
Impact of APRF+ in Combination with Autogenous Fibroblasts on Release Growth Factors, Collagen, and Proliferation and Migration of Gingival Fibroblasts: An In Vitro Study

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Culture and A-PRF+-Based Matrices
2.2. Assessment of Growth Factor Release from Fibroblasts Alone, A-PRF+ Alone, and A-PRF+ with Fibroblasts
2.3. The Quantification of Growth Factors with Enzyme-Linked Immunosorbent Assay (ELISA)
2.4. Quantification of Soluble Collagen Using the Sircol™ Colorimetric Test
2.5. Preparation of the Conditioned Media
2.6. Cell Migration Assay
2.7. Cell Viability Assay
2.8. Statistical Analysis
3. Results
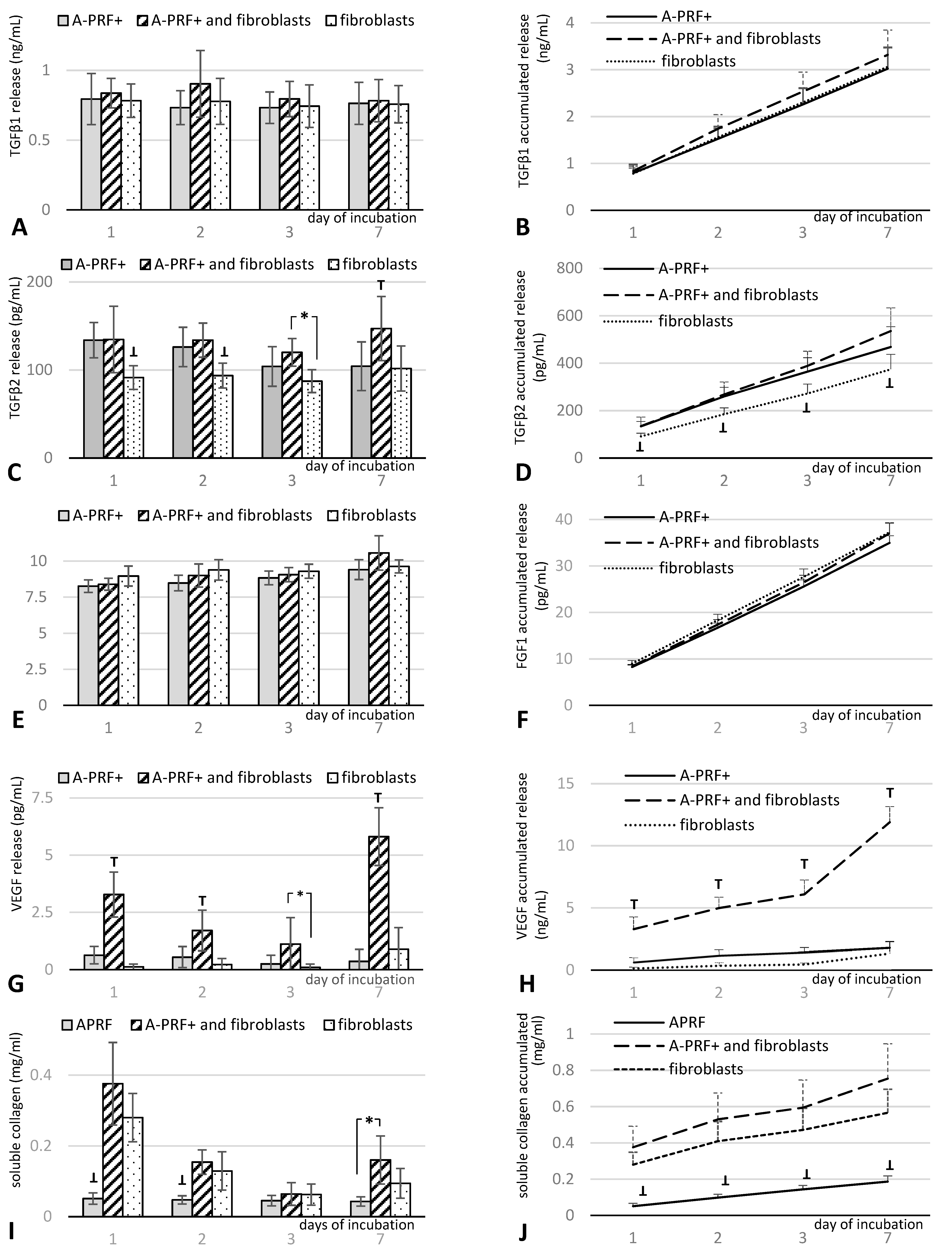
3.1. Growth Factor Release from A-PRF+ Alone, A-PRF+ with Fibroblasts, and Fibroblasts Alone
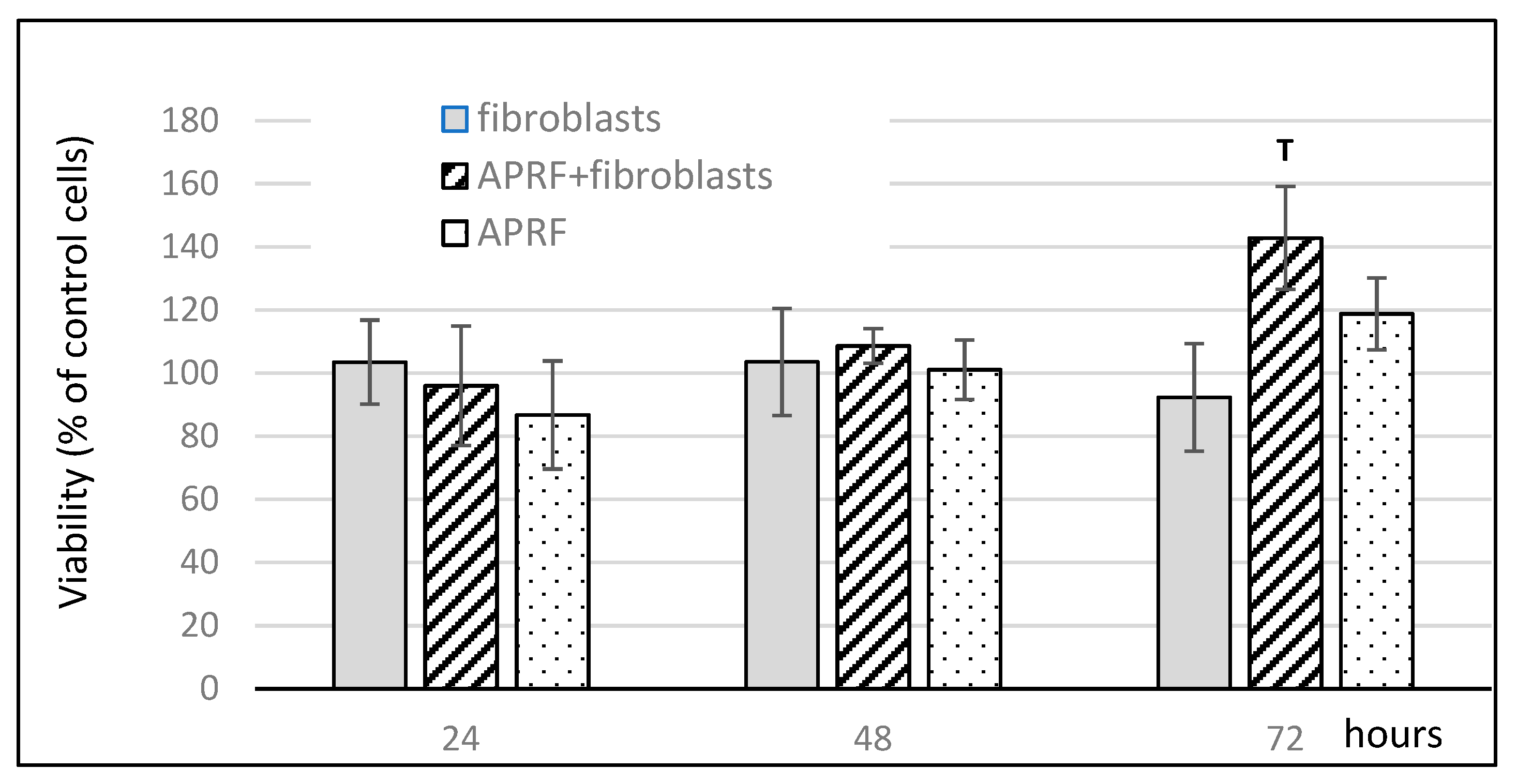
3.2. Influence of Proteins Released from A-PRF+ Combined with Fibroblasts on Cell Viability
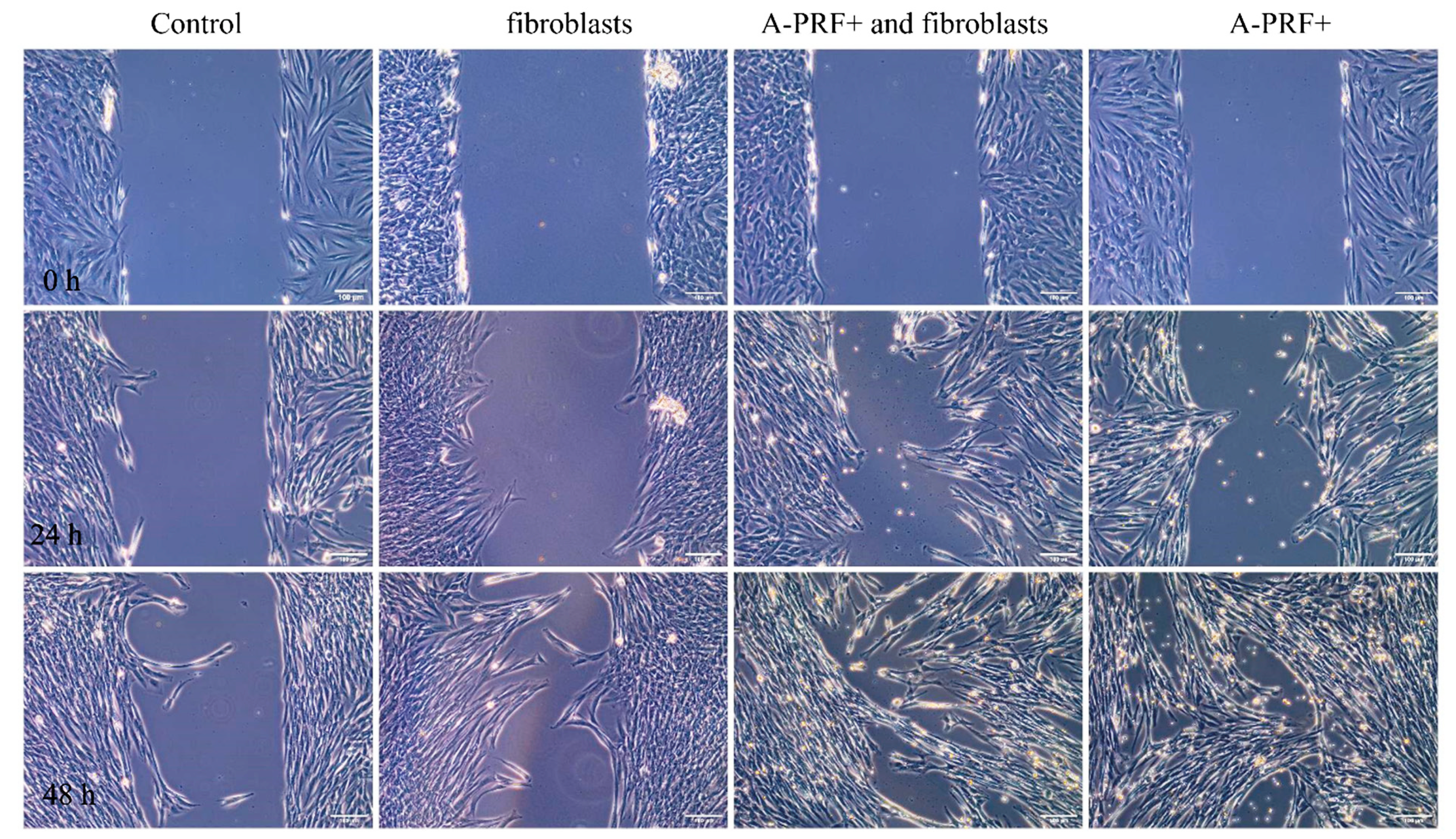
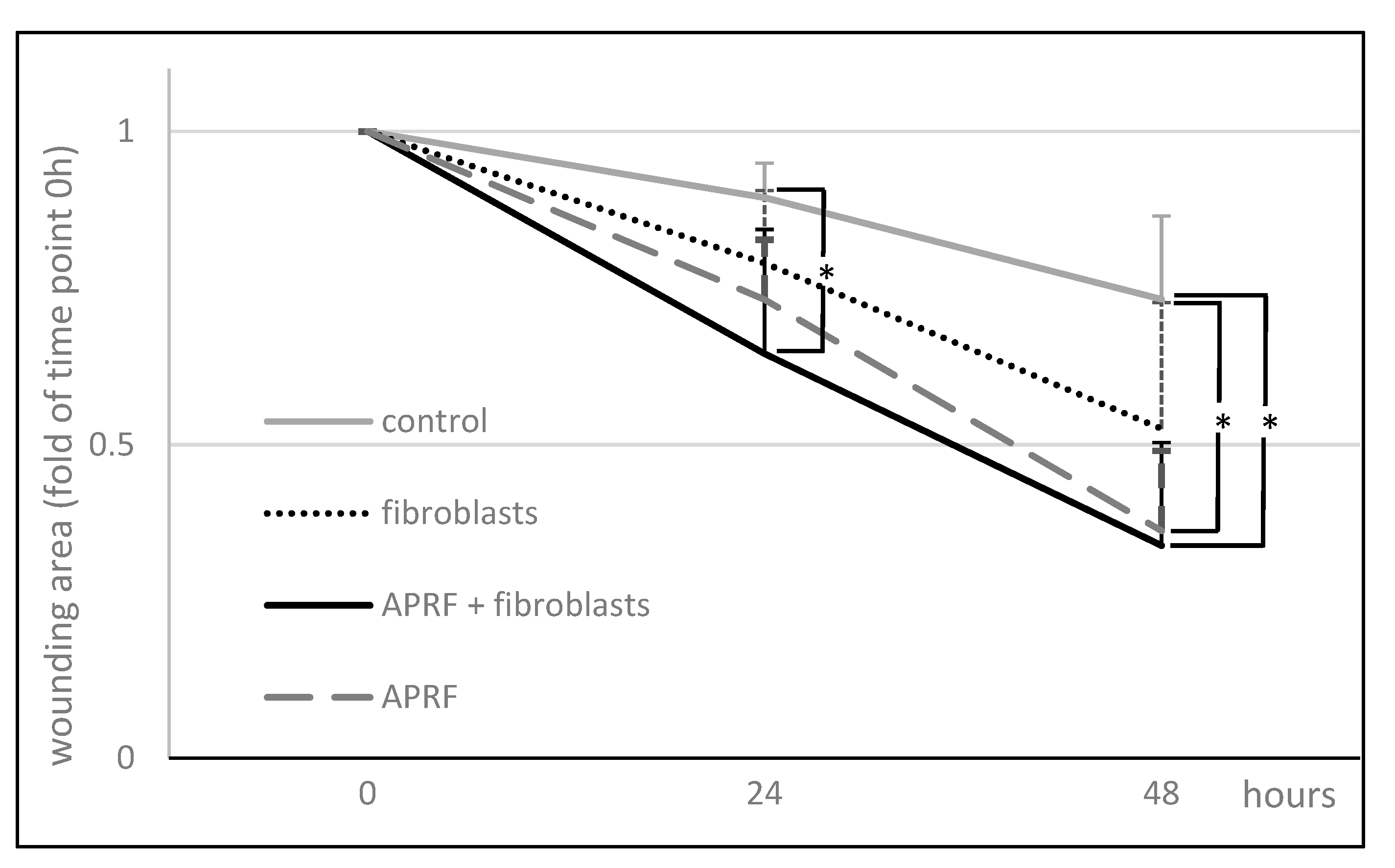
3.3. Enhanced Wound Healing Potential of Primary Human Gingival Fibroblasts Induced with Proteins Released from A-PRF+
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miron, R.J.; Bishara, M.; Choukroun, J. Basics of Platelet-Rich Fibrin Therapy. Dent. Today 2017, 36, 74–76. [Google Scholar] [PubMed]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.J.; Mouhyi, J.; Gogly, B. Platelet-Rich Fibrin (PRF): A Second-Generation Platelet Concentrate. Part I: Technological Concepts and Evolution. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2006, 101, e37–e44. [Google Scholar] [CrossRef]
- Karimi, K.; Rockwell, H. The Benefits of Platelet-Rich Fibrin. Facial Plast. Surg. Clin. N. Am. 2019, 27, 331–340. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.J.; Mouhyi, J.; Gogly, B. Platelet-Rich Fibrin (PRF): A Second-Generation Platelet Concentrate. Part II: Platelet-Related Biologic Features. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e45–e50. [Google Scholar] [CrossRef]
- Demling, R.H. The Role of Anabolic Hormones for Wound Healing in Catabolic States. J. Burn. Wounds 2005, 4, e2. [Google Scholar]
- Miron, R.J.; Zucchelli, G.; Pikos, M.A.; Salama, M.; Lee, S.; Guillemette, V.; Fujioka-Kobayashi, M.; Bishara, M.; Zhang, Y.; Wang, H.L.; et al. Use of Platelet-Rich Fibrin in Regenerative Dentistry: A Systematic Review. Clin. Oral Investig. 2017, 21, 1913–1927. [Google Scholar] [CrossRef] [PubMed]
- Marrelli, M.; Tatullo, M. Influence of PRF in the Healing of Bone and Gingival Tissues. Clinical and Histological Evaluations. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 1958–1962. [Google Scholar]
- Ghanaati, S.; Booms, P.; Orlowska, A.; Kubesch, A.; Lorenz, J.; Rutkowski, J.; Les, C.; Sader, R.; Kirkpatrick, C.J.; Choukroun, J. Advanced Platelet-Rich Fibrin: A New Concept for Cell- Based Tissue Engineering by Means of Inflammatory Cells. J. Oral Implantol. 2014, 40, 679–689. [Google Scholar] [CrossRef]
- Steller, D.; Herbst, N.; Pries, R.; Juhl, D.; Hakim, S.G. Positive Impact of Platelet-Rich Plasma and Platelet-Rich Fibrin on Viability, Migration and Proliferation of Osteoblasts and Fibroblasts Treated with Zoledronic Acid. Sci. Rep. 2019, 9, 8310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujioka-Kobayashi, M.; Miron, R.J.; Hernandez, M.; Kandalam, U.; Zhang, Y.; Choukroun, J. Optimized Platelet-Rich Fibrin With the Low-Speed Concept: Growth Factor Release, Biocompatibility, and Cellular Response. J. Periodontol. 2017, 88, 112–121. [Google Scholar] [CrossRef]
- Choukroun, J.; Ghanaati, S. Reduction of Relative Centrifugation Force within Injectable Platelet-Rich-Fibrin (PRF) Concentrates Advances Patients’ Own Inflammatory Cells, Platelets and Growth Factors: The First Introduction to the Low Speed Centrifugation Concept. Eur. J. Trauma Emerg. Surg. 2018, 44, 87–95. [Google Scholar] [CrossRef] [Green Version]
- el Bagdadi, K.; Kubesch, A.; Yu, X.; Al-Maawi, S.; Orlowska, A.; Dias, A.; Booms, P.; Dohle, E.; Sader, R.; Kirkpatrick, C.J.; et al. Reduction of Relative Centrifugal Forces Increases Growth Factor Release within Solid Platelet-Rich-Fibrin (PRF)-Based Matrices: A Proof of Concept of LSCC (Low Speed Centrifugation Concept). Eur. J. Trauma Emerg. Surg. 2019, 45, 467–479. [Google Scholar] [CrossRef] [Green Version]
- Dohan Ehrenfest, D.M.; de Peppo, G.M.; Doglioli, P.; Sammartino, G. Slow Release of Growth Factors and Thrombospondin-1 in Choukroun’s Platelet-Rich Fibrin (PRF): A Gold Standard to Achieve for All Surgical Platelet Concentrates Technologies. Growth Factors 2009, 27, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Bian, H.; Qi, S.; Xu, Y.; Tang, J.; Li, T.; Liu, X. Effects of Basic Fibroblast Growth Factor on the Expression of Extracellular Matrix and Matrix Metalloproteinase-1 in Wound Healing. Clin. Exp. Dermatol. 2008, 33, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Pitzurra, L.; Jansen, I.D.C.; Vries, T.J.; Hoogenkamp, M.A.; Loos, B.G. Effects of L-PRF and A-PRF+ on Periodontal Fibroblasts in in Vitro Wound Healing Experiments. J. Periodontal Res. 2020, 55, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E. Platelet-Rich Plasma (PRP): What Is PRP and What Is Not PRP? Implant Dent. 2001, 10, 225–228. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Chen, J.; Kirsner, R. Pathophysiology of Acute Wound Healing. Clin. Dermatol. 2007, 25, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Gurtner, G.C.; Werner, S.; Barrandon, Y.; Longaker, M.T. Wound Repair and Regeneration. Nature 2008, 453, 314–321. [Google Scholar] [CrossRef]
- Chaussain, C.; Septier, D.; Bonnefoix, M.; Lecolle, S.; Lebreton-Decoster, C.; Coulomb, B.; Pellat, B.; Godeau, G. Human Dermal and Gingival Fibroblasts in a Three-Dimensional Culture: A Comparative Study on Matrix Remodeling. Clin. Oral Investig. 2002, 6, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Dominiak, M.; Łysiak-Drwal, K.; Saczko, J.; Kunert-Keil, C.; Gedrange, T. The Clinical Efficacy of Primary Culture of Human Fibroblasts in Gingival Augmentation Procedures-A Preliminary Report. Ann. Anat. 2012, 194, 502–507. [Google Scholar] [CrossRef]
- Rognoni, E.; Pisco, A.O.; Hiratsuka, T.; Sipilä, K.H.; Belmonte, J.M.; Mobasseri, S.A.; Philippeos, C.; Dilão, R.; Watt, F.M. Fibroblast State Switching Orchestrates Dermal Maturation and Wound Healing. Mol. Syst. Biol. 2018, 14, e8174. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.E.; Foster, D.S.; Longaker, M.T. Management of Chronic Wounds—2018. JAMA—J. Am. Med. Assoc. 2018, 320, 1481–1482. [Google Scholar] [CrossRef] [PubMed]
- Knychalska-Karwan, Z. Anatomia i fizjologia narządu żucia u ludzi w podeszłym wieku. In Stomatologia wieku podeszłego, 1st ed.; Knychalska-Karwan, Z., Ed.; Czelej: Lublin, Polska, 2005; pp. 1–21. [Google Scholar]
- Pham, T.A.V.; Nguyen, H.T.; Nguyen, M.T.; Trinh, V.N.; Tran, N.Y.; Ngo, L.T.; Tran, H.L. Platelet-Rich Fibrin Influences on Proliferation and Migration of Human Gingival Fibroblasts. Int. J. Exp. Dent. Sci. 2016, 5, 83–88. [Google Scholar] [CrossRef]
- Mudalal, M.; Wang, Z.; Mustafa, S.; Liu, Y.; Wang, Y.; Yu, J.; Wang, S.; Sun, X.; Zhou, Y. Effect of Leukocyte-Platelet Rich Fibrin (L-PRF) on Tissue Regeneration and Proliferation of Human Gingival Fibroblast Cells Cultured Using a Modified Method. Tissue Eng. Regen. Med. 2021, 18, 895–904. [Google Scholar] [CrossRef]
- Dor, Y.; Djonov, V.; Keshet, E. Induction of Vascular Networks in Adult Organs: Implications to Proangiogenic Therapy. Ann. N. Y. Acad. Sci. 2003, 995, 208–216. [Google Scholar] [CrossRef]
- Cabaro, S.; D’Esposito, V.; Gasparro, R.; Borriello, F.; Granata, F.; Mosca, G.; Passaretti, F.; Sammartino, J.C.; Beguinot, F.; Sammartino, G.; et al. White Cell and Platelet Content Affects the Release of Bioactive Factors in Different Blood-Derived Scaffolds. Platelets 2018, 29, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Hinz, B. The Role of Myofibroblasts in Wound Healing. Curr. Res. Transl. Med. 2016, 64, 171–177. [Google Scholar] [CrossRef]
- Arora, P.D.; Narani, N.; McCulloch, C.A.G. The Compliance of Collagen Gels Regulates Transforming Growth Factor-β Induction of α-Smooth Muscle Actin in Fibroblasts. Am. J. Pathol. 1999, 154, 871–882. [Google Scholar] [CrossRef]
- Hata, Y.; Kawanabe, H.; Hisanaga, Y.; Taniguchi, K.; Ishikawa, H. Effects of Basic Fibroblast Growth Factor Administration on Vascular Changes in Wound Healing of Rat Palates. Cleft Palate-Craniofac. J. 2008, 45, 63–72. [Google Scholar] [CrossRef]
- Oda, Y.; Kagami, H.; Ueda, M. Accelerating Effects of Basic Fibroblast Growth Factor on Wound Healing of Rat Palatal Mucosa. J. Oral Maxillofac. Surg. 2004, 62, 73–80. [Google Scholar] [CrossRef]
- Lin, Z.; Nica, C.; Sculean, A.; Asparuhova, M.B. Enhanced Wound Healing Potential of Primary Human Oral Fibroblasts and Periodontal Ligament Cells Cultured on Four Different Porcine-Derived Collagen Matrices. Materials 2020, 13, 3819. [Google Scholar] [CrossRef]
- Coelho, N.M.; Arora, P.D.; van Putten, S.; Boo, S.; Petrovic, P.; Lin, A.X.; Hinz, B.; McCulloch, C.A. Discoidin Domain Receptor 1 Mediates Myosin-Dependent Collagen Contraction. Cell Rep. 2017, 18, 1774–1790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masuki, H.; Okudera, T.; Watanebe, T.; Suzuki, M.; Nishiyama, K.; Okudera, H.; Nakata, K.; Uematsu, K.; Su, C.-Y.; Kawase, T. Growth Factor and Pro-Inflammatory Cytokine Contents in Platelet-Rich Plasma (PRP), Plasma Rich in Growth Factors (PRGF), Advanced Platelet-Rich Fibrin (A-PRF), and Concentrated Growth Factors (CGF). Int. J. Implant Dent. 2016, 2, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, W.F.; Inoue-Yokoo, T.; Tan, K.S.; Lai, M.I.; Sugiyama, D. Hematopoietic Cell Differentiation from Embryonic and Induced Pluripotent Stem Cells. Stem Cell Res. Ther. 2013, 4, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sterczała, B.; Chwiłkowska, A.; Szwedowicz, U.; Kobielarz, M.; Chwiłkowski, B.; Dominiak, M. Impact of APRF+ in Combination with Autogenous Fibroblasts on Release Growth Factors, Collagen, and Proliferation and Migration of Gingival Fibroblasts: An In Vitro Study. Materials 2022, 15, 796. https://doi.org/10.3390/ma15030796
Sterczała B, Chwiłkowska A, Szwedowicz U, Kobielarz M, Chwiłkowski B, Dominiak M. Impact of APRF+ in Combination with Autogenous Fibroblasts on Release Growth Factors, Collagen, and Proliferation and Migration of Gingival Fibroblasts: An In Vitro Study. Materials. 2022; 15(3):796. https://doi.org/10.3390/ma15030796
Chicago/Turabian StyleSterczała, Barbara, Agnieszka Chwiłkowska, Urszula Szwedowicz, Magdalena Kobielarz, Bartłomiej Chwiłkowski, and Marzena Dominiak. 2022. "Impact of APRF+ in Combination with Autogenous Fibroblasts on Release Growth Factors, Collagen, and Proliferation and Migration of Gingival Fibroblasts: An In Vitro Study" Materials 15, no. 3: 796. https://doi.org/10.3390/ma15030796