
COVEVOL: Natural Evolution at 6 Months of COVID-19

 , ,
, ,
Abstract
:1. Introduction
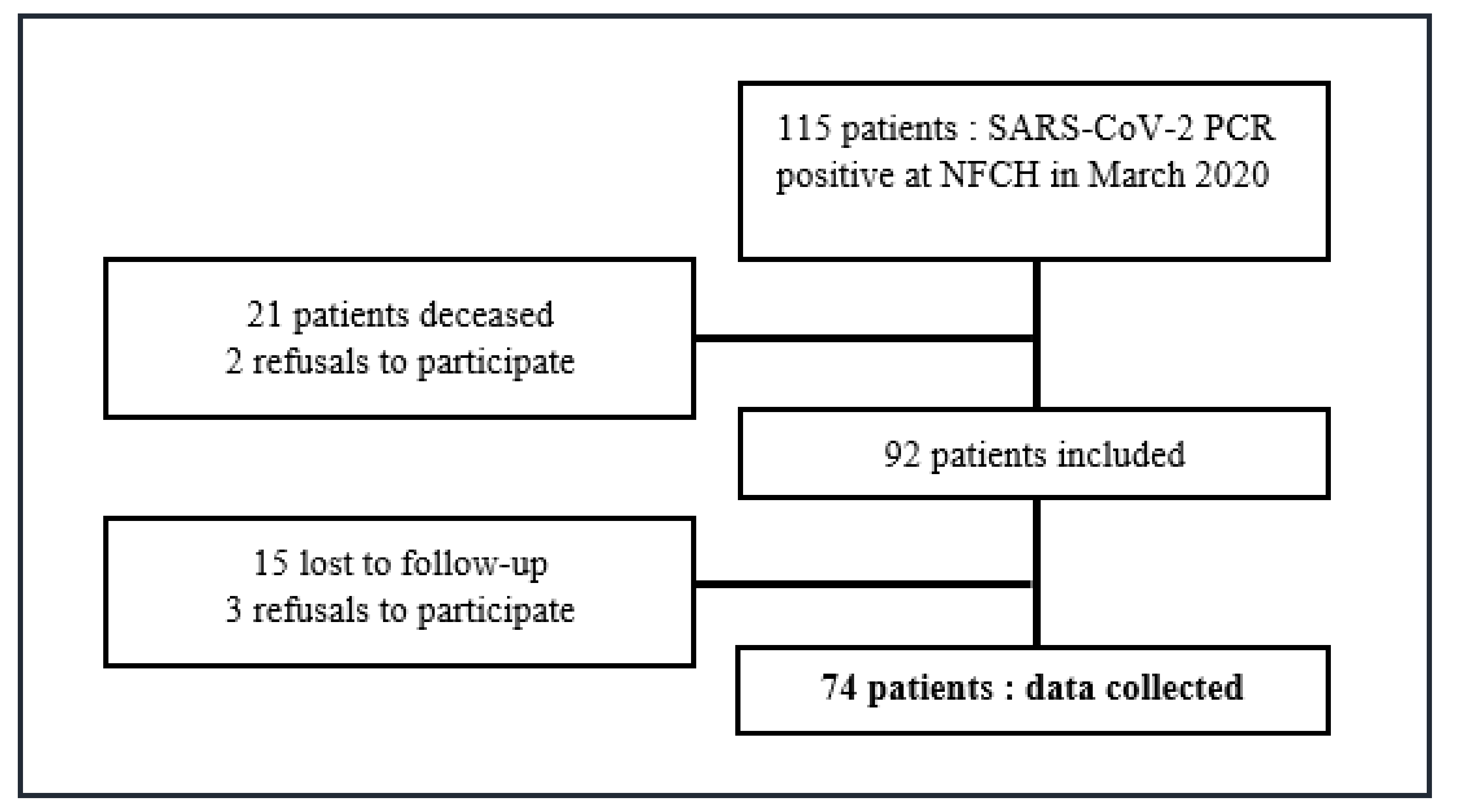
2. Materials and Methods
3. Results
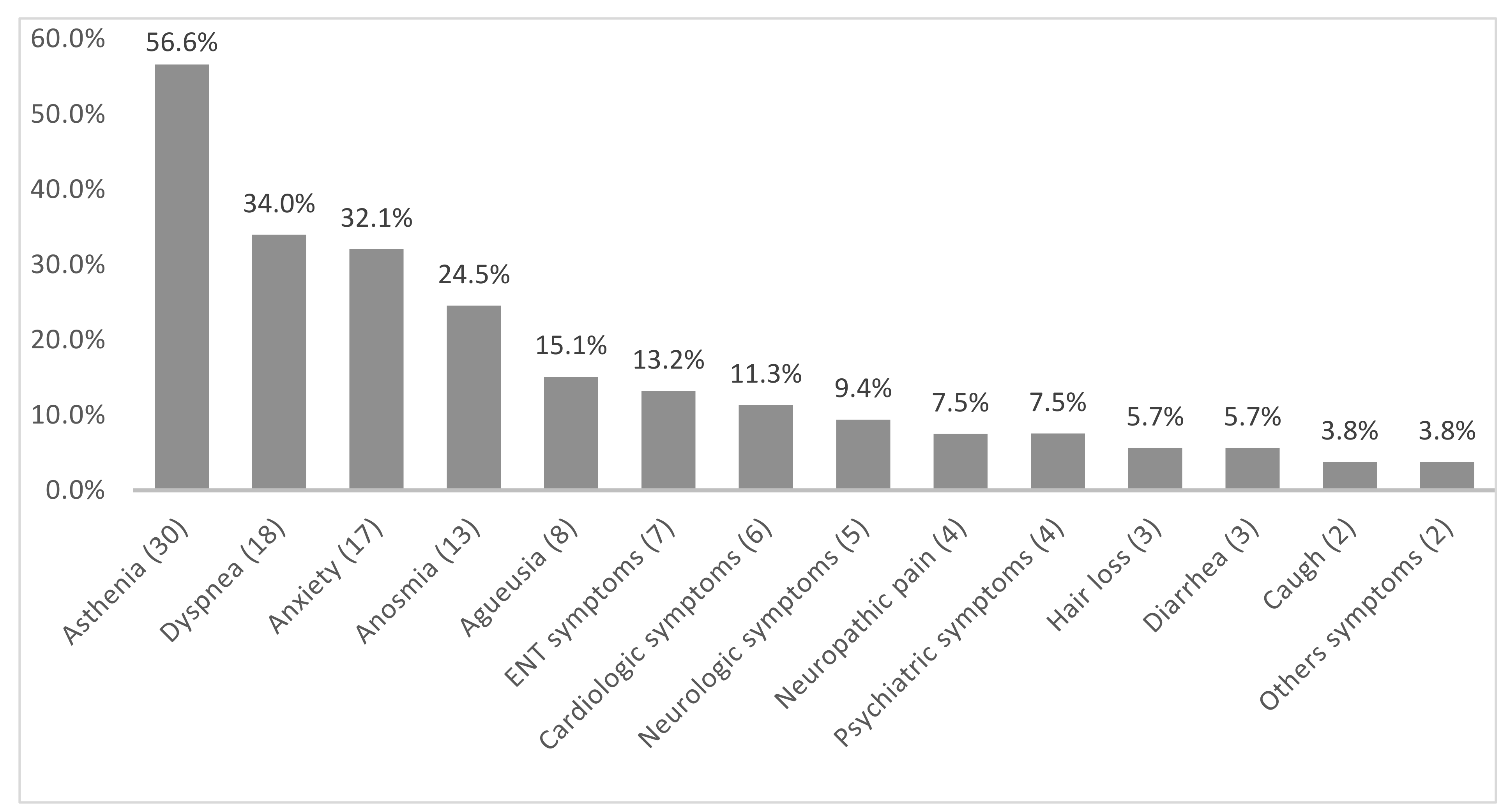
3.1. Description of the PS Group (n = 53)
3.2. Comparison of the Two Groups: PS Group versus No-PS Group
3.3. Comparison According to the Main Persistent Symptoms
3.3.1. Asthenia
3.3.2. Dyspnea
3.3.3. Anxiety
3.3.4. Anosmia
3.3.5. Agueusia
3.4. Description of Patients with Resurgence of Symptoms (n = 10)
3.5. Comparison of the Two Groups: R Group vs. No-R Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shereen, M.A.; Khan, S.; Kazmi, A.; Bashir, N.; Siddique, R. COVID-19 infection: Origin, transmission, and characteristics of human coronaviruses. J. Adv. Res. 2020, 24, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Allocution Liminaire du Directeur Général de l’OMS Lors du Point Presse sur la COVID-19. 2020. Available online: https://www.who.int/fr/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19 (accessed on 11 March 2020).
- Desvaux, É.; Faucher, J.-F. Covid-19: Aspects cliniques et principaux éléments de prise en charge. Rev. Francoph. Lab. 2020, 2020, 40–47. [Google Scholar] [CrossRef]
- Guan, W.; Liang, W.; Zhao, Y.; Liang, H.; Chen, Z.; Li, Y. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 2000547. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7098485/ (accessed on 10 February 2021). [CrossRef] [Green Version]
- Coronavirus: Chiffres Clés et Évolution de la COVID-19 en France et dans le Monde. Available online: https://dossiers/coronavirus-covid-19/coronavirus-chiffres-cles-et-evolution-de-la-covid-19-en-france-et-dans-le-monde (accessed on 10 February 2021).
- Zaffina, S.; Lanteri, P.; Gilardi, F.; Garbarino, S.; Santoro, A.; Vinci, M.R. Recurrence, Reactivation, or Inflammatory Rebound of SARS-CoV-2 Infection With Acute Vestibular Symptoms: A Case Report and Revision of Literature. Front. Hum. Neurosci. 2021, 15, 444. [Google Scholar] [CrossRef]
- Suivi des patients convalescents de la COVID-19 par le médecin généraliste. Bull. Acad. Natl. Med. 2020, 204, 769.
- Petersen, M.S.; Kristiansen, M.F.; Hanusson, K.D.; Danielsen, M.E.; á Steig, B.; Gaini, S. Long COVID in the Faroe Islands—A longitudinal study among non-hospitalized patients. Clin. Infect. Dis. 2020, ciaa1792. [Google Scholar] [CrossRef]
- Laëtitia, L.G. Réponses Rapides Dans le Cadre de la Covid-19: Symptômes Prolongés Suite à une Covid-19 de l’adulte—Diagnostic et Prise en Charge. Available online: https://www.has-sante.fr/upload/docs/application/pdf/2021-02/20rr430_covid_19_symptomes_prolonges_post_cd.pdf (accessed on 4 October 2021).
- Yelin, D.; Wirtheim, E.; Vetter, P.; Kalil, A.C.; Bruchfeld, J.; Runold, M. Long-term consequences of COVID-19: Research needs. Lancet Infect. Dis. 2020, 20, 1115–1117. [Google Scholar] [CrossRef]
- Osikomaiya, B.; Erinoso, O.; Wright, K.O.; Odusola, A.O.; Thomas, B.; Adeyemi, O. ‘Long COVID’: Persistent COVID-19 symptoms in survivors managed in Lagos State, Nigeria. BMC Infect. Dis. 2021, 21, 304. [Google Scholar] [CrossRef] [PubMed]
- Huang, C. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Xiong, Q.; Xu, M.; Li, J.; Liu, Y.; Zhang, J.; Xu, Y. Clinical sequelae of COVID-19 survivors in Wuhan, China: A single-centre longitudinal study. Clin. Microbiol. Infect. 2021, 27, 89–95. [Google Scholar] [CrossRef]
- Cirulli, E.T.; Barrett, K.M.S.; Riffle, S.; Bolze, A.; Neveux, I.; Dabe, S. Long-term COVID-19 symptoms in a large unselected population. medRxiv 2020. [Google Scholar] [CrossRef]
- Havervall, S.; Rosell, A.; Phillipson, M.; Mangsbo, S.M.; Nilsson, P.; Hober, S. Symptoms and Functional Impairment Assessed 8 Months After Mild COVID-19 Among Health Care Workers. JAMA 2021, 325, 2015. [Google Scholar] [CrossRef] [PubMed]
- Peluso, M.J.; Kelly, J.D.; Lu, S.; Goldberg, S.A.; Davidson, M.C.; Mathur, S. Rapid implementation of a cohort for the study of post-acute sequelae of SARS-CoV-2 infection/COVID-19. medRxiv 2021. [Google Scholar] [CrossRef]
- Leth, S.; Gunst, J.D.; Mathiasen, V.; Hansen, K.; Søgaard, O.; Østergaard, L. Persistent Symptoms in Patients Recovering From COVID-19 in Denmark. Open Forum. Infect. Dis. 2021, 8, ofab042. [Google Scholar] [CrossRef] [PubMed]
- Carfì, A.; Bernabei, R.; Landi, F.; The Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603. [Google Scholar] [CrossRef]
- Tenforde, M.W. Symptom Duration and Risk Factors for Delayed Return to Usual Health Among Outpatients with COVID-19 in a Multistate Health Care Systems Network—United States, March–June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 993. Available online: https://www.cdc.gov/mmwr/volumes/69/wr/mm6930e1.htm (accessed on 18 April 2021). [CrossRef] [PubMed]
- Armange, L.; Bénézit, F.; Picard, L.; Pronier, C.; Guillot, S.; Lentz, P.-A. Prevalence and characteristics of persistent symptoms after non-severe COVID-19: A prospective cohort study. Eur. J. Clin. Microbiol. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Moreno-Pérez, O.; Merino, E.; Leon-Ramirez, J.-M.; Andres, M.; Ramos, J.M.; Arenas-Jiménez, J. Post-acute COVID-19 Syndrome. Incidence and risk factors: A Mediterranean cohort study. J. Infect. 2021, 82, 378–383. Available online: http://www.sciencedirect.com/science/article/pii/S0163445321000098 (accessed on 29 January 2021). [CrossRef]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: A cross-sectional evaluation. J. Med. Virol. 2021, 93, 1013–1022. [Google Scholar] [CrossRef]
- Garrigues, E.; Janvier, P.; Kherabi, Y.; Le Bot, A.; Hamon, A.; Gouze, H. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J. Infect. 2020, 81, e4–e6. [Google Scholar] [CrossRef]
- Goërtz, Y.M.J.; Herck, M.V.; Delbressine, J.M.; Vaes, A.W.; Meys, R.; Machado, F.V.C. Persistent symptoms 3 months after a SARS-CoV-2 infection: The post-COVID-19 syndrome? ERJ Open Res. 2020, 6, 00542–2020. Available online: https://openres.ersjournals.com/content/6/4/00542-2020 (accessed on 1 April 2021). [CrossRef] [PubMed]
- Delfraissy, J.-F.; Atlani-Duault, L.; Benamouzig, D.; Bouadma, L.; Cauchemez, S.; Chirouze, C. Anticiper et différencier les stratégies pour sortir des phases aiguës de l’épidémie. MARS 2021, 94, 16H00. [Google Scholar]
- Petrilli, C.M.; Jones, S.A.; Yang, J.; Rajagopalan, H.; O’Donnell, L.; Chernyak, Y. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: Prospective cohort study. BMJ 2020, 369, m1966. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C. Attributes and predictors of Long-COVID: Analysis of COVID cases and their symptoms collected by the Covid Symptoms Study App. medRxiv 2020. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef] [PubMed]
- Reddy, R.K.; Charles, W.N.; Sklavounos, A.; Dutt, A.; Seed, P.T.; Khajuria, A. The effect of smoking on COVID-19 severity: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 1045–1056. [Google Scholar] [CrossRef] [PubMed]
- Klement-Frutos, E.; Burrel, S.; Pourcher, V.; Boutolleau, D. Étude COVL: Impact de la charge virale nasopharyngée du SARS-COV-2 sur l’évolution clinique en hospitalisation. Med. Mal. Infect. 2020, 50 (Suppl. 6), S76–S77. [Google Scholar] [CrossRef]
- Néant, N.; Lingas, G.; Hingrat, Q.L.; Ghosn, J.; Engelmann, I.; Lepiller, Q. Modeling SARS-CoV-2 viral kinetics and association with mortality in hospitalized patients from the French COVID cohort. Proc. Natl. Acad. Sci. USA 2021, 118. Available online: https://www.pnas.org/content/118/8/e2017962118 (accessed on 28 June 2021). [CrossRef]
- Garg, P.; Arora, U.; Kumar, A.; Malhotra, A.; Kumar, S.; Garg, S. Risk factors for prolonged fatigue after recovery from COVID-19. J. Med. Virol. 2021, 93, 1926–1928. [Google Scholar] [CrossRef] [PubMed]
- Jessica, L. Fatigue au Cours des Symptômes Prolongés de la Covid-19. Available online: https://www.has-sante.fr/upload/docs/application/pdf/2021-02/fiche_-_fatigue.pdf (accessed on 4 October 2021).
- Islam, M.F.; Cotler, J.; Jason, L.A. Post-viral fatigue and COVID-19: Lessons from past epidemics. Fatigue Biomed. Health Behav. 2020, 8, 61–69. [Google Scholar] [CrossRef]
- Caussy, C. Obésité et infection par la COVID-19: Une liaison dangereuse. Med. Mal. Metab. 2021, 15, 288–293. [Google Scholar]
- Long-Term Clinical Outcomes in Survivors of Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome Coronavirus (MERS) Outbreaks after Hospitalisation or Icu Admission: A Systematic Review and Meta-Analysis. Available online: http://www.medicaljournals.se/jrm/content/abstract/10.2340/16501977-2694 (accessed on 8 July 2021).
- McGroder, C.F.; Zhang, D.; Choudhury, M.A.; Salvatore, M.M.; D’Souza, B.M.; Hoffman, E.A. Pulmonary Fibrosis 4 Months after COVID-19 Is Associated with Severity of Illness and Blood Leucocyte Telomere Length. Thorax 2021. Available online: https://thorax.bmj.com/content/early/2021/05/13/thoraxjnl-2021-217031 (accessed on 7 June 2021).
- Laëtitia, G. La Dyspnée au Cours des Symptômes Prolongés de la Covid-19. Available online: https://www.has-sante.fr/upload/docs/application/pdf/2021-02/fiche_-_dyspnee.pdf (accessed on 4 October 2021).
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, E1729. [Google Scholar] [CrossRef] [Green Version]
- Taquet, M.; Luciano, S.; Geddes, J.R.; Harrison, P.J. Bidirectional associations between COVID-19 and psychiatric disorder: Retrospective cohort studies of 62,354 COVID-19 cases in the USA. Lancet Psychiatry 2021, 8, 130–140. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; Beckers, E.; Mustin, V.; Ducarme, M.; Journe, F. Prevalence and 6-month recovery of olfactory dysfunction: A multicentre study of 1363 COVID-19 patients. J. Intern. Med. 2021, 290, 451–461. [Google Scholar] [CrossRef]
- Eliezer, M.; Hautefort, C.; Hamel, A.-L.; Verillaud, B.; Herman, P.; Houdart, E. Sudden and Complete Olfactory Loss of Function as a Possible Symptom of COVID-19. JAMA Otolaryngol. Neck Surg. 2020, 146, 674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, X.; Lian, J.-S.; Hu, J.-H.; Gao, J.; Zheng, L.; Zhang, Y.-M. Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut 2020, 69, 1002–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiesa-Estomba, C.M.; Lechien, J.R.; Barillari, M.R.; Saussez, S. Patterns of Gustatory Recovery in Patients Affected by the COVID-19 Outbreak. Virol. Sin. 2020, 35, 833–837. [Google Scholar] [CrossRef] [PubMed]
- Hanif, M.; Haider, M.A.; Ali, M.J.; Naz, S.; Sundas, F. Reinfection of COVID-19 in Pakistan: A First Case Report. Cureus 2020, 12, e11176. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7689968/ (accessed on 9 January 2021). [CrossRef] [PubMed]
- Zayet, S.; Royer, P.-Y.; Toko, L.; Pierron, A.; Gendrin, V.; Klopfenstein, T. Recurrence of COVID-19 after recovery ? A case series in health care workers, France. Microbes Infect. 2021, 23, 104803. [Google Scholar] [CrossRef] [PubMed]
- Ravioli, S.; Ochsner, H.; Lindner, G. Reactivation of COVID-19 pneumonia: A report of two cases. J. Infect. 2020, 81, e72–e73. [Google Scholar] [CrossRef] [PubMed]
- Loconsole, D.; Passerini, F.; Palmieri, V.O.; Centrone, F.; Sallustio, A.; Pugliese, S. Recurrence of COVID-19 after recovery: A case report from Italy. Infection 2020. [Google Scholar] [CrossRef] [PubMed]
- Zayet, S.; Zahra, H.; Royer, P.-Y.; Tipirdamaz, C.; Mercier, J.; Gendrin, V. Post-COVID-19 Syndrome: Nine Months after SARS-CoV-2 Infection in a Cohort of 354 Patients: Data from the First Wave of COVID-19 in Nord Franche-Comté Hospital, France. Microorganisms 2021, 9, 1719. [Google Scholar] [CrossRef] [PubMed]
- Galanti, M.; Shaman, J. Direct observation of repeated infections with endemic coronaviruses. J. Infect. Dis. 2021, 223, 409–415. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Persistent Symptoms | No-PS Group (n = 21) (28.4%) | PS Group (n = 53) (71.6%) | Total (n = 74) (100%) | p-(Value) | |
|---|---|---|---|---|---|
| Demographic and baseline characteristics | |||||
| Age (years) (mean, extremes, SD) | 46.1 (23.7–91.1) ± 19.6 | 54.7 (21–89.2) ± 16.9 | 52.3 (21–91.1) ± 18 | 0.0625 | |
| (number, %) | (18–30) | 4 (19.1) | 5 (9.4) | 9 (12.2) | 0.0048 |
| (31–40) | 7 (33.3) | 8 (15.1) | 15 (20.3) | ||
| (41–50) | 6 (28.6) | 8 (15.1) | 14 (18.9) | ||
| (51–60) | 0 | 9 (17) | 9 (12.2) | ||
| (61–70) | 0 | 14 (26.4) | 14 (18.9) | ||
| >71 | 4 (19.1) | 9 (17) | 13 (17.5) | ||
| Sex (number, %) | Female | 14 (66.7) | 30 (56.6) | 44 (59.5) | 0.4267 |
| HCWs (number, %) | 12 (57.1) | 23 (43.4) | 35 (47.3) | 0.2856 | |
| BMI (kg/m2) (mean, extremes, SD) | 24.3 (19.6–31.4) ± 3 | 27.1 (17.9–42.4) ± 5.4 | 26.3 (17.9–42.4) ± 5 | 0.0071 | |
| (number, %) | <25 | 13 (61.9) | 25 (47.2) | 38 (51.4) | 0.0350 |
| (25–30) | 7 (33.3) | 11 (20.7) | 18 (24.3) | ||
| >30 | 1 (4.8) | 17 (32.1) | 18 (24.3) | ||
| Tobacco (number, %) | Current smoking | 0 | 4 (7.5) | 4 (5.4) | 0.5725 |
| Former smoker | 5 (23.8) | 15 (28.3) | 20 (27) | 0.6948 | |
| Number of pack–year (mean, extremes, SD) | 1 (0–9) ± 2.2 | 4.8 (0–40) ± 9.3 | 3.7 (0–40) ± 8.1 | 0.0074 | |
| Alcohol (number, %) | No alcohol consumption | 4 (19) | 12 (22.6) | 16 (21.6) | 1 |
| Occasional drinking | 14 (66.7) | 34 (64.2) | 48 (64.9) | ||
| Daily alcohol consumption | 3 (14.3) | 7 (13.2) | 10 (13.5) | ||
| Comorbidities (number, %) | 7 (33.3) | 30 (56.6) | 37 (50) | 0.0711 | |
| Allergic condition | 5 (23.8) | 11 (21.1) | 16 (21.9) | 0.7657 | |
| High blood pressure | 2 (9.5) | 11 (20.7) | 13 (17.6) | 0.3264 | |
| Venous thromboembolic disease | 0 | 7 (13.2) | 7 (9.5) | 0.1808 | |
| Diabetes | 1 (4.8) | 5 (9.4) | 6 (8.1) | 0.6681 | |
| Asthma | 2 (9.5) | 3 (5.7) | 5 (6.8) | 0.6163 | |
| Heart failure | 2 (9.5) | 1 (1.9) | 3 (4) | 0.1922 | |
| Active malignancy | 0 | 3 (5.7) | 3 (4) | 0.5536 | |
| Obstructive sleep apnea syndrome | 1 (4.8) | 2 (3.8) | 3 (4) | 1 | |
| Coronary artery disease | 1 (4.8) | 5 (9.4) | 2 (2.7) | 0.4954 | |
| Autoimmune condition | 2 (3.8) | 0 | 2 (2.7) | 1 | |
| Chronic obstructive pulmonary disease | 0 | 1 (1.9) | 1 (1.3) | 1 | |
| Chronic kidney failure | 0 | 1 (1.9) | 1 (1.3) | 1 | |
| Malignancy in remission | 0 | 1 (1.9) | 1 (1.3) | 1 | |
| Charlson score | 0 | 17 (81) | 35 (66) | 52 (70.3) | 0.2658 |
| (1–10) | 4 (19) | 18 (34) | 22 (29.7) | ||
| Chronic treatment (number, %) | 6 (28.6) | 28 (52.8) | 34 (46) | 0.0590 | |
| CEIs | 2 (9.5) | 4 (7.5) | 6 (8.1) | 1 | |
| Statins | 1 (4.8) | 5 (9.4) | 6 (8.1) | 0.6681 | |
| Oral antidiabetics | 1 (4.8) | 4 (7.5) | 5 (6.8) | 1 | |
| NSAIDs | 0 | 4 (7.5) | 4 (5.4) | 0.5725 | |
| ARBs | 1 (4.8) | 1 (1.9) | 2 (2.7) | 0.4898 | |
| Corticosteroids | 0 | 1 (1.9) | 1 (1.3) | 1 | |
| Immunosuppressor | 1 (1.9) | 0 | 1 (1.3) | 1 | |
| Clinical characteristics | |||||
| Initial symptomatology | |||||
| General symptoms (number, %) | Asthenia | 21 (100) | 48 (90.6) | 69 (93.2) | 0.3129 |
| Headaches | 17 (80.9) | 41 (77.4) | 58 (78.4) | 1 | |
| Fever | 14 (66.7) | 42 (79.2) | 56 (75.7) | 0.2555 | |
| Myalgia | 14 (66.7) | 39 (73.6) | 53 (71.6) | 0.5518 | |
| ENT symptoms (number, %) | Dysgueusia | 14 (66.7) | 33 (62.3) | 47 (63.5) | 0.7228 |
| Anosmia | 11 (52.4) | 34 (64.2) | 45 (60.8) | 0.3498 | |
| Rhinorrhea | 9 (42.9) | 25 (47.2) | 34 (46) | 0.7372 | |
| Facial headaches | 6 (28.6) | 21 (39.6) | 27 (36.5) | 0.3733 | |
| Odynophagy | 12 (57.1) | 15 (28.3) | 27 (36.5) | 0.0202 | |
| Sneezing | 8 (38.1) | 17 (32.1) | 25 (33.8) | 0.6216 | |
| Nasal obstruction | 9 (42.9) | 10 (18.9) | 19 (25.7) | 0.0332 | |
| Tinnitus | 2 (9.5) | 6 (11.3) | 8 (10.8) | 1 | |
| Hypoacusis | 1 (4.8) | 4 (7.5) | 5 (6.8) | 1 | |
| Epistaxis | 1 (4.8) | 3 (5.7) | 4 (5.4) | 1 | |
| Cardiopulmonary symptoms (number, %) | Cough | 18 (85.7) | 43 (81.1) | 61 (82.4) | 0.7466 |
| Dyspnea | 4 (19) | 21 (39.6) | 25 (33.8) | 0.0916 | |
| Chest pain | 5 (23.8) | 15 (28.3) | 20 (27) | 0.6948 | |
| Hemoptysis | 0 | 3 (5.7) | 3 (4) | 0.5536 | |
| Digestive symptoms (number, %) | Diarrhea | 10 (47.6) | 30 (56.6) | 40 (54) | 0.4844 |
| Nausea | 7 (33.3) | 23 (43.4) | 30 (40.5) | 0.4267 | |
| Abdominal pain | 4 (19) | 14 (26.4) | 18 (24.3) | 0.5054 | |
| Vomiting | 2 (9.5) | 4 (7.5) | 6 (8.1) | 1 | |
| Anxiety (number, %) | 0 | 15 (71.4) | 26 (49.1) | 41 (55.5) | 0.0585 |
| (1,2) | 6 (28.6) | 17 (32.1) | 23 (31.1) | ||
| (3,4) | 0 | 10 (18.9) | 10 (13.5) | ||
| Duration of symptoms of SARS–CoV–2 infection (days) (mean, extremes, SD) | 12.4 (3–28) ± 6.7 | 14.3 (3–51) ± 9.4 | 13.7 (3–51) ± 8.7 | 0.4170 | |
| Hospitalization (number, %) | 4 (19) | 24 (45.3) | 28 (37.8) | 0.0359 | |
| Conventional hospitalization | 4 (19) | 23 (43.4) | 27 (36.5) | 0.0498 | |
| Intensive care unit | 0 | 4 (7.5) | 4 (5.4) | 0.5725 | |
| Duration of hospitalization (days) (mean, extremes, SD) | 2.0 (0–21) ± 5.9 | 4.1 (0–41) ± 8.7 | 3.5 (0–41) ± 8 | 0.3184 | |
| Oxygenotherapy (number, %) | 2 (9.5) | 15 (28.3) | 17 (23) | 0.1256 | |
| Mechanical ventilation (number, %) | 0 | 3 (5.7) | 3 (4) | 0.5536 | |
| Ct gene E (log10 copies/mL) (mean, extremes, SD) | 23.6 (13.5–34.3) ± 6.9 | 27.5 (15.2–39.8) ± 6.7 | 26.4 (13.5–39.8) ± 6.9 | 0.0303 | |
| 2a. Asthenia | No-Asth Group (n = 44) (59.5%) | Asth Group (n = 30) (40.5%) | Total (n = 74) (100%) | p-(Value) | ||
|---|---|---|---|---|---|---|
| Demographic and baseline characteristics | ||||||
| Age (mean, extremes, SD) | 47.5 (21–91.1) ± 17.3 | 59.2 (29.1–89.2) ± 16.9 | 52.3 (21–91.1) ± 18 | 0.0045 | ||
| Sex (number, %) | Female | 27 (61.4) | 17 (56.7) | 44 (59.5) | 0.8102 | |
| HCWs (number, %) | 25 (56.8) | 10 (33.3) | 35 (47.3) | 0.0597 | ||
| BMI (kg/m2) (mean, extremes, SD) | 25.4 (19.1–42.4) ± 4.9 | 27.6 (17.9–38.6) ± 4.9 | 26.3 (17.9–42.4) ± 5 | 0.0277 | ||
| Comorbidities (number, %) | 17 (38.6) | 20 (66.7) | 37 (50) | 0.0323 | ||
| High blood pressure | 3 (6.8) | 10 (33.3) | 13 (17.6) | 0.0048 | ||
| Charlson score | 0 | 35 (79.6) | 17 (56.7) | 52 (70.3) | 0.0418 | |
| (1–10) | 9 (20.4) | 13 (43.3) | 22 (29.7) | |||
| Chronic treatment (number, %) | 16 (36.4) | 18 (60) | 34 (46) | 0.0588 | ||
| Clinical characteristics | ||||||
| Initial symptomatology | ||||||
| Asthenia | (0–2) | 31 (70.5) | 12 (40) | 43 (58.1) | 0.0158 | |
| (3–4) | 13 (29.5) | 18 (60) | 31 (41.9) | |||
| Nasal obstruction | 17 (38.6) | 2 (6.7) | 19 (25.7) | 0.0024 | ||
| Hospitalization (number, %) | 9 (20.4) | 19 (63.3) | 28 (37.8) | 0.0003 | ||
| Conventional hospitalization | 9 (20.4) | 18 (60) | 27 (36.5) | 0.0012 | ||
| Intensive care unit | 2 (4.5) | 2 (6.7) | 4 (5.4) | 0.5725 | ||
| Duration of hospitalization (days) (mean, extremes, SD) | 2.5 (0–39) ± 7.3 | 5.1 (0–41) ± 8.9 | 3.5 (0–41) ± 8 | 0.0008 | ||
| Oxygenotherapy (number, %) | 6 (13.6) | 11 (36.7) | 17 (23) | 0.0266 | ||
| Mechanical ventilation (number, %) | 1 (2.3) | 2 (6.7) | 3 (4) | 0.5622 | ||
| Ct gene E (log10 copies/mL) (mean, extremes, SD) | 25 (13.5–39.8) ± 7.3 | 28.5 (16.8–38.9) ± 5.9 | 26.4 (13.5–39.8) ± 6.9 | 0.0436 | ||
| 2b. Dyspnea | no-D Group (n = 56) (75,7%) | D Group (n = 18) (24.3%) | Total (n = 74) (100%) | p-(Value) | ||
| Demographic and baseline characteristics | ||||||
| Age (mean, extremes, SD) | 52.9 (23.7–91.1) ± 17.9 | 50.3 (21–89.2) ± 18.5 | 52.3 (21–91.1) ± 18 | 0.6291 | ||
| Sex (number, %) | Female | 33 (58.9) | 11 (61.1) | 44 (59.5) | 1 | |
| HCWs (number, %) | 27 (48.2) | 8 (44.4) | 35 (47.3) | 1 | ||
| BMI (kg/m2) (mean, extremes, SD) | 25.6 (17.9–42.4) ± 4.8 | 28.2 (21–38.6) ± 5.1 | 26.3 (17.9–42.4) ± 5 | 0.0524 | ||
| (number, %) | <25 | 32 (57.1)) | 6 (33.3) | 38 (51.4) | 0.0219 | |
| (25–30) | 15 (26.8) | 3 (16.7) | 18 (24.3) | |||
| >30 | 9 (16.1) | 9 (50) | 18 (24.3) | |||
| Comorbidities (number, %) | 27 (48.2) | 10 (55.6) | 37 (50) | 0.7870 | ||
| Allergic condition | 8 (14.3) | 8 (47.1) | 16 (21.9) | 0.0077 | ||
| Charlson score | 0 | 37 (66.1) | 15 (83.3) | 52 (70.3) | 0.2381 | |
| (1–10) | 19 (33.9) | 3 (16.7) | 22 (29.7) | |||
| Clinical characteristics | ||||||
| Hospitalization (number, %) | 18 (32.1) | 10 (55.6) | 28 (37.8) | 0.0966 | ||
| Conventional hospitalization | 17 (30.4) | 10 (55.6) | 27 (36.5) | 0.0894 | ||
| Intensive care unit | 3 (5.4) | 1 (5.6) | 4 (5.4) | 1 | ||
| 2c. Anxiety HCWs: Healthcare Worker BMI: Body Mass Index | no-Anx Group (n = 57) (77%) | Anx Group (n = 17) (23%) | Total (n = 74) (100%) | p-(Value) | ||
| Demographic and baseline characteristics | ||||||
| Age (mean, extremes, SD) | 49.7 [22.4–91.1] ±17.3 | 60.9[21–89.2] ±18.1 | 52.3 [21–91.1] ±18 | 0.0197 | ||
| (Number, %) | (18–30) | 7 (12.3) | 2 (11.8) | 9 (12.2) | 0.0462 | |
| (31–40) | 15 (26.3) | 0 | 15 (20.3) | |||
| (41–50) | 12 (21) | 2 (11.8) | 14 (18.9) | |||
| (51–60) | 6 (10.5) | 3 (17.6) | 9 (12.2) | |||
| (61–70) | 10(17.5) | 4 (23.5) | 14 (18.9) | |||
| >71 | 7(12.3) | 6 (35.3) | 13 (17.5) | |||
| Sex (number, %) | Female | 34 (59.7) | 10 (58.8) | 44 (59.5) | 1 | |
| HCWs (number, %) | 28 (49.1) | 7 (41.2) | 35 (47.3) | 0.5934 | ||
| BMI (kg/m2) (mean, extremes, SD) | 25.8 (17.9–42.4) ± 4.8 | 27.7 (19.6–39.1) ± 5.5 | 26.3 (17.9–42.4) ± 5 | 0.2296 | ||
| Comorbidities (number, %) | 22 (38.6) | 15 (88.2) | 37 (50) | 0.0006 | ||
| Charlson score | 0 | 46 (80.7) | 6 (35.3) | 52 (70.3) | 0.0007 | |
| (1–10) | 11 (19.3) | 11 (64.7) | 22 (29.7) | |||
| Clinical characteristics | ||||||
| Initial symptomatology | ||||||
| Asthenia | (0–2) | 37 (64.9) | 6 (35.3) | 43 (58.1) | 0.0485 | |
| (3–4) | 20 (35.1) | 11 (64.7) | 31 (41.9) | |||
| Anxiety (number, %) | 0 | 34 (59.7) | 7 (41.2) | 41 (55.5) | <0.0001 | |
| (1–2) | 21 (36.8) | 2 (11.8) | 23 (31.1) | |||
| (3–4) | 2 (3.5) | 8 (47) | 10 (13.5) | |||
| Hospitalization (number, %) | 19 (33.3) | 9 (52.9) | 28 (37.8) | 0.1640 | ||
| 2d. Anosmia | no-An Group (n = 61) (82.4%) | An Group (n = 13) (17.6%) | Total (n = 74) (100%) | p-(Value) | ||
| Demographic and baseline characteristics | ||||||
| Age (mean, extremes, SD) | 53.5 (22.4–91.1) ± 18.2 | 46.3 (21–67.3) ± 16.4 | 52.3 (21–91.1) ± 18 | 0.2052 | ||
| Sex (number, %) | Female | 36 (59) | 8 (61.5) | 44 (59.5) | 1 | |
| BMI (kg/m2) (mean, extremes, SD) | 26.6 (17.9–42.4) ± 5.1 | 24.9 (19.6–32.5) ± 4 | 26.3 (17.9–42.4) ± 5 | 0.3663 | ||
| Comorbidities (number, %) | 31 (50.8) | 6 (46.1) | 37 (50) | 1 | ||
| Charlson score | 0 | 40 (65.6) | 12 (92.3) | 52 (70.3) | 0.0920 | |
| (1–10) | 21 (34.4) | 1(7.7) | 22 (29.7) | |||
| Clinical characteristics | ||||||
| Initial symptomatology | ||||||
| Facial headaches (number, %) | 18 (29.5) | 9 (69.2) | 27 (36.5) | 0.0108 | ||
| Nausea (number, %) | 21 (34.4) | 9 (69.2) | 30 (40.5) | 0.0294 | ||
| Abdominal pain (number, %) | 11 (18) | 7 (53.8) | 18 (24.3) | 0.0117 | ||
| Number of initial symptoms | (0–5) | 6 (9.8) | 0 | 6 (8.1) | 0.0594 | |
| (6–10) | 22 (36.1) | 1 (7.7) | 23 (31) | |||
| (11–15) | 25 (41) | 10 (76.9) | 35 (47.3) | |||
| (16–20) | 8 (13.1) | 2 (15.4) | 10 (13.6) | |||
| Hospitalization (number, %) | 25 (41) | 3 (23.1) | 28 (37.8) | 0.3467 | ||
| Oxygenotherapy (number, %) | 17 (27.9) | 0 | 17 (23) | 0.0312 | ||
| Resurgence Symptoms | No-R Group (n = 64) (86.5%) | R Group (n = 10) (13.5%) | Total (n = 74) (100%) | p-(Value) | |
|---|---|---|---|---|---|
| Demographic and baseline characteristics | |||||
| Age (mean, extremes, SD) (number, %) | 52.3 (21–91.1) ± 18.2 | 51.6 (29.1–81.7) ± 17.1 | 52.3 (21–91.1) ± 18 | 0.9069 | |
| (18–30) | 8 (12.5) | 1 (10.0) | 9 (12.2) | 0.9868 | |
| (31–40) | 13 (20.3) | 2 (20.0) | 15 (20.3) | ||
| (41–50) | 11 (17.2) | 3 (30.0) | 14 (18.9) | ||
| (51–60) | 8 (12.5) | 1 (10.0) | 9 (12.2) | ||
| (61–70) | 12 (18.8) | 2 (20.0) | 14 (18.9) | ||
| >71 | 12 (18.8) | 1 (10.0) | 13 (17.5) | ||
| Sex (number, %) | Female | 38 (59.4) | 6 (60) | 44 (59.5) | 1 |
| HCWs (number, %) | No | 27 (42.2) | 8 (80) | 35 (47.3) | 0.0396 |
| BMI (kg/m2) | <25 | 32 (50) | 6 (60) | 38 (51.4) | 1 |
| (25–30) | 16 (25) | 2 (20) | 18 (24.3) | ||
| >30 | 16 (25) | 2 (20) | 18 (24.3) | ||
| Comorbidities (number, %) | 32 (50) | 5 (50) | 37 (50) | 1 | |
| Clinical characteristics and outcome | |||||
| Duration of symptoms of SARS-CoV-2 infection (days) (mean, extremes, SD) | 14 (3–51) ± 9.1 | 12.4 (3–21) ± 6.1 | 13.7 (3–51) ± 8.7 | 0.6030 | |
| Hospitalization | 25 (39.1) | 3 (30) | 28 (37.8) | 0.7330 | |
| Duration of hospitalization (days) (mean, extremes, SD) | 3.9 (0–41) ± 8.5 | 3.8 (0–9) ± 12 | 3.5 (0–41) ± 8 | 0.0903 | |
| Initial symptomatology | |||||
| Facial headaches | 20 (31.3) | 7 (70) | 27 (36.5) | 0.0309 | |
| Anxiety | 26 (40.6) | 7 (70) | 33 (44.6) | 0.0992 | |
| Time from symptom onset to first visit (days) (mean, extremes, SD) | 3.8 (1–15) ± 3.2 | 2.2 (1–5) ± 1.4 | 3.6 (1–15) ± 3.1 | 0.0141 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Messin, L.; Puyraveau, M.; Benabdallah, Y.; Lepiller, Q.; Gendrin, V.; Zayet, S.; Klopfenstein, T.; Toko, L.; Pierron, A.; Royer, P.-Y. COVEVOL: Natural Evolution at 6 Months of COVID-19. Viruses 2021, 13, 2151. https://doi.org/10.3390/v13112151
Messin L, Puyraveau M, Benabdallah Y, Lepiller Q, Gendrin V, Zayet S, Klopfenstein T, Toko L, Pierron A, Royer P-Y. COVEVOL: Natural Evolution at 6 Months of COVID-19. Viruses. 2021; 13(11):2151. https://doi.org/10.3390/v13112151
Chicago/Turabian StyleMessin, Louise, Marc Puyraveau, Yousri Benabdallah, Quentin Lepiller, Vincent Gendrin, Souheil Zayet, Timothée Klopfenstein, Lynda Toko, Alix Pierron, and Pierre-Yves Royer. 2021. "COVEVOL: Natural Evolution at 6 Months of COVID-19" Viruses 13, no. 11: 2151. https://doi.org/10.3390/v13112151