
A Multidisciplinary Investigation of the First Chikungunya Virus Outbreak in Matadi in the Democratic Republic of the Congo

 , , ,
, , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
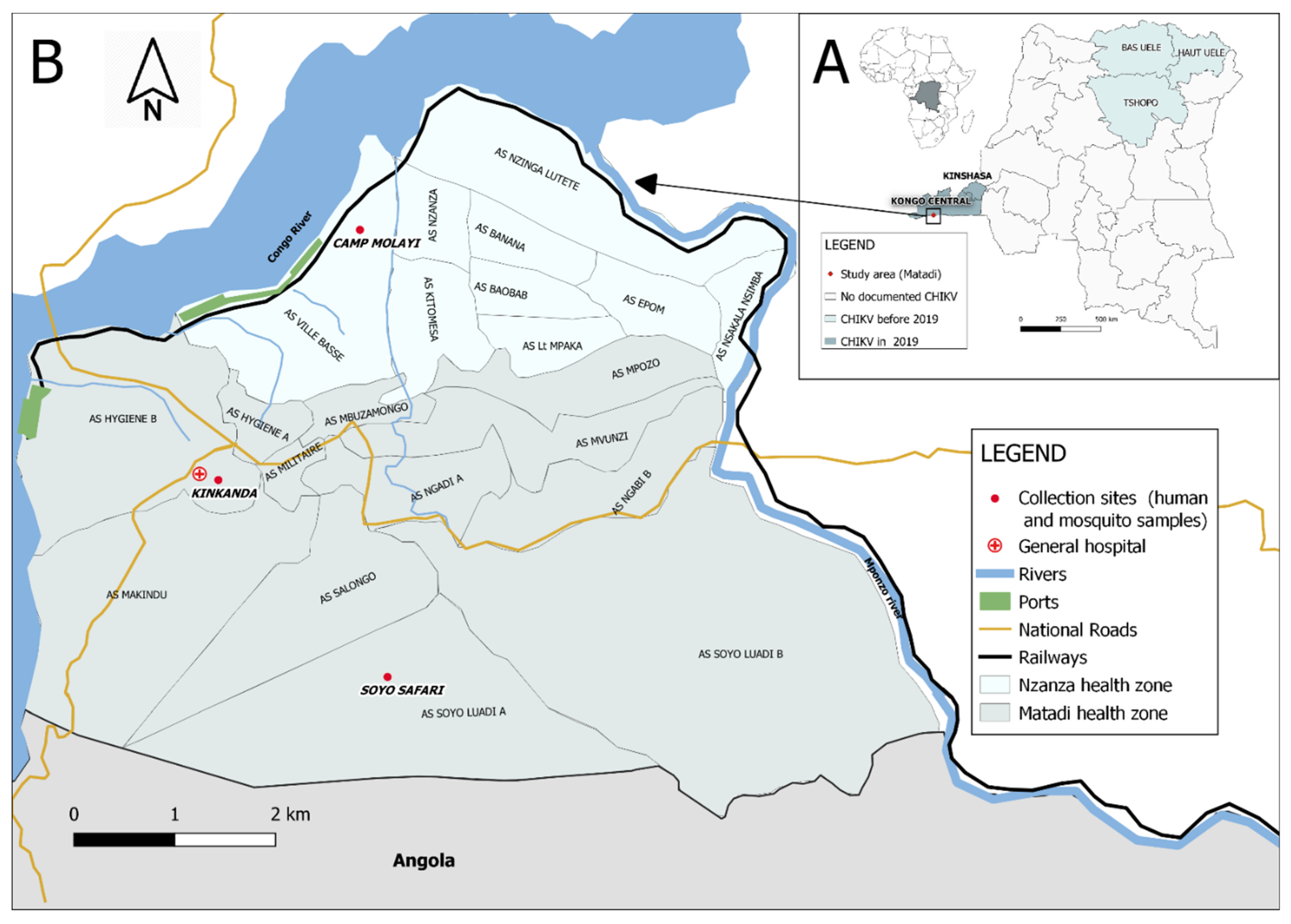
2.1. Outbreak Investigation Setting and Teams
2.2. Data Collection
2.2.1. Epidemiological Investigations
2.2.2. Clinical and Laboratory Investigations
2.2.3. Entomological Investigations
- Container index: number of containers positive for immature stages of Aedes spp. per 100 inspected containers.
- House index: number of houses positive for at least one container with immature stages of Aedes spp. per 100 inspected houses.
- Breteau index: number of containers positive for immature stages of Aedes spp. per 100 inspected houses.
2.2.4. Qualitative Data about Perceptions and Behaviors Related to the Outbreak
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
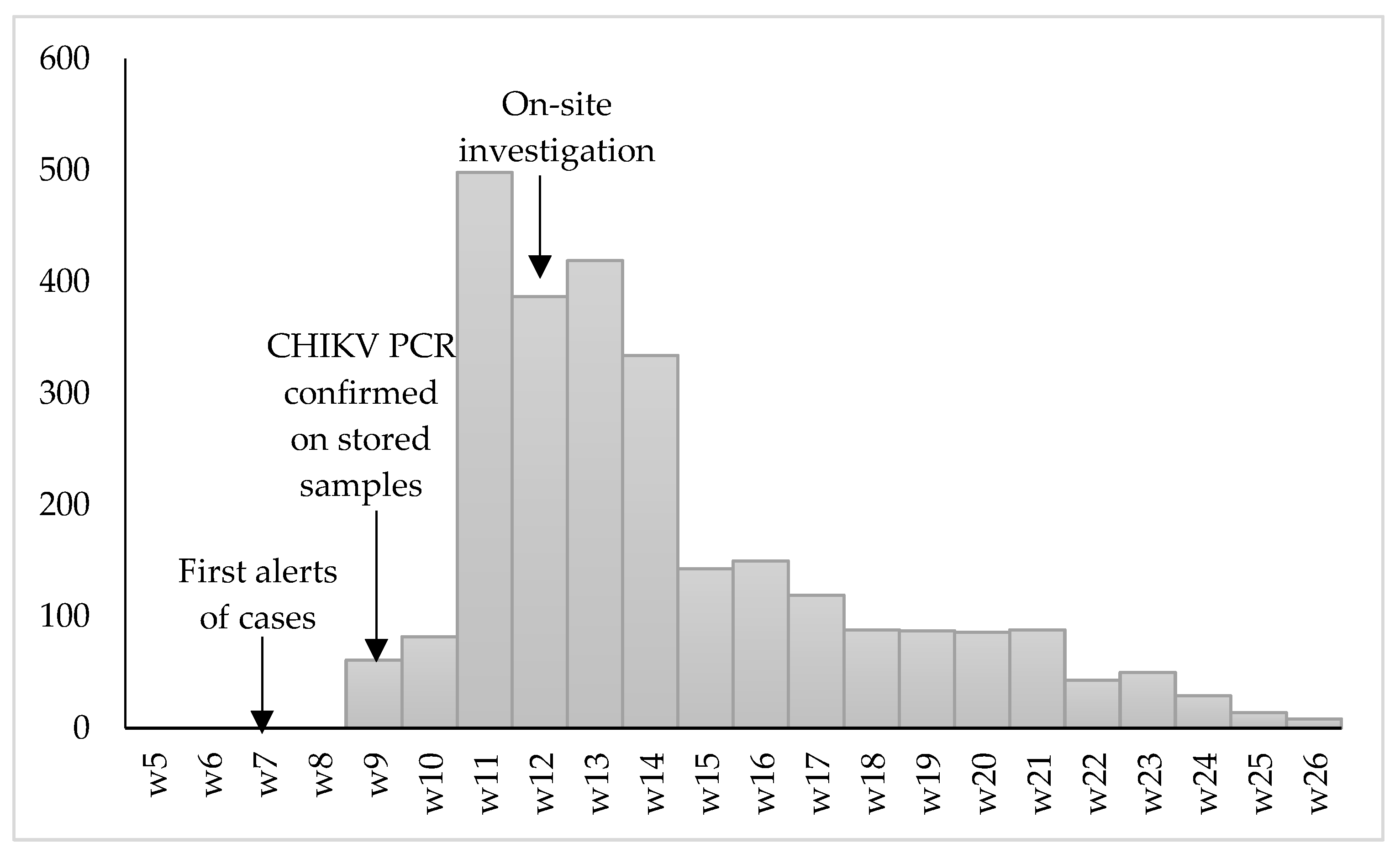
3.1. Epidemiological Description of the Outbreak
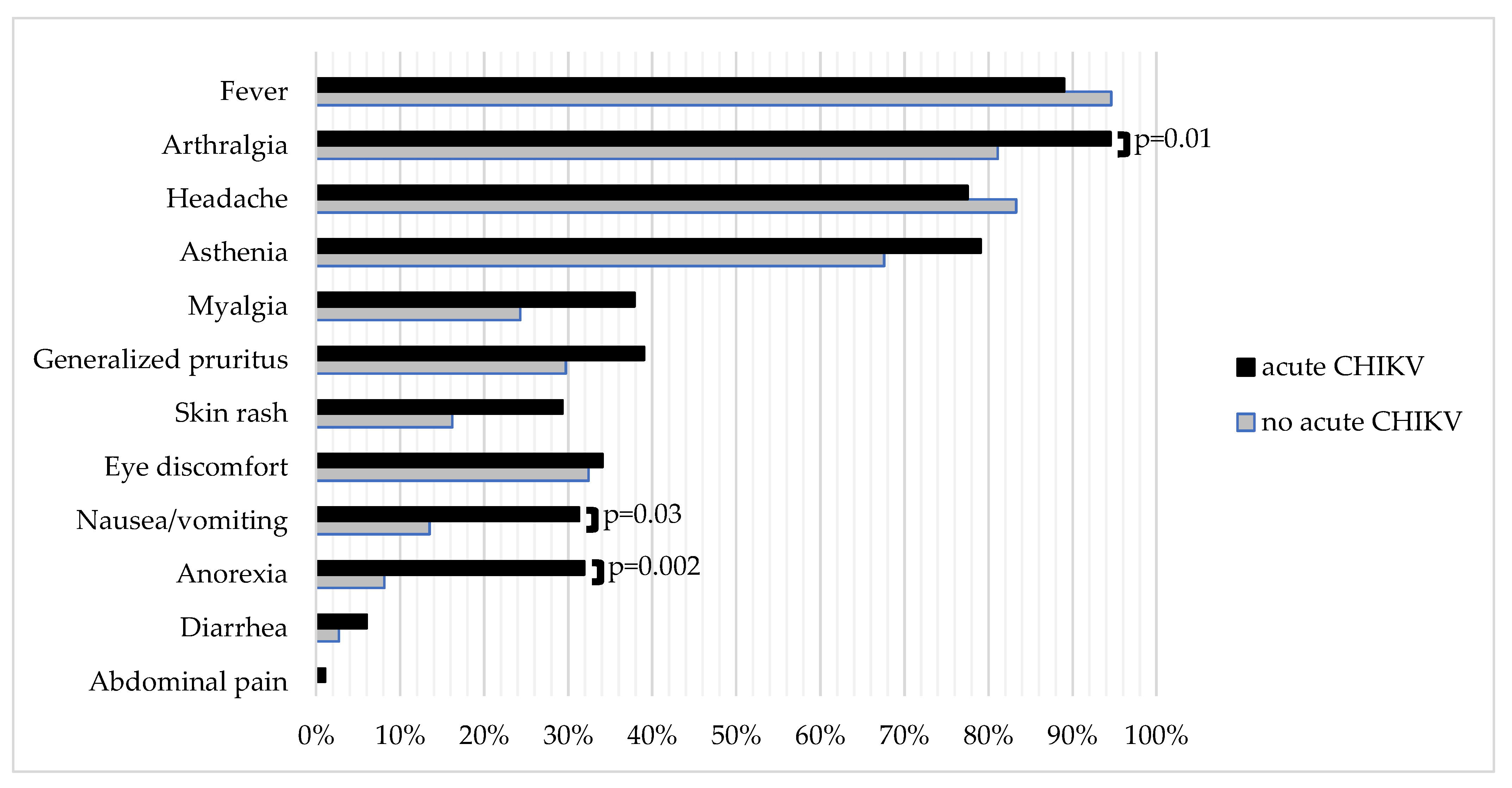
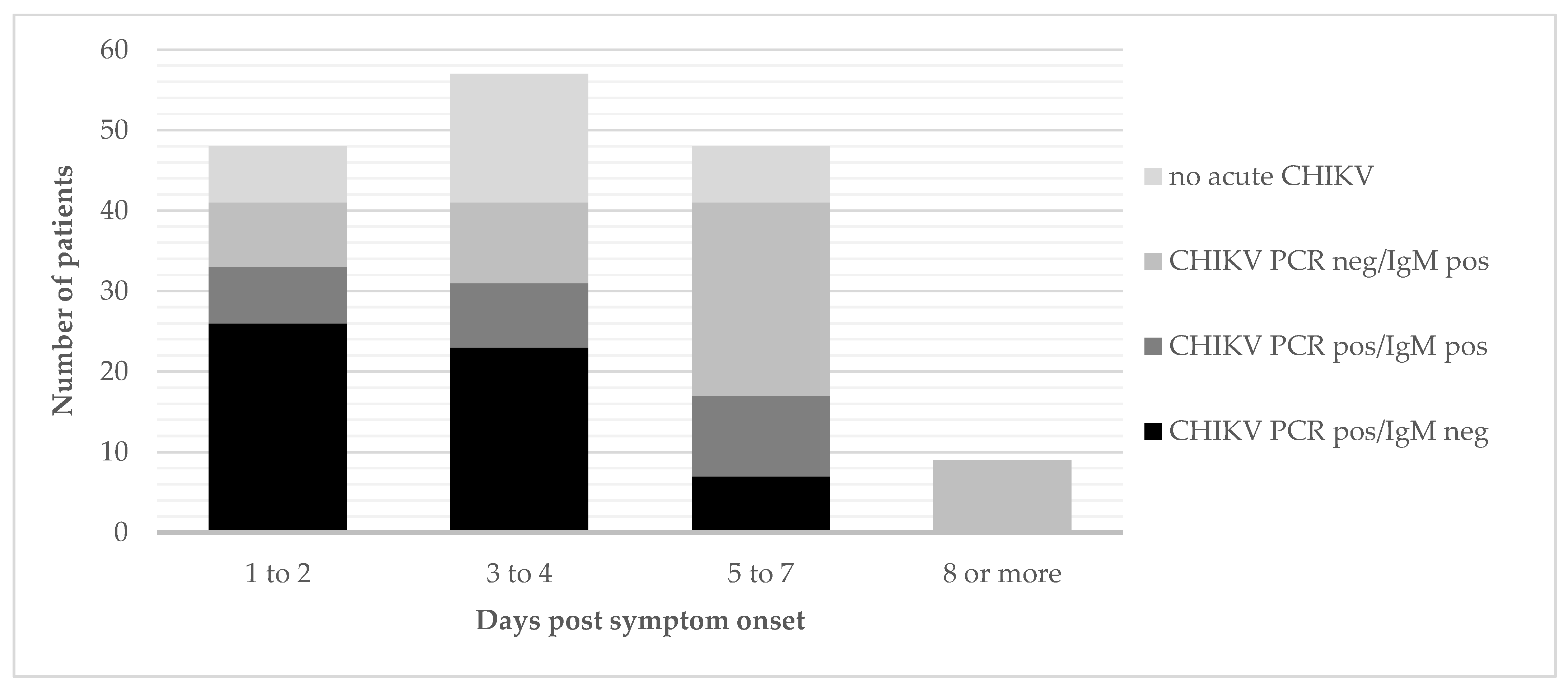
3.2. Clinical Characteristics and Laboratory Results of the Chikungunya Fever Suspected Cases
3.3. Entomological Study
3.4. Perceptions and Behaviors Related to the Outbreak
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Interview guide for patients or their parent (in case of a child)
- Introduction
- The conversations/interviews take place in the setting of a mobile clinic organized in the community in the immediate neighbourhood of the health centre. At the end of the consultation, the patient (and/or his parent in case of a child) is referred for a short interview. The interviews take place in a quiet corner at the same location and are kept short (about 20 to 30 min per person) to avoid overburdening the patients (as they are feeling ill at that moment).
- The researcher introduces himself to the patient, asks him/her how it goes, and explains briefly why and about what he would like to ask some questions and how long this will take. He ends by asking whether the patient is willing to participate in the interview.
- Guiding questions for the interview
- (Questions are meant as prompts, to be used if the topics do not spontaneously arise during the conversation. They will not necessarily be asked in any specific order.)
- Topic 1: Current episode of illness (fever/arthralgia, etc) → to start the conversation
- What type of signs/symptoms do you experience? Since when? Depending on the duration of symptoms, explore what the patient already did/not did in terms of seeking ‘diagnosis and care’ (formal/informal sector)?
- Did you ever experience the same complaints before? What did you think it was before coming here to see the doctor?
- Are there any other persons that you know who have the same complaints?
- What did the doctor explain? What is the diagnosis according to the doctor? What are your thoughts on this? Had you heard before already talking about chikungunya?
- Topic 2: Origin/cause of the outbreak
- Where do you think this disease comes from? What do they say in the community?
- Provide explanation that chikungunya virus is transmitted by mosquitoes that bite during the day, so different ones than the mosquitoes transmitting malaria. Explore whether the patient finds this a plausible explanation, and if not, why not.
- Topic 3: Prevention and clinical management of chikungunya virus disease
- This phenomenon of acute fever with strong pain in the joints is now circulating since a few weeks in the town of Matadi. Did you try to protect yourself from it? If yes, how did you do that?
- Did others in your community do other things to prevent the disease? Can you explain?
- If not yet mentioned spontaneously, ask about the methods mentioned by the health care workers (as the bracelets made from thin twigs).
- What did the other people in your community who had similar symptoms do? Where did they get treatment? Which type of treatment?
- Rounding Up
- The researcher asks whether the patient has any questions he/she would like to ask, or if he would like to come back on anything he/she said previously during the conversation, or if he/she has anything else to add.
- Thank the participant.
References
- Higgs, S.; VanLandingham, D. Chikungunya virus and its mosquito vectors. Vector Borne Zoonotic Dis. 2015, 15, 231–240. [Google Scholar] [CrossRef]
- Bobanga, T.; Moyo, M.; Vulu, F.; Irish, S. First Report of Aedes albopictus (Diptera: Culicidae) in the Democratic Republic of Congo. Afr. Èntomol. 2018, 26, 234–236. [Google Scholar] [CrossRef]
- Thiberville, S.-D.; Moyen, N.; Dupuis-Maguiraga, L.; Nougairede, A.; Gould, E.A.; Roques, P.; de Lamballerie, X. Chikungunya fever: Epidemiology, clinical syndrome, pathogenesis and therapy. Antivir. Res. 2013, 99, 345–370. [Google Scholar] [CrossRef]
- Da Cunha, R.V.; Trinta, K.S. Chikungunya virus: Clinical aspects and treatment—A Review. Memórias Inst. Oswaldo Cruz 2017, 112, 523–531. [Google Scholar] [CrossRef]
- Paixao, E.S.; Rodrigues, L.C.; Costa, M.D.C.N.; Itaparica, M.; Barreto, F.; Gérardin, P.; Teixeira, M.G. Chikungunya chronic disease: A systematic review and meta-analysis. Trans. R. Soc. Trop. Med. Hyg. 2018, 112, 301–316. [Google Scholar] [CrossRef]
- Galatas, B.; Ly, S.; Duong, V.; Baisley, K.; Nguon, K.; Chan, S.; Huy, R.; Ly, S.; Sorn, S.; Som, L.; et al. Long-lasting immune protection and other epidemiological findings after chikungunya emergence in a cambodian rural community, April 2012. PLoS Negl. Trop. Dis. 2016, 10, e0004281. [Google Scholar] [CrossRef]
- Nitatpattana, N.; Kanjanopas, K.; Yoksan, S.; Satimai, W.; Vongba, N.; Langdatsuwan, S.; Nakgoi, K.; Ratchakum, S.; Wauquier, N.; Souris, M.; et al. Long-term persistence of Chikungunya virus neutralizing antibodies in human populations of North Eastern Thailand. Virol. J. 2014, 11, 183. [Google Scholar] [CrossRef] [Green Version]
- Gérardin, P.; Guernier, V.; Perrau, J.; Fianu, A.; Le Roux, K.; Grivard, P.; Michault, A.; De Lamballerie, X.; Flahault, A.; Favier, F. Estimating Chikungunya prevalence in La Réunion Island outbreak by serosurveys: Two methods for two critical times of the epidemic. BMC Infect. Dis. 2008, 8, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staples, J.E.; Breiman, R.F.; Powers, A.M. Chikungunya fever: An epidemiological review of a re-emerging infectious disease. Clin. Infect. Dis. 2009, 49, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Yactayo, S.; Staples, J.E.; Millot, V.; Cibrelus, L.; Ramon-Pardo, P. Epidemiology of Chikungunya in the Americas. J. Infect. Dis. 2016, 214, S441–S445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pezzi, L.; Reusken, C.; Weaver, S.; Drexler, J.F.; Busch, M.; LaBeaud, A.; Diamond, M.; Vasilakis, N.; Drebot, M.; Siqueira, A.; et al. GloPID-R report on Chikungunya, O’nyong-nyong and Mayaro virus, Part I: Biological diagnostics. Antivir. Res. 2019, 166, 66–81. [Google Scholar] [CrossRef] [PubMed]
- Natrajan, M.S.; Rojas, A.; Waggoner, J.J. Beyond fever and pain: Diagnostic methods for chikungunya virus. J. Clin. Microbiol. 2019, 57, e00350-19. [Google Scholar] [CrossRef] [Green Version]
- Osterrieth, P.; Blanes-Ridaura, G. Research on the Chikungunya virus in the Belgian Congo. I. Isolation of the virus in upper Uele. Ann. Soc. Belg.Med. Trop. 1960, 40, 199–203. [Google Scholar]
- Osterrieth, P.; Rathe, E.; Deleplanque-Liegeois, P. Simultaneous isolation of the yellow fever and Chikungunya viruses at Bili (Haut-Uele, Belgian Congo). Ann. Soc. Belg. Med. Trop. 1961, 41, 207–212. [Google Scholar]
- Nur, Y.A.; Tuynman, W.; Copra, C.; Groen, J.; Heuvelmans, H.; Osterhaus, A.D. An outbreak of West Nile fever among migrants in Kisangani, Democratic Republic of Congo. Am. J. Trop. Med. Hyg. 1999, 61, 885–888. [Google Scholar] [CrossRef] [Green Version]
- Muyembe-Tamfum, J.J.; Peyrefitte, C.N.; Yogolelo, R.; Basisya, E.M.; Koyange, D.; Pukuta, E.; Mashako, M.; Tolou, H.; Durand, J.P. Epidemic of Chikungunya virus in 1999 and 200 in the Democratic Republic of the Congo. Med. Trop. Rev. Corps Sante Colon. 2003, 63, 637–638. [Google Scholar]
- Malekani, M.J.; McCollum, A.; Monroe, B.P.; Malekani, V.D.; Mulumba, M.L.; Tshilenge, C.G.; Kondas, A.; Doty, J.B.; Okitolonda, E.W.; Muyembe, J.J.; et al. Cas de dengue chez les patients suspects de Chikungunya à Kinshasa. Ann. Afr. Méd. 2014, 7, 2. [Google Scholar]
- Radio Okapi. February 2019. Available online: https://www.radiookapi.net/2019/02/14/actualite/sante/la-maladie-virale-de-chikungunya-declaree-en-rdc (accessed on 28 March 2021).
- Selhorst, P.; Makiala-Mandanda, S.; De Smet, B.; Mariën, J.; Anthony, C.; Binene-Mbuka, G.; De Weggheleire, A.; Ilombe, G.; Kinganda-Lusamaki, E.; Pukuta-Simbu, E.; et al. Molecular Characterization of Chikungunya Virus during the 2019 Outbreak in the Democratic Republic of the Congo. Emerg. Microbes Infect. 2020, 9, 1–25. [Google Scholar] [CrossRef]
- Mbanzulu, K.M.; Mboera, L.E.G.; Luzolo, F.K.; Wumba, R.; Misinzo, G.; Kimera, S.I. Mosquito-borne viral diseases in the Democratic Republic of the Congo: A review. Parasites Vectors 2020, 13, 1–11. [Google Scholar] [CrossRef]
- WHO country profile DRC—Malaria. Available online: https://www.who.int/malaria/publications/country-profiles/profile_cod_en.pdf?ua=1 (accessed on 5 August 2020).
- Panning, M.; Grywna, K.; Van Esbroeck, M.; Emmerich, P.; Drosten, C. Chikungunya fever in travelers returning to europe from the indian ocean region, 2006. Emerg. Infect. Dis. 2008, 14, 416–422. [Google Scholar] [CrossRef]
- Huits, R.; De Kort, J.; Berg, R.V.D.; Chong, L.; Tsoumanis, A.; Eggermont, K.; Bartholomeeusen, K.; Arien, K.K.; Jacobs, J.; Van Esbroeck, M.; et al. Chikungunya virus infection in Aruba: Diagnosis, clinical features and predictors of post-chikungunya chronic polyarthralgia. PLoS ONE 2018, 13, e0196630. [Google Scholar] [CrossRef] [PubMed]
- Clancy, A.; Crowley, B.; Niesters, H.; Herra, C. The development of a qualitative real-time RT-PCR assay for the detection of hepatitis C virus. Eur. J. Clin. Microbiol. Infect. Dis. 2008, 27, 1177–1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walter Reed Mosquito Identification Keys. Available online: https://www.wrbu.si.edu/vectorspecies/mosquitoes/albopictus (accessed on 22 September 2021).
- Tezzo, F.W.; Fasine, S.; Zola, E.M.; Marquetti, M.D.C.; Mbuka, G.B.; Ilombe, G.; Takasongo, R.M.; Smitz, N.; Bisset, J.A.; Van Bortel, W.; et al. High Aedes spp. larval indices in Kinshasa, Democratic Republic of Congo. Parasites Vectors 2021, 14, 1–13. [Google Scholar] [CrossRef]
- Mariën, J.; Laurent, N.; Smitz, N.; Gombeer, S. First observation of Aedes albopictus in the Tshuapa province (Boende) of the Democratic Republic of the Congo. bioRxiv 2021. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control: New Edition. 2009. Available online: https://apps.who.int/iris/handle/10665/44188 (accessed on 15 September 2020).
- Biggerstaff, B. PooledInfRate, Version 4.0: A Microsoft Office Add-in to Compute Prevalence Estimates from Pooled Samples; Fort Collins Centers Dis Control Prevention: Collins, CO, USA, 2009. [Google Scholar]
- Nekwa, A. Kongo Central: Le Bois d’or ne Lutte Pas Contre le Chikungunya. Available online: https://www.infobascongo.net/beta/2019/03/24/kongo-centralle-bois-dor-ne-lutte-pas-contre-le-chikungunia/ (accessed on 5 August 2020).
- Simon, F.; Javelle, E.; Cabie, A.; Bouquillard, E.; Troisgros, O.; Gentile, G.; Leparc-Goffart, I.; Hoen, B.; Gandjbakhch, F.; Rene-Corail, P.; et al. French guidelines for the management of chikungunya (acute and persistent presentations). November 2014. Méd. Mal. Infect. 2015, 45, 243–263. [Google Scholar] [CrossRef]
- Johnson, B.W.; Russell, B.J.; Goodman, C.H. Laboratory diagnosis of chikungunya virus infections and commercial sources for diagnostic assays. J. Infect. Dis. 2016, 214, S471–S474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ingoba, L.L.; Adedoja, A.; Peko, S.M.; Vairo, F.; Haider, N.; Kock, R.; Ippolito, G.; Zumla, A.; Nguimbi, E.; Pallerla, S.R.; et al. Diagnosis of Chikungunya virus in febrile patients from a malaria holoendemic area. Int. J. Infect. Dis. 2021, 109, 247–252. [Google Scholar] [CrossRef]
- Bower, H.; el Karsany, M.; Adam, A.A.A.H.; Idriss, M.I.; Alzain, M.A.; Alfakiyousif, M.E.A.; Mohamed, R.; Mahmoud, I.; Albadri, O.; Mahmoud, S.A.A.; et al. “Kankasha” in Kassala: A prospective observational cohort study of the clinical characteristics, epidemiology, genetic origin, and chronic impact of the 2018 epidemic of Chikungunya virus infection in Kassala, Sudan. PLoS Negl. Trop. Dis. 2021, 15, e0009387. [Google Scholar] [CrossRef]
- Huits, R.; Okabayashi, T.; Cnops, L.; Barbé, B.; Berg, R.V.D.; Bartholomeeusen, K.; Ariën, K.K.; Jacobs, J.; Bottieau, E.; Nakayama, E.E.; et al. Diagnostic accuracy of a rapid E1-antigen test for chikungunya virus infection in a reference setting. Clin. Microbiol. Infect. 2018, 24, 78–81. [Google Scholar] [CrossRef] [Green Version]
- Fischer, C.; Jo, W.K.; Haage, V.; Moreira-Soto, A.; de Oliveira-Filho, E.F.; Drexler, J.F. Challenges towards serologic diagnostics of emerging arboviruses. Clin. Microbiol. Infect. 2021, 27, 1221–1229. [Google Scholar] [CrossRef]
- UNITAID. Fever Diagnostic Technology Landscape, 1st edition, February 2018. Available online: https://unitaid.org/assets/Fever_diagnostic_technology_and_market_landscape.pdf (accessed on 28 March 2021).
- Dariano, D.F.; Bockarie, A.S.; Taitt, C.R.; Yasuda, C.; Jacobsen, K.H.; Stenger, D.A.; Lamin, J.M.; Bockarie, M.J.; Bangura, U.; Ansumana, R.; et al. Surveillance of Vector-Borne Infections (Chikungunya, Dengue, and Malaria) in Bo, Sierra Leone, 2012–2013. Am. J. Trop. Med. Hyg. 2017, 97, 1151–1154. [Google Scholar] [CrossRef] [PubMed]
- Ansumana, R.; Jacobsen, K.H.; Leski, T.A.; Covington, A.L.; Bangura, U.; Hodges, M.H.; Lin, B.; Bockarie, A.S.; Lamin, J.M.; Bockarie, M.J.; et al. Reemergence of Chikungunya Virus in Bo, Sierra Leone. Emerg. Infect. Dis. 2013, 19, 1108–1110. [Google Scholar] [CrossRef]
- Sow, A.; Faye, O.; Diallo, M.; Diallo, D.; Chen, R.; Faye, O.; Diagne, C.T.; Guerbois, M.; Weidmann, M.; Ndiaye, Y.; et al. Chikungunya Outbreak in Kedougou, Southeastern Senegal in 2009–2010. Open Forum Infect. Dis. 2018, 5, ofx259. [Google Scholar] [CrossRef] [PubMed]
- Buchwald, A.G.; Hayden, M.H.; Dadzie, S.K.; Paull, S.H.; Carlton, E. Aedes-borne disease outbreaks in West Africa: A call for enhanced surveillance. Acta Trop. 2020, 209, 105468. [Google Scholar] [CrossRef] [PubMed]
- Raulino, R.; Thaurignac, G.; Butel, C.; Villabona-Arenas, C.J.; Foe, T.; Loul, S.; Ndimbo-Kumugo, S.-P.; Mbala-Kingebeni, P.; Makiala-Mandanda, S.; Ahuka-Mundeke, S.; et al. Multiplex detection of antibodies to Chikungunya, O’nyong-nyong, Zika, Dengue, West Nile and Usutu viruses in diverse non-human primate species from Cameroon and the Democratic Republic of Congo. PLoS Negl. Trop. Dis. 2021, 15, e0009028. [Google Scholar] [CrossRef] [PubMed]
- Fritz, M.; Taty, R.T.; Portella, C.; Guimbi, C.; Mankou, M.; Leroy, E.M.; Becquart, P. Re-emergence of chikungunya in the Republic of the Congo in 2019 associated with a possible vector-host switch. Int. J. Infect. Dis. 2019, 84, 99–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honório, N.A.; Wiggins, K.; Eastmond, B.; Câmara, D.C.P.; Alto, B.W. Experimental vertical transmission of chikungunya virus by brazilian and florida aedes albopictus populations. Viruses 2019, 11, 353. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Missing Values | Total N = 220 | Acute CHIKV N = 183 | No Acute CHIKV N = 37 | p-Value | |
|---|---|---|---|---|---|
| Gender | 0 | 0.70 | |||
| Male | 84 (38.2) | 69 (37.7) | 15 (40.5) | ||
| Female | 136 (61.8) | 114 (62,3) | 22 (59.5) | ||
| Age (years): median (IQR) | 7 | 23 (10–38) | 23 (11–39) | 20 (6–33) | 0.05 |
| Age groups | 7 | 0.02 | |||
| <5 years | 18 (8.5) | 10 (5.7) | 8 (21.6) | ||
| 5–10 years | 27 (12.7) | 21 (11.9) | 6 (16.2) | ||
| 10–15 years | 32 (15.0) | 30 (17.1) | 2 (5.4) | ||
| 15–55 years | 126 (59.2) | 106 (60.2) | 20 (54.1) | ||
| ≥55 years | 10 (4.7) | 9 (5.1) | 1 (2.7) | ||
| Days of symptoms: median (IQR) | 30 | 3 (2–5) | 3 (2–5) | 3 (2.5–4) | 0.96 |
| Sites | 0 | 0.52 | |||
| Mobile clinic Soyo Safari, Matadi HZ | 82 (37.3) | 66 (36) | 16 (43) | ||
| Mobile clinic Camp Molayi, Nzanza HZ | 80 (36.4) | 66 (36) | 14 (38) | ||
| Outpatient consultations | 58 (26.3) | 51 (28) | 7 (19) | ||
| Malaria | 0 | 0.26 | |||
| Positive Malaria RDT | 44 (20) | 34 (18.6) | 10 (27.0) |
| Location | Stage | Ae. albopictus (n) | Ae. aegypti (n) | Container Index (%) 1 | House Index (%) 2 | Breteau Index 3 |
|---|---|---|---|---|---|---|
| Soyo Safari | Adult | 41 | 0 | |||
| Larvae | 307 | 0 | 19 | 49 | 85 | |
| Kinkanda | Adult | 410 | 0 | |||
| Larvae | 91 | 7 | 11 | 31 | 32 | |
| Camp Molayi | Adult | 44 | 4 | |||
| Larvae | 346 | 23 | 9 | 5 | 5 |
| Place | Stage | CHIKV Positive/Total Pools | ML Estimated Minimum Infection Rate (95%CI) | Number of Mosquitoes per Pool 2 | Ct-Values of Positive Pool(s) 3 |
|---|---|---|---|---|---|
| Soyo Safari | Adult 1 | 1/1 | not possible | (41) | (19) |
| Larva | 2/6 | 0.82 % [0.15–2.93] | (50,50,20,50,50,50) | (43,37) | |
| Kinkanda | Adult male | 2/4 | 1.31 % [0.25–5.26] | (50,50,50,30) | (37,20) |
| Adult female | 2/5 | 0.93 % [0.18–3.27] | (50,50,50,50,30) | (29,17) | |
| Larva | 0/2 | 0.00 % [0.00–2.38] | (53,35) | ||
| Camp Molayi | Adult male | 0/0 | - | - | - |
| Adult female | 1/1 | not possible | (44) | (17) | |
| Larva | 0/7 | 0.00 % [0.00–0.88] | (50,50,50,50,50,50,46) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Weggheleire, A.; Nkuba-Ndaye, A.; Mbala-Kingebeni, P.; Mariën, J.; Kindombe-Luzolo, E.; Ilombe, G.; Mangala-Sonzi, D.; Binene-Mbuka, G.; De Smet, B.; Vogt, F.; et al. A Multidisciplinary Investigation of the First Chikungunya Virus Outbreak in Matadi in the Democratic Republic of the Congo. Viruses 2021, 13, 1988. https://doi.org/10.3390/v13101988
De Weggheleire A, Nkuba-Ndaye A, Mbala-Kingebeni P, Mariën J, Kindombe-Luzolo E, Ilombe G, Mangala-Sonzi D, Binene-Mbuka G, De Smet B, Vogt F, et al. A Multidisciplinary Investigation of the First Chikungunya Virus Outbreak in Matadi in the Democratic Republic of the Congo. Viruses. 2021; 13(10):1988. https://doi.org/10.3390/v13101988
Chicago/Turabian StyleDe Weggheleire, Anja, Antoine Nkuba-Ndaye, Placide Mbala-Kingebeni, Joachim Mariën, Esaie Kindombe-Luzolo, Gillon Ilombe, Donatien Mangala-Sonzi, Guillaume Binene-Mbuka, Birgit De Smet, Florian Vogt, and et al. 2021. "A Multidisciplinary Investigation of the First Chikungunya Virus Outbreak in Matadi in the Democratic Republic of the Congo" Viruses 13, no. 10: 1988. https://doi.org/10.3390/v13101988