

An Optimized Bioassay for Screening Combined Anticoronaviral Compounds for Efficacy against Feline Infectious Peritonitis Virus with Pharmacokinetic Analyses of GS-441524, Remdesivir, and Molnupiravir in Cats
 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. In Vitro Propagation of FIPV I and II
2.2. Determination of Antiviral Efficacy In Vitro
2.3. Single Dose Pharmacokinetics of Orally Administered MPV, GS-441524, and RDV and Intravenously Administered RDV
2.4. LCMSMS Quantitation of Serum MPV Concentrations and Pharmacokinetic Analysis
2.5. Mass Spectrometry and Liquid Chromatography Conditions
2.6. LC-MS/MS Quantification of GS-441524 in Plasma
2.7. Pharmacokinetic Analysis
3. Results
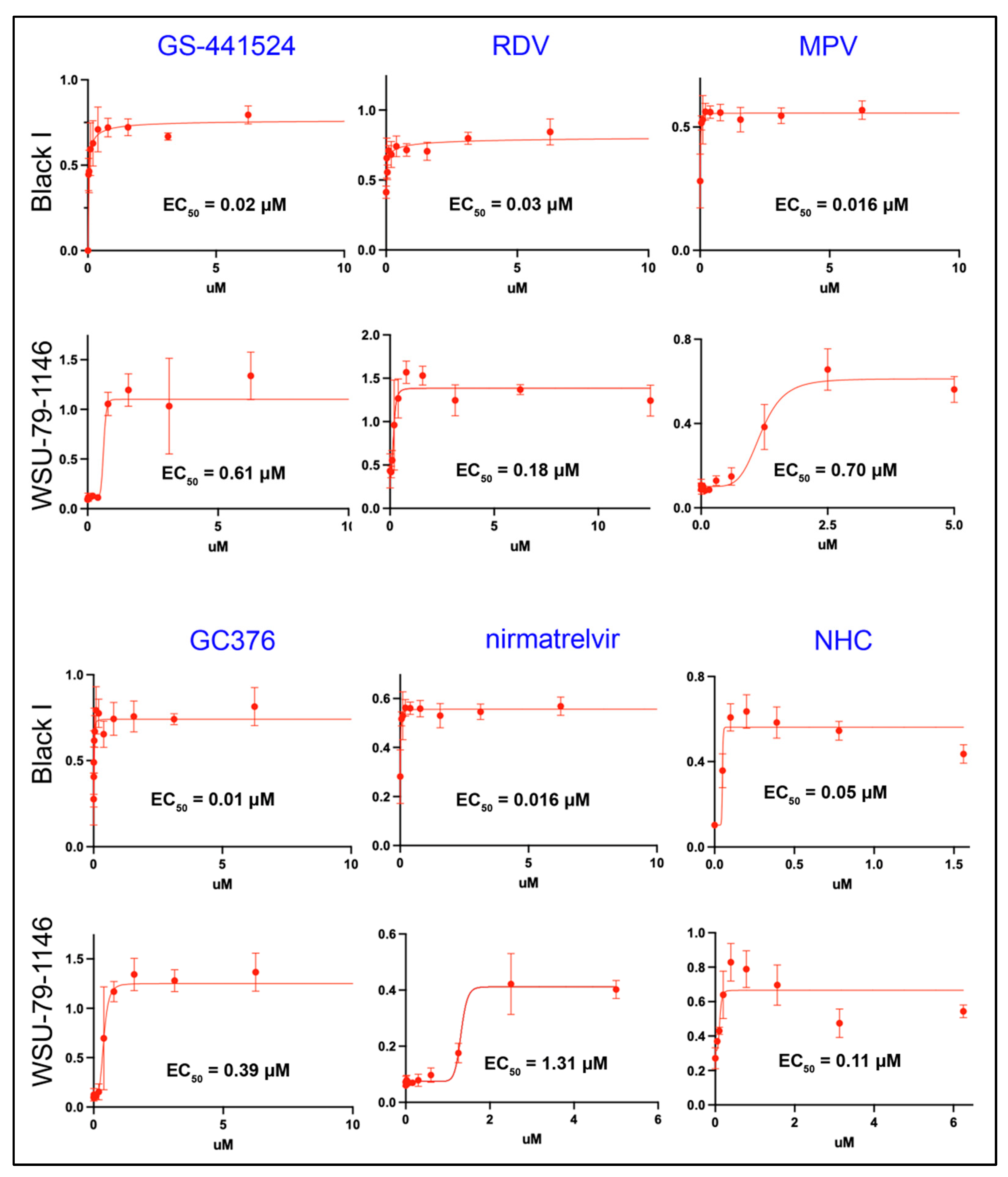
3.1. All of the Antiviral Agents Effectively Block the In Vitro Replication of Both Serotype I and II FIPV as Monotherapies
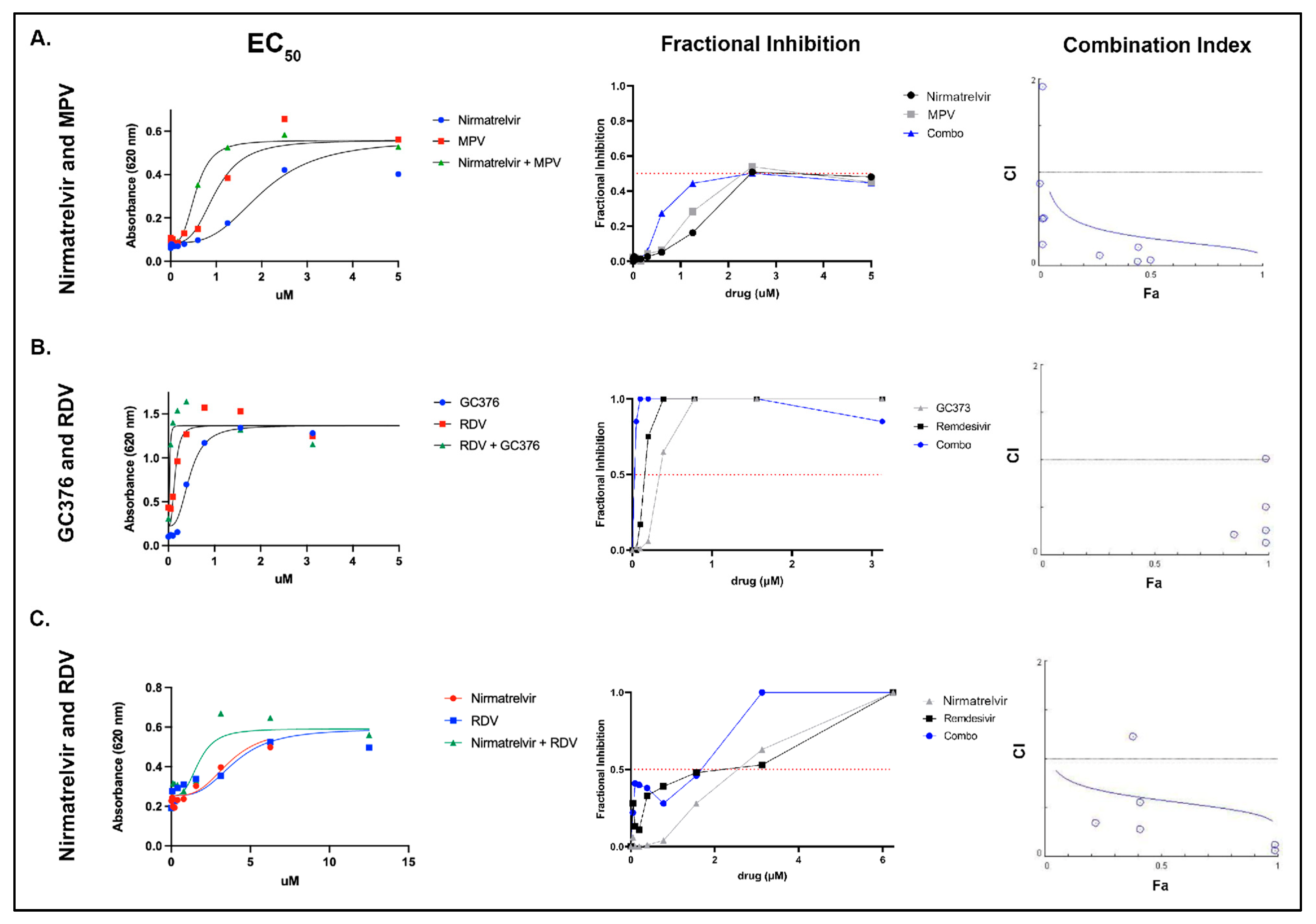
3.2. Select Antiviral Agents Have a Synergistic Effect When Used in Combination
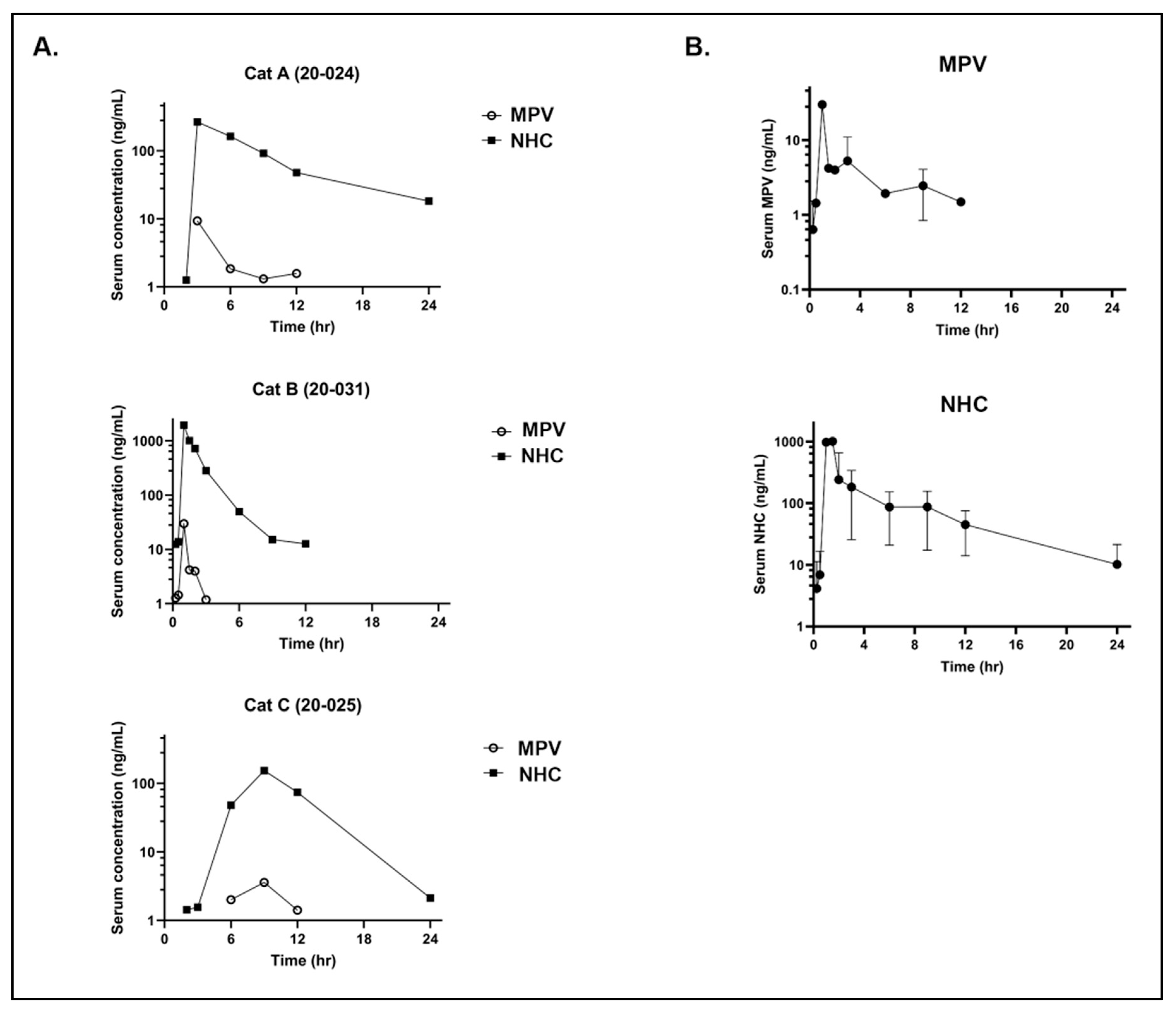
3.3. Pharmacokinetics of Oral MPV in Cats
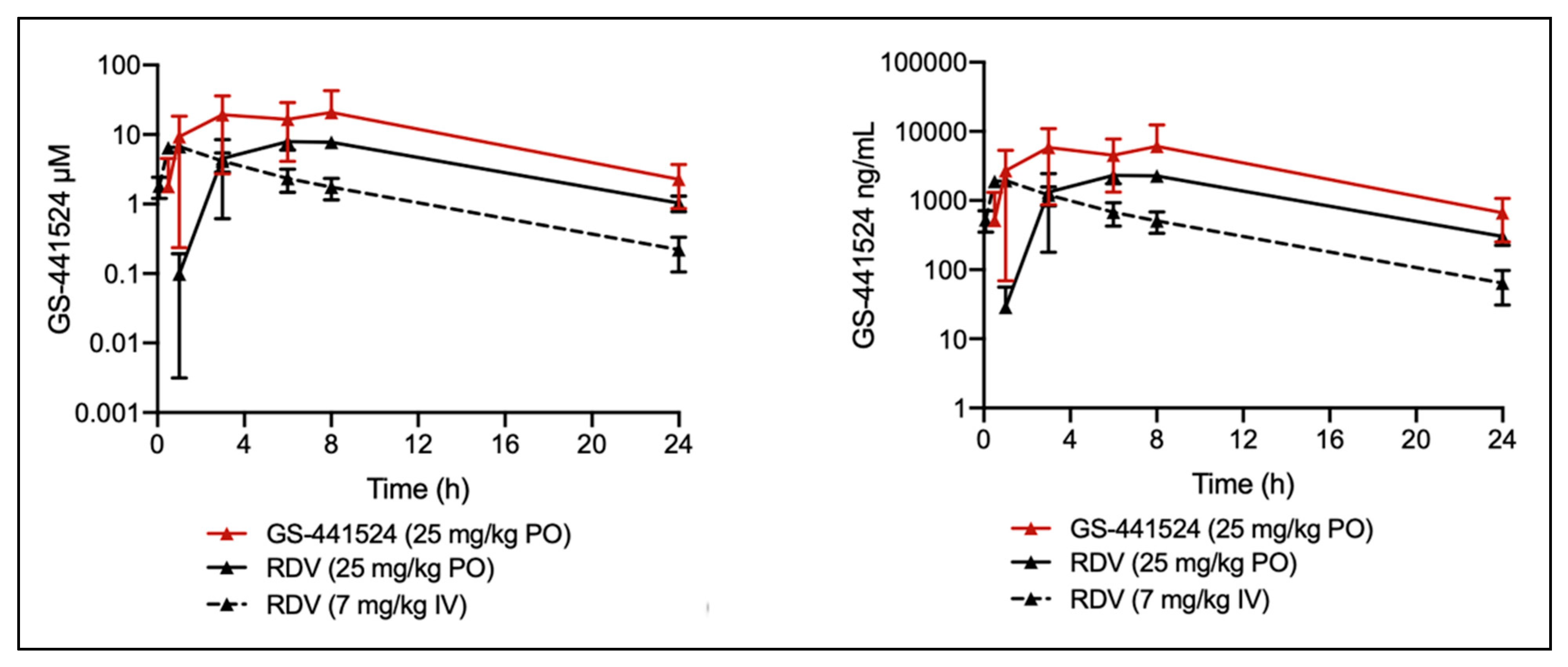
3.4. Pharmacokinetics of GS-441524 after Administration of GS-441524 or RDV in Cats
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pedersen, N.C.; Liu, H.; Dodd, K.A.; Pesavento, P.A. Significance of coronavirus mutants in feces and diseased tissues of cats suffering from feline infectious peritonitis. Viruses 2009, 1, 166–184. [Google Scholar] [CrossRef]
- Vennema, H.; Poland, A.; Foley, J.; Pedersen, N.C. Feline infectious peritonitis viruses arise by mutation from endemic feline enteric coronaviruses. Virology 1998, 243, 150–157. [Google Scholar] [CrossRef]
- Herrewegh, A.A.; Smeenk, I.; Horzinek, M.C.; Rottier, P.J.; De Groot, R.J. Feline coronavirus type II strains 79-1683 and 79-1146 originate from a double recombination between feline coronavirus type I and canine coronavirus. J. Virol. 1998, 72, 4508–4514. [Google Scholar] [CrossRef]
- Premkumar, L.; Segovia-Chumbez, B.; Jadi, R.; Martinez, D.R.; Raut, R.; Markmann, A.J.; Cornaby, C.; Bartelt, L.; Weiss, S.; Park, Y. The receptor-binding domain of the viral spike protein is an immunodominant and highly specific target of antibodies in SARS-CoV-2 patients. Sci. Immunol. 2020, 5, eabc8413. [Google Scholar] [CrossRef]
- Whittaker, G.R.; André, N.M.; Millet, J.K. Improving virus taxonomy by recontextualizing sequence-based classification with biologically relevant data: The case of the alphacoronavirus 1 species. MSphere 2018, 3, e00463-17. [Google Scholar] [CrossRef]
- Jaimes, J.A.; Millet, J.K.; Stout, A.E.; André, N.M.; Whittaker, G.R. A tale of two viruses: The distinct spike glycoproteins of feline coronaviruses. Viruses 2020, 12, 83. [Google Scholar] [CrossRef]
- Montali, R.; Strandberg, J. Extraperitoneal lesions in feline infectious peritonitis. Vet. Pathol. 1972, 9, 109–121. [Google Scholar] [CrossRef]
- Foley, J.E.; Lapointe, J.M.; Koblik, P.; Poland, A.; Pedersen, N.C. Diagnostic features of clinical neurologic feline infectious peritonitis. J. Vet. Intern. Med. 1998, 12, 415–423. [Google Scholar] [CrossRef]
- Jones, S.; Novicoff, W.; Nadeau, J.; Evans, S. Unlicensed GS-441524-like antiviral therapy can be effective for at-home treatment of feline infectious peritonitis. Animals 2021, 11, 2257. [Google Scholar] [CrossRef]
- Tsai, H.-Y.; Chueh, L.-L.; Lin, C.-N.; Su, B.-L. Clinicopathological findings and disease staging of feline infectious peritonitis: 51 cases from 2003 to 2009 in Taiwan. J. Feline Med. Surg. 2011, 13, 74–80. [Google Scholar] [CrossRef]
- Pedersen, N.C.; Kim, Y.; Liu, H.; Galasiti Kankanamalage, A.C.; Eckstrand, C.; Groutas, W.C.; Bannasch, M.; Meadows, J.M.; Chang, K.-O. Efficacy of a 3C-like protease inhibitor in treating various forms of acquired feline infectious peritonitis. J. Feline Med. Surg. 2018, 20, 378–392. [Google Scholar] [CrossRef] [PubMed]
- Perera, K.D.; Rathnayake, A.D.; Liu, H.; Pedersen, N.C.; Groutas, W.C.; Chang, K.-O.; Kim, Y. Characterization of amino acid substitutions in feline coronavirus 3C-like protease from a cat with feline infectious peritonitis treated with a protease inhibitor. Vet. Microbiol. 2019, 237, 108398. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, N.C.; Perron, M.; Bannasch, M.; Montgomery, E.; Murakami, E.; Liepnieks, M.; Liu, H. Efficacy and safety of the nucleoside analog GS-441524 for treatment of cats with naturally occurring feline infectious peritonitis. J. Feline Med. Surg. 2019, 21, 271–281. [Google Scholar] [CrossRef]
- Murphy, B.G.; Perron, M.; Murakami, E.; Bauer, K.; Park, Y.; Eckstrand, C.; Liepnieks, M.; Pedersen, N.C. The nucleoside analog GS-441524 strongly inhibits feline infectious peritonitis (FIP) virus in tissue culture and experimental cat infection studies. Vet. Microbiol. 2018, 219, 226–233. [Google Scholar] [CrossRef]
- Krentz, D.; Zenger, K.; Alberer, M.; Felten, S.; Bergmann, M.; Dorsch, R.; Matiasek, K.; Kolberg, L.; Hofmann-Lehmann, R.; Meli, M.L. Curing cats with feline infectious peritonitis with an oral multi-component drug containing GS-441524. Viruses 2021, 13, 2228. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.E.; Vogel, H.; Castillo, D.; Olsen, M.; Pedersen, N.; Murphy, B.G. Investigation of monotherapy and combined anticoronaviral therapies against feline coronavirus serotype II in vitro. J. Feline Med. Surg. 2021, 24, 1098612X2110486. [Google Scholar] [CrossRef]
- Kim, Y.; Liu, H.; Galasiti Kankanamalage, A.C.; Weerasekara, S.; Hua, D.H.; Groutas, W.C.; Chang, K.-O.; Pedersen, N.C. Reversal of the progression of fatal coronavirus infection in cats by a broad-spectrum coronavirus protease inhibitor. PLoS Pathog. 2016, 12, e1005531. [Google Scholar]
- Yan, S.; Wu, G. Potential 3-chymotrypsin-like cysteine protease cleavage sites in the coronavirus polyproteins pp1a and pp1ab and their possible relevance to COVID-19 vaccine and drug development. FASEB J. 2021, 35, e21573. [Google Scholar] [CrossRef]
- Weiss, S.R.; Hughes, S.A.; Bonilla, P.J.; Turner, J.D.; Leibowitz, J.L.; Denison, M.R. Coronavirus Polyprotein Processing; Springer: Vienna, Austria, 1994; pp. 349–358. [Google Scholar]
- Yin, Y.; Li, T.; Wang, C.; Liu, X.; Ouyang, H.; Ji, W.; Liu, J.; Liao, X.; Li, J.; Hu, C. A retrospective study of clinical and laboratory features and treatment on cats highly suspected of feline infectious peritonitis in Wuhan, China. Sci. Rep. 2021, 11, 5208. [Google Scholar] [CrossRef]
- Li, Y.; Cao, L.; Li, G.; Cong, F.; Li, Y.; Sun, J.; Luo, Y.; Chen, G.; Li, G.; Wang, P.; et al. Remdesivir Metabolite GS-441524 Effectively Inhibits SARS-CoV-2 Infection in Mouse Models. J. Med. Chem. 2022, 65, 2785–2793. [Google Scholar] [CrossRef]
- Yan, V.C.; Muller, F.L. Advantages of the parent nucleoside GS-441524 over remdesivir for COVID-19 treatment. ACS Med. Chem. Lett. 2020, 11, 1361–1366. [Google Scholar] [CrossRef] [PubMed]
- Agostini, M.L.; Andres, E.L.; Sims, A.C.; Graham, R.L.; Sheahan, T.P.; Lu, X.; Smith, E.C.; Case, J.B.; Feng, J.Y.; Jordan, R. Coronavirus susceptibility to the antiviral remdesivir (GS-5734) is mediated by the viral polymerase and the proofreading exoribonuclease. MBio 2018, 9, e00221-18. [Google Scholar] [CrossRef] [PubMed]
- Olender, S.A.; Perez, K.K.; Go, A.S.; Balani, B.; Price-Haywood, E.G.; Shah, N.S.; Wang, S.; Walunas, T.L.; Swaminathan, S.; Slim, J. Remdesivir for severe coronavirus disease 2019 (COVID-19) versus a cohort receiving standard of care. Clin. Infect. Dis. 2021, 73, e4166–e4174. [Google Scholar] [CrossRef] [PubMed]
- Sheahan, T.P.; Sims, A.C.; Leist, S.R.; Schäfer, A.; Won, J.; Brown, A.J.; Montgomery, S.A.; Hogg, A.; Babusis, D.; Clarke, M.O. Comparative therapeutic efficacy of remdesivir and combination lopinavir, ritonavir, and interferon beta against MERS-CoV. Nat. Commun. 2020, 11, 222. [Google Scholar] [CrossRef] [PubMed]
- De Wit, E.; Feldmann, F.; Cronin, J.; Jordan, R.; Okumura, A.; Thomas, T.; Scott, D.; Cihlar, T.; Feldmann, H. Prophylactic and therapeutic remdesivir (GS-5734) treatment in the rhesus macaque model of MERS-CoV infection. Proc. Natl. Acad. Sci. USA 2020, 117, 6771–6776. [Google Scholar] [CrossRef]
- Yethindra, V. Role of GS-5734 (Remdesivir) in inhibiting SARS-CoV and MERS-CoV: The expected role of GS-5734 (Remdesivir) in COVID-19 (2019-nCoV)-VYTR hypothesis. Int. J. Res. Pharm. Sci. 2020, 11, 1–6. [Google Scholar] [CrossRef]
- Bohm, M. Successful treatment of a South African cat with effusive feline infectious peritonitis with remdesivir. J. S. Afr. Vet. Assoc. 2022, 93, 1–4. [Google Scholar] [CrossRef]
- Lo, M.K.; Feldmann, F.; Gary, J.M.; Jordan, R.; Bannister, R.; Cronin, J.; Patel, N.R.; Klena, J.D.; Nichol, S.T.; Cihlar, T. Remdesivir (GS-5734) protects African green monkeys from Nipah virus challenge. Sci. Transl. Med. 2019, 11, eaau9242. [Google Scholar] [CrossRef]
- Lo, M.K.; Jordan, R.; Arvey, A.; Sudhamsu, J.; Shrivastava-Ranjan, P.; Hotard, A.L.; Flint, M.; McMullan, L.K.; Siegel, D.; Clarke, M.O. GS-5734 and its parent nucleoside analog inhibit Filo-, Pneumo-, and Paramyxoviruses. Sci. Rep. 2017, 7, 43395. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. FDA Approves First Treatment for COVID-19; FDA News Release: Silver Spring, MD, USA, 2020.
- Malik, R. Treatment of FIP in Cats with Subcutaneous Remdesivir Followed by Oral GS-441524 Tablets. 2022. Available online: https://www.zenbycat.org/blog/treatment-of-fip-in-cats-with-subcutaneous-remdesivir-followed-by-oral-gs-441524-tablets (accessed on 19 July 2022).
- U.S. Food and Drug Administration. Fact Sheet for Healthcare Providers: Emergency Use Authorization for Paxlovid. 2021. Available online: https://www.fda.gov/media/155050/download (accessed on 19 July 2022).
- Acosta, E.P. Pharmacokinetic enhancement of protease inhibitors. J. Acquir. Immune Defic. Syndr. 2002, 29, S11–S18. [Google Scholar] [CrossRef]
- Zeldin, R.K.; Petruschke, R.A. Pharmacological and therapeutic properties of ritonavir-boosted protease inhibitor therapy in HIV-infected patients. J. Antimicrob. Chemother. 2004, 53, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Wahl, A.; Gralinski, L.E.; Johnson, C.E.; Yao, W.; Kovarova, M.; Dinnon, K.H.; Liu, H.; Madden, V.J.; Krzystek, H.M.; De, C.; et al. SARS-CoV-2 infection is effectively treated and prevented by EIDD-2801. Nature 2021, 591, 451–457. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Library of Medicine. The Safety of Molnupiravir (EIDD-2801) and Its Effect on Viral Shedding of SARS-CoV-2 (END-COVID). Identifier NCT04405739. 28 May 2020–21 March 2022. Available online: https://clinicaltrials.gov/ct2/show/NCT04405739?id=NCT04405739&draw=2&rank=1&load=cart (accessed on 25 August 2022).
- Warriors, F. EIDD-2801. Available online: https://www.fipwarriors.eu/en/eidd-2801-molnupiravir/ (accessed on 19 July 2022).
- Sheahan, T.P.; Sims, A.C.; Zhou, S.; Graham, R.L.; Hill, C.S.; Leist, S.R.; Schäfer, A.; Dinnon, K.H.; Montgomery, S.A.; Agostini, M.L. An orally bioavailable broad-spectrum antiviral inhibits SARS-CoV-2 and multiple endemic, epidemic and bat coronavirus. Biorxiv 2020, 12, eabb5883. [Google Scholar]
- Dickinson, P.J.; Bannasch, M.; Thomasy, S.M.; Murthy, V.D.; Vernau, K.M.; Liepnieks, M.; Montgomery, E.; Knickelbein, K.E.; Murphy, B.; Pedersen, N.C. Antiviral treatment using the adenosine nucleoside analogue GS-441524 in cats with clinically diagnosed neurological feline infectious peritonitis. J. Vet. Intern. Med. 2020, 34, 1587–1593. [Google Scholar] [CrossRef] [PubMed]
- Lima, V.D.; Harrigan, R.; Bangsberg, D.R.; Hogg, R.S.; Gross, R.; Yip, B.; Montaner, J.S. The combined effect of modern highly active antiretroviral therapy regimens and adherence on mortality over time. J. Acquir. Immune Defic. Syndr. 2009, 50, 529. [Google Scholar] [CrossRef] [PubMed]
- Poordad, F.; Lawitz, E.; Kowdley, K.V.; Cohen, D.E.; Podsadecki, T.; Siggelkow, S.; Heckaman, M.; Larsen, L.; Menon, R.; Koev, G. Exploratory study of oral combination antiviral therapy for hepatitis C. N. Engl. J. Med. 2013, 368, 45–53. [Google Scholar] [CrossRef]
- Fabrizi, F.; Dixit, V.; Martin, P.; Messa, P. Combined antiviral therapy of hepatitis C virus in dialysis patients: Meta-analysis of clinical trials. J. Viral Hepat. 2011, 18, e263–e269. [Google Scholar] [CrossRef]
- O’Brien, A.; Mettelman, R.C.; Volk, A.; André, N.M.; Whittaker, G.R.; Baker, S.C. Characterizing replication kinetics and plaque production of type I feline infectious peritonitis virus in three feline cell lines. Virology 2018, 525, 1–9. [Google Scholar] [CrossRef]
- Cook, S.; Castillo, D.; Williams, S.; Haake, C.; Murphy, B. Serotype I and II Feline Coronavirus Replication and Gene Expression Patterns of Feline Cells—Building a Better Understanding of Serotype I FIPV Biology. Viruses 2022, 14, 1356. [Google Scholar] [CrossRef]
- Rathnayake, A.D.; Zheng, J.; Kim, Y.; Perera, K.D.; Mackin, S.; Meyerholz, D.K.; Kashipathy, M.M.; Bataile, K.P.; Lovell, S.; Perlman, S.; et al. 3C-like protease inhibitors block coronavirus replication in vitro and improve survival in MERS-CoV–infected mice. Sci. Transl. Med. 2020, 12, eabc5332. [Google Scholar] [CrossRef]
- Chou, T.-C. Drug Combination Studies and Their Synergy Quantification Using the Chou-Talalay MethodSynergy Quantification Method. Cancer Res. 2010, 70, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Warren, T.K.; Jordan, R.; Lo, M.K.; Ray, A.S.; Mackman, R.L.; Soloveva, V.; Siegel, D.; Perron, M.; Bannister, R.; Hui, H.C. Therapeutic efficacy of the small molecule GS-5734 against Ebola virus in rhesus monkeys. Nature 2016, 531, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Sheahan, T.P.; Sims, A.C.; Graham, R.L.; Menachery, V.D.; Gralinski, L.E.; Case, J.B.; Leist, S.R.; Pyrc, K.; Feng, J.Y.; Trantcheva, I. Broad-spectrum antiviral GS-5734 inhibits both epidemic and zoonotic coronaviruses. Sci. Transl. Med. 2017, 9, eaal3653. [Google Scholar] [CrossRef] [PubMed]
- Humeniuk, R.; Mathias, A.; Cao, H.; Osinusi, A.; Shen, G.; Chng, E.; Ling, J.; Vu, A.; German, P. Safety, tolerability, and pharmacokinetics of remdesivir, an antiviral for treatment of COVID-19, in healthy subjects. Clin. Transl. Sci. 2020, 13, 896–906. [Google Scholar] [CrossRef]
- Amara, A.; Penchala, S.D.; Else, L.; Hale, C.; FitzGerald, R.; Walker, L.; Lyons, R.; Fletcher, T.; Khoo, S. The development and validation of a novel LC-MS/MS method for the simultaneous quantification of Molnupiravir and its metabolite ß-d-N4-hydroxycytidine in human plasma and saliva. J. Pharm. Biomed. Anal. 2021, 206, 114356. [Google Scholar] [CrossRef]
- Vuong, W.; Khan, M.B.; Fischer, C.; Arutyunova, E.; Lamer, T.; Shields, J.; Saffran, H.A.; McKay, R.T.; Van Belkum, M.J.; Joyce, M.A.; et al. Feline coronavirus drug inhibits the main protease of SARS-CoV-2 and blocks virus replication. Nat. Commun. 2020, 11, 4282. [Google Scholar] [CrossRef]
- Sticher, Z.M.; Lu, G.; Mitchell, D.G.; Marlow, J.; Moellering, L.; Bluemling, G.R.; Guthrie, D.B.; Natchus, M.G.; Painter, G.R.; Kolykhalov, A.A. Analysis of the potential for N 4-hydroxycytidine to inhibit mitochondrial replication and function. Antimicrob. Agents Chemother. 2020, 64, e01719-19. [Google Scholar] [CrossRef]
- Xie, J.; Wang, Z. Can remdesivir and its parent nucleoside GS-441524 be potential oral drugs? An in vitro and in vivo DMPK assessment. Acta Pharm. Sin. B 2021, 11, 1607–1616. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Painter, W.P.; Holman, W.; Bush, J.A.; Almazedi, F.; Malik, H.; Eraut, N.C.; Morin, M.J.; Szewczyk, L.J.; Painter, G.R. Human safety, tolerability, and pharmacokinetics of molnupiravir, a novel broad-spectrum oral antiviral agent with activity against SARS-CoV-2. Antimicrob. Agents Chemother. 2021, 65, e02428-20. [Google Scholar] [CrossRef]
- O’Malley, K.; Crooks, J.; Duke, E.; Stevenson, I.H. Effect of Age and Sex on Human Drug Metabolism. BMJ 1971, 3, 607–609. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, S.D.; Testa, B. The Biochemistry of Drug Metabolism—An Introduction: Part 6. Inter-Individual Factors Affecting Drug Metabolism. Chem. Biodivers. 2008, 5, 2465–2578. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.M.; Faus, M.C.L.; Court, M.H. High interindividual variability in plasma clopidogrel active metabolite concentrations in healthy cats is associated with sex and cytochrome P450 2C genetic polymorphism. J. Vet. Pharmacol. Ther. 2019, 42, 16–25. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cat ID | Cmax (ng/mL; µM) | AUC (h*ng/mL) | Vz/F (L/kg) | Cl/F (L/h/kg) | MRT (h) |
|---|---|---|---|---|---|
| 20-024 | 9.3 (0.03) | 39.6 | 1101.7 | 209.0 | 4.4 |
| 20-025 | 3.6 (0.01) | 21.7 | 1229.4 | 381.8 | 8.1 |
| 20-031 | 29.8 (0.09) | 21.4 | 312.4 | 449.6 | 1.2 |
| Mean | 14.2 (0.04) | 27.5 | 881.1 | 346.8 | 4.6 |
| SD | 13.8 | 10.4 | 405.5 | 101.3 | 3.4 |
| Cat ID | Cmax (ng/mL; μM) | Tmax (h) | Kel (1/h) | T1/2 (h) | AUC (h*ng/mL) | MRT (h) |
|---|---|---|---|---|---|---|
| 20-024 | 265 (1.02) | 3.0 | 0.12 | 6 | 1709.47 | 8.33 |
| 20-025 | 154 (0.15) | 9.0 | 0.29 | 2.4 | 950.03 | 10.51 |
| 20-031 | 1950 (7.52) | 1.0 | 0.26 | 2.65 | 2679.57 | 2.46 |
| Mean | 790 (3.05) | 4.3 | 0.2 | 3.1 | 1779.7 | 7.1 |
| SD | 1006 | 4.2 | 0.1 | 1.2 | 866.9 | 4.2 |
| Cat ID | Cmax (ng/mL; μM) | Tmax (h) | T1/2 (h) | AUC (h*ng/mL) | F% * |
|---|---|---|---|---|---|
| 20-036 | 13,300 (45.66) | 8 | 4.5 | 132,232 | 235 |
| 20-044 | 9100 (31.24) | 3 | 8.8 | 54,756 | 100 |
| 20-046 | 8470 (29.08) | 3 | 5.6 | 82,135 | 145 |
| Mean | 10,290 (35.33) | 4.7 | 6.3 | 89,708 | 160 |
| SD | 2625 (9.01) | 2.9 | 2.2 | 39,028 | 69 |
| Cat ID | Cmax (ng/mL;μM) | Tmax (h) | T1/2 (h) | AUC (h*ng/mL) | F% * |
| 20-003 | 2100 (7.21) | 8 | 5.9 | 31,747 | 120 |
| 20-024 | 2390 (8.21) | 8 | 4.6 | 28,252 | 103 |
| 20-031 | 2950 (10.13) | 6 | 6.0 | 36,116 | 137 |
| Mean | 2480 (8.51) | 7.3 | 5.5 | 32,038 | 120 |
| SD | 432 (1.48) | 1.2 | 0.8 | 4077 | 17 |
| Cat ID | Cmax (ng/mL; μM) | Tmax (h) | T1/2 (h) | AUC (h*ng/mL) |
|---|---|---|---|---|
| 20-045 | 1730 (5.94) | 0.5 | 5.3 | 14,271 |
| 21-001 | 1960 (6.73) | 1 | 5.7 | 15,291 |
| 21-004 | 2320 (7.97) | 1 | 4.5 | 9924 |
| Mean | 2003 (6.88) | 0.83 | 5.2 | 13,162 |
| SD | 297 (1.0) | 0.29 | 0.6 | 2850 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cook, S.; Wittenburg, L.; Yan, V.C.; Theil, J.H.; Castillo, D.; Reagan, K.L.; Williams, S.; Pham, C.-D.; Li, C.; Muller, F.L.; et al. An Optimized Bioassay for Screening Combined Anticoronaviral Compounds for Efficacy against Feline Infectious Peritonitis Virus with Pharmacokinetic Analyses of GS-441524, Remdesivir, and Molnupiravir in Cats. Viruses 2022, 14, 2429. https://doi.org/10.3390/v14112429
Cook S, Wittenburg L, Yan VC, Theil JH, Castillo D, Reagan KL, Williams S, Pham C-D, Li C, Muller FL, et al. An Optimized Bioassay for Screening Combined Anticoronaviral Compounds for Efficacy against Feline Infectious Peritonitis Virus with Pharmacokinetic Analyses of GS-441524, Remdesivir, and Molnupiravir in Cats. Viruses. 2022; 14(11):2429. https://doi.org/10.3390/v14112429
Chicago/Turabian StyleCook, Sarah, Luke Wittenburg, Victoria C. Yan, Jacob H. Theil, Diego Castillo, Krystle L. Reagan, Sonyia Williams, Cong-Dat Pham, Chun Li, Florian L. Muller, and et al. 2022. "An Optimized Bioassay for Screening Combined Anticoronaviral Compounds for Efficacy against Feline Infectious Peritonitis Virus with Pharmacokinetic Analyses of GS-441524, Remdesivir, and Molnupiravir in Cats" Viruses 14, no. 11: 2429. https://doi.org/10.3390/v14112429