April-May 2009: An observational study. Epidemiol. Infect. 2010, 138, 183–191. [Google Scholar] [CrossRef]
- Cauchemez, S.; Valleron, A.J.; Boelle, P.Y.; Flahault, A.; Ferguson, N.M. Estimating the impact of school closure on influenza transmission from Sentinel data. Nature 2008, 452, 750–754. [Google Scholar] [CrossRef]
- Ferguson, N.M.; Cummings, D.A.; Fraser, C.; Cajka, J.C.; Cooley, P.C.; Burke, D.S. Strategies for mitigating an influenza pandemic. Nature 2006, 442, 448–452. [Google Scholar] [CrossRef]
- Belongia, E.A.; Simpson, M.D.; King, J.P.; Sundaram, M.E.; Kelley, N.S.; Osterholm, M.T.; McLean, H.Q. Variable influenza vaccine effectiveness by subtype: A systematic review and meta-analysis of test-negative design studies. Lancet Infect. Dis. 2016, 16, 942–951. [Google Scholar] [CrossRef]
- Osterholm, M.T.; Kelley, N.S.; Sommer, A.; Belongia, E.A. Efficacy and effectiveness of influenza vaccines: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 36–44. [Google Scholar] [CrossRef]
- Longini, I.M., Jr.; Halloran, M.E. Strategy for distribution of influenza vaccine to high-risk groups and children. Am. J. Epidemiol. 2005, 161, 303–306. [Google Scholar] [CrossRef] [PubMed]
- King, J.C., Jr.; Stoddard, J.J.; Gaglani, M.J.; Moore, K.A.; Magder, L.; McClure, E.; Rubin, J.D.; Englund, J.A.; Neuzil, K. Effectiveness of school-based influenza vaccination. N. Engl. J. Med. 2006, 355, 2523–2532. [Google Scholar] [CrossRef] [PubMed]
- Loeb, M.; Russell, M.L.; Moss, L.; Fonseca, K.; Fox, J.; Earn, D.J.; Aoki, F.; Horsman, G.; Van Caeseele, P.; Chokani, K.; et al. Effect of influenza vaccination of children on infection rates in Hutterite communities: A randomized trial. JAMA 2010, 303, 943–950. [Google Scholar] [CrossRef]
- Piedra, P.A.; Gaglani, M.J.; Kozinetz, C.A.; Herschler, G.; Riggs, M.; Griffith, M.; Fewlass, C.; Watts, M.; Hessel, C.; Cordova, J.; et al. Herd immunity in adults against influenza-related illnesses with use of the trivalent-live attenuated influenza vaccine (CAIV-T) in children. Vaccine 2005, 23, 1540–1548. [Google Scholar] [CrossRef] [PubMed]
- Tsang, T.K.; Fang, V.J.; Ip, D.K.M.; Perera, R.; So, H.C.; Leung, G.M.; Peiris, J.S.M.; Cowling, B.J.; Cauchemez, S. Indirect protection from vaccinating children against influenza in households. Nat. Commun. 2019, 10, 106. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Marchisio, P.; Cavagna, R.; Gironi, S.; Bosis, S.; Lambertini, L.; Droghetti, R.; Principi, N. Effectiveness of influenza vaccination of children with recurrent respiratory tract infections in reducing respiratory-related morbidity within the households. Vaccine 2003, 21, 3162–3168. [Google Scholar] [CrossRef]
- Hurwitz, E.S.; Haber, M.; Chang, A.; Shope, T.; Teo, S.; Ginsberg, M.; Waecker, N.; Cox, N.J. Effectiveness of influenza vaccination of day care children in reducing influenza-related morbidity among household contacts. JAMA 2000, 284, 1677–1682. [Google Scholar] [CrossRef]
- Belshe, R.B.; Mendelman, P.M.; Treanor, J.; King, J.; Gruber, W.C.; Piedra, P.; Bernstein, D.I.; Hayden, F.G.; Kotloff, K.; Zangwill, K.; et al. The efficacy of live attenuated, cold-adapted, trivalent, intranasal influenzavirus vaccine in children. N. Engl. J. Med. 1998, 338, 1405–1412. [Google Scholar] [CrossRef]
- Cauchemez, S.; Ferguson, N.M.; Fox, A.; Mai le, Q.; Thanh le, T.; Thai, P.Q.; Thoang, D.D.; Duong, T.N.; Minh Hoa le, N.; Tran Hien, N.; et al. Determinants of influenza transmission in South East Asia: Insights from a household cohort study in Vietnam. PLoS Pathog. 2014, 10, e1004310. [Google Scholar] [CrossRef]
- Chao, D.L.; Halloran, M.E.; Obenchain, V.J.; Longini, I.M., Jr. FluTE, a publicly available stochastic influenza epidemic simulation model. PLoS Comput. Biol. 2010, 6, e1000656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cowling, B.J.; Ng, S.; Ma, E.S.; Fang, V.J.; So, H.C.; Wai, W.; Cheng, C.K.; Wong, J.Y.; Chan, K.H.; Ip, D.K.; et al. Protective efficacy against pandemic influenza of seasonal influenza vaccination in children in Hong Kong: A randomized controlled trial. Clin. Infect. Dis. 2012, 55, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Cowling, B.J.; Ng, S.; Ma, E.S.; Cheng, C.K.; Wai, W.; Fang, V.J.; Chan, K.H.; Ip, D.K.; Chiu, S.S.; Peiris, J.S.; et al. Protective efficacy of seasonal influenza vaccination against seasonal and pandemic influenza virus infection during 2009 in Hong Kong. Clin. Infect. Dis. 2010, 51, 1370–1379. [Google Scholar] [CrossRef] [PubMed]
- Cowling, B.J.; Perera, R.A.; Fang, V.J.; Chan, K.H.; Wai, W.; So, H.C.; Chu, D.K.; Wong, J.Y.; Shiu, E.Y.; Ng, S.; et al. Incidence of influenza virus infections in children in Hong Kong in a 3-year randomized placebo-controlled vaccine study, 2009–2012. Clin. Infect. Dis. 2014, 59, 517–524. [Google Scholar] [CrossRef]
- Cowling, B.J.; Chan, K.H.; Fang, V.J.; Lau, L.L.H.; So, H.C.; Fung, R.O.P.; Ma, E.S.K.; Kwong, A.S.K.; Chan, C.W.; Tsui, W.W.S.; et al. Comparative epidemiology of pandemic and seasonal influenza A in households. N. Engl. J. Med. 2010, 362, 2175–2184. [Google Scholar] [CrossRef]
- Demiris, N.; O’Neill, P.D. Bayesian inference for stochastic multitype epidemics in structured populations via random graphs. J. R. Stat. Soc. Ser. B 2005, 67, 731–745. [Google Scholar] [CrossRef]
- Longini, I.M., Jr.; Koopman, J.S.; Monto, A.S.; Fox, J.P. Estimating household and community transmission parameters for influenza. Am. J. Epidemiol. 1982, 115, 736–751. [Google Scholar] [CrossRef]
- O’Neill, P.D.; Balding, D.J.; Becker, N.G.; Eerola, M.; Mollison, D. Analyses of infectious disease data from household outbreaks by Markov Chain Monte Carlo methods. Appl. Statist. 2000, 49, 517–542. [Google Scholar] [CrossRef]
- Hobson, D.; Curry, R.L.; Beare, A.S.; Ward-Gardner, A. The role of serum haemagglutination-inhibiting antibody in protection against challenge infection with influenza A2 and B viruses. J. Hyg. 1972, 70, 767–777. [Google Scholar] [CrossRef]
- Spiegelhalter, D.J.; Best, N.; Carlin, B.; Van Der Linde, A. Bayesian Measures of Model Complexity and Fit. J. R. Stat. Soc. B 2002, 64, 583–639. [Google Scholar] [CrossRef]
- Spiegelhalter, D.J.; Thomas, A.; Best, N.G. WinBUGS Version 1.3 User Manual; MRC Biostatistics Unit: Cambridge, UK, 2000. [Google Scholar]
- Celeux, G.; Forbes, F.; Robert, C.P.; Titterington, D.M. Deviance Information Criteria for Missing Data Models. Bayesian Anal. 2006, 1, 651–673. [Google Scholar] [CrossRef]
- Liu, J.S. Monte Carlo Strategies in Scientific Computing; Springer: New York, NY, USA, 2001. [Google Scholar]
- Cowling, B.J.; Chan, K.H.; Fang, V.J.; Cheng, C.K.; Fung, R.O.; Wai, W.; Sin, J.; Seto, W.H.; Yung, R.; Chu, D.W.; et al. Facemasks and hand hygiene to prevent influenza transmission in households: A cluster randomized trial. Ann. Intern. Med. 2009, 151, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Tsang, T.K.; Fang, V.J.; Chan, K.H.; Ip, D.K.; Leung, G.M.; Peiris, J.S.; Cowling, B.J.; Cauchemez, S. Individual Correlates of Infectivity of Influenza A Virus Infections in Households. PLoS ONE 2016, 11, e0154418. [Google Scholar]
- Chan, D.P.; Wong, N.S.; Wong, E.L.; Cheung, A.W.; Lee, S.S. Household characteristics and influenza vaccination uptake in the community-dwelling elderly: A cross-sectional study. Prev. Med. Rep. 2015, 2, 803–808. [Google Scholar] [CrossRef]
- Tsang, T.K.; Cauchemez, S.; Perera, R.A.; Freeman, G.; Fang, V.J.; Ip, D.K.; Leung, G.M.; Malik Peiris, J.S.; Cowling, B.J. Association between antibody titers and protection against influenza virus infection within households. J. Infect. Dis. 2014, 210, 684–692. [Google Scholar] [CrossRef]
- Cauchemez, S.; Bhattarai, A.; Marchbanks, T.L.; Fagan, R.P.; Ostroff, S.; Ferguson, N.M.; Swerdlow, D.; Pennsylvania H1N1 Working Group. Role of social networks in shaping disease transmission during a community outbreak of 2009 H1N1 pandemic influenza. Proc. Natl. Acad. Sci. USA 2011, 108, 2825–2830. [Google Scholar] [CrossRef]
- Cauchemez, S.; Carrat, F.; Viboud, C.; Valleron, A.J.; Boelle, P.Y. A Bayesian MCMC approach to study transmission of influenza: Application to household longitudinal data. Stat. Med. 2004, 23, 3469–3487. [Google Scholar] [CrossRef]
- Cauchemez, S.; Donnelly, C.A.; Reed, C.; Ghani, A.C.; Fraser, C.; Kent, C.K.; Finelli, L.; Ferguson, N.M. Household transmission of 2009 pandemic influenza A (H1N1) virus in the United States. N. Engl. J. Med. 2009, 361, 2619–2627. [Google Scholar] [CrossRef]
- Dahlgren, F.S.; Foppa, I.M.; Stockwell, M.S.; Vargas, C.Y.; LaRussa, P.; Reed, C. Household transmission of influenza A and B within a prospective cohort during the 2013–2014 and 2014–2015 seasons. Stat. Med. 2021, 40, 6260–6276. [Google Scholar] [CrossRef]
- Tsang, T.K.; Cowling, B.J.; Fang, V.J.; Chan, K.H.; Ip, D.K.; Leung, G.M.; Peiris, J.S.; Cauchemez, S. Influenza A Virus Shedding and Infectivity in Households. J. Infect. Dis. 2015, 212, 1420–1428. [Google Scholar] [CrossRef]
- Tsang, T.K.; Lau, L.L.; Cauchemez, S.; Cowling, B.J. Household Transmission of Influenza Virus. Trends Microbiol. 2016, 24, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Cauchemez, S.; Horby, P.; Fox, A.; Mai le, Q.; Thanh le, T.; Thai, P.Q.; Hoa le, N.M.; Hien, N.T.; Ferguson, N.M. Influenza infection rates, measurement errors and the interpretation of paired serology. PLoS Pathog. 2012, 8, e1003061. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors in the Models | ∆DIC |
|---|---|
| Age relative susceptibility + household size + protection of HAI titer | 0 |
| Age relative susceptibility + household size + protection of HAI titer + age relative infectivity | 30.3 |
| Age relative susceptibility + protection of HAI titer | 38.3 |
| Age relative susceptibility + household size | 372.9 |
| household size + protection of HAI titer | 494.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsang, T.K.; Wang, C.; Fang, V.J.; Perera, R.A.P.M.; So, H.C.; Ip, D.K.M.; Peiris, J.S.M.; Leung, G.M.; Cauchemez, S.; Cowling, B.J. Indirect Protection from Vaccinating Children against Influenza A Virus Infection in Households. Viruses 2022, 14, 2097. https://doi.org/10.3390/v14102097
Tsang TK, Wang C, Fang VJ, Perera RAPM, So HC, Ip DKM, Peiris JSM, Leung GM, Cauchemez S, Cowling BJ. Indirect Protection from Vaccinating Children against Influenza A Virus Infection in Households. Viruses. 2022; 14(10):2097. https://doi.org/10.3390/v14102097
Chicago/Turabian StyleTsang, Tim K., Can Wang, Vicky J. Fang, Ranawaka A. P. M. Perera, Hau Chi So, Dennis K. M. Ip, J. S. Malik Peiris, Gabriel M. Leung, Simon Cauchemez, and Benjamin J. Cowling. 2022. "Indirect Protection from Vaccinating Children against Influenza A Virus Infection in Households" Viruses 14, no. 10: 2097. https://doi.org/10.3390/v14102097