
Temporal and Spatial Epidemiological Analysis of Peste Des Petits Ruminants Outbreaks from the Past 25 Years in Sheep and Goats and Its Control in India

 ,
,  ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
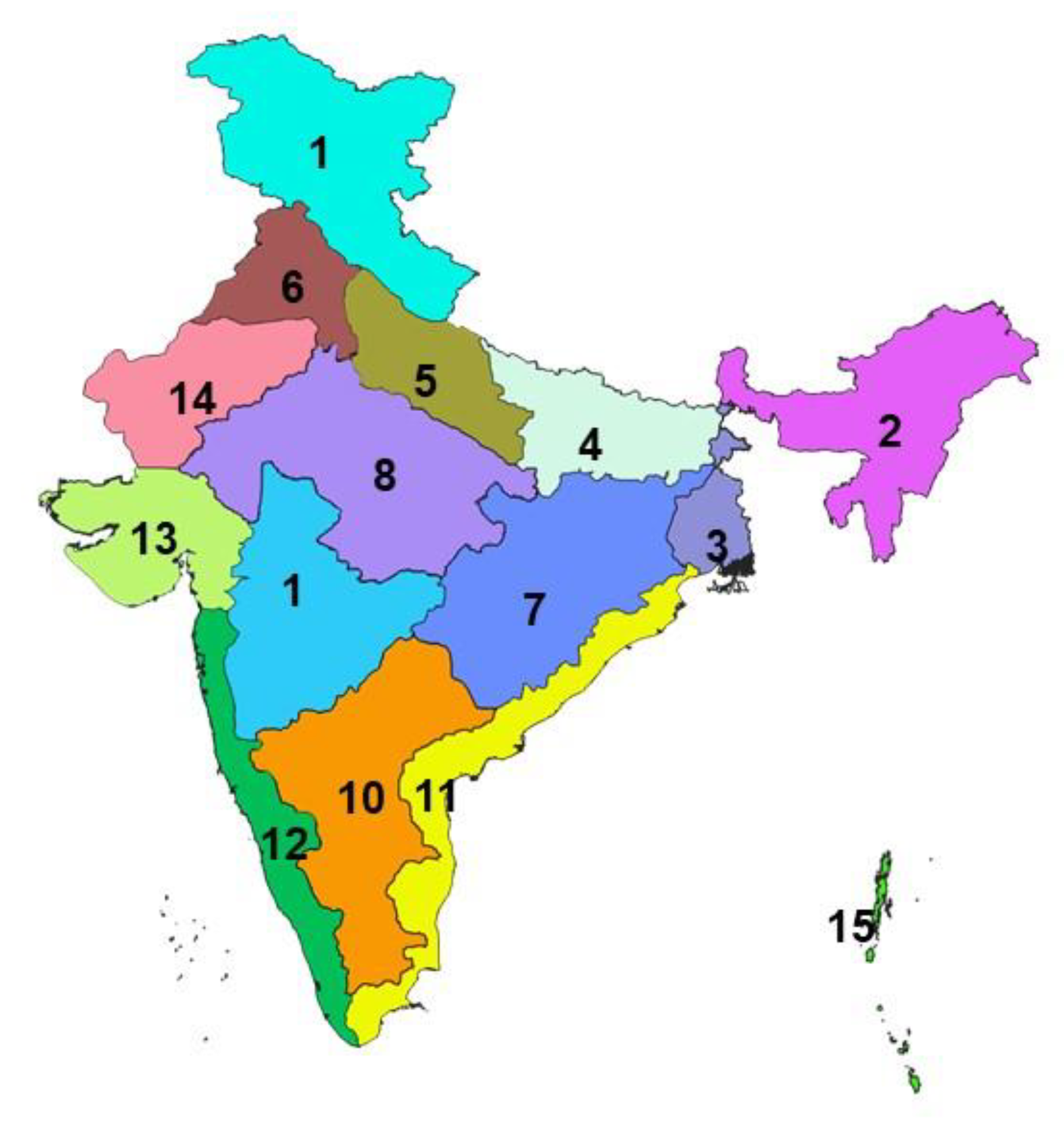
2.1. Study Area Description
2.2. Data Source
2.3. Data Analysis
3. Results
3.1. Disease Burden
3.2. Temporal Patterns
3.3. Species Susceptibility
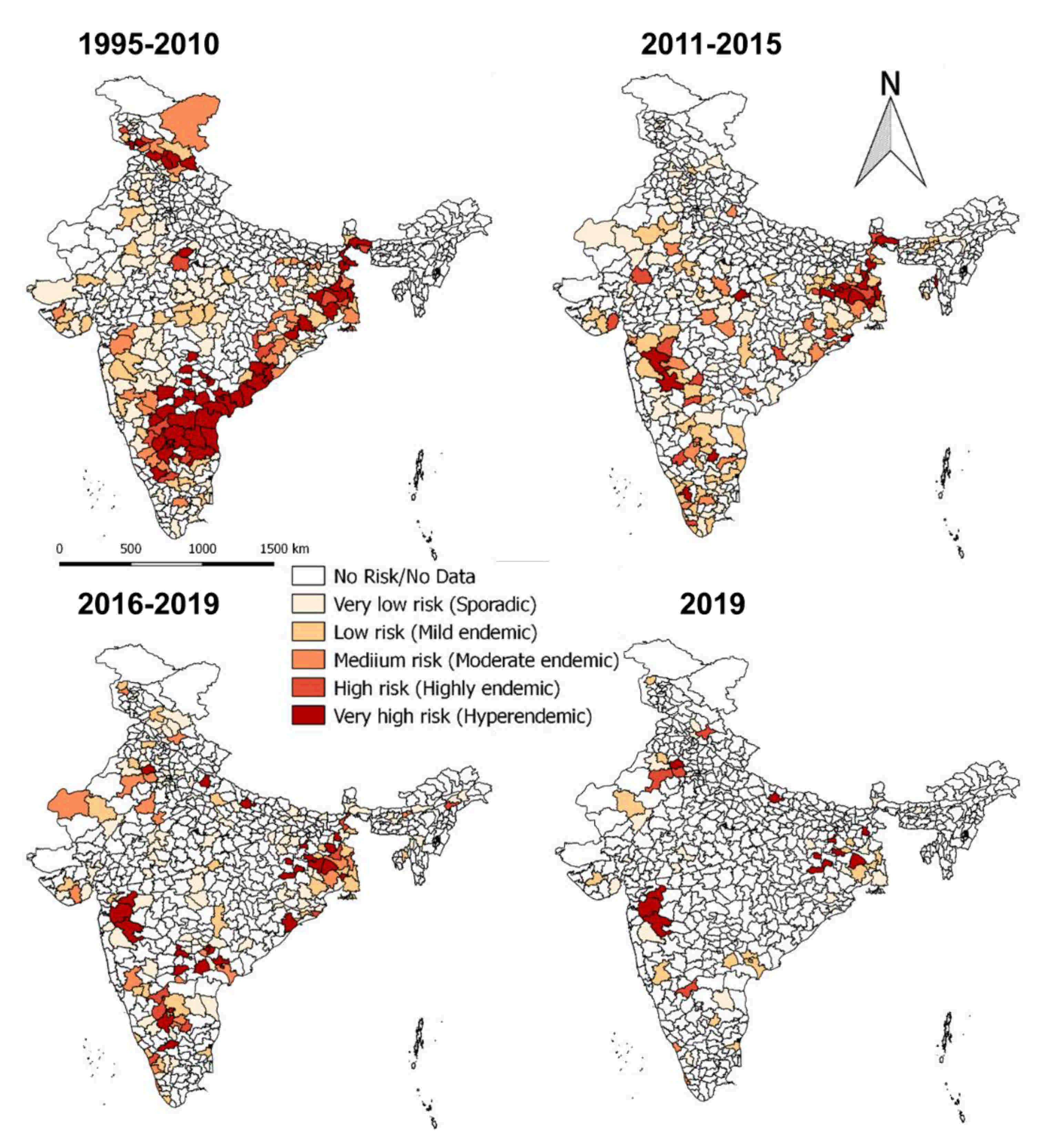
3.4. Spatial Distribution
3.5. Effect of Vaccination
3.6. Case Studies of the States
4. Discussion
4.1. Epidemiological Analysis
4.2. PPR Control Program
4.2.1. Vaccination
4.2.2. Seromonitoring and Surveillance
4.2.3. National Strategic Plan for PPR Eradication
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data availability statement
Acknowledgments
Conflicts of Interest
References
- ICTV Morbillivirus. International Committee on Taxonomy of Viruses (ICTV). Available online: https://talk.ictvonline.org/ictv-reports/ictv_online_report/negative-sense-rna-viruses/w/paramyxoviridae/1183/genus-morbillivirus (accessed on 21 December 2020).
- Balamurugan, V.; Hemadri, D.; Gajendragad, M.R.; Singh, R.K.; Rahman, H. Diagnosis and control of peste des petits ruminants: A comprehensive review. Virusdisease 2014, 25, 39–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- FAO Supporting Livelihoods and Building Resilience through Peste des Petits Ruminants (PPR) and Small Ruminant Diseases Control. Available online: http://www.fao.org/ppr/en/ (accessed on 21 December 2020).
- Albina, E.; Kwiatek, O.; Minet, C.; Lancelot, R.; Servan de Almeida, R.; Libeau, G. Peste des Petits Ruminants, the next eradicated animal disease? Vet. Microbiol. 2013, 165, 38–44. [Google Scholar] [CrossRef]
- Baron, M.D.; Diallo, A.; Lancelot, R.; Libeau, G. Peste des Petits Ruminants Virus. Adv. Virus Res. 2016, 95, 1–42. [Google Scholar]
- Kamel, M.; El-Sayed, A. Toward peste des petits virus (PPRV) eradication: Diagnostic approaches, novel vaccines, and control strategies. Virus Res. 2019, 274, 197774. [Google Scholar] [CrossRef] [PubMed]
- OIE. FAO Manual on Global Strategy for the Control and Eradication of Pesti des Petits Ruminants. 2015. Available online: http://www.fao.org/3/a-i4460e.pdf (accessed on 21 December 2020).
- DAHD 20th Livestock Census 2019-All India Report; Department of Animal Husbandry and Dairying: New Delhi, India, 2020; pp. 71–79. Available online: https://dadf.gov.in/sites/default/filess/20th%20Livestock%20census-2019%20All%20India%20Report.pdf (accessed on 21 December 2020).
- Shaila, M.S.; Purushothaman, V.; Bhavasar, D.; Venugopal, K.; Venkatesan, R.A. Peste des petits ruminants of sheep in India. Vet. Rec. 1989, 125, 602. [Google Scholar] [PubMed]
- Kulkarni, D.D.; Bhikane, A.U.; Shaila, M.S.; Varalakshmi, P.; Apte, M.P.; Narladkar, B.W. Peste des petits ruminants in goats in India. Vet. Rec. 1996, 138, 187–188. [Google Scholar] [CrossRef]
- Singh, R.K.; Balamurugan, V.; Bhanuprakash, V.; Sen, A.; Saravanan, P.; Pal Yadav, M. Possible control and eradication of peste des petits ruminants from India: Technical aspects. Vet. Ital. 2009, 45, 449–462. [Google Scholar] [PubMed]
- Singh, R.P.; Saravanan, P.; Sreenivasa, B.P.; Singh, R.K.; Bandyopadhyay, S.K. Prevalence and distribution of peste des petits ruminants virus infection in small ruminants in India. Rev. Sci. Tech. 2004, 23, 807–819. [Google Scholar] [CrossRef]
- DAHD Peste des Petits Ruminants Control Programme (PPR-CP). Available online: https://dahd.nic.in/about-us/divisions/livestock-health (accessed on 21 December 2020).
- Balamurugan, V.; Govindaraj, G.N.; Rahman, H. Planning, implementation of peste des petits ruminants control programme and strategies adopted for disease control in India. Br. J. Virol. 2016, 3, 53–62. [Google Scholar] [CrossRef]
- Balamurugan, V.; Saravanan, P.; Sen, A.; Rajak, K.K.; Venkatesan, G.; Krishnamoorthy, P.; Bhanuprakash, V.; Singh, R.K. Prevalence of peste des petits ruminants among sheep and goats in India. J. Vet. Sci. 2012, 13, 279–285. [Google Scholar] [CrossRef] [Green Version]
- Balamurugan, V.; Saravanan, P.; Sen, A.; Rajak, K.K.; Bhanuprakash, V.; Krishnamoorthy, P.; Singh, R.K. Sero-epidemiological study of peste des petits ruminants in sheep and goats in India between 2003 and 2009. Rev. Sci. Tech. 2011, 30, 889–896. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.P.; Sreenivasa, B.P.; Dhar, P.; Shah, L.C.; Bandyopadhyay, S.K. Development of a monoclonal antibody based competitive-ELISA for detection and titration of antibodies to peste des petits ruminants (PPR) virus. Vet. Microbiol. 2004, 98, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Balamurugan, V.; Varghese, B.; Kumar Vinod, K.; Muthuchelvan, D.; Dheeraj, R.; Govindaraj, G.; Suresh, K.P.; Hemadri, D.; Roy, P. Seroprevalence study of peste des petits ruminants in sheep and goats in the northern region of India. Vet. World 2020, 13, 1573–1580. [Google Scholar] [CrossRef] [PubMed]
- Balamurugan, V.; Varghese, B.; Muthuchelvan, D.; Kumar, K.V.; Govindaraj, G.; Suresh, K.P.; Kumar, P.; Hemadri, D.; Roy, P. Seroprevalence of peste des petits ruminants in sheep and goats in Eastern India. Virusdisease 2020, 31, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Balamurugan, V.; Varghese, B.; Muthuchelvan, D.; SowjanyaKumari, S.; Vinod Kumar, K.; Dheeraj, R.; Govindaraj, G.; Suresh, K.P.; Hemadri, D.; Roy, P. Towards eradication of Peste des petits ruminants: Post-vaccination evaluation in sheep and goats in Southern Peninsular India. Virusdisease 2020, 31, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Balamurugan, V.; Varghese, B.; Muthuchelvan, D.; SowjanyaKumari, S.; Vinod Kumar, K.; Dheeraj, R.; Govindaraj, G.; Suresh, K.P.; Hemadri, D.; Roy, P. Seroprevalence of Peste des petits ruminants in small ruminants in the North Eastern Region of India. Vet. Ital. 2020, 56, 55–60. [Google Scholar]
- Dash, S. Contribution of livestock sector to Indian economy. Paripex-Indian J. Res. 2017, 6, 890–891. [Google Scholar]
- Chakraborty, T.; Gupta, A. Loan Repayment Behaviour of Farmers: Analysing Indian Households; Indian Institute of Technology: Kanpur, India, 2017; Available online: http://home.iitk.ac.in/~tanika/files/research/BorrowingBehaviorAT.pdf (accessed on 21 December 2020).
- MeitY Agro Climatic Zones in India. Available online: https://vikaspedia.in/agriculture/crop-production/weather-information/agro-climatic-zones-in-inida (accessed on 24 August 2020).
- ICAR-NIVEDI National Animal Disease Referral Expert System (NADRES) of ICAR-NIVEDI. Available online: https://nivedi.res.in/Nadres_v2/ (accessed on 21 December 2020).
- Sudharshana, K.J.; Rajasekhar, M.; Upadhye, A.S. Prevalence of peste des petits ruminants and rinderpest antibodies in small ruminants. Indian Vet. J. 1995, 72, 1246–1250. [Google Scholar]
- Narayanaswamy, M.; Ramani, K. Preliminary studies on rinderpest virus isolated from outbreaks in sheep in Mysore State. Indian Vet. J. 1973, 50, 829–832. [Google Scholar]
- Singh, R.P. Control strategies for peste des petits ruminants in small ruminants of India. Rev. Sci. Tech. 2011, 30, 879–887. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.P.; Bandyopadhyay, S.K. Peste des petits ruminants vaccine and vaccination in India: Sharing experience with disease endemic countries. Virusdisease 2015, 26, 215–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venkataramanan, R.; Bandyopadhyay, S.K.; Oberoi, M.S. Present status and strategies for the control of transboundary and other economically important animal diseases in India: A review. Indian J. Anim. Sci. 2005, 75, 456–464. [Google Scholar]
- Singh, R.P.; Sreenivasa, B.P.; Dhar, P.; Bandyopadhyay, S.K. A sandwich-ELISA for the diagnosis of Peste des petits ruminants (PPR) infection in small ruminants using anti-nucleocapsid protein monoclonal antibody. Arch. Virol. 2004, 149, 2155–2170. [Google Scholar] [CrossRef]
- Butswat, I.S.R.; Zahraddeen, D.; Hussaini, A.S. Prevalence of peste de pestits ruminant (PPR) and helminthiasis in sheep and goats in Bauchi, Nigeria. Bull. Anim. Health Prod. Afr. 2005, 53, 131–134. [Google Scholar] [CrossRef]
- Taylor, W.P.; Diallo, A.; Gopalakrishna, S.; Sreeramalu, P.; Wilsmore, A.J.; Nanda, Y.P.; Libeau, G.; Rajasekhar, M.; Mukhopadhyay, A.K. Peste des petits ruminants has been widely present in southern India since, if not before, the late 1980s. Prev. Vet. Med. 2002, 52, 305–312. [Google Scholar] [CrossRef]
- Srinivas, R.P.; Gopal, T. PPR: A new menace of sheep and goats. Livest. Advis. 1996, 21, 22–26. [Google Scholar]
- Hegde, R.; Gomes, A.R.; Muniyellappa, H.K.; Byregowda, S.M.; Giridhar, P.; Renukaprasad, C. A short note on peste des petits ruminants in Karnataka, India. Rev. Sci. Tech. 2009, 28, 1031–1035. [Google Scholar] [CrossRef]
- Soundararajan, C.; Sivakumar, T.; Ramesh, S.; Muthukrishnan, S.; Palanidorai, R. Peste des petits ruminants among sheep and goats in an organized farm in Tamil Nadu. Indian Vet. J. 2006, 83, 1045–1047. [Google Scholar]
- Taylor, W.P. The distribution and epidemiology of peste des petits ruminants. Prev. Vet. Med. 1984, 2, 157–166. [Google Scholar] [CrossRef]
- Kumar, P.; Kumar, R.; Sharma, A.K.; Tripathi, B.N. Pathology of peste des petits ruminats (PPR) in goats and sheep: Spontaneous study. Indian J. Vet. Pathol. 2002, 26, 15–18. [Google Scholar]
- Tripathi, B.N.; Chhattopadhyay, S.K.; Parihar, N.S. Clinicopathological studies on an outbreak of peste des petits ruminants in goats and sheep. Indian J. Vet. Pathol. 1996, 20, 99. [Google Scholar]
- Mondal, A.K.; Chottopadhyay, A.P.; Sarkar, S.; Saha, G.R.; Bhowmik, M.K. Report on epizootiological and clinicopathological observations on peste des petits ruminants (PPR) of goats in West Bengal. Indian J. Anim. Health 1995, 34, 145–148. [Google Scholar]
- Nanda, Y.P.; Chatterjee, A.; Purohit, A.K.; Diallo, A.; Innui, K.; Sharma, R.N.; Libeau, G.; Thevasagayam, J.A.; Bruning, A.; Kitching, R.P.; et al. The isolation of peste des petits ruminants virus from Northern. India. Vet. Microbiol. 1996, 51, 207–216. [Google Scholar] [CrossRef]
- Munir, M.; Zohari, S.; Berg, M. Molecular Biology and Pathogenesis of Peste des Petits Ruminants Virus; Springer: Berlin, Germany, 2013; pp. 23–32. [Google Scholar]
- Raghavendra, A.G.; Gajendragad, M.R.; Sengupta, P.P.; Patil, S.S.; Tiwari, C.B.; Balumahendiran, M.; Sankri, V.; Prabhudas, K. Seroepidemiology of peste des petits ruminants in sheep and goats of southern peninsular India. Rev. Sci. Tech. 2008, 27, 861–867. [Google Scholar] [CrossRef] [Green Version]
- Balamurugan, V.; Das, S.; Raju, D.S.N.; Chakravarty, I.; Nagalingam, M.; Hemadri, D.; Govindaraj, G.; Ibotombi Singh, N.; Ltu, K.; Devi, M.; et al. Prevalence of peste des petits ruminants in goats in North-East India. Virusdisease 2014, 25, 488–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balamurugan, V.; Varghese, B.; Muthuchelvan, D.; Vinod Kumar, K.; Suresh, K.P.; Govindaraj, G.; Hemadri, D.; Roy, P. Serosurvey of peste des petits ruminants in small ruminants in the hilly terrain north-eastern Sikkim state of India. Adv. Anim. Vet. Sci. 2020, 8, 1421–1426. [Google Scholar] [CrossRef]
- Sen, A.; Saravanan, P.; Balamurugan, V.; Rajak, K.K.; Sudhakar, S.B.; Bhanuprakash, V.; Parida, S.; Singh, R.K. Vaccines against peste des petits ruminants virus. Expert Rev. Vaccines 2010, 9, 785–796. [Google Scholar] [CrossRef] [PubMed]
- Saravanan, P.; Balamurugan, V.; Sen, A.; Sreenivasa, B.P.; Singh, R.P.; Bandyopadhyay, S.K.; Singh, R.K. Long term immune response of goats to a Vero cell adapted live attenuated homologous PPR vaccine. Indian Vet. J. 2010, 87, 1–3. [Google Scholar]
- Hodgson, S.; Moffat, K.; Hill, H.; Flannery, J.T.; Graham, S.P.; Baron, M.D.; Darpel, K.E. Comparison of the Immunogenicities and Cross-Lineage Efficacies of Live Attenuated Peste des Petits Ruminants Virus Vaccines PPRV/Nigeria/75/1 and PPRV/Sungri/96. J. Virol. 2018, 92, e01471-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahapatra, M.; Selvaraj, M.; Parida, S. Comparison of Immunogenicity and Protective Efficacy of PPR Live Attenuated Vaccines (Nigeria 75/1 and Sungri 96) Administered by Intranasal and Subcutaneous Routes. Vaccines 2020, 8, 168. [Google Scholar] [CrossRef] [Green Version]
- Govindaraj, G.N.; Roy, G.; Mohanty, B.S.; Balamurugan, V.; Pandey, A.K.; Sharma, V.; Patel, A.; Mehra, M.; Pandey, S.K.; Roy, P. Evaluation of effectiveness of mass vaccination campaign against Peste des petits ruminants in Chhattisgarh state, India. Transbound. Emerg. Dis. 2019, 66, 1349–1359. [Google Scholar] [CrossRef]
- Sireesha, S.; Krishna Jyothi, Y.; Jyothi, N.; Hanmanth, G.R. Strategic control of PPR disease in Andhra Pradesh. In Proceedings of the National Conference on PPR Disease “Control of PPR Diseases: Challenges and Opportunities”, New Delhi, India, 28–29 November 2014; pp. 31–33. [Google Scholar]
- Roy, G.; Gordiya, N.; Siyar, D.K.; Pandey, S.K. Mass vaccination for prevention of PPR disease on the lines of pulse polio campaign- Experiences from Chhattisgarh. In Proceedings of the National Conference on PPR Disease: “Control of PPR diseases: Challenges and Opportunities”, New Delhi, India, 28–29 November 2014; pp. 65–68. [Google Scholar]
- Balamurugan, V.; Muthuchelvan, D.; Govindaraj, G.; Roy, G.; Sharma, V.; Sowjanya Kumari, S.; Choudhary, D.; Mohanty, B.S.; Suresh, K.P.; Rajak, K.K.; et al. Serosurvey for assessing PPR vaccination status in rural system of Chhattisgarh state of India. Small Rum. Res. 2018, 165, 87–92. [Google Scholar] [CrossRef]
- Balamurugan, V.; Varghese, B.; Muthuchelvan, D.; SowjanyaKumari, S.; Kumar, K.V.; Suresh, K.P.; Govindaraj, G.; Sunder, J.; Hemadri, D.; Roy, P. Cross-sectional seroprevalence study of peste des petits ruminants in goats in Andaman and Nicobar Islands, India. Small Rum. Res. 2019, 178, 111–116. [Google Scholar] [CrossRef]
- Balamurugan, V.; Krishnamoorthy, P.; Veeregowda, B.M.; Sen, A.; Rajak, K.K.; Bhanuprakash, V.; Gajendragad, M.R.; Prabhudas, K. Seroprevalence of Peste des petits ruminants in cattle and buffaloes from Southern Peninsular India. Trop. Anim. Health Prod. 2012, 44, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.R.; Veeregowda, B.M.; Byregowda, S.M.; Balamurugan, V. Comprehensive review on recent developments in the diagnostics and vaccines against Peste des petits ruminants. Br. J. Virol. 2016, 3, 90–104. [Google Scholar] [CrossRef]
- Balamurugan, V.; Govindaraj, G.; SowjanyaKumari, S.; Nagalingam, M.; Tapase, J.; Manjunathareddy, G.B.; Rahman, H. Scorecard method for assessing the severity of peste des petits ruminants in sheep and goats. Virusdisease 2019, 30, 574–578. [Google Scholar] [CrossRef] [PubMed]
- OIE Peste Des Petits Ruminants Aetiology Epidemiology Diagnosis Prevention and Control References; World Organisation for Animal Health: 2020. Available online: https://www.oie.int/fileadmin/Home/eng/Animal_Health_in_the_World/docs/pdf/Disease_cards/PESTE_DES_PETITS_RUMINANTS.pdf (accessed on 21 December 2020).












Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balamurugan, V.; Vinod Kumar, K.; Dheeraj, R.; Kurli, R.; Suresh, K.P.; Govindaraj, G.; Shome, B.R.; Roy, P. Temporal and Spatial Epidemiological Analysis of Peste Des Petits Ruminants Outbreaks from the Past 25 Years in Sheep and Goats and Its Control in India. Viruses 2021, 13, 480. https://doi.org/10.3390/v13030480
Balamurugan V, Vinod Kumar K, Dheeraj R, Kurli R, Suresh KP, Govindaraj G, Shome BR, Roy P. Temporal and Spatial Epidemiological Analysis of Peste Des Petits Ruminants Outbreaks from the Past 25 Years in Sheep and Goats and Its Control in India. Viruses. 2021; 13(3):480. https://doi.org/10.3390/v13030480
Chicago/Turabian StyleBalamurugan, Vinayagamurthy, Kirubakaran Vinod Kumar, Ramesh Dheeraj, Rashmi Kurli, Kuralayanapalya Puttahonnappa Suresh, GurrappaNaidu Govindaraj, Bibek Ranjan Shome, and Parimal Roy. 2021. "Temporal and Spatial Epidemiological Analysis of Peste Des Petits Ruminants Outbreaks from the Past 25 Years in Sheep and Goats and Its Control in India" Viruses 13, no. 3: 480. https://doi.org/10.3390/v13030480