
SARSPLEX: Multiplex Serological ELISA with a Holistic Approach
 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Specimens
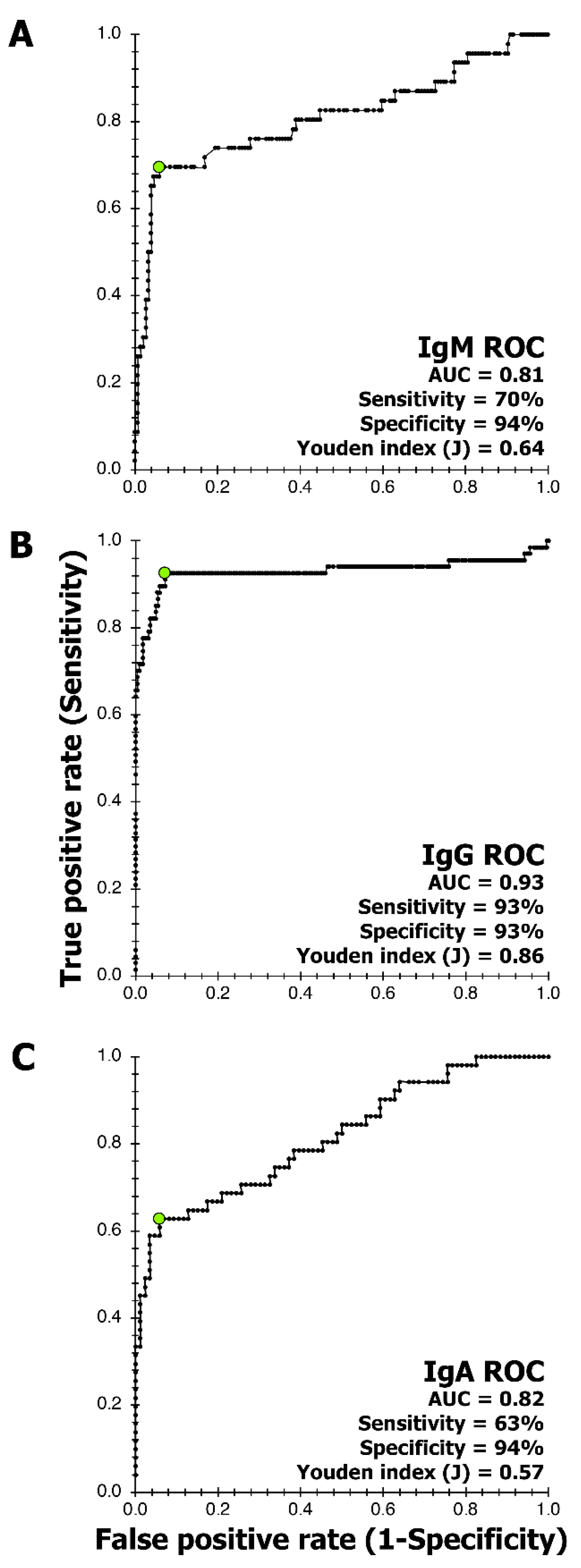
2.2. ELISA Procedure and Cut-Off Determination Using Receiver Operating Curve
2.3. Precision
2.4. Clinical Performance
2.5. Occupational Surveillance
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- John Hopkins University of Medicine. Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 31 August 2022).
- WHO. Coronavirus Disease (COVID-19) Technical Guidance: Laboratory Testing for 2019-nCoV in Humans. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/laboratory-guidance (accessed on 3 June 2022).
- 360Dx. An Independent Online News Organization Based in New York. 360Dx was launched in 2016, to Cover Emerging Economic and Technological Trends in the Clinical Diagnostic Market. Available online: https://www.360dx.com/ (accessed on 3 June 2022).
- Farge, E.; Revill, J. ‘Test, Test, Test’: WHO Chief’s Coronavirus Message to World. Reuters. 2020. Available online: https://www.reuters.com/article/us-healthcare-coronavirus-who-idUSKBN2132S4 (accessed on 30 October 2022).
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.Y.; Chen, L.; Wang, M. Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [Green Version]
- Hu, Z.; Song, C.; Xu, C.; Jin, G.; Chen, Y.; Xu, X.; Ma, H.; Chen, W.; Lin, Y.; Zheng, Y.; et al. Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China. Sci. China Life Sci. 2020, 63, 706–711. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Yi, Y.; Luo, X.; Xiong, N.; Liu, Y.; Li, S.; Sun, R.; Wang, Y.; Hu, B.; Chen, W.; et al. Development and Clinical Application of a Rapid IgM-IgG Combined Antibody Test for SARS-CoV-2 Infection Diagnosis. J. Med. Virol. 2020, 92, 1518–1524. [Google Scholar] [CrossRef] [PubMed]
- EC, European Commission. Current Performance of COVID-19 Test Methods and Devices and Proposed Performance criteria. Available online: https://ec.europa.eu/docsroom/documents/40805 (accessed on 6 June 2022).
- Rotondo, J.C.; Martini, F.; Maritati, M.; Caselli, E.; Gallenga, C.E.; Guarino, M.; De Giorgio, R.; Mazziotta, C.; Tramarin, M.L.; Badiale, G.; et al. Advanced Molecular and Immunological Diagnostic Methods to Detect SARS-CoV-2 Infection. Microorganisms 2022, 10, 1193. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Li, J. Immunologic Testing for SARS-CoV-2 Infection from the Antigen Perspective. J. Clin. Microbiol. 2021, 59, e02160-20. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Ren, L.; Yang, S.; Xiao, M.; Chang, D.; Yang, F.; Cruz, C.S.D.; Wang, Y.; Wu, C.; Xiao, Y.; et al. Profiling Early Humoral Response to Diagnose Novel Coronavirus Disease (COVID-19). Clin. Infect. Dis. 2020, 71, 778–785. [Google Scholar] [CrossRef] [Green Version]
- Amanat, F.; Stadlbauer, D.; Strohmeier, S.; Nguyen, T.H.O.; Chromikova, V.; McMahon, M.; Jiang, K.; Asthagiri Arunkumar, G.; Jurczyszak, D.; Polanco, J.; et al. A serological assay to detect SARS-CoV-2 seroconversion in humans. Nat. Med. 2020, 26, 1033–1036. [Google Scholar] [CrossRef]
- Walls, A.C.; Park, Y.-J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell 2020, 181, 281–292.e6. [Google Scholar] [CrossRef]
- Kannan, S.; Ali, P.S.S.; Sheeza, A.; Hemalatha, K. COVID-19 (Novel Coronavirus 2019)-recent trends. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 2006–2011. [Google Scholar] [CrossRef]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. Discovery of a novel coronavirus associated with the recent pneumonia outbreak in humans and its potential bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef]
- Fraire, A.E.; Woda, B.A.; Welsh, R.M.; Kradin, R.L. (Eds.) Coronavirus. In Viruses and the Lung: Infections and Non-Infectious Viral-Linked Lung Disorders; Springer: Berlin/Heidelberg, Germany, 2014; pp. XIV, 243. [Google Scholar]
- Leung, D.T.M.; Tam, F.C.H.; Ma, C.H.; Chan, P.; Cheung, J.L.K.; Niu, H.; Tam, J.S.L.; Lim, P.L. Antibody Response of Patients with Severe Acute Respiratory Syndrome (SARS) Targets the Viral Nucleocapsid. J. Infect. Dis. 2004, 190, 379–386. [Google Scholar] [CrossRef] [Green Version]
- FIND. 2020. Available online: https://www.finddx.org/covid-19/pipeline/ (accessed on 6 June 2022).
- Liu, W.; Liu, L.; Kou, G.; Zheng, Y.; Ding, Y.; Ni, W.; Wang, Q.; Tan, L.; Wu, W.; Tang, S.; et al. Evaluation of Nucleocapsid and Spike Protein-based ELISAs for detecting antibodies against SARS-CoV-2. J. Clin. Microbiol. 2020, 58, e00461-20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Zhang, X.; Liu, J.; Ban, Y.; Li, N.; Wu, Y.; Liu, Y.; Ye, R.; Liu, J.; Li, X.; et al. Serological detection of 2019-nCoV respond to the epidemic: A useful complement to nucleic acid testing. Int. Immunopharmacol. 2020, 88, 106861. [Google Scholar] [CrossRef] [PubMed]
- Long, Q.; Deng, H.; Chen, J.; Hu, J.; Liu, B.; Liao, P.; Lin, Y.; Yu, L.; Mo, Z.; Xu, Y.; et al. Antibody responses to SARS-CoV-2 in COVID-19 patients: The perspective application of serological tests in clinical practice. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.F.; Korevaar, D.A.; Altman, D.G.; Bruns, D.E.; Gatsonis, C.A.; Hooft, L.; Irwig, L.; Levine, D.; Reitsma, J.B.; de Vet, H.C.W.; et al. STARD 2015 guidelines for reporting diagnostic accuracy studies: Explanation and elaboration. BMJ Open 2016, 6, e012799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, M.J.; Powers, M.L.; Gronowski, K.S.; Gronowski, A.M. Clinical Chemistry Human Tissue Ownership and Use in Research: What Laboratorians and Researchers Should Know. Clin. Chem. 2010, 56, 1675–1682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garg, K.; Meriläinen, L.; Franz, O.; Pirttinen, H.; Quevedo-Diaz, M.; Croucher, S.; Gilbert, L. Evaluating polymicrobial immune responses in patients suffering from tick-borne diseases. Nat. Sci. Rep. 2018, 8, 15932. [Google Scholar] [CrossRef] [PubMed]
- TICKPLEX. Available online: www.tezted.com (accessed on 3 June 2022).
- Banoo, S.; Bell, D.; Bossuyt, P.; Herring, A.; Mabey, D.; Poole, F.; Smith, P.G.; Sriram, N.; Wongsrichanalai, C.; Linke, R.; et al. Diagnostics Evaluation Expert Panel (WHO/TDR) Evaluation of diagnostic tests for infectious diseases: General principles. Nat. Rev. Genet. 2006, 4, S21–S31. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using SPSS; SAGE: London, UK, 2009. [Google Scholar]
- Andreasson, U.; Perret-Liaudet, A.; van Waalwijk van Doorn, L.J.C.; Blennow, K.; Chiasserini, D.; Engelborghs, S.; Fladby, T.; Genc, S.; Kruse, N.; Kuiperij, H.B.; et al. A Practical Guide to Immunoassay Method Validation. Front. Neurol. 2015, 6, 179. [Google Scholar] [CrossRef]
- Reed, G.F.; Lynn, F.; Meade, B.D. Use of Coefficient of Variation in Assessing Variability of Quantitative Assays. Clin. Vaccine Immunol. 2002, 9, 1235–1239. [Google Scholar] [CrossRef]
- Cicchetti, D.V.; Feinstein, A.R. High agreement but low kappa: II. Resolving the paradoxes. J. Clin. Epidemiol. 1990, 43, 551–558. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Sim, J.; Wright, C.C. The Kappa Statistic in Reliability Studies: Use, Interpretation, and Sample Size Requirements. Phys. Ther. 2005, 85, 257–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okba, N.M.A.; Müller, M.A.; Li, W.; Wang, C.; Geurtsvan Kessel, C.H.; Corman, V.M.; Lamers, M.M.; Sikkema, R.S.; de Bruin, E.; Chandler, F.D.; et al. SARS-CoV-2 specific antibody responses in COVID-19 patients. Emerg. Infect. Dis. 2020, 26, 1478–1488. [Google Scholar] [CrossRef]
- Leeflang, M.; Moons, K.G.M.; Reitsma, J.B.; Zwinderman, A.H. Bias in sensitivity and specificity caused by data-driven selection of optimal cutoff values: Mechanisms, magnitude, and solutions. Clin. Chem. 2008, 54, 729–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawlins, M.L.; Swenson, E.M.; Hill, H.R.; Litwin, C.M. Evaluation of an Enzyme Immunoassay for Detection of Immunoglobulin M Antibodies to West Nile Virus and the Importance of Background Subtraction in Detecting Nonspecific Reactivity. Clin. Vaccine Immunol. 2007, 14, 665–668. [Google Scholar] [CrossRef] [Green Version]
- Pickering, J.W.; Forghanib, B.; Shellb, G.R.; Wu, L. Comparative evaluation of three recombinant antigen-based enzyme immunoassays for detection of IgM and IgG antibodies to human parvovirus B19. Clin. Diagn. Virol. 1998, 9, 57–63. [Google Scholar] [CrossRef]
- Sananez, I.; Raiden, S.C.; Algieri, S.C.; Uranga, M.; Grisolía, N.A.; Filippo, D.; De Carli, N.; Di Lalla, S.; Cairoli, H.; Chiolo, M.J.; et al. A poor and delayed anti-SARS-CoV2 IgG response is associated to severe COVID-19 in children. eBioMedicine 2021, 72, 103615. [Google Scholar] [CrossRef]
- Wan, W.Y.; Lim, S.H.; Seng, E.H. Cross-reaction of sera from COVID-19 patients with SARS-CoV assays. Ann. Acad. Med. Singap. 2021, 50, 703–711. [Google Scholar] [CrossRef]
- Chan, K.H.; Cheng, V.C.C.; Woo, P.C.Y.; Lau, S.K.P.; Poon, L.; Guan, Y.; Seto, W.H.; Yuen, K.-Y.; Peiris, J.S.M. Serological responses in patients with severe acute respiratory syndrome coronavirus infection and cross-reactivity with human coronaviruses 229E, OC43, and NL63. Clin. Vaccine Immunol. 2005, 12, 1317–1321. [Google Scholar] [CrossRef]
- Khan, S.; Nakajima, R.; Jain, A.; Ramiro de Assis, R.; Jasinskas, A.; Obiero, J.M.; Adenaiye, O.; Tai, S.; Hong, F.; Milton, D.K.; et al. Prometheus Study Group Analysis of Serologic Cross-Reactivity Between Common Human Coronaviruses and SARS-CoV-2 Using Coronavirus Antigen Microarray. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Ou, X.; Liu, Y.; Lei, X.; Li, P.; Mi, D.; Ren, L.; Guo, L.; Guo, R.; Chen, T.; Hu, J.; et al. Characterization of spike glycoprotein of SARS-CoV-2 on virus entry and its immune cross-reactivity with SARS-CoV. Nat. Commun. 2020, 11, 1620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senol, G.; Demirci, F. A case of parvovirus B19 infection diagnosed as COVID-19 due to false PCR positivity. Klimik Derg. Turk. 2022, 35, 54–57. [Google Scholar] [CrossRef]
- Harvey, R.; Mattiuzzo, G.; Hassall, M.; Sieberg, A.; Muller, M.A.; Drosten, C.; Rigsby, P.; Oxenford, C.J. study participants. Comparison of Serologic Assays for Middle East Respiratory Syndrome Coronavirus. Emerg. Infect. Dis. 2019, 25, 1878–1883. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Specimen Categories | IgM (n) | IgG (n) | IgA (n) |
|---|---|---|---|
| SARS-CoV-2 antibody positive | 13 | 66 | 23 |
| SARS-CoV-2 antibody negative | 52 | 78 | 22 |
| RT-PCR positive with disease onset <19 days | 7 | 7 | 7 |
| RT-PCR positive with disease onset ≥19 days | 26 | 26 | 26 |
| RT-PCR negative | 2 | 2 | 2 |
| Human Parvovirus B19 positive | 2 | 2 | 2 |
| Pre-2019-CoV | 64 | 102 | 39 |
| Summer flu | 36 | 44 | 25 |
| Grand total | 202 | 293 | 139 |
| IgM | IgG | IgA | ||
|---|---|---|---|---|
| Reference tests * | RT-PCR positive with disease onset ≥19 days (n) | 26 | 26 | 26 |
| RT-PCR negative, pre-CoV-2019, & summer flu (n) | 102 | 148 | 66 | |
| Index test (SARSPLEX) | Positive immune response to RT-PCR positive (n) | 20 | 19 | 21 |
| Negative immune responses to RT-PCR negative, pre-CoV-2019, & summer flu (n) | 93 | 137 | 61 | |
| Performance analysis parameters | Positive agreement (%) | 78 | 73 | 81 |
| Negative agreement (%) | 91 | 93 | 92 | |
| Positive predictive value (%) | 69 | 63 | 81 | |
| Negative predictive value (%) | 94 | 95 | 92 | |
| False positive rate (%) | 9 | 7 | 8 | |
| False negative rate (%) | 23 | 27 | 19 | |
| Cohen’s Kappa (k) | 0.65 SUA | 0.61 SUA | 0.73 SUA |
| IgM | IgG | IgA | ||
|---|---|---|---|---|
| Reference tests * | Positive sera (n) | 13 | 66 | 23 |
| Negative sera (n) | 52 | 78 | 22 | |
| Index test (SARSPLEX) | Positive immune response to positive sera (n) | 10 | 61 | 15 |
| Negative immune responses negative sera (n) | 52 | 73 | 21 | |
| Performance analysis parameters | Positive agreement (%) | 77 | 93 | 65 |
| Negative agreement (%) | 100 | 94 | 95 | |
| Positive predictive value (%) | 100 | 91 | 94 | |
| Negative predictive value (%) | 95 | 94 | 72 | |
| False positive rate (%) | 0 | 8 | 5 | |
| False negative rate (%) | 23 | 8 | 35 | |
| Cohen’s Kappa (k) | 0.84 APA | 0.84 APA | 0.60 MOA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garg, K.; Campolonghi, S.; Schwarzbach, A.; Alonso, M.L.G.; Villavicencio-Aguilar, F.M.; Fajardo-Yamamoto, L.M.; Gilbert, L. SARSPLEX: Multiplex Serological ELISA with a Holistic Approach. Viruses 2022, 14, 2593. https://doi.org/10.3390/v14122593
Garg K, Campolonghi S, Schwarzbach A, Alonso MLG, Villavicencio-Aguilar FM, Fajardo-Yamamoto LM, Gilbert L. SARSPLEX: Multiplex Serological ELISA with a Holistic Approach. Viruses. 2022; 14(12):2593. https://doi.org/10.3390/v14122593
Chicago/Turabian StyleGarg, Kunal, Sara Campolonghi, Armin Schwarzbach, Maria Luisa Garcia Alonso, Fausto M. Villavicencio-Aguilar, Liria M. Fajardo-Yamamoto, and Leona Gilbert. 2022. "SARSPLEX: Multiplex Serological ELISA with a Holistic Approach" Viruses 14, no. 12: 2593. https://doi.org/10.3390/v14122593