
High Immune Response Rate to the Fourth Boost of the BNT162b2 Vaccine against the Omicron Variants of Concern among Liver Transplant Recipients
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Serology Assay
2.1.1. Antibody Detection Testing
2.1.2. Viral Isolation of the Wild-Type and Omicron Variants and SARS-CoV-2 Micro-neutralization Assays
2.2. Statistical Analysis
3. Results
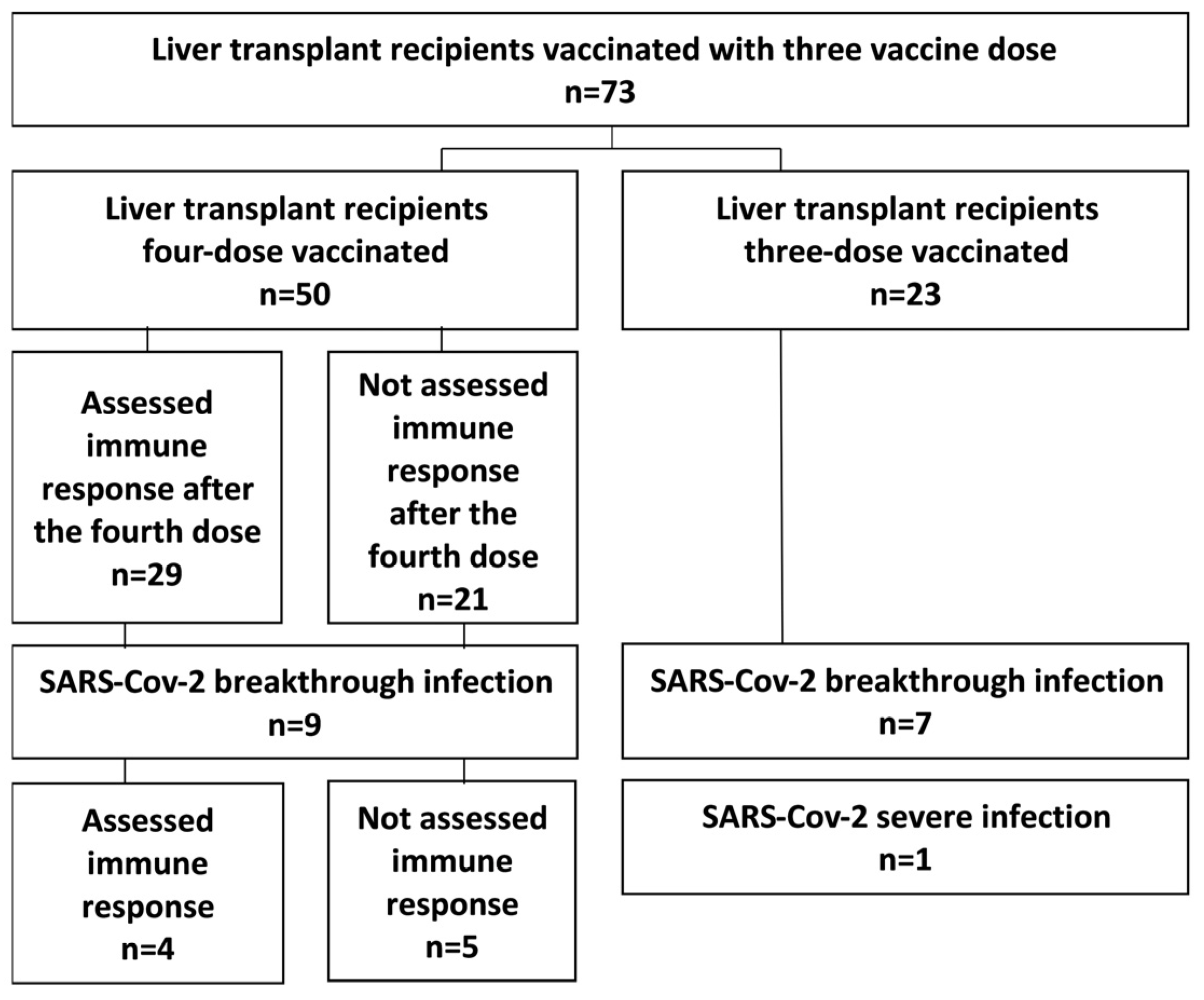
3.1. Baseline Characteristics
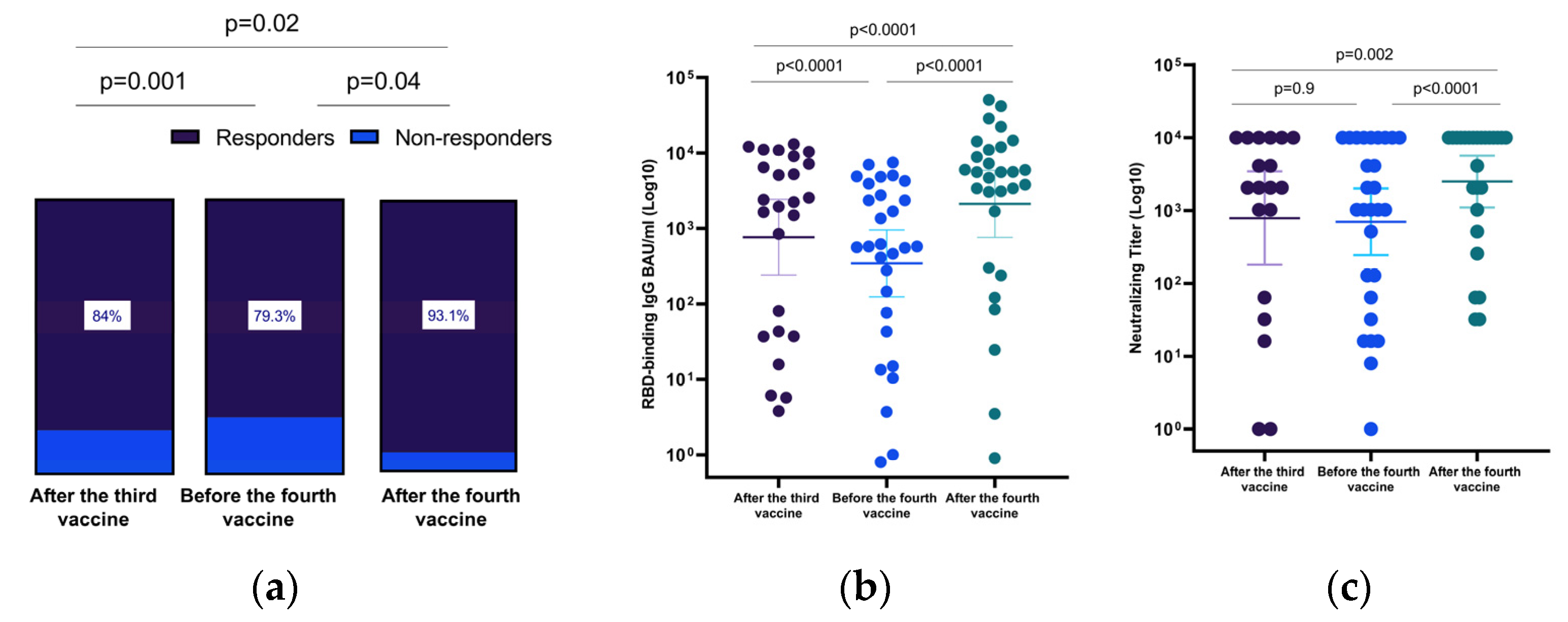
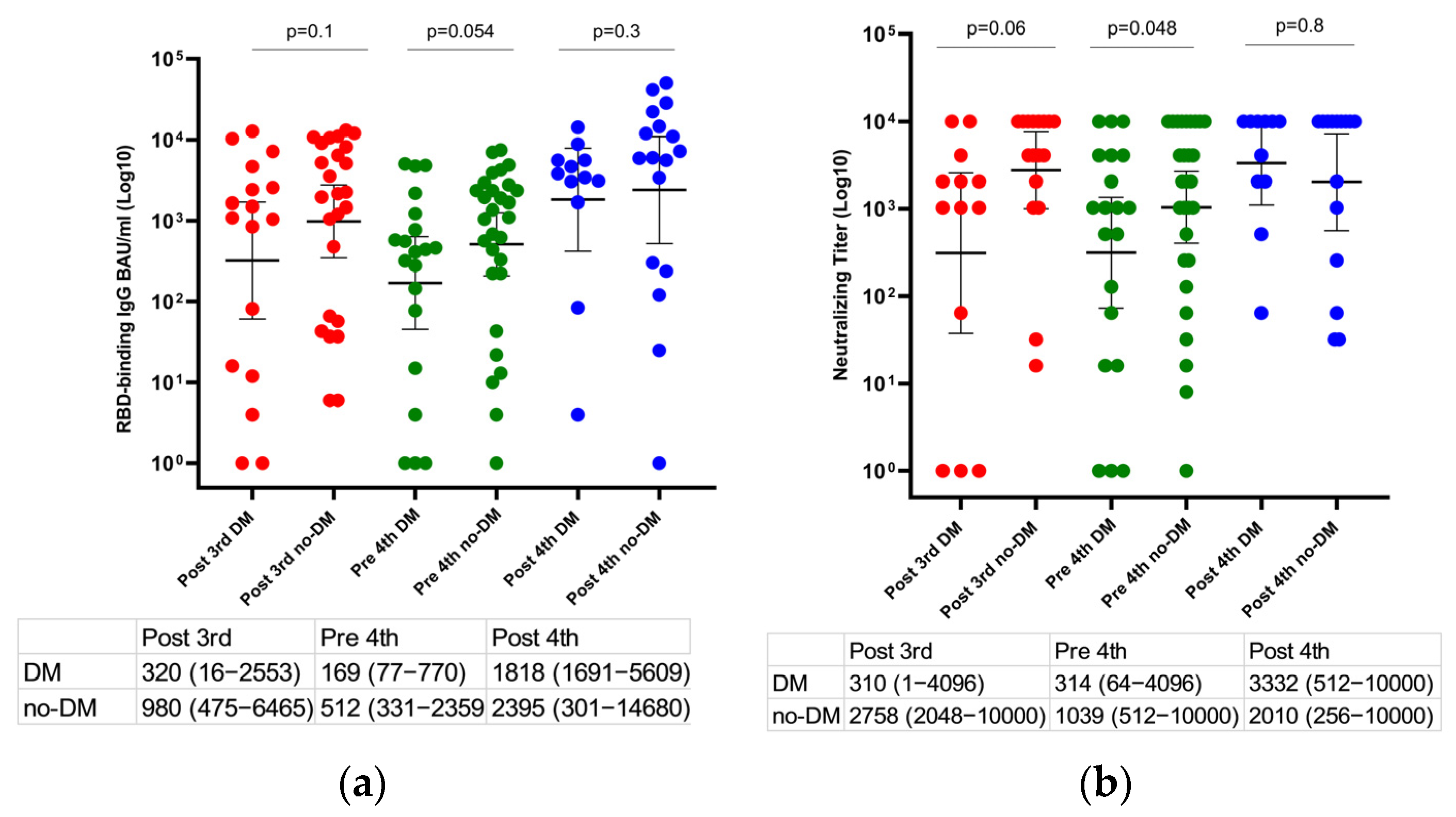
3.2. Humoral Immunity to the Fourth BNT162b2 mRNA Vaccine Dose
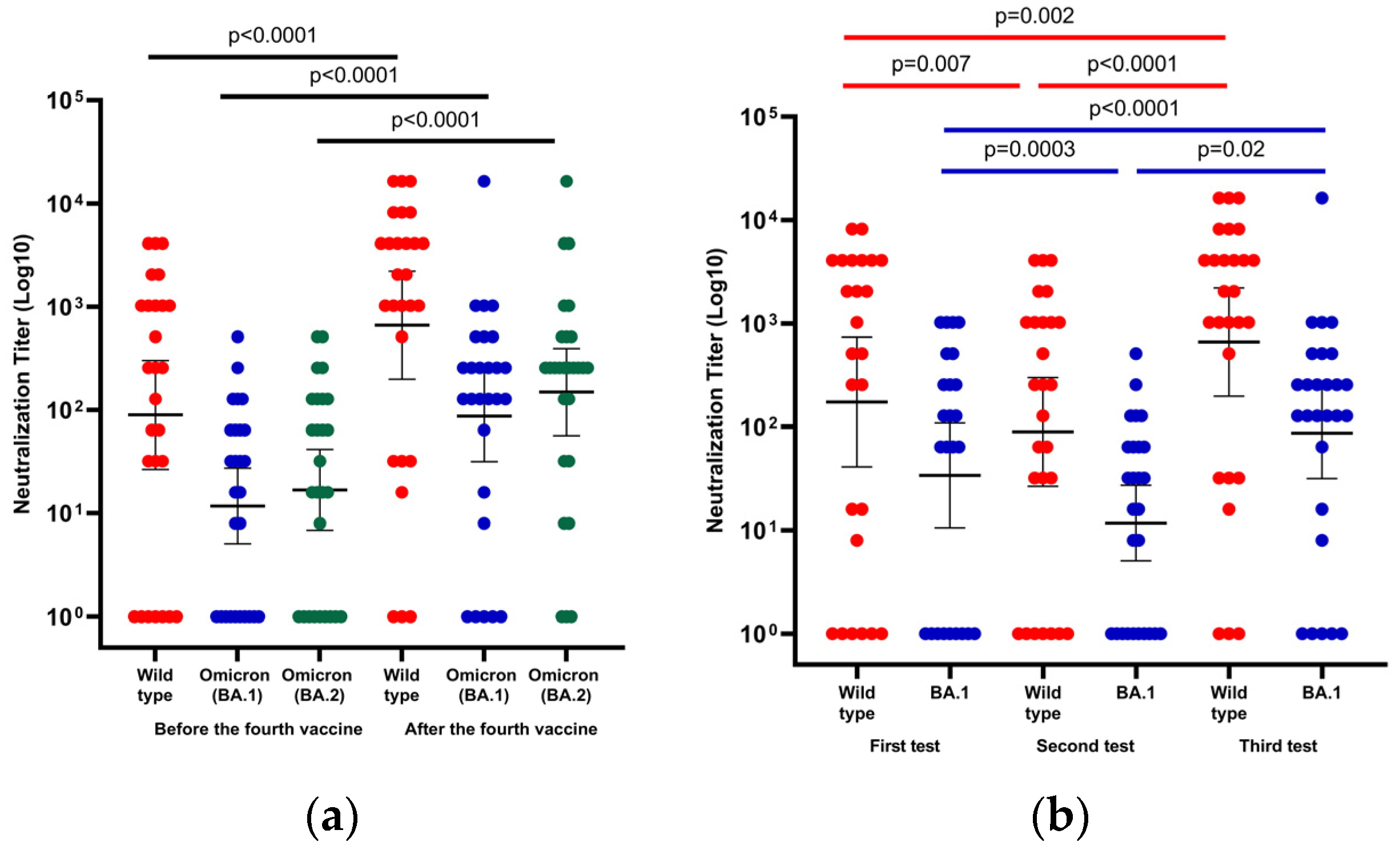
3.3. Neutralization of Wild-Type and Omicron Variants (BA.1 and BA.2 Variants)
3.4. Breakthrough Infection
3.5. Adverse Effects of the Fourth BNT162b2 mRNA Vaccine Dose
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davidov, Y.; Tsaraf, K.; Cohen-Ezra, O.; Likhter, M.; Ben Yakov, G.; Levy, I.; Levin, E.G.; Lustig, Y.; Mor, O.; Rahav, G.; et al. Immunogenicity and Adverse Effects of the 2-Dose BNT162b2 Messenger RNA Vaccine Among Liver Transplantation Recipients. Liver Transplant. 2021, 28, 215–223. [Google Scholar] [CrossRef]
- Rabinowich, L.; Grupper, A.; Baruch, R.; Ben-Yehoyada, M.; Halperin, T.; Turner, D.; Katchman, E.; Levi, S.; Houri, I.; Lubezky, N.; et al. Low immunogenicity to SARS-CoV-2 vaccination among liver transplant recipients. J. Hepatol. 2021, 75, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Grupper, A.; Rabinowich, L.; Schwartz, D.; Schwartz, I.F.; Ben-Yehoyada, M.; Shashar, M.; Katchman, E.; Halperin, T.; Turner, D.; Goykhman, Y.; et al. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus. Arab. Archaeol. Epigr. 2021, 21, 2719–2726. [Google Scholar] [CrossRef] [PubMed]
- Peled, Y.; Ram, E.; Lavee, J.; Sternik, L.; Segev, A.; Wieder-Finesod, A.; Mandelboim, M.; Indenbaum, V.; Levy, I.; Raanani, E.; et al. BNT162b2 vaccination in heart transplant recipients: Clinical experience and antibody response. J. Heart Lung Transplant. 2021, 40, 759–762. [Google Scholar] [CrossRef] [PubMed]
- Peled, Y.; Ram, E.; Lavee, J.; Segev, A.; Matezki, S.; Wieder-Finesod, A.; Halperin, R.; Mandelboim, M.; Indenbaum, V.; Levy, I.; et al. Third dose of the BNT162b2 vaccine in heart transplant recipients: Immunogenicity and clinical experience. J. Heart Lung Transplant. 2021, 41, 148–157. [Google Scholar] [CrossRef]
- Davidov, Y.; Indenbaum, V.; Tsaraf, K.; Cohen-Ezra, O.; Likhter, M.; Ben Yakov, G.; Halperin, R.; Levy, I.; Mor, O.; Agmon-Levin, N.; et al. A third dose of the BNT162b2 mRNA vaccine significantly improves immune responses among liver transplant recipients. J. Hepatol. 2022, 77, 702–709. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Amir, O.; Freedman, L.; Alroy-Preis, S.; Ash, N.; Huppert, A.; Milo, R. Protection by a Fourth Dose of BNT162b2 against Omicron in Israel. N. Engl. J. Med. 2022, 386, 1712–1720. [Google Scholar] [CrossRef]
- Nemet, I.; Kliker, L.; Lustig, Y.; Zuckerman, N.; Erster, O.; Cohen, C.; Kreiss, Y.; Alroy-Preis, S.; Regev-Yochay, G.; Mendelson, E.; et al. Third BNT162b2 Vaccination Neutralization of SARS-CoV-2 Omicron Infection. N. Engl. J. Med. 2022, 386, 492–494. [Google Scholar] [CrossRef]
- Regev-Yochay, G.; Gonen, T.; Gilboa, M.; Mandelboim, M.; Indenbaum, V.; Amit, S.; Meltzer, L.; Asraf, K.; Cohen, C.; Fluss, R.; et al. Efficacy of a Fourth Dose of COVID-19 mRNA Vaccine against Omicron. N. Engl. J. Med. 2022, 386, 1377–1380. [Google Scholar] [CrossRef]
- Ito, K.; Piantham, C.; Nishiura, H. Relative instantaneous reproduction number of Omicron SARS-CoV-2 variant with respect to the Delta variant in Denmark. J. Med. Virol. 2022, 94, 2265–2268. [Google Scholar] [CrossRef]
- Maslo, C.; Friedland, R.; Toubkin, M.; Laubscher, A.; Akaloo, T.; Kama, B. Characteristics and Outcomes of Hospitalized Patients in South Africa During the COVID-19 Omicron Wave Compared with Previous Waves. JAMA 2022, 327, 583. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Han, J.; Zhang, Y.; He, J.; Yu, W.; Zhang, X.; Wu, J.; Zhang, S.; Kong, Y.; Guo, Y.; et al. SARS-CoV-2 Omicron Variant: Epidemiological Features, Biological Characteristics, and Clinical Significance. Front. Immunol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Collier, A.-R.Y.; Rowe, M.; Mardas, F.; Ventura, J.D.; Wan, H.; Miller, J.; Powers, O.; Chung, B.; Siamatu, M.; et al. Neutralization of the SARS-CoV-2 Omicron BA.1 and BA.2 Variants. N. Engl. J. Med. 2022, 386, 1579–1580. [Google Scholar] [CrossRef] [PubMed]
- Ma, E.; Ai, J.; Zhang, Y.; Zheng, J.; Gao, X.; Xu, J.; Yin, H.; Fu, Z.; Xing, H.; Li, L.; et al. Omicron infections profile and vaccination status among 1881 liver transplant recipients: A multi-centre retrospective cohort. Emerg. Microbes Infect. 2022, 11, 2636–2644. [Google Scholar] [CrossRef] [PubMed]
- Peled, Y.; Afek, A.; Nemet, I.; Rahav, G.; Raanani, E.; Patel, J.K.; Mandelboim, M. Fourth BNT162b2 vaccination neutralization of omicron infection after heart transplantation. J. Heart Lung Transplant. 2022, 41, 1210–1213. [Google Scholar] [CrossRef]
- Midtvedt, K.; Vaage, J.T.; Heldal, K.; Munthe, L.A.; Lund-Johansen, F.; Åsberg, A. Fourth dose of the SARS-CoV -2 vaccine in kidney transplant recipients with previously impaired humoral antibody response. Am. J. Transplant. 2022, 22, 2704–2706. [Google Scholar] [CrossRef]
- Harberts, A.; Schaub, G.M.; Ruether, D.F.; Duengelhoef, P.M.; Brehm, T.T.; Karsten, H.; Fathi, A.; Jahnke-Triankowski, J.; Fischer, L.; Addo, M.M.; et al. Humoral and Cellular Immune Response After Third and Fourth SARS-CoV-2 mRNA Vaccination in Liver Transplant Recipients. Clin. Gastroenterol. Hepatol. 2022, 20, 2558–2566.e5. [Google Scholar] [CrossRef] [PubMed]
- Lustig, Y.; Sapir, E.; Regev-Yochay, G.; Cohen, C.; Fluss, R.; Olmer, L.; Indenbaum, V.; Mandelboim, M.; Doolman, R.; Amit, S.; et al. BNT162b2 COVID-19 vaccine and correlates of humoral immune responses and dynamics: A prospective, single-centre, longitudinal cohort study in health-care workers. Lancet Respir. Med. 2021, 9, 999–1009. [Google Scholar] [CrossRef]
- Lustig, Y.; Nemet, I.; Kliker, L.; Zuckerman, N.; Yishai, R.; Alroy-Preis, S.; Mendelson, E.; Mandelboim, M. Neutralizing Response against Variants after SARS-CoV-2 Infection and One Dose of BNT162b2. N. Engl. J. Med. 2021, 384, 2453–2454. [Google Scholar] [CrossRef]
- Lustig, Y.; Gonen, T.; Meltzer, L.; Gilboa, M.; Indenbaum, V.; Cohen, C.; Amit, S.; Jaber, H.; Doolman, R.; Asraf, K.; et al. Superior immunogenicity and effectiveness of the third compared to the second BNT162b2 vaccine dose. Nat. Immunol. 2022, 23, 940–946. [Google Scholar] [CrossRef]
- Prasad, N.; Derado, G.; Nanduri, S.A.; Reses, H.E.; Dubendris, H.; Wong, E.; Soe, M.M.; Li, Q.; Dollard, P.; Bagchi, S.; et al. Effectiveness of a COVID-19 Additional Primary or Booster Vaccine Dose in Preventing SARS-CoV-2 Infection Among Nursing Home Residents During Widespread Circulation of the Omicron Variant—United States, February 14–March 27, 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Kantauskaite, M.; Müller, L.; Kolb, T.; Fischer, S.; Hillebrandt, J.; Ivens, K.; Andree, M.; Luedde, T.; Orth, H.M.; Adams, O.; et al. Intensity of mycophenolate mofetil treatment is associated with an impaired immune response to SARS-CoV-2 vaccination in kidney transplant recipients. Am. J. Transplant. 2021, 22, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N. Metabolic disorders, COVID-19 and vaccine-breakthrough infections. Nat. Rev. Endocrinol. 2021, 18, 75–76. [Google Scholar] [CrossRef] [PubMed]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. COVID-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total LT Cohort n = 73 | Three Vaccine Doses n = 23 | Four Vaccine Doses n = 50 | p |
|---|---|---|---|---|
| Age, years | 63.8 (52.1–70.4) | 65.3 (44.7–70.1) | 62.7 (53.1–70.6) | 0.8 |
| Male, n (%) | 37 (51) | 11 (47.8) | 26 (52) | 0.7 |
| Indication for LT | 0.3 | |||
| Hepatitis C, n (%) | 16 (21.9) | 5 (21.7) | 11 (22) | |
| NASH, n (%) | 16 (21.9) | 2 (8.7) | 14 (28) | |
| Hepatitis B, n (%) | 6 (8.2) | 4 (17.4) | 2 (4) | |
| PSC, n (%) | 9 (12.3) | 1 (4.3) | 8 (16) | |
| PBC, n (%) | 3 (4.1) | 1 (4.3) | 2 (4) | |
| ALD, n (%) | 5 (6.8) | 3 (13) | 2 (4) | |
| Other, n (%) ¶ | 18 (24.7) | 7 (30.4) | 11 (22) | |
| Age at transplantation, years | 52.5 (41.9–62.1) | 49 (30.8–60.3) | 53 (44.8–62.8) | 0.2 |
| Time since liver transplantation, years | 9.2 (5.3–16.4) | 12.4 (5.3–23.3) | 7.7 (5.3–15.5) | 0.3 |
| Comorbidities | ||||
| Diabetes mellitus, n (%) | 30 (41.1) | 9 (39.1) | 21 (42) | 0.8 |
| Hypertension, n (%) | 39 (53.4) | 12 (52.2) | 27 (54) | 0.8 |
| Dyslipidemia, n (%) | 34 (46.6) | 11 (47.8) | 23 (46) | 0.8 |
| Chronic kidney disease, n (%) | 28 (38.4) | 10 (43.5) | 18 (36) | 0.5 |
| BMI, kg/m2 | 25.8 (22.3–27.9) | 24.7 (21–27.9) | 26.2 (22.7–27.9) | 0.5 |
| WBC, K/microL | 5.7 (4.7–6.8) | 7 (5.1–7.2) | 5.4 (4.5–6.7) | 0.2 |
| Hemoglobin, g/dL | 13 (11.8–14.3) | 13.3 (10.9–14) | 13 (12–14.7) | 0.1 |
| Platelets, K/microL | 168 (131–217) | 170 (121–191) | 164 (131–221) | 0.6 |
| Creatinine, mg/dL | 1 (0.81–1.25) | 1.0 (0.8–1.3) | 1.0 (0.8–1.2) | 0.9 |
| ALT, IU/L | 20.5 (15–29.5) | 23 (14–34) | 20 (16–27) | 0.9 |
| ALP, IU/L | 100 (75–134) | 109 (84–130) | 99.5 (74.5–137.5) | 0.6 |
| Bilirubin, mg/dL | 0.6 (0.5–0.8) | 0.6 (0.4–0.9) | 0.6 (0.5–0.8) | 0.9 |
| Characteristics | Total LT Cohort n = 73 | Three Vaccine Doses n = 23 | Four Vaccine Doses n = 50 | p |
|---|---|---|---|---|
| Tacrolimus dose, mg/trough level, ng/mL | 3 (2–4)/5 (4–7) | 3 (2–4)/5 (4–7) | 3 (2–4)/5 (4–6) | 0.8/0.8 |
| Prednisone, n (%)/dose, mg | 13 (17.8)/5 (5–8) | 4 (17.4) | 9 (18) | 0.9/0.3 |
| MMF, n (%)/dose mg | 21 (28.8)/100 (720–1000) | 6 (26.1)/1000 (720–1000) | 15 (30)/1000 (500–1000) | 0.7/0.9 |
| Everolimus, n (%)/dose mg/trough level, ng/mL | 10 (13.7)/2 (2–3)/4 (3–6) | 1 (4.3)/1/4 | 9 (18)/2 (2–3)/4 (3–6) | 0.1/0.2/1 |
| CNI monotherapy, n (%) | 38 (53.5) | 13 (56.5) | 25 (52.1) | 0.7 |
| Double ‡/triple, n (%) ‡‡ immunosuppression | 28 (38.4)/6 (8.2) | 10 (43.5)/0 | 18 (36)/6 (12) | 0.2 |
| SARS-CoV-2 infection | 16 (21.9) | 7 (30.4) | 9 (18) | 0.2 |
| Positive immune response * one month after the third vaccine § | 47 (81) | 12 (75) | 35 (83.3) | 0.5 |
| Positive immune response * four months after the third vaccine §§ | 56 (77.8) | 16 (69.6) | 40 (81.6) | 0.3 |
| Characteristics | First Test One Month after the Third Dose ‡ n = 25 | Second Test Four Months after the Third Dose ‡‡ n = 29 | Third test One Month after the Fourth Dose ‡‡‡ n = 29 |
|---|---|---|---|
| Positive anti-RBD IgG *, n (%) | 21 (84) | 23 (79.3) | 27 (93.1) |
| 50% SARS-CoV-2 pseudo-virus neutralization titer, GM (CI 95%) | 785 (180–3434) | 699 (244–2008) | 2489 (1098–5640) |
| Anti-RBD IgG titer, BAU/mL, GM (CI 95%) | 766 (241–2428) | 345 (124–955) | 2118 (761–5900) |
| 50% wild-type neutralization titer, GM (CI 95%) | 174 (41–737) | 89 (27–301) | 662 (198–2209) |
| 50% Omicron BA.1 neutralization titer, GM (CI 95%) | 34 (11–109) | 12 (5–27) | 87 (32–241) |
| Characteristics | Serology Assessment after the Fourth Vaccine n = 29 | Non-Responders n = 2 | Responders n = 27 | p |
|---|---|---|---|---|
| Age, years | 64.2 (54.3–70.4) | 64.8 (54.3–75.4) | 64 (49.2–10.4) | 0.8 |
| Male, n (%) | 16 (55.2) | 1 (50) | 15 (55.6) | 0.7 |
| Age at transplantation, years | 54.2 (41–63.1) | 59.4 (53.4–65.4) | 54.2 (40.1–63.1) | 0.5 |
| Time since liver transplantation, years | 7.5 (4.3–15) | 5.4 (0.9–9.97) | 7.5 (4.3–15.2) | 0.4 |
| Comorbidities | ||||
| Diabetes mellitus, n (%) | 12 (41.4) | 1 (50) | 11 (40.7) | 0.7 |
| Hypertension, n (%) | 13 (44.8) | 1 (50) | 12 (44.4) | 0.7 |
| Dyslipidemia, n (%) | 12 (41.4) | 1 (50) | 11 (40.7) | 0.7 |
| Chronic kidney disease, n (%) | 10 (34.5) | 1 (50) | 9 (33.3) | 0.6 |
| BMI, kg/m2 | 25.3 (22.1–27) | 20.9 (15.8–26.1) | 25.3 (22.1–27.4) | 0.4 |
| WBC, K/microL | 5.7 (4.8–6.6) | 4.5 (4.2–4.7) | 5.7 (4.8–6.7) | 0.1 |
| Hemoglobin, g/dL | 13.1 (12.4–15.5) | 11.1 (10.2–12) | 13.6 (12.4–16) | 0.04 |
| Creatinine, mg/dL | 0.97 (0.8–1.2) | 1.2 (1.1–1.3) | 0.9 (0.8–1.2) | 0.2 |
| ALT, IU/L | 19 (17–26) | 20.5 (17–24) | 19 (16–27) | 1.0 |
| Prednisone, n (%) | 3 (10.3) | 0 | 3 (11.1) | 0.8 |
| MMF, n (%) | 8 (27.6) | 1 (50) | 7 (25.9) | 0.5 |
| Everolimus, n (%) | 4 (13.8) | 1 (50) | 3 (11.1) | 0.3 |
| CNI monotherapy, n (%) | 13 (44.8) | 0 | 16 (59.3) | 0.1 |
| Double/triple immunosuppression, n (%) | 11 (37.9)/2 (6.9) | 2 (100) | 9 (33.3)/2 (7.4) | 0.2 |
| SARS-CoV-2 infection, n (%) | 3 (10.3) | 0 | 3 (11.1) | 0.8 |
| Characteristics | No SARS-CoV-2 Infection n = 41 | SARS-CoV-2 Infection n = 9 | p-Value |
|---|---|---|---|
| Age, years | 61.8 (54–71) | 66.4 (52–70.4) | 0.8 |
| Male, n (%) | 20 (48.8) | 6 (66.7) | 0.9 |
| Age at transplantation, years | 53 (45–60) | 54 (45–63) | 0.9 |
| Comorbidities | |||
| Diabetes mellitus, n (%) | 14 (34.1) | 7 (77.8) | 0.016 |
| Hypertension, n (%) | 21 (51) | 6 (66.7) | 0.4 |
| Dyslipidemia, n (%) | 18 (44) | 5 (55.6) | 0.5 |
| Chronic kidney disease, n (%) | 14 (34) | 4 (44.4) | 0.5 |
| BMI, kg/m2 | 25 (22–28) | 27 (26–28) | |
| WBC, K/microL | 5.7 (4.7–7.0) | 4.6 (3.9–5.2) | 0.05 |
| Hemoglobin, g/dL | 13 (12.3–15.2) | 13.7 (11.5–14.1) | 0.6 |
| Creatinine, mg/dL | 0.97 (0.8–1.2) | 1.23 (1.0–1.5) | 0.096 |
| ALT, IU/L | 19 (16–26) | 26.5 (15.5–44.5) | 0.4 |
| Prednisone, n (%) | 8 (19)/5 (5–6) | 1 (11.1)/5 | 0.5/1 |
| MMF, n (%) | 11 (26.8)/1000 (750–1500) | 9 (100)/625 (500–875) | 0.3/0.2 |
| Everolimus, n (%) | 4 (3–6)/9 (22) | 0 | 0.1/NA |
| CNI monotherapy, n (%) | 20 (51.3) | 5 (55.6) | 0.8 |
| Double/triple immunosuppression, n (%) | 14 (34.1)/6 (14.6) | 4(44.4)/0 | 0.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davidov, Y.; Indenbaum, V.; Atari, N.; Kliker, L.; Tsaraf, K.; Asraf, K.; Cohen-Ezra, O.; Likhter, M.; Mor, O.; Doolman, R.; et al. High Immune Response Rate to the Fourth Boost of the BNT162b2 Vaccine against the Omicron Variants of Concern among Liver Transplant Recipients. Viruses 2022, 14, 2769. https://doi.org/10.3390/v14122769
Davidov Y, Indenbaum V, Atari N, Kliker L, Tsaraf K, Asraf K, Cohen-Ezra O, Likhter M, Mor O, Doolman R, et al. High Immune Response Rate to the Fourth Boost of the BNT162b2 Vaccine against the Omicron Variants of Concern among Liver Transplant Recipients. Viruses. 2022; 14(12):2769. https://doi.org/10.3390/v14122769
Chicago/Turabian StyleDavidov, Yana, Victoria Indenbaum, Nofar Atari, Limor Kliker, Keren Tsaraf, Keren Asraf, Oranit Cohen-Ezra, Mariya Likhter, Orna Mor, Ram Doolman, and et al. 2022. "High Immune Response Rate to the Fourth Boost of the BNT162b2 Vaccine against the Omicron Variants of Concern among Liver Transplant Recipients" Viruses 14, no. 12: 2769. https://doi.org/10.3390/v14122769