
Updates on the Epidemiology of the Human T-Cell Leukemia Virus Type 1 Infection in the Countries of the Eastern Mediterranean Regional Office of the World Health Organization with Special Emphasis on the Situation in Iran

 , and
, and
Abstract
:1. Introduction
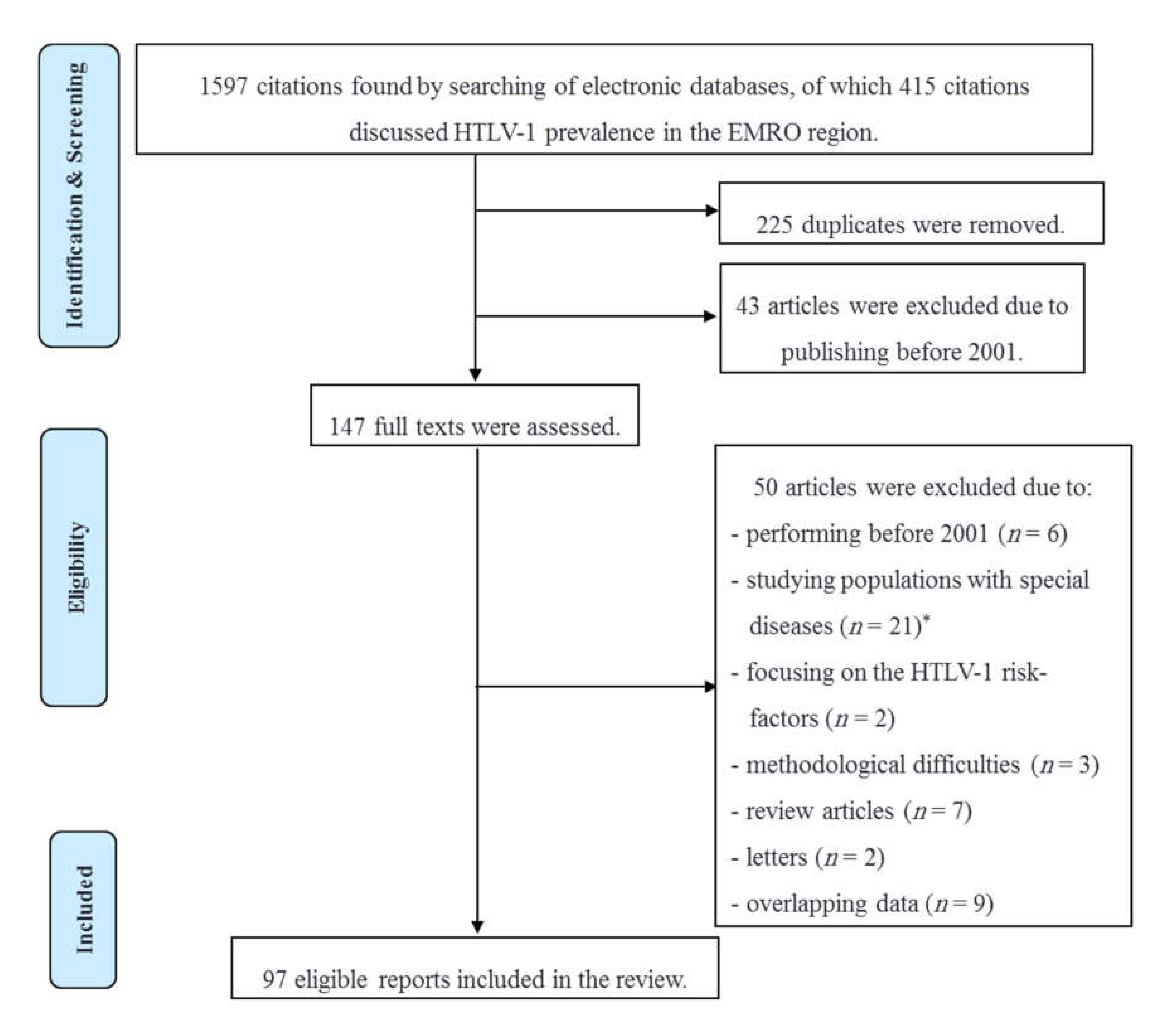
2. Material and Methods
3. Results and Discussion
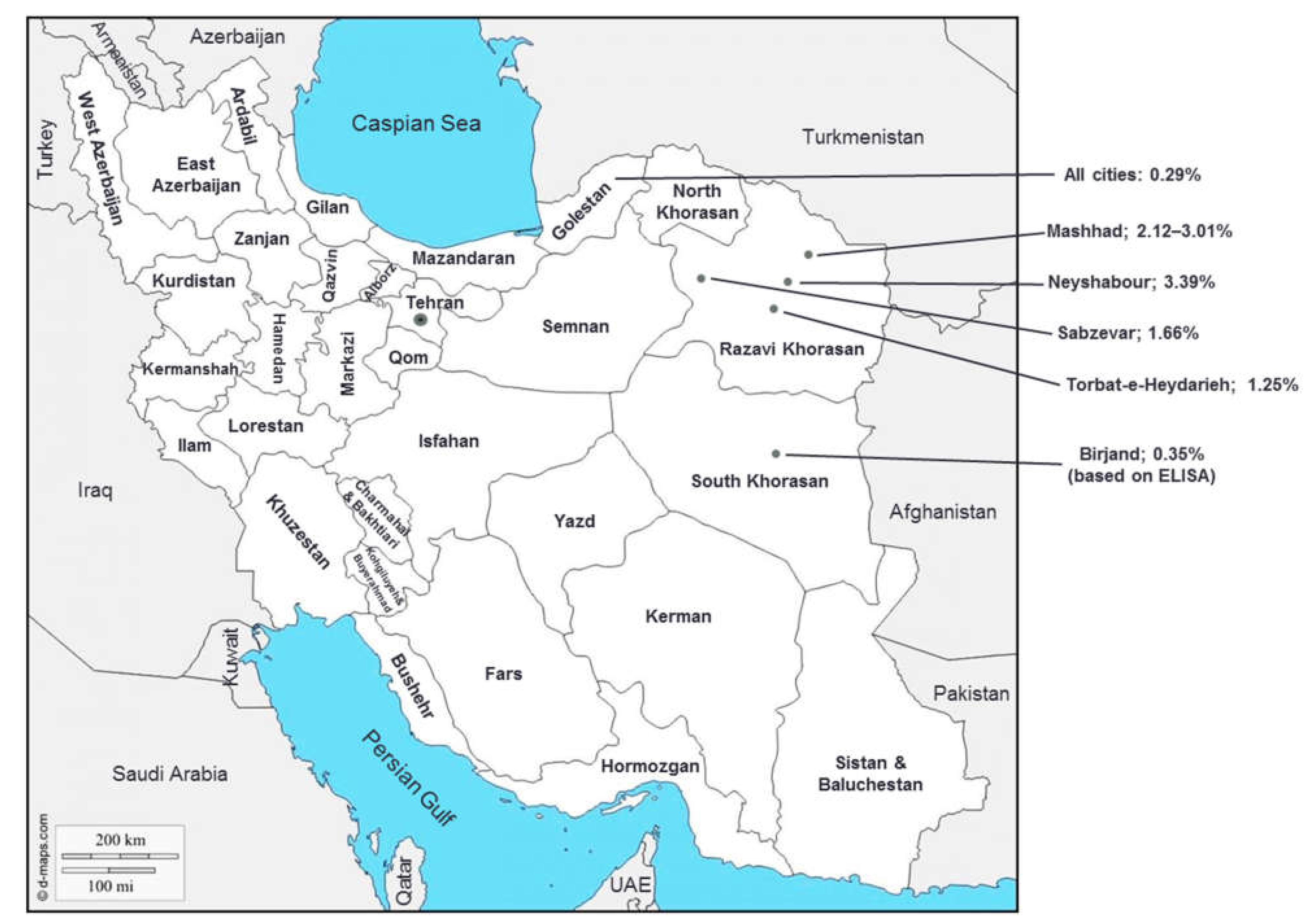
3.1. HTLV-1 Infection in Iran
3.1.1. HTLV-1 Infection in Iranian Low-Risk Population
3.1.2. HTLV-1 Infection among High-Risk Iranian Population
3.2. HTLV-2 Infection in Iran
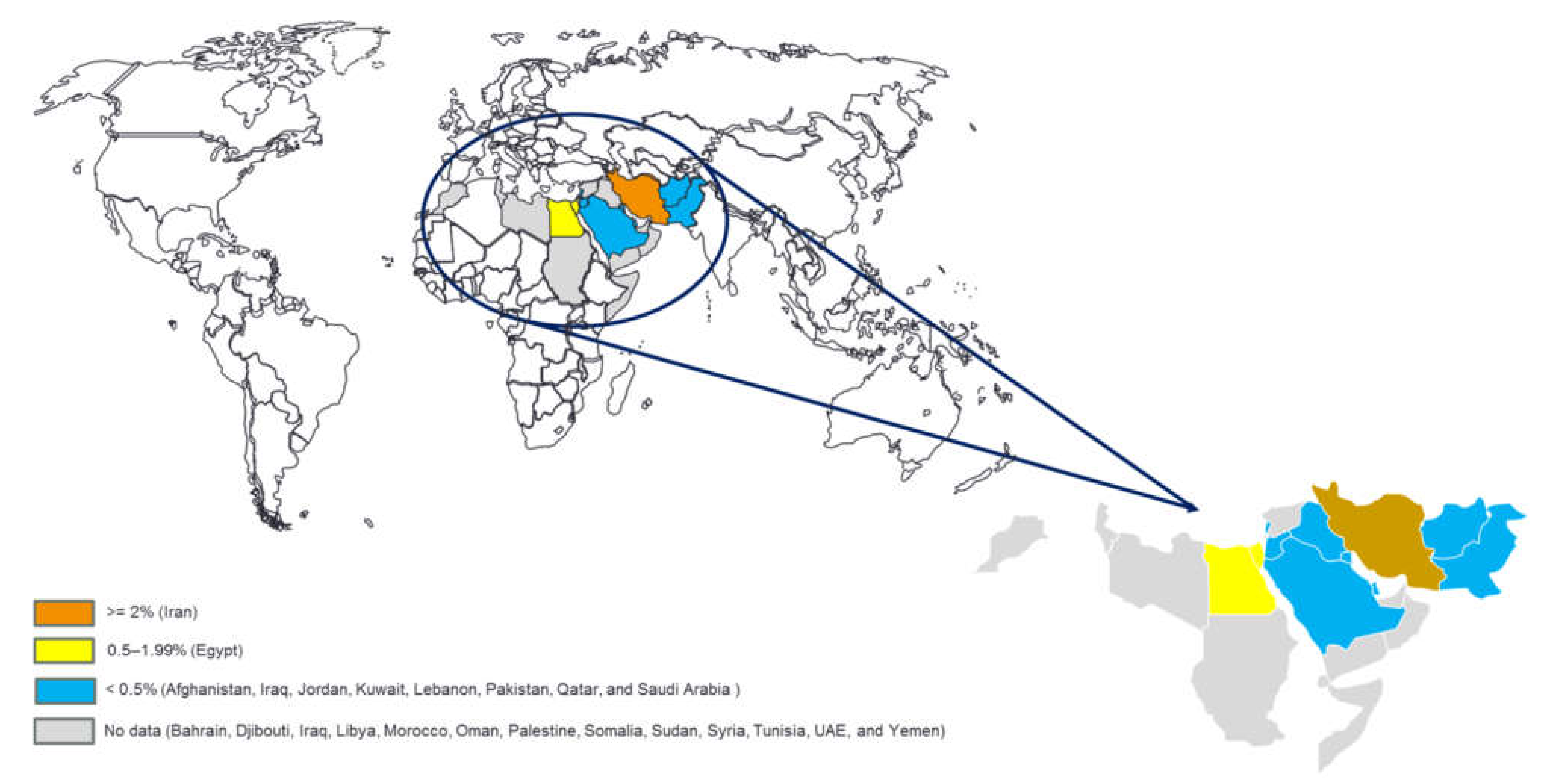
3.3. HTLV-1 Infection in EMRO Countries except for Iran
3.3.1. HTLV-1 Infection in Asian Countries of EMRO
3.3.2. HTLV-1 Infection in African Countries of EMRO
3.4. Study Limitations
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Poiesz, B.J.; Ruscetti, F.W.; Gazdar, A.F.; Bunn, P.A.; Minna, J.D.; Gallo, R.C. Detection and isolation of type C retrovirus particles from fresh and cultured lymphocytes of a patient with cutaneous T-cell lymphoma. Proc. Natl. Acad. Sci. USA 1980, 77, 7415–7419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalyanaraman, V.S.; Sarngadharan, M.G.; Robert-Guroff, M.; Miyoshi, I.; Blayney, D.; Golde, D.; Gallo, R.C. A new subtype of human t-cell leukemia virus (HTLV-II) associated with a t-cell variant of hairy cell leukemia. Science 1982, 218, 571–573. [Google Scholar] [CrossRef] [PubMed]
- Willems, L.; Hasegawa, H.; Accolla, R.; Bangham, C.; Bazarbachi, A.; Bertazzoni, U.; Carneiro-Proietti, A.B.D.F.; Cheng, H.; Chieco-Bianchi, L.; Ciminale, V.; et al. Reducing the global burden of HTLV-1 infection: An agenda for research and action. Antivir. Res. 2016, 137, 41–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gessain, A.; Cassar, O. Epidemiological Aspects and World Distribution of HTLV-1 Infection. Front. Microbiol. 2012, 3, 388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catovsky, D.; Greaves, M.F.; Rose, M.; Galton, D.A.; Goolden, A.W.; McCluskey, D.R.; White, J.M.; Lampert, I.; Bourikas, G.; Ireland, R.; et al. Adult T-cell lymphoma-leukaemia in Blacks from the West Indies. Lancet 1982, 1, 639–643. [Google Scholar] [CrossRef]
- Harrington, W.J., Jr.; Ucar, A.; Gill, P.; Snodgrass, S.; Sheremata, W.; Cabral, L.; Rabin, M.; Byrne, G.E., Jr.; Berger, J.; Voight, W.; et al. Clinical spectrum of HTLV-I in south Florida. J. Acquir. Immune Defic. Syndr. Hum. Retrovirology 1995, 8, 466–473. [Google Scholar] [CrossRef]
- Afonso, P.V.; Cassar, O.; Gessain, A. Molecular epidemiology, genetic variability and evolution of HTLV-1 with special emphasis on African genotypes. Retrovirology 2019, 16, 39. [Google Scholar] [CrossRef] [Green Version]
- Cassar, O.; Einsiedel, L.; Afonso, P.V.; Gessain, A. Human T-cell lymphotropic virus type 1 subtype c molecular variants among indigenous Australians: New insights into the molecular epidemiology of HTLV-1 in Australo-melanesia. PLoS Neglected Trop. Dis. 2013, 7, e2418. [Google Scholar] [CrossRef] [Green Version]
- Percher, F.; Jeannin, P.; Martin-Latil, S.; Gessain, A.; Afonso, P.V.; Vidy-Roche, A.; Ceccaldi, P.-E. Mother-to-Child Transmission of HTLV-1 Epidemiological Aspects, Mechanisms and Determinants of Mother-to-Child Transmission. Viruses 2016, 8, 40. [Google Scholar] [CrossRef] [Green Version]
- Roucoux, D.F.; Wang, B.; Smith, D.; Nass, C.C.; Smith, J.; Hutching, S.T.; Newman, B.; Lee, T.; Chafets, D.M.; Murphy, E.L.; et al. A prospective study of sexual transmission of human T lymphotropic virus (HTLV)–I and HTLV-II. J. Infect. Dis. 2005, 191, 1490–1497. [Google Scholar] [CrossRef] [Green Version]
- Murphy, E. Infection with human T-lymphotropic virus types-1 and -2 (HTLV-1 and -2): Implications for blood transfusion safety. Transfus. Clin. Biol. 2016, 23, 13–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowhani-Rahbar, A.; Tabatabee-Yazdi, A.; Panahi, M. Prevalence of common blood-borne infections among imprisoned injection drug users in Mashhad, North-East of Iran. Arch. Iran. Med. 2004, 7, 190–194. [Google Scholar]
- Proietti, F.A.; Carneiro-Proietti AB, F.; Catalan-Soares, B.C.; Murphy, E.L. Global epidemiology of HTLV-I infection and associated diseases. Oncogene 2005, 24, 6058–6068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schierhout, G.; McGregor, S.; Gessain, A.; Einsiedel, L.; Martinello, M.; Kaldor, J. Association between HTLV-1 infection and adverse health outcomes: A systematic review and meta-analysis of epidemiological studies. Lancet Infect. Dis. 2019, 20, 133–143. [Google Scholar] [CrossRef]
- Keikha, M.; Karbalaei, M. Overview on coinfection of HTLV-1 and tuberculosis: Mini-review. J. Clin. Tuberc. Other Mycobact. Dis. 2021, 23, 100224. [Google Scholar] [CrossRef] [PubMed]
- Page, J.B.; Lai, S.H.; Chitwood, D.D.; Klimas, N.G.; Smith, P.C.; Fletcher, M.A. HTLV-I/II seropositivity and death from AIDS among HIV-1 seropositive intravenous drug users. Lancet 1990, 335, 1439–1441. [Google Scholar] [CrossRef]
- World Health Organization. Human T-Lymphotropic Virus Type 1: Technical Report; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization Regional Office for the Eastern Mediterranean. Available online: http://www.emro.who.int/countries.html (accessed on 15 May 2021).
- Azarpazhooh, M.R.; Hasanpour, K.; Ghanbari, M.; Rezaee, S.R.; Mashkani, B.; Hedayati-Moghaddam, M.R.; Valizadeh, N.; Hosseini, R.F.; Foroghipoor, M.; Soltanifar, A.; et al. Human T-lymphotropic virus type 1 prevalence in northeastern Iran, Sabzevar: An epidemiologic-based study and phylogenetic analysis. AIDS Res. Hum. Retrovir. 2012, 28, 1095–1101. [Google Scholar] [CrossRef]
- Kalavi, K.; Moradi, A.; Tabarraei, A. Population-based Seroprevalence of HTLV-I Infection in Golestan Province, South East of Caspian Sea, Iran. Iran J. Basic Med. Sci. 2013, 16, 225–228. [Google Scholar]
- Rafatpanah, H.; Hedayati-Moghaddam, M.R.; Fathimoghadam, F.; Bidkhori, H.R.; Shamsian, S.K.; Ahmadi, S.; Sohgandi, L.; Azarpazhooh, M.R.; Rezaee, S.A.; Farid, R.; et al. High prevalence of HTLV-I infection in Mashhad, Northeast Iran: A population-based seroepidemiology survey. J. Clin. Virol. 2011, 52, 172–176. [Google Scholar] [CrossRef]
- Rafatpanah, H.; Torkamani, M.; Valizadeh, N.; Vakili, R.; Meshkani, B.; Khademi, H.; Gerayli, S.; Mozhgani, S.H.R.; Rezaee, S.A. Prevalence and phylogenetic analysis of HTLV-1 in a segregated population in Iran. J. Med. Virol. 2016, 88, 1247–1253. [Google Scholar] [CrossRef]
- Yousefi, M.; Sharifzadeh, G.R.; Ebrahimzadeh, A.; Azarkar, Z.; Namaei, M.H.; Azarkar, G.; Ghezeldasht, S.A.; Rezaee, R.; Zare, N.V.; Mosavat, A.; et al. Prevalence and Associated Risk Factors of HTLV-1 and Co-infections of Blood-Borne Viruses in Birjand, Iran’s Eastern Border. Arch. Iran. Med. 2020, 23, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Farid Hoseini, R.; Parizadeh, M.; Ghafari, J.; Miri, S.; Nasirian, A.; Rafatpanah, H. Seroepidemiology of HTLV-1 infection in Neyshabour. Med. J. Mashad Univ. Med. Sci. 2005, 47, 417–424. (In Persian) [Google Scholar]
- Rezvan, H.; Ahmadi, J.; Farhadi, M. A cluster of HTLV1 infection in northeastern of Iran. Transfus. Today 1996, 27, 8–9. [Google Scholar]
- Safai, B.; Huang, J.-L.; Boeri, E.; Farid, R.; Raafat, J.; Schutzer, P.; Ahkami, R.; Franchini, G. Prevalence of HTLV Type I Infection in Iran: A Serological and Genetic Study. AIDS Res. Hum. Retrovir. 1996, 12, 1185–1190. [Google Scholar] [CrossRef]
- Hedayati-Moghaddam, M.R.; Fathimoghadam, F.; Eftekharzadeh Mashhadi, I.; Soghandi, L.; Bidkhori, H.R. Epidemiology of HTLV-1 in Neyshabour, Northeast of Iran. Iran. Red Crescent Med. J. 2011, 13, 424–427. [Google Scholar]
- Keramati, M.R.; Sadeghian, M.H.; Ayatollahi, H. Clinical and laboratory features in adult T-cell leukemia/lymphoma in Khorasan, Iran. Leuk. Lymphoma 2010, 51, 727–729. [Google Scholar] [CrossRef]
- Shoeibi, A.; Rafatpanah, H.; Azarpazhooh, A.; Mokhber, N.; Hedayati-Moghaddam, M.R.; Amiri, A.; Hashemi, P.; Foroghipour, M.; Hoseini, R.F.; Bazarbachi, A.; et al. Clinical features of HTLV-1-associated myelopathy/tropical spastic paraparesis (HAM/TSP) in northeast Iran. Acta Neurol. Belg. 2013, 113, 427–433. [Google Scholar] [CrossRef]
- Darroudi, S.; Abolbashari, S.; Ahangari, N.; Tayefi, M.; Khashyarmanesh, Z.; Zamani, P.; Haghighi, H.M.; Mohammadpour, A.H.; Tavalaei, S.; Esmaily, H.; et al. Association Between Trace Element Status and Depression in HTLV-1-Infected Patients: A Retrospective Cohort Study. Biol. Trace Element Res. 2019, 191, 75–80. [Google Scholar] [CrossRef]
- Karimi, G.; Zadsar, M.; Pourfathollah, A.A. Seroprevalence and geographical distribution of human T-lymphotropic virus type 1 among volunteer blood donors in endemic areas of Iran. Virol. J. 2017, 14, 14. [Google Scholar] [CrossRef] [Green Version]
- Omidkhoda, A.; Razi, B.; Arabkhazaeli, A.; Kafi-Abad, S.A. Trends and epidemiological analysis of hepatitis B virus, hepatitis C virus, human immunodeficiency virus, and human T-cell lymphotropic virus among Iranian blood donors: Strategies for improving blood safety. BMC Infect. Dis. 2020, 20, 736. [Google Scholar] [CrossRef]
- Poukarim, M.R.; Khamisipour, G.; Zandi, K.; Roustaee, M.H. Prevalence of anti-HTLV-I & anti- HTLV-II antibodies in blood donors in Bushehr province. Iran South Med. J. 2004, 6, 161–164. (In Persian) [Google Scholar]
- Karimi, A.; Nafici, M.; Imani, R. Comparison of human T-cell leukemia virus type-1 [HTLV-1]seroprevalence in high risk patients [thalassemia and hemodialysis]and healthy individuals from charmahal-Bakhtiari province, Iran. KMJ-Kuwait Med. J. 2007, 39, 259–261. [Google Scholar]
- Arjmandi, F.; Shahriari, M.; Sadeghi Hasanabadi, A. A comparitive study of the prevalence of HTLV–I infection in luekemia/ non–hodgkins lymphoma patients, thalassemic patients and blood donors. J. Shahid Sadoughi Univ. Med. Sci. 2003, 10, 25–29. [Google Scholar]
- Habibabadi, H.M.; Parsania, M.; Pourfathollah, A.A.; Bahrami, A.; Sharifi, Z. Prevalence and phylogenetic analysis of HTLV-1 in blood donors in Golestan Province, in the Northeast of Iran. J. Virol. Methods 2021, 290, 114073. [Google Scholar] [CrossRef]
- Abedi, F.; Yavarian, M.; Shakibzadeh, A.; Khalvati, B.; Asadi, A. A pilot Seroepidemiologic study of HTLV in thalassemia, hemophilia, and hemodialysed patients in Hormozgan. Hormozgan Med. J. 2009, 13, e88635. [Google Scholar]
- Zalei, B.; Pourmand, D.; Rahmani, Y.; Bilvaye, S. Investigating the prevalence of HTLV and HCV infection in blood donors (for the first time) in blood transfusion organization of Kermanshah, Iran. Ann. Clin. Anal. Med. 2017, 8, 509–512. [Google Scholar] [CrossRef]
- Ghadiri, K.; Hashemian, A.; Rezaei, M.; Payandeh, M.; Zare, M.E. Serologic prevalence of human T-lymphotropic virus (HTLV) among major thalassemic patients in Kermanshah 2010. Int. J. Hematol.-Oncol. Stem Cell Res. 2011, 5, 14–17. [Google Scholar]
- Yahyapour, Y.; Aghajanipour, K.; Mir, S.M.; Khademian, A.; Sadeghi, F. Human T- Lymphotropic Virus Type 1 in Blood Donors from Babol County Blood Transfusion Center: A Pilot Study From Northern Iran. Jundishapur J. Microbiol. 2017, 10, e13757. [Google Scholar] [CrossRef] [Green Version]
- Tarhini, M.; Kchour, G.; Zanjani, D.S.; Rafatpanah, H.; Otrock, Z.K.; Bazarbachi, A.; Farid, R. Declining tendency of human T-cell leukaemia virus type I carrier rates among blood donors in Mashhad, Iran. Pathology 2009, 41, 498–499. [Google Scholar] [CrossRef]
- Hatami, H.; Karimi, G.; Safabakhsh, H.R. Seroepidemiologic prevalence of HTLV in voluntary blood donors in Mashhad. Sci. J. Iran. Blood Transfus. Organ. 2012, 9, 149–159. [Google Scholar]
- Sayadpour Zanjani, D.; Shahabi, M.; Talaei, N.; Afzalaghaee, M.; Tehranian, F.; Bazargani, R. Molecular Analysis of Human T Cell Lymphotropic Virus Type 1 and 2 (HTLV-1/2) Seroindeterminate Blood Donors from Northeast Iran: Evidence of Proviral tax, env, and gag Sequences. AIDS Res. Hum. Retrovir. 2011, 27, 131–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Safabakhsh, H.r.; Karimi, G.; Hatami, H. The prevalence of HTLV-1 infection in blood donation volunteers in Mashhad. J. Sch. Public Health Inst. Public Health Res. 2014, 11, 85–94. [Google Scholar]
- Tabriznia Tabrizi, S.; Gholampour, M.; Zarmehri, A.M.; Sadeghian, M.H.; Keramati, M.R. The frequency and risk factors of human T-cell lymphotropic virus type I among blood donors in Khorasan-e Razavi, Iran, from 2002 to 2013. Niger. Med. J. Niger. Med. Assoc. 2020, 61, 151–155. [Google Scholar] [CrossRef]
- Safabakhsh, H.; Jalalian, M.; Karimi, G. Seroepidemiology of human T-Cell lymphotropic virus Type-1 (HTLV1) in mashhad. Glob. J. Health Sci. 2014, 6, 99–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maghsudlu, M.; Safabakhsh, H.; Jamili, P. Seroepidemiology of human T-cell lymphotropic virus type-I in blood donors of Northeastern Iran, Sabzevar. Asian J. Transfus. Sci. 2015, 9, 203–206. [Google Scholar] [CrossRef]
- Ferdowsi, S.; Najafzadeh, M.; Ameli, M.R.; Sajjadi, S.M. Evaluating the Frequency of Human T-Lymphotropic Virus Type 1 Infection in Iranian Population. Iran. J. Blood Cancer 2019, 11, 47–50. [Google Scholar]
- Pirayeshfard, L.; Sharifi, Z.; Amini-Kafiabad, S.; Sadaghiani, N.H. Phylogenetic analysis of HTLV-1 in Iranian blood donors, HIV-1 positive patients and patients with beta thalassemia. J. Med. Virol. 2018, 90, 1398–1405. [Google Scholar] [CrossRef]
- Rostamzadeh Khameneh, Z.; Baradaran, M.; Sepehrvand, N. Survey of the seroprovalence of HTLV I/II in hemodialysis patients and blood donors in Urmia. Saudi J. Kidney Dis. Transplant. Off. Publ. Saudi Cent. Organ Transplant. Saudi Arab. 2008, 19, 838–841. [Google Scholar]
- Emadi, B.; Rezaieh, M.G.; Sedighi, M. Seroprevalence and trends of transfusion transmissible infections among retrospective blood donors in Western Azerbaijan Regional Blood Transfusion Center, Iran: A ten-years evaluation. Transfus. Apher. Sci. Off. J. World Apher. Assoc. Off. J. Eur. Soc. Haemapheresis 2021, 60, 103132. [Google Scholar] [CrossRef]
- Rezaei Kanavi, M.; Javadi, M.; Nazparvar, B.; Bayat Makoo, K. Seropositivity for human T-cell lymphotropic virus [HTL V] in donors at the eye bank of I.R. Iran. Bina J. Ohthalmol. 2008, 14, 40–43. [Google Scholar]
- Arjmand, B.; Aghayan, S.H.; Goodarzi, P.; Farzanehkhah, M.; Mortazavi, S.M.; Nicknam, M.H.; Jafarian, A.; Arjmand, F.; Far, S.J. Seroprevalence of human T lymphtropic virus (HTLV) among tissue donors in Iranian tissue bank. Cell Tissue Bank. 2008, 10, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Hamedi, A.; Akhlaghi, F.; Meshkat, Z.; Sezavar, M.; Nomani, H. The Prevalence of Human T-Cell lymphotropic Virus Type 1 in Pregnant Women and Their Newborns. ISRN Obstet. Gynecol. 2012, 2012, 975135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salehi, M.; Mostafavi, S.K.S.; Ghasemian, A.; Gholami, M.; Kazemi-Vardanjani, A.; Rahimi, M.K. Seroepidemiology of HTLV-1 and HTLV-2 Infection in Neyshabur City, North-Eastern Iran, during 2010–2014. Iran. Biomed. J. 2017, 21, 57–60. [Google Scholar] [CrossRef] [Green Version]
- Salehi, M.; Mobini, M. The seroepidemiological of Human T-lymphotropic virus on children, teenage and juveniles in Nyshabor city. Iran. J. Med. Microbiol. 2015, 9, 31–35. [Google Scholar]
- Mobini, M.; Salehi, M. Prevalence of Human T-cell Leukemia Virus Antibodies among Young Females Attending a Large Medical Diagnostic Laboratory in Neyshabour, Northeast of Iran, During 2011 to 2015. Arch. Clin. Infect. Dis. 2018, 13, e62305. [Google Scholar] [CrossRef] [Green Version]
- Ghaffari, J.; Naghshvar, F.; Nazari, Z.; Farid, R. Seroprevalence of human T-cell lymphotropic virus type 1 infection (HTLV1) in different patients in the north of Iran. Afr. J. Biotechnol. 2011, 10, 10752–10755. [Google Scholar] [CrossRef]
- Ghodsi, A.; Jamehdar, S.A.; Hamedi, A.K. Frequency of HTLV-1 Antibody in Children of 6 Months to 14 Years old Hospitalized in the Pediatric Ward of Imam Reza Hospital, Mashhad, Iran. Int. J. Pediatrics-Mashhad 2021, 9, 12975–12980. [Google Scholar] [CrossRef]
- Tahaei, S.M.E.; Mohebbi, S.R.; Fatemi, S.R.; Azimzadeh, P.; Mirsattari, D.; Sanati, A.; Sharifian, A. Evaluation of antibody frequency against HBV, HCV and HTLV-1. Gastroenterol. Hepatol. Bed Bench 2012, 5, 161–165. [Google Scholar]
- Razavi Pashabayg, C.; Momenifar, N.; Malekpour, S.A.; Sadeghi, M.; Foroushani, A.R.; Rafatpanah, H.; Valizadeh, N.; Sabet, F.; Jazayeri, S.M.; Keyvani, H.; et al. Phylogenetic and phylodynamic study of Human T-cell lymphotropic virus Type 1 (HTLV-1) in Iran. Infect. Genet. Evol. 2020, 85, 104426. [Google Scholar] [CrossRef]
- Hedayati-Moghaddam, M.R. A Systematic Review for Estimation of HTLV-I Infection in the Blood Donors of Iran. Iran. J. Basic Med. Sci. 2013, 16, 196–201. [Google Scholar] [CrossRef]
- Azami, M.; Badfar, G.; Esmaeli, E.; Moslemirad, M.; Rahmati, S. Epidemiology of human T-lymphotropic virus type 1 among blood donors and general population in Iran: A meta-analysis. Futur. Virol. 2018, 13, 585–599. [Google Scholar] [CrossRef]
- Rezvan, H.; Abolghassemi, H.; Kafiabad, S.A. Transfusion-transmitted infections among multitransfused patients in Iran: A review. Transfus. Med. 2007, 17, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Hedayati-Moghaddam, M.R.; Tehranian, F.; Bayati, M. Human T-Lymphotropic Virus Type I (HTLV-1) Infection among Iranian Blood Donors: First Case-Control Study on the Risk Factors. Viruses 2015, 7, 5736–5745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dayyani, M.; Hedayati-Moghaddam, M.R.; Amini, A.R. HTLV-1 infection as a serious health issue among iranian multi-transfused patients: Evidence from a systematic review and meta-analysis. Iran. J. Blood Cancer 2015, 7, 85–94. [Google Scholar]
- Ahmadi Ghezeldasht, S.; Hassannia, T.; Rafatpanah, H.; Hekmat, R.; Valizadeh, N.; Mobarhan, M.G.; Rezaee, S.A. Oncogenic Virus Infections in the General Population and End-stage Renal Disease Patients with Special Emphasis on Kaposi’s Sarcoma Associated Herpes Virus (KSHV) in Northeast of Iran. Jundishapur J. Microbiol. 2015, 8, e14920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedayati-Moghaddam, M.R.; Fathimoghadam, F.; Soghandi, L.; Darrudi, A. High Prevalence of HTLV-1 Infection Among Hemodialysis Patients in Neyshabur, Northeast of Iran. Int. J. Infect. 2019, 6, e85164. [Google Scholar] [CrossRef] [Green Version]
- Karimi, A.; Nafisi, M. Seroprevalence of Human T-Cell Leukemia Virus Type-1 (HTLV-1) in High Risk Patients. J. Res. Health Sci. 2006, 6, 44–47. [Google Scholar]
- Anaraki Mohammadi, G.; Sadeghipour, A.R.; Vossough, P.; Nour Mohammadi, I.; Mirnateghi, A.M. Assessment of the Prevalence of Human T-Lymphotropic Virus type 1 among Thalassemic Patients with Frequent Blood Transfusion in Tehran in 2003. Razi J. Med. Sci. 2005, 12, 19–24. [Google Scholar]
- Keshvari, M.; Hajibeigi, B.; Azarkeivan, A.; Keyvani, H.; Behnava, B.; Hosseini, S.Y.S.; Sharafi, H.; Alavian, S.M. Seroepidemiology of human T-cell lymphotropic virus among Iranian adult thalassemic patients. Transfus. Med. 2014, 24, 227–232. [Google Scholar] [CrossRef]
- Abbasnia, S.; Hassannia, T.; Ariaee, N.; Sabet, F.; Pashabayg, K.R.; Keyvani, H.; Sarv-Ghad, M.R.; Ziaeemehr, A.; Fakor, F.; Valizadeh, N. Immunovirological Assessment of HIV-Infected Patients and Phylogenetic Analysis of the Virus in Northeast of Iran. Jundishapur J. Microbiol. 2021, 14, e112123. [Google Scholar] [CrossRef]
- Alavi, S.M.; Etemadi, A. HIV/HBV, HIV/HCV and HIV/HTLV-1 Co infection among injecting drug user patients hospitalized at the infectious disease ward of a training hospital in Iran. Pak. J. Med. Sci. 2007, 23, 510–513. [Google Scholar]
- Khajedaluee, M.; Babaei, A.; Vakili, R.; Valizade, N.; Shandiz, F.H.; Alavian, S.M.; Nozadi, M.S.; Jazayeri, S.M.; Hassannia, T. Sero-Prevalence of Bloodborne Tumor Viruses (HCV, HBV, HTLV-I and KSHV Infections) and Related Risk Factors among Prisoners in Razavi Khorasan Province, Iran, in 2008. Hepat. Mon. 2016, 16, e31541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention and the U.S.P.H.S. Working Group. Guidelines for counseling persons infected with human T-lymphotropic virus type I (HTLV-I) and type II (HTLV-II). Ann. Intern. Med. 1993, 118, 448–454. [Google Scholar] [CrossRef]
- Pourkarim, M.; Khamisipour, G.; Hajiani, G.; Tahmasebi, R.; Ardeshirdavani, N. Seroepidemiological investigation of HTLV I, II infection among Busherian multi-transfused patients in 2003. Sci. J. Iran. Blood Transfus. Organ. 2005, 2, 99–104. [Google Scholar]
- Ardalan, N.; Abdi, M.; Zarif, B.R.; Amini, A.; Meamari, F.; Haydari, E.; Ahmadi, A. Prevalence of human T-lymphotropic virus types I & II among high risk groups in Sanandaj in 2010. Sci. J. Kurd. Univ. Med. Sci. 2013, 18, 51–57. [Google Scholar]
- Ghaffari, J.; Ebrahimi, M.; Makhlough, A.; Mohammadjafari, H.; Nazari, Z. Seroepidemiology of human T-cell lymphotropic virus 1 infection in hemodialysis patients: Should we be concerned about it? Iran. J. Kidney Dis. 2013, 7, 187–190. [Google Scholar]
- Ziaee, M.; Azizee, R.; Namaei, M.H.; Masood, Z.; Roghiya, A.; Hasan, N. Prevalence of HCV infection in hemodialysis patients of South Khorasan in comparison with HBV, HDV, HTLV I/II, And HIV infection. Bangladesh J. Med. Sci. 2013, 13, 36–39. [Google Scholar] [CrossRef] [Green Version]
- Yazdani, R.; Dadmanesh, M.; Ghorban, K. First Report of the Prevalence of Human T-Lymphotropic Virus Type 1 (HTLV-1) for Hemodialysis Patients in Tehran. Arch. Clin. Infect. Dis. 2018, 13, e65512. [Google Scholar] [CrossRef]
- Hatatian, F.; Babakhani, F.; Gudarzi, H.; Momenifar, N.; Norouzi, M.; Shafieifar, M.; Kakavandi, E.; Sadeghi, A.; Sharbatdar-Alaei, H.; Farahmand, M.; et al. Relative Frequency of Blood-Borne Viruses in Hemodialysis-Dependent and Kidney Transplant Recipients in Iran. Iran. J. Public Health 2020, 49, 2136–2143. [Google Scholar] [CrossRef]
- Moradi, A.; Mansurian, A.; Ahmadi, A.; Ghaemi, E.A.; Kalavi, K.; Marjani, A.; Moghaddam, E.S. Prevalence of HTLV-1 Antibody among Major Thalassemic Patients in Gorgan (South East of Caspian Sea). J. Appl. Sci. 2008, 8, 391–393. [Google Scholar] [CrossRef] [Green Version]
- Mortezaie, Z.; Bouzari, M.; Roghanian, R. Evaluating the frequency of HTLV-I/Π infection among blood donors, major thalassemic patients and individuals infected with hepatitis B and C viruses in Isfahan, Iran. Iran. J. Blood Cancer 2012, 4, 75–80. [Google Scholar]
- Mahzounieh, M.; Ghorani, M.; Karimi, A.; Pourgheysari, B.; Nikoozad, R. Prevalence of Human T-Lymphotropic Virus Types I and II in Patients with Hematological Disorders in Isfahan, Iran. Jundishapur J. Microbiol. 2015, 8, e17201. [Google Scholar] [CrossRef] [Green Version]
- Ghaffari, J.; Kowsarian, M.; Mahdavi, M.; Shahi, K.V.; Rafatpanah, H.; Tafreshian, A. Prevalence of HTLV-I Infection in Patients with Thalassemia Major in Mazandaran, North of Iran. Jundishapur J. Microbiol. 2012, 6, 57–60. [Google Scholar] [CrossRef]
- Hamidi, S.; Bashizadeh-Fakhar, H.; Nazemi, A. Identification of Human T-Cell Lymphotropic Virus Type 1 Pro-Invasion in Patients with β-Thalassemia Major Using TaqMan Real-Time PCR in Tonekabon, Iran. Zahedan J. Res. Med. Sci. 2018, 20, e59961. [Google Scholar] [CrossRef]
- Mansouritorghabeh, H.; Badiei, Z. Transfusion-Transmitted Viruses in Individuals with β Thalassemia Major at Northeastern Iran, a Retrospective Sero-Epidemiological Survey. Iran. J. Blood Cancer 2008, 1, 1–4. [Google Scholar]
- Abedi, F.; Mozhgani, S.-H.; Rahimzadegan, M.; Gudarzi, H.; Valizadeh, N.; Rezaee, S.A. Prevalence and phylogenic study of human T-lymphotropic virus 1 in patients with thalassemia in the northeast of Iran. Futur. Virol. 2017, 12, 253–258. [Google Scholar] [CrossRef]
- Ziaee, M.; Zarban, A.; Malekinejad, P.; Akhbary, H. Evaluation of HGV viremia prevalence and its co-infection with HBV, HCV, HIV and HTLV-1 in hemophilic patients of southern Khorassan, Iran. Hepat. Mon. 2007, 7, 11–14. [Google Scholar]
- Ziaee, M.; Namaei, M.H.; Azarkar, G. The prevalence of HTLV-1 and its Co-Infection with HCV, HBV and HIV in Hemophilic patients. Pak. J. Med. Sci. 2015, 31, 1246–1249. [Google Scholar] [CrossRef]
- Rostamzadeh, Z.; Valizadeh, N.; Mohammadian, M. Prevalence of Seropositivity for Human T lymphocytes Virus in Patients with Hereditary Bleeding Diseases in Population of West Azerbaijan. Int. J. Med. Lab. 2016, 3, 159–162. [Google Scholar]
- Mansouritorghabeh, H.; Farid Hosseini, R.; Pourfath Elah, A.A.; Behjati, A.A. Serological markers of blood borne viruses among persons with combined factor V & VIII deficiency. Hepat. Mon. 2008, 8, 221–224. [Google Scholar]
- Meidani, M.; Ahmadi, N.; Jamali, B.; Askarian, Z. Relative frequency of Human T-cell Lymphotropic Virus I/II in HIV/AIDS patients. Adv. Biomed. Res. 2014, 3, 8. [Google Scholar] [CrossRef] [PubMed]
- Meidani, M.; Farzaneh, S.; Baferani, A.; Zade, A. [Seroprevalence of HTLV1, 2 virus among injection drug addicts in Isfahan, 2007–2008]. J. Shaheed Sadoughi Univ. Med. Sci. 2009, 17, 286–290. [Google Scholar]
- Tavanaee Sani, A.; Khaleghinia, M. Epidemiologic evaluation and some species in injection drug users that admitted in infectious department of Imam Reza hospital [2007–2009]. J. Med. Counc. Iran 2012, 30, 155–161. [Google Scholar]
- Ramezani, A.; Aghakhani, A.; Banifazl, M.; Boland-Ghamat, Z.; Foroughi, M.; Gachkar, L.; Khadem-Sadegh, A.; Mohraz, M. Frequency of human T-Cell lymphotropic virus (HTLV) type 1 and 2 infection in HIV infected patients. Iran. J. Pathol. 2012, 7, 9–13. [Google Scholar]
- Abedi, F.; Saeedi, E.; Sharifzadeh, G.R.; Ziaee, M. Comparing the Prevalence of HTLV-1 and Its Risk Factors in Prisoners with Intravenous and Non-Intravenous Drug Use in Birjand. Mod. Care J. 2019, 16, e95601. [Google Scholar] [CrossRef]
- Rafatpanah, H.; Hedayati-Moghaddam, M.R.; Fathimoghadam, F.; Bidkhori, H.R.; Shamsian, S.K.; Ahmadi, S.; Sohgandi, L.; Azarpazhooh, M.R.; Rezaee, S.A.; Farid, R.; et al. Prevalence of human T-cell lymphotropic virus type 2 infection in general population of Mashhad, Iran. J. Isfahan Med. Sch. 2015, 32, 2260–2267. [Google Scholar]
- Rafatpanah, H.; Fathimoghadam, F.; Shahabi, M.; Eftekharzadeh, I.; Hedayati-Moghaddam, M.; Valizadeh, N.; Tadayon, M.; Shamsian, S.A.; Bidkhori, H.; Miri, R.; et al. No Evidence of HTLV-II Infection Among Immonoblot Indeterminate Samples Using Nested PCR in Mashhad, Northeast of Iran. Iran J. Basic Med. Sci. 2013, 16, 229–234. [Google Scholar]
- Lowis, G. Epidemiologic Features of HTLV-II Serologic and Molecular Evidence. Ann. Epidemiol. 2002, 12, 46–66. [Google Scholar] [CrossRef]
- Husseini, A.A.; Saeed, K.M.I.; Yurdcu, E.; Sertoz, R.; Bozdayi, A.M. Epidemiology of blood-borne viral infections in Afghanistan. Arch. Virol. 2019, 164, 2083–2090. [Google Scholar] [CrossRef]
- Mousavi, S.H.; Khairkhah, N.; Bahri, T.D.; Anvar, A.; Saraji, A.A.; Behnava, B.; Alavian, S.M.; Namvar, A. First Report of Prevalence of Blood-Borne Viruses (HBV, HCV, HIV, HTLV-1 and Parvovirus B19) Among Hemophilia Patients in Afghanistan. Sci. Rep. 2019, 9, 7259. [Google Scholar] [CrossRef]
- Zaki, S.M.; Darwish, M.M.; Mahmoud, M.H. Sporadic carriers of human T-cell lymphotropic virus type 1 among blood donors in Egypt. Egypt. J. Med. Lab. Sci. 2007, 16, 77–87. [Google Scholar]
- Ibrahim, A.I.; Al-Musawi, Y.A.; Abdullah, A.I. Seroprevalence of HTLV-type-1 and type-2 among Blood Donors in Some Iraqi Provinces. Indian J. Forensic Med. Toxicol. 2020, 14, 2179–2184. [Google Scholar] [CrossRef]
- Souan, L.; Tout, F.; Siag, M.; Sughayer, M.A. Seroprevalence rates of transfusion-transmitted infections among blood donors in Jordan. J. Infect. Dev. Ctries. 2016, 10, 377–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ameen, R.; Sanad, N.; Al-Shemmari, S.; Siddique, I.; Chowdhury, R.I.; Al-Hamdan, S.; Al-Bashir, A. Prevalence of viral markers among first-time Arab blood donors in Kuwait. Transfusion 2005, 45, 1973–1980. [Google Scholar] [CrossRef] [PubMed]
- Ramia, S.; Klayme, S.; Naman, R. Infection with hepatitis B and C viruses and human retroviruses (HTLV-I and HIV) among high-risk Lebanese patients. Ann. Trop. Med. Parasitol. 2003, 97, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Tamim, H.; Musharrafieh, U.; Ramia, S.; Almawi, W.Y.; Al-Jisr, T.; Ayoub, T.; Nabulsi-Majzoub, M.; Kazma, H.; Baz, E.K. Is seroprevalence of HTLV-I/II among blood donors in Lebanon relevant? Am. J. Infect. Control 2004, 32, 220–223. [Google Scholar] [CrossRef] [PubMed]
- Fawzi, Z.O.; Al Malki, A.; Al Mutawa, H. Prevalence of Human T-Lymphotropic Virus (HTLV) Antibodies Among the Donor Population in the State of Qatar. Qatar Med. J. 2006, 2006, 9. [Google Scholar] [CrossRef]
- Aabdien, M.; Selim, N.; Himatt, S.; Hmissi, S.; Merenkov, Z.; AlKubaisi, N.; Abdel-Rahman, M.; Abdelmola, A.; Khelfa, S.; Farag, E.; et al. Prevalence and trends of transfusion transmissible infections among blood donors in the State of Qatar, 2013–2017. BMC Infect. Dis. 2020, 20, 617. [Google Scholar] [CrossRef]
- Niazi, S.K.; Bhatti, F.A.; Salamat, N. Seroprevalence of Human T-Cell Lymphotropic Virus-1/2 in Blood Donors in Northern Pakistan: Implications for Blood Donor Screening. J. Coll. Physicians Surg. Pak. JCPSP 2015, 25, 874–877. [Google Scholar]
- Taha, M.A.; Bashawri, L.A.; Ahmed, M.S.; Ahmed, M.A. Prevalence of antibodies to human T-lymphotropic viruses types I and II among healthy blood donors. Saudi Med. J. 2003, 24, 637–640. [Google Scholar]
- Fawaz, N.; Tamim, H.; Almawi, W. Low prevalence of antibodies to human T-lymphotropic virus-I/II among blood donors in Eastern Saudi Arabia. Am. J. Infect. Control 2005, 33, 189–191. [Google Scholar] [CrossRef]
- Balkhy, H.H.; Memish, Z.A.; Abed, E.; Qasem, L.; Bin Amer, A.; Masoud, S.; Hajeer, A.H. Saudi national guard donor screening for human T cell lymphotropic virus I/II: Time to use molecular biology techniques. Mil. Med. 2004, 169, 251–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Hazmi, M. Prevalence of HBV, HCV, HIV-1, 2 and HTLV-I/II infections among blood donors in a teaching hospital in the Central region of Saudi Arabia. Saudi Med. J. 2004, 25, 26–33. [Google Scholar] [PubMed]
- Ul-Hassan, Z.; Al-Bahrani, A.T.; Panhotra, B.R. Prevalence of human T-lymphotropic virus type I and type II antibody among blood donors in Eastern Saudi Arabia. Saudi Med. J. 2004, 25, 1419–1422. [Google Scholar] [PubMed]
- Kawashti, M.I.; Hindawi, S.I.; Damanhouri, G.A.; Rowehy, N.G.; Bawazeer, M.M.; Alshawa, M. Serologial screening of human T cell lymphotropic virus I and II (HTLV I/II) in blood banks by immunoblotting and enzyme-immuno assays: To demand or to defeat? Egypt. J. Immunol. 2005, 12, 137–142. [Google Scholar]
- Hindawi, S.; Badawi, M.; Fouda, F.; Mallah, B.; Rajab, H.; Madani, T.A. Testing for HTLV 1 and HTLV 2 among blood donors in Western Saudi Arabia: Prevalence and cost considerations. Transfus. Med. 2018, 28, 60–64. [Google Scholar] [CrossRef]
- Almutairi, H.H.; AlAhmari, M.M.; Al-Zahran, B.H.; Abbas, I.S.; Al Ghamdi, J.S.; Raja’a, Y.A.; Sallam, T.A. Prevalence of serological markers and nucleic acid for blood-borne viral infections in blood donors in Al-Baha, Saudi Arabia. J. Infect. Dev. Ctries. 2016, 10, 619–625. [Google Scholar] [CrossRef] [Green Version]
- AlShehri, A. Human T Lymphotropic Virus-I (HTLV-I), the Causative Agent of Acute T-Cell Leukaemia/Lymphoma, Is Absent among Blood Donors in Aseer Region, Saudi Arabia. J. King Abdulaziz Univ. Sci. 2014, 26, 35–52. [Google Scholar] [CrossRef]
- Kilany, M.; Bin Dajem, S.M.; Ibrahim, Y.M.; Alshehri, A.; Aljeamelani, A.A.; Ibrahim, E.H. Seroprevalence of Anti-Treponemapallidum Antibodies (Syphilis) In Blood Donors in the Southern Area of Saudi Arabia. Res. J. Pharm. Biol. Chem. Sci. 2015, 6, 549–556. [Google Scholar]
- Almaiman, A.A.; Almaiman, S.H. Evaluation of Blood Donors and Transfusion Transmitted Infections and their Association with ABO and Rh Blood Groups in Unaizah, Saudi Arabia: A Retrospective Study. Int. J. Med. Res. Health Sci. 2018, 7, 143–150. [Google Scholar]
- Sarah, Y.A.E.G.A.; Sabry, A.E.G.A.E.H.E.S.; Maryam, A.A.-S. Seropositivity of TTIs among blood donors in Hail, Saudi Arabia, from 2014 to 2015. Asian Pac. J. Trop. Dis. 2016, 6, 141–146. [Google Scholar] [CrossRef]
- Alaidarous, M.; Choudhary, R.K.; Waly, M.I.; Mir, S.; Bin Dukhyil, A.; Banawas, S.S.; Alshehri, B.M. The prevalence of transfusion-transmitted infections and nucleic acid testing among blood donors in Majmaah, Saudi Arabia. J. Infect. Public Health 2018, 11, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Alabdulmonem, W.; Shariq, A.; Alqossayir, F.; AbaAlkhail, F.M.; Al-Musallam, A.Y.; Alzaaqi, F.O.; Aloqla, A.A.; Alodhaylah, S.A.; Alsugayyir, A.H.; Aldoubiab, R.K.; et al. Sero-prevalence ABO and Rh blood groups and their associated Transfusion-Transmissible Infections among Blood Donors in the Central Region of Saudi Arabia. J. Infect. Public Health 2020, 13, 299–305. [Google Scholar] [CrossRef]
- Alshehri, O.M.; Nahari, M.H.; Hassan, E.E.; Alqahtani, M.F.; Awaji, T.H. Prevalence of ABO, Rh and KELL Blood Group Types and Transfusion- Transmissible Infections (TTI) among Blood Donors in Najran City, Saudi Arabia. Biomed. Pharmacol. J. 2021, 14, 1065–1076. [Google Scholar] [CrossRef]
- Bitar, N.; El Hajj, H.; Houmani, Z.; Sabbah, A.; Otrock, Z.K.; Mahfouz, R.; Zaatari, G.; Bazarbachi, A. Adult T-cell leukemia/lymphoma in the Middle East: First report of two cases from Lebanon. Transfusion 2009, 49, 1859–1864. [Google Scholar] [CrossRef] [PubMed]
- Cassar, O.; Desrames, A.; Marçais, A.; Gout, O.; Taylor, G.P.; Hermine, O.; Soriano, V.; De Mendoza, C.; Dehan, O.; Le Mener, M.; et al. Multiple recombinant events in human T-cell Leukemia virus Type 1: Complete sequences of recombinant African strains. Emerg. Microbes Infect. 2020, 9, 913–923. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Population | Province (City, Direction in Country) | Study Year | Sample Size | Participants’ Age; Ranges (Mean ± SD) | Male to Female Ratio | Lab Techniques | Total Prevalence (%) | Prevalence by Sex (%) | Ref. | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Males | Females | p-Value | |||||||||
| General population | Golestan (North) | 2007 | 2034 | (38.7 ± 16.50) | 0.72 | ELISA, WB | 0.29 | 0.35 | 0.25 | 0.49 | [20] |
| Razavi Khorasan (Mashhad, Northeast) | ? | 9274 | ? | 0.67 | ELISA, PCR | 3.01 | 2.34 | 3.46 | 0.002 | [30] | |
| 2009 | 1654 | 1–90 | 0.83 | ELISA, WB, PCR | 2.12 | 1.46 | 2.66 | 0.093 | [21] | ||
| Razavi Khorasan (Neyshabour, Northeast) | 2002 | 1003 | 10–80 (32 ± ?) | 0.68 | ELISA, WB | 3.39 | 2.96 | 3.68 | 0.539 | [24] | |
| Razavi Khorasan (Sabzevar, Northeast) | 2008 | 1445 | 5–88 (36.6 ± 15.6) | 0.46 | ELISA, PCR | 1.66 | 2.42 | 1.31 | 0.128 | [19] | |
| Razavi Khorasan (Torbat-e-Heydarieh, Northeast) | 2011 | 400 | 14–89 (45.0 ± 16.8) | 1.05 | ELISA, PCR | 1.25 | 1.46 | 1.03 | 0.09 | [22] | |
| South Khorasan (East) | 2013–2014 | 3441 | 14–70 (38.7 ± 14.50) | 0.88 | ELISA | 0.35 | 0.25 | 0.44 | 0.34 | [23] | |
| Blood donors | Seven provinces | 2009–2013 | 1,864,489 | 18–65 (34.8 ± 10.4) | 10.32 | ELISA, WB | 0.10 | 0.09 | 0.18 | <0.001 | [31] |
| Razavi Khorasan (Northeast) | 628,667 | ? | ? | ELISA, WB | 0.21 | ? | ? | ? | |||
| West Azerbaijan (Northwest) | 307,422 | ? | ? | ELISA, WB | 0.07 | ? | ? | ? | |||
| North Khorasan (Northeast) | 79,035 | ? | ? | ELISA, WB | 0.06 | ? | ? | ? | |||
| Alborz (Center) | 264,340 | ? | ? | ELISA, WB | 0.06 | ? | ? | ? | |||
| South Khorasan (East) | 72,185 | ? | ? | ELISA, WB | 0.03 | ? | ? | ? | |||
| Gilan (North) | 373,227 | ? | ? | ELISA, WB | 0.02 | ? | ? | ? | |||
| Ardabil (Northwest) | 139,613 | ? | ? | ELISA, WB | 0.01 | ? | ? | ? | |||
| Seven provinces (East, North, Northeast, Northwest, Center)1 | 2010–2018 | 3,622,860 | 18–65 | 18.48 | ELISA, WB | 0.07 | 0.06 | 0.23 | <0.001 | [32] | |
| Bushehr (Southwest) | 2002–2003 | 22,740 | ? | 3.79 | ELISA, WB | 0.01 | 0.02 | 0 | - | [33] | |
| Charmahal and Bakhtiari (Southwest) | 2005–2006 | 800 | ? | ? | ELISA, WB | 0.50 | ? | ? | ? | [34] | |
| Fars (Shiraz) | ? | 500 | ? | 15.97 | ELISA | 0.20 | ? | ? | ? | [35] | |
| Golestan (North) | 2017 | 4226 | males: (37.6 ± 7.9), females: (38.3 ± 8.9) | ELISA, WB, PCR | 0.09 | ? | ? | ? | [36] | ||
| Hormozgan (South) | 2007–2008 | 1100 | ? | ? | ELISA, WB, PCR | 0.18 | ? | ? | ? | [37] | |
| Kermanshah (West) | 2015 | 470 | 10–59 | 9.0 | ELISA, WB | 0 | 0 | 0 | - | [38] | |
| 2011 | 1000 | (43.1 ± 19.8) | 0.71 | ELISA, WB | 0.50 | 0 | 0.86 | 0.079 | [39] | ||
| Mazandaran (Babol, North) | 2015–2016 | 503 | 19–61, males: (40.8 ± 9.8), females: (41.2 ± 11.4) | 24.15 | ELISA, PCR | 0.20 | 0.21 | 0 | - | [40] | |
| Razavi Khorasan (Mashhad, Northeast) | 2001–2002 | 60,892 | ? | ? | ELISA, WB | 0.66 | ? | ? | ? | [12] | |
| 2004–2006 | 232,648 | 18–65 (30 ± ?) | 9.88 | ELISA, WB | 0.45 | 0.42 | 0.76 | <0.001 | [41] | ||
| 2006–2008 | 250,582 | 17–63 (38.3 ± 10.8) | 11.74 | ELISA, WB | 0.40 | 0.36 | 0.88 | <0.001 | [42] | ||
| 2008–2009 | 79,687 | 17–65 | ? | ELISA, WB | 0.38 | ? | ? | ? | [43] | ||
| 2009–2010 | 165,860 | 17–59 (39.9 ± 10.5) | 13.71 | ELISA, WB | 0.26 | 0.23 | 0.70 | <0.001 | [44] | ||
| 2002–2013 | 983,000 | (35 ± 10 to 41 ± 11) | 14.63 | ELISA, WB | 0.30 | 0.28 | 0.48 | <0.001 | [45] | ||
| 2011–2013 | 174,662 | ? | 12.90 | ELISA, WB | 0.19 | 0.16 | 0.56 | <0.001 | [46] | ||
| Razavi Khorasan (Sabzevar, Northeast) | 2009–2012 | 35,067 | 17–59 (38.1 ± 11.8) | 9.06 | ELISA, WB | 0.14 | 0.13 | 0.26 | 0.095 | [47] | |
| South Khorasan (East) | 2005–2015 | 165,267 | males: (29.5 ± ?), females: (32.8 ± ?) | 11.55 | ELISA, WB | 0.03 | 0.03 | 0.02 | 0.038 | [48] | |
| Tehran (North) | ? | 2000 | ? | ? | ELISA, PCR | 0.05 | ? | ? | ? | [49] | |
| West Azerbaijan (Northwest) | 2005 | 2046 | (31.9 ± 10.2) | 14.04 | ELISA, WB | 0.34 | 0.26 | 1.47 | 0.074 | [50] | |
| 2009–2019 | 682,171 | 18–65 | 30.13 | ELISA, WB | 0.05 | 0.05 | 0.14 | <0.001 | [51] | ||
| Corneal donors | Nationwide | 2005–2007 | 5533 | 2–84 | 4.19 | ELISA, WB | 0.67 | 0.58 | 1.03 | 0.105 | [52] |
| Tissue donors | Nationwide | 2002–2007 | 1548 | 0–66 (29.1 ± 11.6) | 3.11 | ELISA | 1.61 | 1.45 | 2.12 | 0.369 | [53] |
| Pregnant women | Razavi Khorasan (Mashhad, Northeast) | 2010–2011 | 407 | (26 ± ?) | ? | ELISA, PCR | 1.47 | ? | ? | ? | [54] |
| People who referred to a medical lab | Razavi Khorasan (Neyshabour, Northeast) | 2009 | 483 | 5–84 (37.4 ± 15.4) | 0.26 | ELISA, WB | 7.25 | 10.31 | 6.49 | 0.196 | [27] |
| 2010–2014 | 8054 | males: (46 ± 3), females: (51 ± 3) | 0.24 | ELISA | 6.56 | 8.31 | 6.13 | 0.002 | [55] | ||
| 2013–2014 | 1169 2 | 2–35, (26.3 ± 5.4) | 0.14 | ELISA | 3.34 | 6.38 | 2.92 | 0.058 | [56] | ||
| 2011–2015 | 5724 3 | 15–40 (28.2 ± 6.0) | ? | ELISA | 2.04 | - | 2.04 | - | [57] | ||
| People who admitted to a referral hospital | Mazandaran (Sari, North) | 2009–2010 | 1200 | 1–76 | 0.55 | ELISA, WB | 0.08 | 0.24 | 0 | - | [58] |
| Razavi Khorasan (Northeast) | 2016–2017 | 758 4 | 0–14 (6.4 ± 1.8) | 1.14 | ELISA, PCR | 1.45 | ? | ? | ? | [59] | |
| Tehran (North) | 2009–2011 | 219 | 13–84 (39.9 ± 16.5) | 0.72 | ELISA | 1.83 | 1.09 | 2.36 | 0.641 | [60] | |
| Population | Province (City, Direction in Country) | Study Year | Sample Size | Participants’ Age; Ranges (Mean ± SD) | Male to Female Ratio | Lab Techniques | Prevalence (%) | Ref. |
|---|---|---|---|---|---|---|---|---|
| Hemodialysis patients | Busher (Southwest) | 2003 | 101 | ? | ? | ELISA, WB | 0 | [76] |
| Charmahal and Bakhtiari (Southwest) | 2005 | 107 | 18–90, (65 ± ?) | ? | ELISA, WB | 6.54 | [69] | |
| Hormozgan (South) | 2007–2008 | 40 | ? | ? | ELISA, WB | 0 | [37] | |
| Kurdistan (Sanandaj, West) | 2010 | 65 | (45.1 ± ?) | ? | ELISA, WB | 0 | [77] | |
| Mazandaran (Sari and Ghaemshahr, North) | 2011 | 160 | (59.1 ± 14.7) | 1.0 | ELISA, WB | 0.63 | [78] | |
| Razavi Khorasan (Mashhad, Northeast) | 2009–2010 | 135 | males: (43.5 ± 12.5), females: (50.5 ± 13.2) | 0.99 | ELISA, PCR | 5.93 | [67] | |
| Razavi Khorasan (Neyshabour, Northeast) | 2012 | 138 | 12–84, (53.3 ± 17.9) | 1.23 | ELISA, WB | 14.49 | [68] | |
| South Khorasan (Birjand, East) | 2010 | 41 | (54.9 ± 16.5) | 2.15 | ELISA, WB | 2.44 | [79] | |
| Tehran (North) | ? | 150 | 24–88, (63.6 ± 13.4) | 1.34 | ELISA, WB | 0.67 | [80] | |
| 2016–2017 | 174 | 17–86, (56 ± ?) | 1.32 | ELISA, PCR | 1.15 | [81] | ||
| West Azerbaijan (Urmia, Northwest) | 2006 | 95 | (31.9 ± 10.2) | ? | ELISA, WB | 1.05 | [50] | |
| Thalassemia patients | Busher (Southwest) | 2003 | 455 | ? | ? | ELISA, WB | 3.08 | [76] |
| Charmahal and Bakhtiari (Southwest) | 2005 | 250 | 1–45, (25 ± ?) | ? | ELISA, WB | 6.80 | [69] | |
| Fars (Shiraz, South) | ? | 200 | ? | ? | ELISA | 3.00 | [35] | |
| Golestan (Gorgan, North) | 2004–2005 | 181 | 1–25, (14.1 ± 6.5) | 1.06 | ELISA, WB | 4.42 | [82] | |
| Hormozgan (South) | 2007–2008 | 163 | ? | ? | ELISA, WB, PCR | 3.07 | [37] | |
| Isfahan (Center) | 2007 | 150 | 1–49, (17.7 ± ?) | 1.42 | ELISA, WB | 3.33 | [83] | |
| 2012 | 67 | ? | ? | ELISA, PCR | 1.49 | [84] | ||
| Kermanshah (West) | 2011 | 116 | (16.8 ± 6.6) | 1.23 | ELISA, WB | 3.45 | [39] | |
| Kurdistan (Sanandaj, West) | 2010 | 46 | (13.3 ± ?) | ? | ELISA, WB | 2.17 | [77] | |
| Mazandaran (North) | 2009 | 288 | (21.5 ± 6.6) | 0.91 | ELISA, PCR | 1.39 | [85] | |
| Mazandaran (Tonekabon, North) | 2015 | 80 | ? | ? | ELISA, PCR | 2.50 | [86] | |
| Razavi Khorasan (Mashhad, Northeast) | 2007 | 360 | 1–52, (11.6 ± 0.5) | 1.38 | ELISA | 6.11 | [87] | |
| 2006–2013 | 100 | 5–46, (22.7 ± ?) | 1.38 | ELISA, PCR | 4.00 | [88] | ||
| Tehran (North) | 2003 | 175 | (18.1 ± 1.0) | 1.36 | ELISA, WB | 6.29 | [70] | |
| 2008–2010 | 257 | ? | 0.89 | ELISA, WB | 11.28 | [71] | ||
| ? | 100 | ? | ? | ELISA, PCR | 8.00 | [49] | ||
| Hemophilia patients | Busher (Southwest) | 2003 | 86 | ? | ? | ELISA, WB | 0 | [76] |
| South Khorasan (East) | ? | 80 | (21.3 ± 12.1) | 25.67 | ELISA, WB | 1.25 | [89] | |
| 2010–2012 | 108 | 14–85, (27.7 ± 16.4) | 14.43 | ELISA | 2.78 | [90] | ||
| West Azerbaijan (Northwest) | ? | 50 | (10.3 ± ?) | 6.14 | ELISA, WB | 0 | [91] | |
| Patients with combined factor 5 and 8 deficiency | Razavi Khorasan (Mashhad, Northeast) | 2007 | 24 | 6–61, (26.9 ± 15.1) | 2.0 | ELISA, WB | 0 | [92] |
| HIV-positive patients | Isfahan (Center) | 2010–2011 | 56 | (37.0 ± 8.7) | 5.22 | ELISA | 1.79 | [93] |
| Khuzestan (Ahwaz, Southwest) | 2001–2003 | 104 1 | ? | * | ELISA, WB | 16.35 | [73] | |
| Kurdistan (Sanandaj, West) | 2010 | 130 1 | (27.2 ± ?) | 239.0 | ELISA, WB | 0.77 | [77] | |
| Razavi Khorasan (Mashhad, Northeast) | ? | 20 | 22–50, (36.4 ± 8.6) | 4.0 | ELISA, WB | 15.0 | [72] | |
| Tehran (North) | ? | 100 | ? | ? | ELISA, PCR | 5.00 | [49] | |
| People who inject drugs | Isfahan (Center) | 2007–2008 | 150 2 | (30.7 ± 7.1) | 74.0 | ELISA | 2.67 | [94] |
| Khuzestan (Ahwaz, Southwest) | 2001–2003 | 104 1 | ? | * | ELISA, WB | 16.35 | [73] | |
| Kurdistan (Sanandaj, West) | 2010 | 130 1 | (27.2 ± ?) | 239.0 | ELISA, WB | 0.77 | [77] | |
| 2010 | 110 3 | ? | ? | ELISA, WB | 0.91 | [77] | ||
| Razavi Khorasan (Mashhad, Northeast) | 2001 | 101 4 | (32.8 ± 8.9) | ? | ELISA, WB | 51.49 | [12] | |
| 2007–2008 | 62 5 | (34.3 ± ?) | 30.0 | ELISA | 8.06 | [95] | ||
| Tehran (North) | ? | 180 | 9–67, (36.9 ± 9.2) | ? | ELISA, WB | 0 | [96] | |
| Prisoners | Razavi Khorasan (Northeast) | 2001 | 101 4 | (32.8 ± 8.9) | ? | ELISA, WB | 51.49 | [12] |
| 2008 | 1114 6 | males: (34.4 ± 10.9), females: (40.7 ± 14.2) | 8.13 | ELISA, PCR | 1.97 | [74] | ||
| South Khorasan (Birjand, East) | 2014–2015 | 300 7 | 20–78, (37.4 ± 9.4) | * | ELISA, WB | 0 | [97] |
| Population | Country (Province, City) | Study Year | Sample Size | Participants’ Age; Ranges (Mean ± SD) | Male to Female Ratio | Lab Techniques | Prevalence (%) | Ref. |
|---|---|---|---|---|---|---|---|---|
| General population | Afghanistan (5 provinces) 1 | 2015 | 466 | 25–70, (38.9 ± 12.0) | 0.98 | CMIA | 0.64 | [101] |
| Blood donors | Egypt (Cairo) | 2005–2006 | 90 | 18–47, (29.3 ± 6.5) | 6.50 | ELISA, PCR | 1.11 | [103] |
| Iraq (7 provinces) 2 | 2015 | 15,239 | 20–57, (36 ± ?) | ? | ELISA, CMIA | 0.26 | [104] | |
| Jordan (Amman) | 2009–2013 | 62,933 | 18–60 | ? | ELISA | 0 | [105] | |
| Kuwait (Nationwide) | 2002 | 12,798 | males: 20–56, (35 ± ?), females: 24–50, (30 ± ?) | ? | ELISA, CMIA | 0.01 | [106] | |
| Lebanon (Beirut) | 2000–2002 | 500 | (38.7 ± ?) | 3.17 | ELISA | 0 | [107] | |
| Lebanon (Nationwide) | 2001–2002 | 3529 | (30.0 ± 8.9) | 22.80 | ELISA, WB, PCR | 0.06 (WB), 0.03 (PCR) | [108] | |
| Qatar (Nationwide) | 1991–2003 | 124,266 | ? | ? | ELISA, WB | 0.0002 | [109] | |
| Qatar (Doha) | 2013–2017 | 190,509 | ? | 10.03 | CMIA, LIA | 0.18 | [110] | |
| Pakistan (Rawalpindi) | 2013 | 2100 | 18–60, (29.0 ± 9.3) | 62.64 | CMIA, LIA, PCR | 0.19 | [111] | |
| Saudi Arabia (Al-Khobar) | 1995–2001 | 23,493 | (33.8 ± ?) | ? | ELISA, WB | 0.05 | [112] | |
| Saudi Arabia (Dammam) | 1998–2001 | 13,443 | ? | ? | ELISA, WB | 0.06 | [113] | |
| Saudi Arabia (Riyadh) | 1999–2001 | 24,654 | ? | ? | ELISA, WB | 0.004 | [114] | |
| Saudi Arabia (Riyadh) | 2000–2002 | 24,173 | (33.8 ± ?) | 108.38 | ELISA, LIA | 0 | [115] | |
| Saudi Arabia (Al-Hasa) | 1997–2003 | 47,426 | 18–55 | ? | ELISA, WB | 0.01 | [116] | |
| Saudi Arabia (Jeddah) | ? | 30,000 | ? | ? | ELISA, WB | 0 | [117] | |
| 2006–2015 | 107,419 | ? | ? | CMIA, WB | 0 | [118] | ||
| Saudi Arabia (Al-Baha) | 2009–2011 | 2807 | 16–66 | * | ELISA | 0.04 | [119] | |
| Saudi Arabia (Aseer) | 2012 | 4432 | 18–60, (30 ± ?) | * | ELISA | 0 | [120] | |
| Saudi Arabia (Aseer) | 2012–2013 | 7267 | 18–60 | 278.50 | ELISA | 0 | [121] | |
| Saudi Arabia (Qassim/Unaizah) | 2013–2016 | 9460 | 18–48, (31.4 ± 8.7) | 26.82 | ELISA, PCR | 0.10 | [122] | |
| Saudi Arabia (Hail) | 2016 | 361 | <20 to >50 | ? | ELISA | 2.22 | [123] | |
| Saudi Arabia (Majmaah) | 2015–2017 | 3028 | 18–61 | 44.6 | ELISA | 0.20 | [124] | |
| Saudi Arabia (Buraidah) | 2017–2018 | 4590 | 16–65 | 4.88 | ELISA | 0 | [125] | |
| Saudi Arabia (Najran) | ? | 953 | ? | 237.25 | ELISA | 0 | [126] | |
| Hemophilia patients | Afghanistan (four cities) 3 | 2017 | 80 | 2–38, (13.7 ± 9.8) | ? | ELISA | 0 | [102] |
| Lebanon (Beirut) | 2000–2002 | 30 | (37.4 ± ?) | * | ELISA | 0 | [107] | |
| Malignancy patients with multiply transfusions | Lebanon (Beirut) | 2000–2002 | 65 | (30.5 ± ?) | 1.32 | ELISA | 0 | [107] |
| People who inject drugs | Lebanon (Beirut) | 2000–2002 | 40 | (50.3 ± ?) | 3.0 | ELISA | 0 | [107] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hedayati-Moghaddam, M.R.; Jafarzadeh Esfehani, R.; El Hajj, H.; Bazarbachi, A. Updates on the Epidemiology of the Human T-Cell Leukemia Virus Type 1 Infection in the Countries of the Eastern Mediterranean Regional Office of the World Health Organization with Special Emphasis on the Situation in Iran. Viruses 2022, 14, 664. https://doi.org/10.3390/v14040664
Hedayati-Moghaddam MR, Jafarzadeh Esfehani R, El Hajj H, Bazarbachi A. Updates on the Epidemiology of the Human T-Cell Leukemia Virus Type 1 Infection in the Countries of the Eastern Mediterranean Regional Office of the World Health Organization with Special Emphasis on the Situation in Iran. Viruses. 2022; 14(4):664. https://doi.org/10.3390/v14040664
Chicago/Turabian StyleHedayati-Moghaddam, Mohammad Reza, Reza Jafarzadeh Esfehani, Hiba El Hajj, and Ali Bazarbachi. 2022. "Updates on the Epidemiology of the Human T-Cell Leukemia Virus Type 1 Infection in the Countries of the Eastern Mediterranean Regional Office of the World Health Organization with Special Emphasis on the Situation in Iran" Viruses 14, no. 4: 664. https://doi.org/10.3390/v14040664