
Human T-Cell Leukemia Virus Type 1-Related Diseases May Constitute a Threat to the Elimination of Human Immunodeficiency Virus, by 2030, in Gabon, Central Africa

 ,
, 
Abstract
:1. Introduction
2. Epidemiological Situation of the HIV-1 Infection in Gabon
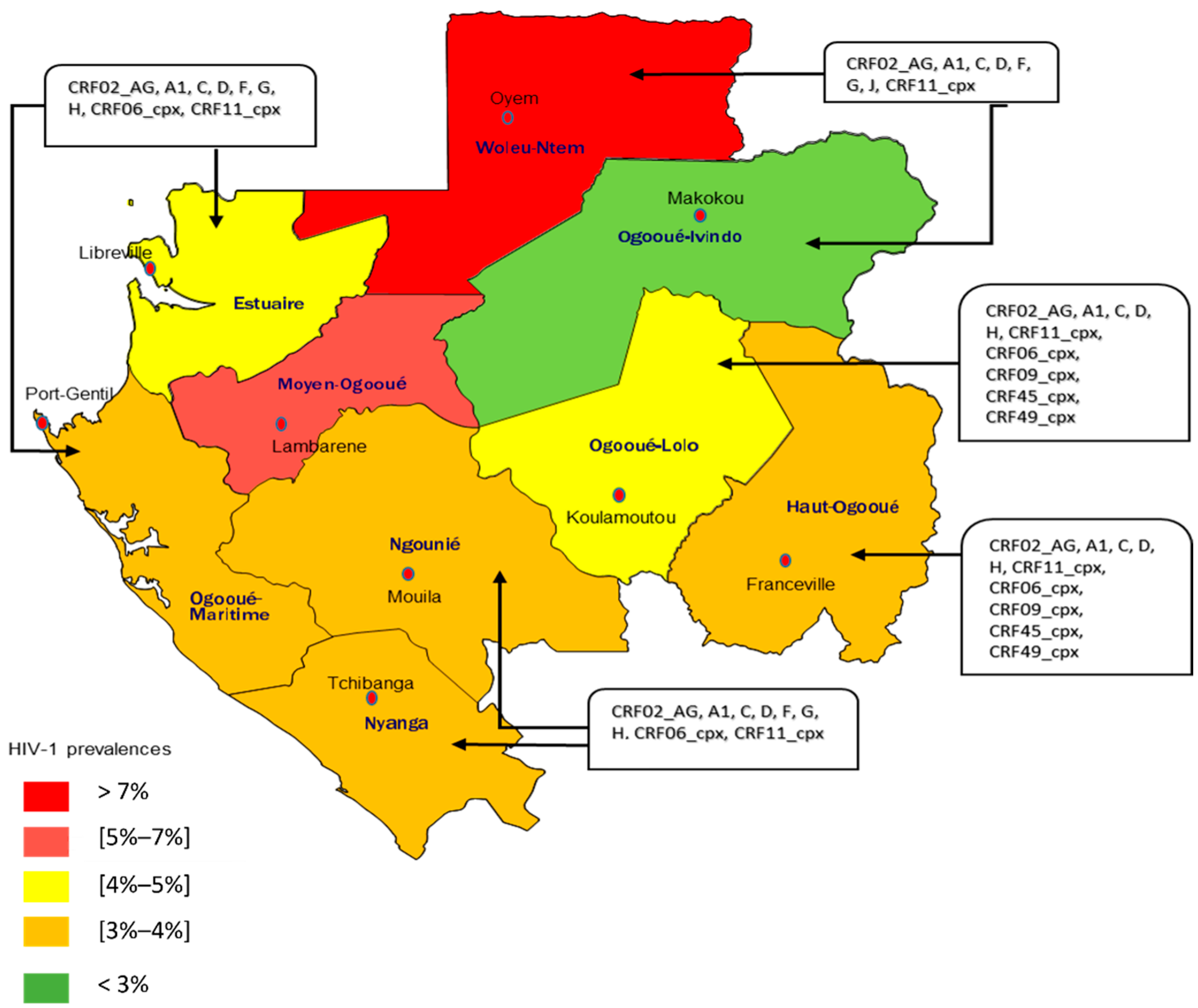
2.1. HIV-1 Prevalence
2.2. Genetic Diversity of HIV-1
2.3. Diagnosis of HIV-1 in Gabon and the Therapeutic Management
2.4. Treatment-Related Challenges and Complications Associated with HIV-1 in Gabon
3. Human T-Cell Leukemia Virus Type 1 (HTLV-1) in Gabon
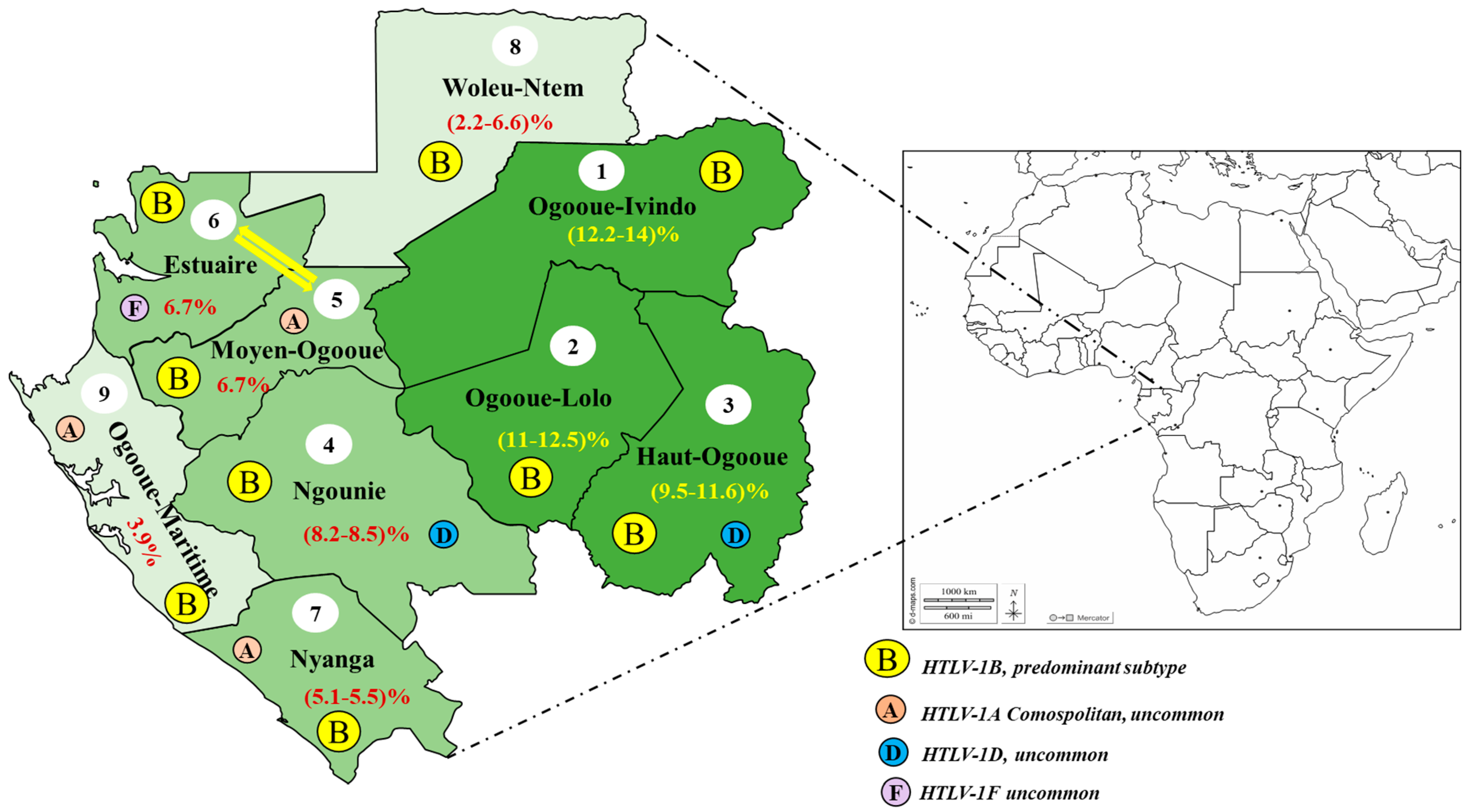
3.1. General Epidemiological Data
3.2. Modes of the HTLV-1 Transmission in Gabon
3.3. Cases of the Associated Disease with the HTLV-1 Infection Described in Gabon
3.4. Molecular Epidemiology of HTLV-1 in Gabon
4. HIV-1 and HTLV-1 Co-Infections in Gabon
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fiche d’information 2022-Statistiques Mondiales sur le VIH. Available online: https://www.unaids.org/fr/resources/fact-sheet (accessed on 29 July 2022).
- Ministère de la Santé. EDSG-2: Enquête Démographique et de Santé 2012/Rapport de Synthèse; Ministère de la Santé: Paris, France, 2012.
- ONUSIDA. Rapports D’avancement Nationaux-Gabon/Rapport Mondial D’avancement sur la Lutte Contre le Sida 2020; ONUSIDA: Geneva, Switzerland, 2020. [Google Scholar]
- Peeters, M.; Jung, M.; Ayouba, A. The origin and molecular epidemiology of HIV. Expert Rev. Anti-Infect. Ther. 2013, 11, 885–896. [Google Scholar] [CrossRef] [PubMed]
- Gordon, T.P.; Talbert, M.; Mugisha, M.K.; Herbert, A.E. Factors associated with HIV viral suppression among adolescents in Kabale district, South Western Uganda. PLoS ONE 2022, 17, e0270855. [Google Scholar] [CrossRef] [PubMed]
- Montaño-Castellón, I.; Marconi, C.S.C.; Saffe, C.; Brites, C. Clinical and Laboratory Outcomes in HIV-1 and HTLV-1/2 Coinfection: A Systematic Review. Front. Public Health 2022, 10, 820727. [Google Scholar] [CrossRef] [PubMed]
- de Mendoza, C.; Caballero, E.; Aguilera, A.; Benito, R.; Maciá, D.; García-Costa, J.; Soriano, V. HIV co-infection in HTLV-1 carriers in Spain. Virus Res. 2019, 266, 48–51. [Google Scholar] [CrossRef]
- Poiesz, B.J.; Ruscetti, F.W.; Gazdar, A.F.; Bunn, P.A.; Minna, J.D.; Gallo, R.C. Detection and isolation of type C retrovirus particles from fresh and cultured lymphocytes of a patient with cutaneous T-cell lymphoma. Proc. Natl. Acad. Sci. USA 1980, 77, 7415–7419. [Google Scholar] [CrossRef] [Green Version]
- Gessain, A.; Barin, F.; Vernant, J.C.; Gout, O.; Maurs, L.; Calender, A.; de Thé, G. Antibodies to human T-lymphotropic virus type-I in patients with tropical spastic paraparesis. Lancet 1985, 2, 407–410. [Google Scholar] [CrossRef]
- Osame, M.; Usuku, K.; Izumo, S.; Ijichi, N.; Amitani, H.; Igata, A.; Matsumoto, M.; Tara, M. HTLV-I associated myelopathy, a new clinical entity. Lancet 1986, 1, 1031–1032. [Google Scholar] [CrossRef]
- Caron, M.; Besson, G.; Padilla, C.; Makuwa, M.; Nkoghe, D.; Leroy, E.; Kazanji, M. Revisiting human T-cell lymphotropic virus types 1 and 2 infections among rural population in Gabon, central Africa thirty years after the first analysis. PLoS Negl. Trop. Dis. 2018, 12, e0006833. [Google Scholar] [CrossRef] [Green Version]
- Djuicy, D.D.; Mouinga-Ondémé, A.; Cassar, O.; Ramassamy, J.L.; Idam Mamimandjiami, A.; Bikangui, R.; Fontanet, A.; Gessain, A. Risk factors for HTLV-1 infection in Central Africa: A rural population-based survey in Gabon. PLoS Negl. Trop. Dis. 2018, 12, e0006832. [Google Scholar] [CrossRef] [Green Version]
- Pilotti, E.; Bianchi, M.V.; De Maria, A.; Bozzano, F.; Romanelli, M.G.; Bertazzoni, U.; Casoli, C. HTLV-1/-2 and HIV-1 co-infections: Retroviral interference on host immune status. Front. Microbiol. 2013, 4, 372. [Google Scholar] [CrossRef]
- Casoli, C.; Vicenzi, E.; Cimarelli, A.; Magnani, G.; Ciancianaini, P.; Cattaneo, E.; Dall’Aglio, P.; Poli, G.; Bertazzoni, U. HTLV-II down-regulates HIV-1 replication in IL-2-stimulated primary PBMC of coinfected individuals through expression of MIP-1alpha. Blood 2000, 95, 2760–2769. [Google Scholar] [CrossRef] [PubMed]
- Makuwa, M.; Souquière, S.; Apetrei, C.; Tevi-Benissan, C.; Bedjabaga, I.; Simon, F. HIV prevalence and strain diversity in Gabon: The end of a paradox. AIDS 2000, 14, 1275–1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandrea, I.; Robertson, D.L.; Onanga, R.; Gao, F.; Makuwa, M.; Ngari, P.; Bedjabaga, I.; Roques, P.; Simon, F.; Apetrei, C. Analysis of partial pol and env sequences indicates a high prevalence of HIV type 1 recombinant strains circulating in Gabon. AIDS Res. Hum. Retrovir. 2002, 18, 1103–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caron, M.; Makuwa, M.; Souquière, S.; Descamps, D.; Brun-Vézinet, F.; Kazanji, M. Human immunodeficiency virus type 1 seroprevalence and antiretroviral drug resistance-associated mutations in miners in Gabon, central Africa. AIDS Res. Hum. Retrovir. 2008, 24, 1225–1228. [Google Scholar] [CrossRef] [PubMed]
- Mintsa-Ndong, A.; Caron, M.; Plantier, J.C.; Makuwa, M.; Le Hello, S.; Courgnaud, V.; Roques, P.; Kazanji, M. High HIV Type 1 prevalence and wide genetic diversity with dominance of recombinant strains but low level of antiretroviral drug-resistance mutations in untreated patients in northeast Gabon, Central Africa. AIDS Res. Hum. Retrovir. 2009, 25, 411–418. [Google Scholar] [CrossRef]
- Caron, M.; Lekana-Douki, S.E.; Makuwa, M.; Obiang-Ndong, G.P.; Biba, O.; Nkoghé, D.; Kazanji, M. Prevalence, genetic diversity and antiretroviral drugs resistance-associated mutations among untreated HIV-1-infected pregnant women in Gabon, central Africa. BMC Infect. Dis. 2012, 12, 64. [Google Scholar] [CrossRef] [Green Version]
- Liégeois, F.; Vella, C.; Eymard-Duvernay, S.; Sica, J.; Makosso, L.; Mouinga-Ondémé, A.; Mongo, A.D.; Boué, V.; Butel, C.; Peeters, M.; et al. Virological failure rates and HIV-1 drug resistance patterns in patients on first-line antiretroviral treatment in semirural and rural Gabon. J. Int. AIDS Soc. 2012, 15, 17985. [Google Scholar] [CrossRef] [PubMed]
- Engone-Ondo, J.D.; Mouinga-Ondémé, A.; Lékana-Douki, S.E.; Diané, A.; Mamimandjiami, A.I.; Banga, O.; Ndong-Atome, G.R.; Aghokeng, A.F. High rate of virological failure and HIV drug resistance in semi-rural Gabon and implications for dolutegravir-based regimen efficacy. J. Antimicrob. Chemother. 2021, 76, 1051–1056. [Google Scholar] [CrossRef] [PubMed]
- Engone-Ondo, J.D.; Bignoumba, M.; Boundzanga Moussavou, P.; Gafou, A.; Diane, A.; Yangawagou, L.M.; Kassa Kassa, R.F.; Onanga, R.; Mouinga-Ondémé, A.; Aghokeng, A.F. HIV-1 non-B resistance mutations and natural polymorphisms to integrase strand transfer inhibitors in recently diagnosed patients in Gabon, Central Africa. J. Antimicrob. Chemother. 2022, 77, 2035–2037. [Google Scholar] [CrossRef]
- Liégeois, F.; Boué, V.; Butel, C.; Mouinga-Ondémé, A.; Sica, J.; Zamba, C.; Peeters, M.; Delaporte, E.; Rouet, F. HIV type-1 group O infection in Gabon: Low prevalence rate but circulation of genetically diverse and drug-resistant HIV type-1 group O strains. AIDS Res. Hum. Retrovir. 2013, 29, 1085–1090. [Google Scholar] [CrossRef]
- Delaporte, E.; Janssens, W.; Peeters, M.; Buvé, A.; Dibanga, G.; Perret, J.L.; Ditsambou, V.; Mba, J.R.; Courbot, M.C.; Georges, A.; et al. Epidemiological and molecular characteristics of HIV infection in Gabon, 1986–1994. AIDS 1996, 10, 903–910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PNLS. Guide de Prise en Charge des Personnes Vivant avec le VIH et le SIDA au Gabon; Programme National de Lutte Contre les IST et le VIH/SIDA (PNLS): Abidjan, Côte d’Ivoire, 2019. [Google Scholar]
- Abongwa, L.E.; Nyamache, A.K.; Torimiro, J.N.; Okemo, P.; Charles, F. Human immunodeficiency virus type 1 ((HIV-1) subtypes in the northwest region, Cameroon. Virol. J. 2019, 16, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamaguchi, J.; Bodelle, P.; Vallari, A.S.; Coffey, R.; McArthur, C.P.; Schochetman, G.; Devare, S.G.; Brennan, C.A. HIV infections in northwestern Cameroon: Identification of HIV type 1 group O and dual HIV type 1 group M and group O infections. AIDS Res. Hum. Retrovir. 2004, 20, 944–957. [Google Scholar] [CrossRef] [PubMed]
- Vallari, A.; Bodelle, P.; Ngansop, C.; Makamche, F.; Ndembi, N.; Mbanya, D.; Kaptué, L.; Gürtler, L.G.; McArthur, C.P.; Devare, S.G.; et al. Four new HIV-1 group N isolates from Cameroon: Prevalence continues to be low. AIDS Res. Hum. Retrovir. 2010, 26, 109–115. [Google Scholar] [CrossRef]
- Vallari, A.; Holzmayer, V.; Harris, B.; Yamaguchi, J.; Ngansop, C.; Makamche, F.; Mbanya, D.; Kaptué, L.; Ndembi, N.; Gürtler, L.; et al. Confirmation of putative HIV-1 group P in Cameroon. J. Virol. 2011, 85, 1403–1407. [Google Scholar] [CrossRef] [Green Version]
- Yamaguchi, J.; Vallari, A.; Ndembi, N.; Coffey, R.; Ngansop, C.; Mbanya, D.; Kaptué, L.; Gürtler, L.G.; Devare, S.G.; Brennan, C.A. HIV type 2 intergroup recombinant identified in Cameroon. AIDS Res. Hum. Retrovir. 2008, 24, 86–91. [Google Scholar] [CrossRef]
- Yebra, G.; de Mulder, M.; Holguín, Á. Description of HIV-1 group M molecular epidemiology and drug resistance prevalence in Equatorial Guinea from migrants in Spain. PLoS ONE 2013, 8, e64293. [Google Scholar] [CrossRef] [Green Version]
- Kwon, E.H.; Musema, G.M.A.; Boelter, J.; Townsend, S.; Tshala-Katumbay, D.; Kayembe, P.K.; West, J.; Wood, C. HIV-1 subtypes and drug resistance mutations among female sex workers varied in different cities and regions of the Democratic Republic of Congo. PLoS ONE 2020, 15, e0228670. [Google Scholar] [CrossRef] [Green Version]
- ONUSIDA. Accélérer la Riposte Mettre fin à L’épidémie de Sida d’ici à 2030; ONUSIDA: Geneva, Switzerland, 2014. [Google Scholar]
- Castelan, A.; Nellen, J.F.; van der Valk, M.; Nieuwkerk, P.T. Intentional- but not Unintentional Medication Non-adherence was Related with Beliefs about Medicines among a Multi-Ethnic Sample of People with HIV. AIDS Behav. 2022, 1–10. [Google Scholar] [CrossRef]
- Mongo-Delis, A.; Mombo, L.E.; Mickala, P.; Bouassa, W.; Bouedy, W.S.; M’Batchi, B.; Bisseye, C. Factors associated with adherence to ARV treatment in people living with HIV/AIDS in a rural area (Koula-Moutou) in East Gabon. Afr. J. AIDS Res. 2019, 18, 51–57. [Google Scholar] [CrossRef]
- Luebbert, J.; Tweya, H.; Phiri, S.; Chaweza, T.; Mwafilaso, J.; Hosseinipour, M.C.; Ramroth, H.; Schnitzler, P.; Neuhann, F. Virological failure and drug resistance in patients on antiretroviral therapy after treatment interruption in Lilongwe, Malawi. Clin. Infect. Dis. 2012, 55, 441–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mouinga-Ondémé, A.; Boundenga, L.; Koumba Koumba, I.P.; Idam Mamimandjiami, A.; Diané, A.; Engone-Ondo, J.D.; Djuicy, D.D.; Sica, J.; Mombo, L.E.; Gessain, A.; et al. Human T-Lymphotropic virus type 1 and human immunodeficiency virus co-infection in rural Gabon. PLoS ONE 2022, 17, e0271320. [Google Scholar] [CrossRef] [PubMed]
- Delaporte, E.; Dupont, A.; Peeters, M.; Josse, R.; Merlin, M.; Schrijvers, D.; Hamono, B.; Bedjabaga, L.; Cheringou, H.; Boyer, F.; et al. Epidemiology of HTLV-I in Gabon (Western Equatorial Africa). Int. J. Cancer 1988, 42, 687–689. [Google Scholar] [CrossRef] [PubMed]
- Schrijvers, D.; Delaporte, E.; Peeters, M.; Dupont, A.; Meheus, A. Seroprevalence of retroviral infection in women with different fertility statuses in Gabon, western equatorial Africa. J. Acquir. Immune Defic. Syndr. 1991, 4, 468–470. [Google Scholar] [PubMed]
- Berteau, F.; Mention, J.; Tissedre, J.; Narraido, B.; Grall, C.; Glowaczover, E.; Kéita, A.D.; Laval, Y.; Bedjabaga, I.; Ossari, S. Evaluation of human immunodeficiency virus (HIV) and human T-cell lymphotropic virus (HTLV) seroprevalence in Haut Ogooué province Gabon in pregnant women and blood donor control groups. Bull. Soc. Pathol. Exot. 1993, 86, 12–15. [Google Scholar]
- Le Hesran, J.Y.; Delaporte, E.; Gaudebout, C.; Trebuck, A.; Schrijvers, D.; Josse, R.; Peeters, M.; Cheringou, H.; Dupont, A.; Larouze, B. Demographic factors associated with HTLV-1 infection in a Gabonese community. Int. J. Epidemiol. 1994, 23, 812–817. [Google Scholar] [CrossRef]
- Hlela, C.; Shepperd, S.; Khumalo, N.P.; Taylor, G.P. The prevalence of human T-cell lymphotropic virus type 1 in the general population is unknown. AIDS Rev. 2009, 11, 205–214. [Google Scholar]
- Bertherat, E.; Makuwa, M.; Renaut, A.; Nabias, R.; Georges-Courbot, M.C. HIV-1, HTLV-I, and HTLV-II in a semiurban population in East Gabon. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1998, 19, 430–432. [Google Scholar] [CrossRef]
- Delaporte, E.; Monplaisir, N.; Louwagie, J.; Peeters, M.; Martin-Prével, Y.; Louis, J.P.; Trebucq, A.; Bedjabaga, L.; Ossari, S.; Honoré, C.; et al. Prevalence of HTLV-I and HTLV-II infection in Gabon, Africa: Comparison of the serological and PCR results. Int. J. Cancer 1991, 49, 373–376. [Google Scholar] [CrossRef]
- Etenna, S.L.; Caron, M.; Besson, G.; Makuwa, M.; Gessain, A.; Mahé, A.; Kazanji, M. New insights into prevalence, genetic diversity, and proviral load of human T-cell leukemia virus types 1 and 2 in pregnant women in Gabon in equatorial central Africa. J. Clin. Microbiol. 2008, 46, 3607–3614. [Google Scholar] [CrossRef] [Green Version]
- Kazanji, M.; Mouinga-Ondémé, A.; Lekana-Douki-Etenna, S.; Caron, M.; Makuwa, M.; Mahieux, R.; Gessain, A. Origin of HTLV-1 in hunters of nonhuman primates in Central Africa. J. Infect. Dis. 2015, 211, 361–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capdepont, S.; Londos-Gagliardi, D.; Joubert, M.; Correze, P.; Lafon, M.-E.; Guillemain, B.; Fleury, H. New Insights in HTLV-I Phylogeny by Sequencing and Analyzing the Entire Envelope Gene. AIDS Res. Hum. Retrovir. 2005, 21, 28–42. [Google Scholar] [CrossRef] [PubMed]
- Mahieux, R.; Ibrahim, F.; Mauclere, P.; Herve, V.; Michel, P.; Tekaia, F.; Chappey, C.; Garin, B.; Van Der Ryst, E.; Guillemain, B.; et al. Molecular epidemiology of 58 new African human T-cell leukemia virus type 1 (HTLV-1) strains: Identification of a new and distinct HTLV-1 molecular subtype in Central Africa and in Pygmies. J. Virol. 1997, 71, 1317–1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.F.; Goubau, P.; Van Brussel, M.; Van Laethem, K.; Chen, Y.C.; Desmyter, J.; Vandamme, A.M. The three human T-lymphotropic virus type I subtypes arose from three geographically distinct simian reservoirs. J. Gen. Virol. 1996, 77, 359–368. [Google Scholar] [CrossRef]
- Proietti, F.A.; Carneiro-Proietti, A.B.; Catalan-Soares, B.C.; Murphy, E.L. Global epidemiology of HTLV-I infection and associated diseases. Oncogene 2005, 24, 6058–6068. [Google Scholar] [CrossRef] [Green Version]
- Delaporte, E.; Peeters, M.; Simoni, M.; Piot, P. HTLV-I infection in western equatorial Africa. Lancet 1989, 2, 1226. [Google Scholar] [CrossRef]
- Delaporte, E.; Klotz, F.; Peeters, M.; Martin-Prevel, Y.; Bedjabaga, L.; Larouzé, B.; Nguembi-Mbina, C.; Walter, P.; Piot, P. Non-Hodgkin lymphoma in Gabon and its relation to HTLV-I. Int. J. Cancer 1993, 53, 48–50. [Google Scholar] [CrossRef]
- Mahieux, R.; Chappey, C.; Georges-Courbot, M.C.; Dubreuil, G.; Mauclere, P.; Georges, A.; Gessain, A. Simian T-cell lymphotropic virus type 1 from Mandrillus sphinx as a simian counterpart of human T-cell lymphotropic virus type 1 subtype D. J. Virol. 1998, 72, 10316–10322. [Google Scholar] [CrossRef] [Green Version]
- Perret, J.L.; Moussavou-Kombila, J.B.; Delaporte, E.; Coniquet, S.; Nguemby-Mbina, C.; Normand, P. Mycosis fungoides in a Gabonese patient infected with HTLV-I. Med. Trop. (Mars) 1996, 56, 66–68. [Google Scholar]
- Koralnik, I.J.; Boeri, E.; Saxinger, W.C.; Monico, A.L.; Fullen, J.; Gessain, A.; Guo, H.G.; Gallo, R.C.; Markham, P.; Kalyanaraman, V.; et al. Phylogenetic associations of human and simian T-cell leukemia/lymphotropic virus type I strains: Evidence for interspecies transmission. J. Virol. 1994, 68, 2693–2707. [Google Scholar] [CrossRef] [Green Version]
- Ramassamy, J.L.; Cassar, O.; Toumbiri, M.; Diané, A.; Idam Mamimandjiami, A.; Bengone, C.; Ntsame-Ndong, J.M.; Mouinga-Ondémé, A.; Gessain, A. High prevalence of human T-cell leukemia virus type-1b genotype among blood donors in Gabon, Central Africa. Transfusion 2020, 60, 1483–1491. [Google Scholar] [CrossRef] [PubMed]
- Richard, L.; Mouinga-Ondémé, A.; Betsem, E.; Filippone, C.; Nerrienet, E.; Kazanji, M.; Gessain, A. Zoonotic Transmission of Two New Strains of Human T-lymphotropic Virus Type 4 in Hunters Bitten by a Gorilla in Central Africa. Clin. Infect. Dis. 2016, 63, 800–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippone, C.; Betsem, E.; Tortevoye, P.; Cassar, O.; Bassot, S.; Froment, A.; Fontanet, A.; Gessain, A. A Severe Bite from a Nonhuman Primate Is a Major Risk Factor for HTLV-1 Infection in Hunters from Central Africa. Clin. Infect. Dis. 2015, 60, 1667–1676. [Google Scholar] [CrossRef] [PubMed]
- Mossoun, A.; Calvignac-Spencer, S.; Anoh, A.E.; Pauly, M.S.; Driscoll, D.A.; Michel, A.O.; Nazaire, L.G.; Pfister, S.; Sabwe, P.; Thiesen, U.; et al. Bushmeat Hunting and Zoonotic Transmission of Simian T-Lymphotropic Virus 1 in Tropical West and Central Africa. J. Virol. 2017, 91, e02479-16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gessain, A.; Cassar, O. Epidemiological Aspects and World Distribution of HTLV-1 Infection. Front. Microbiol. 2012, 3, 388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gessain, A. Le rétrovirus humain oncogène HTLV-1: Épidémiologie descriptive et moléculaire, origine, évolution et aspects diagnostiques et maladies associées. Bull. Société Pathol. Exot. 2011, 104, 167. [Google Scholar] [CrossRef] [PubMed]
- Iwanaga, M. Epidemiology of HTLV-1 Infection and ATL in Japan: An Update. Front. Microbiol. 2020, 11, 1124. [Google Scholar] [CrossRef]
- Igala, M.; Ledaga, L.; Rérambhia, L.K.; Ngoua, S.N.; Sima, F.N.; Cheme, S.B.; Lamine, S.D.L.; Iba-Ba, J.; Boguikoumba, J. Leucémie/Lymphome T de l’adulte HTLV 1+, une réalité au Gabon. Bull. Médical D’owendo 2019, 17, 56–60. [Google Scholar]
- Umekita, K.; Okayama, A. HTLV-1 Infection and Rheumatic Diseases. Front. Microbiol. 2020, 11, 152. [Google Scholar] [CrossRef]
- Morgan, O.S.; Rodgers-Johnson, P.; Mora, C.; Char, G. HTLV-1 and polymyositis in Jamaica. Lancet 1989, 2, 1184–1187. [Google Scholar] [CrossRef]
- Eguchi, K.; Matsuoka, N.; Ida, H.; Nakashima, M.; Sakai, M.; Sakito, S.; Kawakami, A.; Terada, K.; Shimada, H.; Kawabe, Y.; et al. Primary Sjögren’s syndrome with antibodies to HTLV-I: Clinical and laboratory features. Ann. Rheum. Dis. 1992, 51, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Fukasawa, M.; Tsujimoto, H.; Ishikawa, K.; Miura, T.; Ivanoff, B.; Cooper, R.W.; Frost, E.; Delaporte, E.; Mingle, J.A.; Grant, F.C.; et al. Human T-cell leukemia virus type I isolates from Gabon and Ghana: Comparative analysis of proviral genomes. Virology 1987, 161, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Besson, G.; Kazanji, M. One-step, multiplex, real-time PCR assay with molecular beacon probes for simultaneous detection, differentiation, and quantification of human T-cell leukemia virus types 1, 2, and 3. J. Clin. Microbiol. 2009, 47, 1129–1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salemi, M.; Van Dooren, S.; Audenaert, E.; Delaporte, E.; Goubau, P.; Desmyter, J.; Vandamme, A.M. Two new human T-lymphotropic virus type I phylogenetic subtypes in seroindeterminates, a Mbuti pygmy and a Gabonese, have closest relatives among African STLV-I strains. Virology 1998, 246, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Miura, T.; Fukunaga, T.; Igarashi, T.; Yamashita, M.; Ido, E.; Funahashi, S.; Ishida, T.; Washio, K.; Ueda, S.; Hashimoto, K.; et al. Phylogenetic subtypes of human T-lymphotropic virus type I and their relations to the anthropological background. Proc. Natl. Acad. Sci. USA 1994, 91, 1124–1127. [Google Scholar] [CrossRef] [Green Version]
- Moynet, D.; Cosnefroy, J.Y.; Bedjabaga, I.; Roelants, G.; Georges-Courbot, M.C.; Guillemain, B. Identification of new genetic subtypes of human T cell leukemia virus type I in Gabon from encoding sequence of surface envelope glycoprotein. AIDS Res. Hum. Retrovir. 1995, 11, 1407–1411. [Google Scholar] [CrossRef]
- Moynet, D.; Pouliquen, J.F.; Londos-Gagliardi, D.; Buigues, R.P.; Moreau, J.F.; Bedjabaga, I.; Georges, M.C.; Talarmin, A.; Joubert, M.; Fleury, H.; et al. High variability of HTLV-I in a remote population of Gabon as compared to that of a similar population of French Guiana. Virus Genes 2001, 23, 257–261. [Google Scholar] [CrossRef]
- Bahia, F.; Novais, V.; Evans, J.; Le Marchand, C.; Netto, E.; Page, K.; Brites, C. The impact of human T-cell lymphotropic virus I infection on clinical and immunologic outcomes in patients coinfected with HIV and hepatitis C virus. J. Acquir. Immune Defic. Syndr. 2011, 57, S202–S207. [Google Scholar] [CrossRef] [Green Version]
- Brites, C.; Alencar, R.; Gusmão, R.; Pedroso, C.; Netto, E.M.; Pedral-Sampaio, D.; Badaró, R. Co-infection with HTLV-1 is associated with a shorter survival time for HIV-1-infected patients in Bahia, Brazil. AIDS 2001, 15, 2053–2055. [Google Scholar] [CrossRef]
- Rossheim, A.E.B.; Cunningham, T.D.; Troy, S.B. Human T-lymphotropic Virus Co-infections in Adults Infected with Human Immunodeficiency Virus. Am. J. Med. Sci. 2016, 352, 258–260. [Google Scholar] [CrossRef]
- AlShamrani, N.H.; Alshaikh, M.A.; Elaiw, A.M.; Hattaf, K. Dynamics of HIV-1/HTLV-I Co-Infection Model with Humoral Immunity and Cellular Infection. Viruses 2022, 14, 1719. [Google Scholar] [CrossRef] [PubMed]
- Robert-Guroff, M.; Blayney, D.W.; Safai, B.; Lange, M.; Gelmann, E.P.; Gutterman, J.W.; Mansell, P.W.; Goedert, J.L.; Groopman, J.E.; Steigbigel, N.H.; et al. HTLV-I-specific antibody in AIDS patients and others at risk. Lancet 1984, 2, 128–131. [Google Scholar] [CrossRef] [PubMed]
- Pereira, F.M.; Santos, F.L.N.; Silva, Â.A.O.; Nascimento, N.M.; Almeida, M.; Carreiro, R.P.; Galvão-Castro, B.; Rios Grassi, M.F. Distribution of Human Immunodeficiency Virus and Human T-Leukemia Virus Co-infection in Bahia, Brazil. Front. Med. 2021, 8, 788176. [Google Scholar] [CrossRef]
- Casoli, C.; Pilotti, E.; Bertazzoni, U. Molecular and cellular interactions of HIV-1/HTLV coinfection and impact on AIDS progression. AIDS Rev. 2007, 9, 140–149. [Google Scholar] [PubMed]
- Gudo, E.S.; Bhatt, N.B.; Bila, D.R.; Abreu, C.M.; Tanuri, A.; Savino, W.; Silva-Barbosa, S.D.; Jani, I.V. Co-infection by human immunodeficiency virus type 1 (HIV-1) and human T cell leukemia virus type 1 (HTLV-1): Does immune activation lead to a faster progression to AIDS? BMC Infect Dis. 2009, 9, 211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrahão, M.H.; Lima, R.G.; Netto, E.; Brites, C. Short communication: Human lymphotropic virus type 1 coinfection modulates the synthesis of cytokines by peripheral blood mononuclear cells from HIV type 1-infected individuals. AIDS Res. Hum. Retrovir. 2012, 28, 806–808. [Google Scholar] [CrossRef]
- Geddes, V.E.V.; José, D.P.; Leal, F.E.; Nixon, D.F.; Tanuri, A.; Aguiar, R.S. HTLV-1 Tax activates HIV-1 transcription in latency models. Virology 2017, 504, 45–51. [Google Scholar] [CrossRef]
- Kubota, S.; Furuta, R.A.; Hatanaka, M.; Pomerantz, R.J. Modulation of HTLV-I gene expression by HIV-1 Rev through an alternative RxRE-independent pathway mediated by the RU5 portion of the 5’-LTR. Biochem. Biophys. Res. Commun. 1998, 243, 79–85. [Google Scholar] [CrossRef]
- Boxus, M.; Willems, L. Mechanisms of HTLV-1 persistence and transformation. Br. J. Cancer 2009, 101, 1497–1501. [Google Scholar] [CrossRef] [Green Version]
- Grassmann, R.; Aboud, M.; Jeang, K.-T. Molecular mechanisms of cellular transformation by HTLV-1 Tax. Oncogene 2005, 24, 5976–5985. [Google Scholar] [CrossRef] [Green Version]
- Norrgren, H.R.; Bamba, S.; Larsen, O.; Da Silva, Z.; Aaby, P.; Koivula, T.; Andersson, S. Increased prevalence of HTLV-1 in patients with pulmonary tuberculosis coinfected with HIV, but not in HIV-negative patients with tuberculosis. J. Acquir. Immune Defic. Syndr. 2008, 48, 607–610. [Google Scholar] [CrossRef] [PubMed]
- Pedral-Sampaio, D.B.; Martins Netto, E.; Pedrosa, C.; Brites, C.; Duarte, M.; Harrington, W., Jr. Co-Infection of Tuberculosis and HIV/HTLV Retroviruses: Frequency and Prognosis Among Patients Admitted in a Brazilian Hospital. Braz. J. Infect. Dis. 1997, 1, 31–35. [Google Scholar] [PubMed]
- Casseb, J.; Posada-Vergara, M.P.; Montanheiro, P.; Fukumori, L.M.; Olah, I.; Smid, J.; Duarte, A.J.; Penalva de Oliveira, A.C. T CD4+ cells count among patients co-infected with human immunodeficiency virus type 1 (HIV-1) and human T-cell leukemia virus type 1 (HTLV-1): High prevalence of tropical spastic paraparesis/HTLV-1-associated myelopathy (TSP/HAM). Rev. Inst. Med. Trop. Sao Paulo 2007, 49, 231–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oo, Z.; Barrios, C.S.; Castillo, L.; Beilke, M.A. High levels of CC-chemokine expression and downregulated levels of CCR5 during HIV-1/HTLV-1 and HIV-1/HTLV-2 coinfections. J. Med. Virol. 2015, 87, 790–797. [Google Scholar] [CrossRef]
- Toro, C.; Blanco, F.; García-Gascó, P.; Sheldon, J.; Benito, J.; Rallón, N.; Soriano, V. Human T Lymphotropic Virus Type 1-Associated Myelopathy/Tropical Spastic Paraparesis in an HIV-Positive Patient Coinfected with Human T Lymphotropic Virus Type 2 Following Initiation of Antiretroviral Therapy. Clin. Infect. Dis. 2007, 45, e118–e120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pau, A.K.; George, J.M. Antiretroviral therapy: Current drugs. Infect. Dis. Clin. N. Am. 2014, 28, 371–402. [Google Scholar] [CrossRef] [Green Version]
- Marino-Merlo, F.; Balestrieri, E.; Matteucci, C.; Mastino, A.; Grelli, S.; Macchi, B. Antiretroviral Therapy in HTLV-1 Infection: An Updated Overview. Pathogens 2020, 9, 342. [Google Scholar] [CrossRef]
- Barski, M.S.; Minnell, J.J.; Maertens, G.N. Inhibition of HTLV-1 Infection by HIV-1 First- and Second-Generation Integrase Strand Transfer Inhibitors. Front. Microbiol. 2019, 10, 1877. [Google Scholar] [CrossRef] [Green Version]
- Etoh, K.; Tamiya, S.; Yamaguchi, K.; Okayama, A.; Tsubouchi, H.; Ideta, T.; Mueller, N.; Takatsuki, K.; Matsuoka, M. Persistent clonal proliferation of human T-lymphotropic virus type I-infected cells in vivo. Cancer Res. 1997, 57, 4862–4867. [Google Scholar]
- Beilke, M.A.; Traina-Dorge, V.L.; Sirois, M.; Bhuiyan, A.; Murphy, E.L.; Walls, J.M.; Fagan, R.; Winsor, E.L.; Kissinger, P.J. Relationship between human T lymphotropic virus (HTLV) type 1/2 viral burden and clinical and treatment parameters among patients with HIV type 1 and HTLV-1/2 coinfection. Clin. Infect. Dis. 2007, 44, 1229–1234. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Country | Groups and Subtypes | Recombinant Forms | Origin | Reference |
|---|---|---|---|---|
| Cameroon | HIV-1 Group M, N, O, P A–D, F–H, J, K | CRF01_AE, CRF02_AG, CRF06_cpx, CRF09_cpx, CRF11_cpx, CRF13_cpx, CRF18_cpx, CRF22_01A1cpx, CRF25_cpx, CRF36_cpx, CRF37_cpx | Human immunodeficiency virus type 1 (HIV-1) subtypes in the northwest region, Cameroon | [26] |
| HIV infections in Northwestern Cameroon: identification of HIV-1 group O and dual HIV- 1 group M and group O infections | [27] | |||
| Four New HIV-1 group N isolates from Cameroon: Prevalence continues to be low | [28] | |||
| Confirmation of the putative HIV-1 group P in Cameroon | [29] | |||
| HIV-2 | HIV-2 intergroup recombinant identified in Cameroon | [30] | ||
| Equatorial Guinea | Group M A, B, C, D, E, F, G, H | CRF02_AG, CRF06_cpx, CRF09_cpx, CRF11_cpx CRF18_cpx | Description of the HIV-1 group M molecular epidemiology and drug resistance prevalence in Equatorial Guinea from migrants in Spain | [31] |
| Democratic Republic of Congo | Group M A1, A2, B, C, D, F1, G, F, J, K, L | CRF02_AG, CRF13_cpx, CRF25_cpx, CRF26_cpx, | HIV-1 subtypes and drug resistance mutations among female sex workers varied in different cities and regions of the Democratic Republic of Congo | [32] |
| Pathologies | Area of Diagnosis | Provincial Origin of the Patients | Sex | Age (by Year) | Outcome Diagnosis | Year of Diagnosis | References |
|---|---|---|---|---|---|---|---|
| TSP/HAM | Franceville | HAUT-OGOOUE | M | 55 | ND | 1989 | [67] |
| TSP/HAM | Franceville | HAUT-OGOOUE | M | 60 | ND | 1989 | [67] |
| TSP/HAM? | Ayanabo | HAUT-OGOOUE | M | ≈48 | ND | 2005 | [68] |
| TSP/HAM | Franceville | HAUT-OGOOUE | F | 70 | ND | 1997 | [69] |
| TSP/HAM | Franceville | HAUT-OGOOUE | F | … | ND | 1997 | [69] |
| ATL | Libreville | ESTUAIRE? | F | 35 | LNH | 1989 | [70] |
| ATL | Libreville | ESTUAIRE? | F | 48 | LNH | 1989 | [70] |
| ATL | Libreville | ESTUAIRE? | F | 52 | LNH | 1989 | [70] |
| ATL | Libreville | ESTUAIRE? | M | 42 | LNH | 1989 | [70] |
| ATL? | Libreville | … | M | 58 | MF | 1996 | [71] |
| ATL | Libreville | HAUT-OGOOUE | F | 50 | LNH | 2019 | [72] |
| ATL | Libreville | HAUT-OGOOUE | M | 50 | LNH | 2019 | [72] |
| ATL | Libreville | HAUT-OGOOUE | M | 39 | LNH | 2019 | [72] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oloumbou, E.F.; Engone-Ondo, J.D.; Mamimandjiami Idam, I.; Moussavou-Boudzanga, P.; Mfouo-Tynga, I.; Mouinga-Ondeme, A. Human T-Cell Leukemia Virus Type 1-Related Diseases May Constitute a Threat to the Elimination of Human Immunodeficiency Virus, by 2030, in Gabon, Central Africa. Viruses 2022, 14, 2808. https://doi.org/10.3390/v14122808
Oloumbou EF, Engone-Ondo JD, Mamimandjiami Idam I, Moussavou-Boudzanga P, Mfouo-Tynga I, Mouinga-Ondeme A. Human T-Cell Leukemia Virus Type 1-Related Diseases May Constitute a Threat to the Elimination of Human Immunodeficiency Virus, by 2030, in Gabon, Central Africa. Viruses. 2022; 14(12):2808. https://doi.org/10.3390/v14122808
Chicago/Turabian StyleOloumbou, Eldridge Fedricksen, Jéordy Dimitri Engone-Ondo, Issakou Mamimandjiami Idam, Pamela Moussavou-Boudzanga, Ivan Mfouo-Tynga, and Augustin Mouinga-Ondeme. 2022. "Human T-Cell Leukemia Virus Type 1-Related Diseases May Constitute a Threat to the Elimination of Human Immunodeficiency Virus, by 2030, in Gabon, Central Africa" Viruses 14, no. 12: 2808. https://doi.org/10.3390/v14122808