
The Alpha Variant (B.1.1.7) of SARS-CoV-2 in Children: First Experience from 3544 Nucleic Acid Amplification Tests in a Cohort of Children in Germany

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
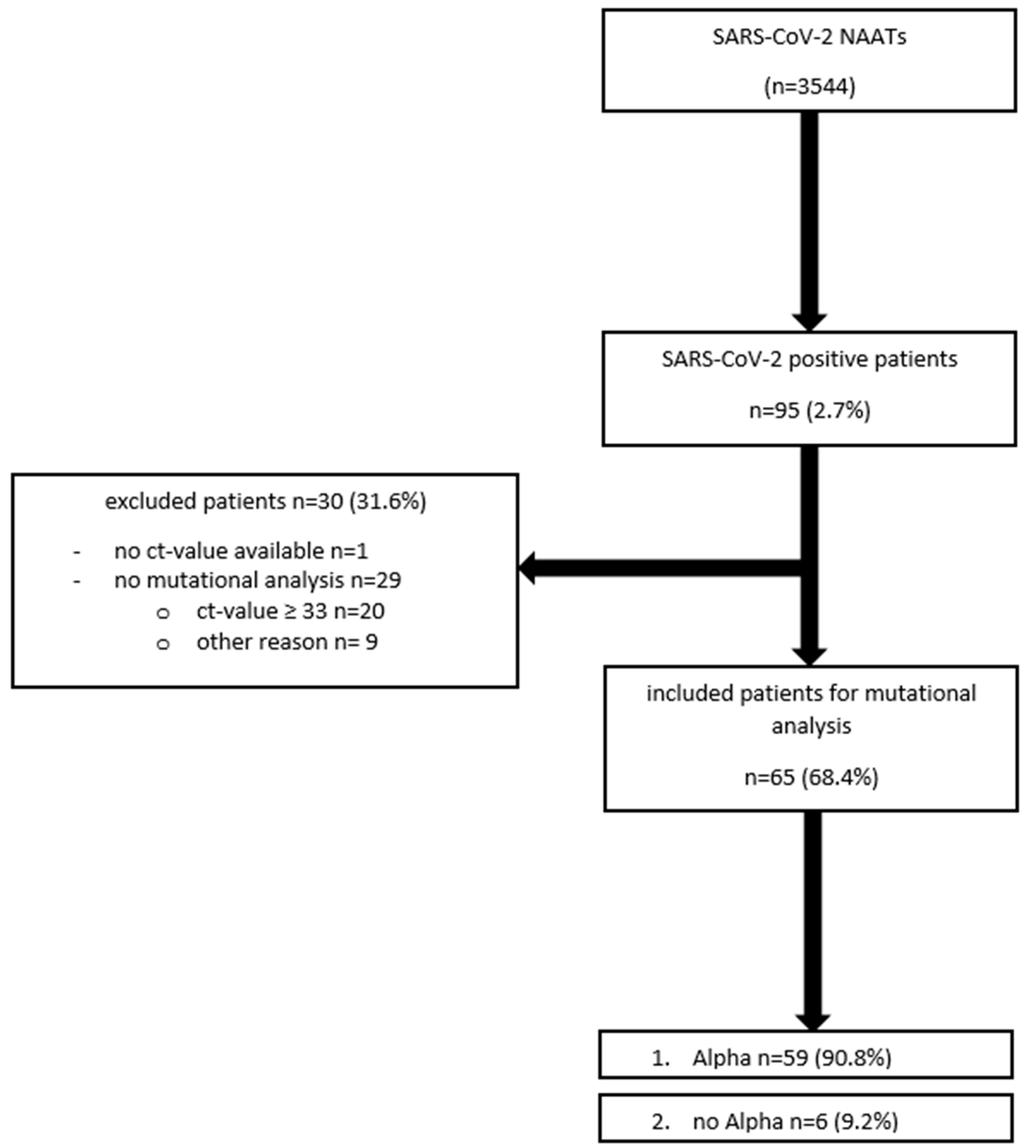
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---8-june-2021 (accessed on 10 June 2021).
- Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Jun_2021/2021-06-03-en.pdf?__blob=publicationFile (accessed on 10 June 2021).
- Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Daten/Altersverteilung.html (accessed on 10 June 2021).
- Lu, X.; Zhang, L.; Du, H. SARS-CoV-2 Infection in Children. N. Engl. J. Med. 2020, 382, 1663–1665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: https://dgpi.de/stellungnahme-dgpi-dgkh-hospitalisierung-und-sterblichkeit-von-covid-19-bei-kindern-in-deutschland-18-04-2021/ (accessed on 10 June 2021).
- Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Dez_2020/2020-12-26-en.pdf?__blob=publicationFile (accessed on 10 June 2021).
- Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/DESH/Bericht_VOC_2021-05-19.pdf?__blob=publicationFile (accessed on 10 June 2021).
- Davies, N.G.; Abbott, S.; Barnard, R.C. Estimated transmissibility and impact of SARS-CoV-2lineage B.1.1.7 in England. Science 2021, 372, eabg3055. [Google Scholar] [CrossRef] [PubMed]
- Brookman, S.; Cook, J.; Zucherman, M. Effect of the new SARS-CoV-2-variant B.1.1.7 on children and young people. Lancet Child. Adolesc. Health 2021, 5, e9–e10. [Google Scholar] [CrossRef]
- Meyer, M.; Rübsteck, E.; Lehmann, C. Prävalenz von SARS-CoV-2 bei Kindern in einer Kohorte von 2192 Patienten [Prevalence of SARS-CoV-2 in children from a cohort of 2192 patients]. Monatsschr Kinderheilkd. 2020, 1–6, Epub ahead of print. [Google Scholar] [CrossRef]
- Mithal, L.B.; Machut, K.Z.; Muller, W.J. SARS-CoV-2 Infection in Infants Less than 90 Days Old. J. Pediatr. 2020, 224, 150–152. [Google Scholar] [CrossRef] [PubMed]
- Frampton, D.; Rampling, T.; Cross, A. Genomic characteristics and clinical effect of the emergent SARS-CoV-2 B.1.1.7 lineage in London, UK: A whole-genome sequencing and hospital-based cohort study. Lancet Infect. Dis. 2007, 107, 2411–2502. [Google Scholar] [CrossRef]
- Calistri, P.; Amato, L.; Puglia, I. Infection sustained by lineage B.1.1.7 of SARS-CoV-2 is characterised by longer persistence and higher viral RNA loads in nasopharyngeal swabs. Infect. Dis. 2021, 105, 753–755. [Google Scholar] [CrossRef]
- Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Vorl_Testung_nCoV.html;jsessionid=853B1402519672CAB4993152D320FD65.internet111?nn=13490888#doc13490982bodyText4 (accessed on 10 June 2021).
- Jones, T.C.; Biele, G.; Mühlemann, B. Estimating infectiousness throughout SARS-CoV-2 infection course. Science 2021, 373, eabi5273. [Google Scholar] [CrossRef] [PubMed]
- Golubchik, T.; Lythgoe, K.A.; Hall, M. Early Analysis of a Potential Link between Viral Load and the N501Y Mutation in the SARS-COV-2 Spike Protein. 2020. Available online: https://www.coronavirus-fraser-group.org/files/files/updated_report_to_nervtag_oxford_20201222.pdf (accessed on 10 June 2021).
- Bager, P.; Wohlfahrt, J.; Fonager, J. Increased risk of hospitalisation associated with infection with SARS-CoV-2 lineage B.1.1.7 in Denmark. Lancet Infect Dis. 2021. Epub ahead of print. [Google Scholar] [CrossRef]
- Davies, N.G.; Jarvis, C.I.; Edmunds, W.J. Increased mortality in community-tested cases of SARS-CoV-2 lineage B.1.1.7. Nature 2021, 593, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Grint, D.J.; Wing, K.; Williamson, E. Case fatality risk of the SARS-CoV-2 variant of concern B.1.1.7 in England, 16 November to 5 February. Euro Surveill. 2021, 26, 2100256. [Google Scholar] [CrossRef] [PubMed]
- Graham, M.S.; Sudre, C.H.; May, A. Changes in symptomatology, reinfection, and transmissibility associated with the SARS-CoV-2 variant B.1.1.7: An ecological study. Lancet Public Health. 2021, 6, e335–e345. [Google Scholar] [CrossRef]
- Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/coronaviruscovid19infectionsinthecommunityinengland/characteristicsofpeopletestingpositiveforcovid19inengland27january2021 (accessed on 23 June 2021).
- Swann, O.V.; Holden, K.A.; Turtle, L. Clinical characteristics of children and young people admitted to hospital with COVID-19 in United Kingdom: Prospective multicentre observational cohort study. BMJ 2020, 37, m3249. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.lzg.nrw.de/covid19/covid19_mags.html?RegionCases7DaysRelative#:~:text=Die%20aktuelle%207%2DTage%2DInzidenz,19%2DF%C3%A4lle%20pro%20100.000%20Einwohner (accessed on 23 June 2021).
- Rankin, D.A.; Talj, R.; Howard, L.M. Epidemiological trends and characteristics of SARS-CoV-2 infections among children in the United States. Curr. Opin. Pediatr. 2021, 33, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Meyer, M.; Ruebsteck, E.; Gruell, H. COVID-19 study found that 0.4% of 5730 asymptomatic children aged 0–18 years tested positive for virus before hospital procedures or admission. Acta Paediatr. 2021, 110, 2584–2585. [Google Scholar] [CrossRef] [PubMed]
- Volz, E.; Msihra, S.; Chand, M. Assessing transmissibility of SARS-CoV-2 lineage B.1.1.7 in England. Nature. 2021, 593, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Jentsch, B.; Schnock, B. Kinder im Blick? Kindeswohl in Zeiten von Corona. Soz. Extra. 2020, 44, 304–309. [Google Scholar] [CrossRef]
- Ghosh, R.; Dubey, M.J.; Chatterjee, S. Impact of COVID -19 on children: Special focus on the psychosocial aspect. Minerva Pediatr. 2020, 72, 226–235. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | SARS-CoV-2 NAATs (n = 3544) |
|---|---|
| Age (median) | 5.1 years |
| (min 0 years; max 17.9) | |
| Gender (male) | 53.5% (n = 1897) |
| SARS-CoV-2-Positive NAATs | 2.7% (n = 95) |
| Admission to Hospital | 27.5% (n = 976) |
| Underlying Chronic Disease | 41.8% (n = 1480) |
| Contact to Somebody Recently Tested Positive for SARS-CoV-2 | 5.6% (n = 199) |
| Symptomatic | 19.8% (n = 703) |
| Mortality | 0.0% (n = 0) |
| Variable | Negative SARS-CoV-2 NAATs (n = 3449) | Positive SARS-CoV-2 NAATs (n = 95) | p-Value |
|---|---|---|---|
| Age (median) | 5.0 years | 9.3 years | p < 0.0001 |
| (min 0.0 years; max 17.0 years) | (min 0.0 years; max 17.8 years) | ||
| 0 ≤ 3 years | 37.2% (n = 1284) | 21.1% (n = 20) | p = 0.0011 |
| 3 ≤ 6 years | 19.2% (n = 663) | 10.5% (n = 10) | p = 0.0333 |
| 6 ≤ 12 years | 20.4% (n = 705) | 31.6% (n = 30) | p = 0.0014 |
| 12 ≤ 18 years | 23.1% (n = 797) | 36.8% (n = 35) | p = 0.0030 |
| Gender (male) | 53.6% (n = 1848) | 51.6% (n = 46) | p = 0.3486 |
| SARS-CoV-2-Positive NAATs | - | 100.0% (n = 95) | - |
| Suffering from a | 42.6% (n = 1470) | 10.5% (n = 10) | p < 0.0001 |
| Chronic Disease | |||
| Contact to Somebody Recently Tested Positive for SARS-CoV-2 | 4.6% (n = 160) | 41.1% (n = 39) | p < 0.0001 |
| Symptomatic | 18.8% (n = 650) | 55.8% (n = 53) | p < 0.0001 |
| Fever | 0.0% (n = 0) | 28.4% (n = 27) | p < 0.0001 |
| Cough | 5.9% (n = 203) | 27.4% (n = 26) | p < 0.0001 |
| Rhinitis | 6.1% (n = 210) | 25.3% (n = 24) | p < 0.0001 |
| Headache | 2.9% (n = 100) | 9.5% (n = 9) | p = 0.0023 |
| Dyspnea | 1.3% (n = 46) | 4.2% (n = 4) | p = 0.0436 |
| Sore Throat | 2.6% (n = 88) | 4.2% (n = 4) | p = 0.3115 |
| Gastrointestinal Symptoms | 4.1% (n = 142) | 8.4% (n = 8) | p = 0.0617 |
| Myalgia | 0.2% (n = 7) | 3.2% (n = 3) | p = 0.0020 |
| Dysgeusia and Dysosmia | 0.2% (n = 6) | 7.4% (n = 7) | p < 0.0001 |
| Admission to Hospital | 27.7% (n = 955) | 22.1% (n = 21) | p = 0.2464 |
| Ct Value (median) | - | 26.0 (min 17.0; max 41.0) | - |
| Variant Analysis | - | 68.4% (n = 65) | - |
| Wild Type | - | 4.2% (n = 4) | - |
| Alpha Mutation Pattern | - | 90.8% (n = 59) | - |
| Alpha Mutation Pattern with Escape Mutation | - | 1.5% (n = 1) | |
| Beta Mutation Pattern | 1.5% (n = 1) | - |
| Variable | Alpha Variant (n = 59) | No Alpha Variant (n = 6) | p-Value |
|---|---|---|---|
| Age (median) | 8.6 years | 14.0 years | p = 0.0953 |
| (min 0.0 years; max 17.8 years) | (min 7.1 years; max 16.3 years) | ||
| 0 ≤ 3 years | 20.3% (n = 12) | 0% (n = 0) | p = 0.5831 |
| 3 ≤ 6 years | 13.6% (n = 8) | 0% (n = 0) | p > 0.9999 |
| 6 ≤ 12 years | 37.3% (n = 22) | 44.4% (n = 2) | p > 0.9999 |
| 12 ≤ 18 years | 28.8% (n = 17) | 66.6% (n = 4) | p = 0.0800 |
| Gender (male) | 55.9% (n = 33) | 44.4% (n = 2) | p = 0.4025 |
| Suffering from a | 3.4% (n = 2) | 0% (n = 0) | p > 0.9999 |
| Chronic Disease | |||
| Contact to Somebody Recently Tested Positive for SARS-CoV-2 | 45.8% (n = 27) | 16.7% (n = 1) | p = 0.2245 |
| Symptomatic | 54.2% (n = 32) | 66.6% (n = 4) | p = 0.6841 |
| Fever | 25.7% (n = 15) | 0.0% (n = 0) | p = 0.3225 |
| Cough | 23.7% (n = 14) | 44.4% (n = 2) | p = 0.6306 |
| Rhinitis | 23.7% (n = 14) | 44.4% (n = 2) | p = 0.6306 |
| Headache | 11.9% (n = 7) | 2.9% (n = 1) | p = 0.5607 |
| Dyspnea | 8.5% (n = 5) | 0.0% (n = 0) | p > 0.9999 |
| Sore Throat | 6.8% (n = 4) | 44.4% (n = 2) | p = 0.0908 |
| Gastrointestinal Symptoms | 6.8% (n = 4) | 0.0% (n = 0) | p > 0.9999 |
| Myalgia | 5.1% (n = 3) | 0.0% (n = 0) | p > 0.9999 |
| Dysgeusia and Dysosmia | 1.7% (n = 1) | 16.7% (n = 1) | p > 0.9999 |
| Admission to Hospital | 20.3% (n = 12) | 0.0% (n = 0) | p = 0.5831 |
| for COVID-19 | 15.3% (n = 9) | 0.0% (n = 0) | p = 0.5838 |
| Ct Value (median) | 24.0 (min 17.0; max 32.7) | 25.0 (min 19.0; max 32.0) | p = 0.3886 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meyer, M.; Holfter, A.; Ruebsteck, E.; Gruell, H.; Dewald, F.; Koerner, R.W.; Klein, F.; Lehmann, C.; Huenseler, C.; Weber, L.T. The Alpha Variant (B.1.1.7) of SARS-CoV-2 in Children: First Experience from 3544 Nucleic Acid Amplification Tests in a Cohort of Children in Germany. Viruses 2021, 13, 1600. https://doi.org/10.3390/v13081600
Meyer M, Holfter A, Ruebsteck E, Gruell H, Dewald F, Koerner RW, Klein F, Lehmann C, Huenseler C, Weber LT. The Alpha Variant (B.1.1.7) of SARS-CoV-2 in Children: First Experience from 3544 Nucleic Acid Amplification Tests in a Cohort of Children in Germany. Viruses. 2021; 13(8):1600. https://doi.org/10.3390/v13081600
Chicago/Turabian StyleMeyer, Meike, Anna Holfter, Esra Ruebsteck, Henning Gruell, Felix Dewald, Robert Walter Koerner, Florian Klein, Clara Lehmann, Christoph Huenseler, and Lutz Thorsten Weber. 2021. "The Alpha Variant (B.1.1.7) of SARS-CoV-2 in Children: First Experience from 3544 Nucleic Acid Amplification Tests in a Cohort of Children in Germany" Viruses 13, no. 8: 1600. https://doi.org/10.3390/v13081600