
Cross-Contamination Risk of Dental Tray Adhesives: An In Vitro Study

 and
and
Abstract
:1. Introduction
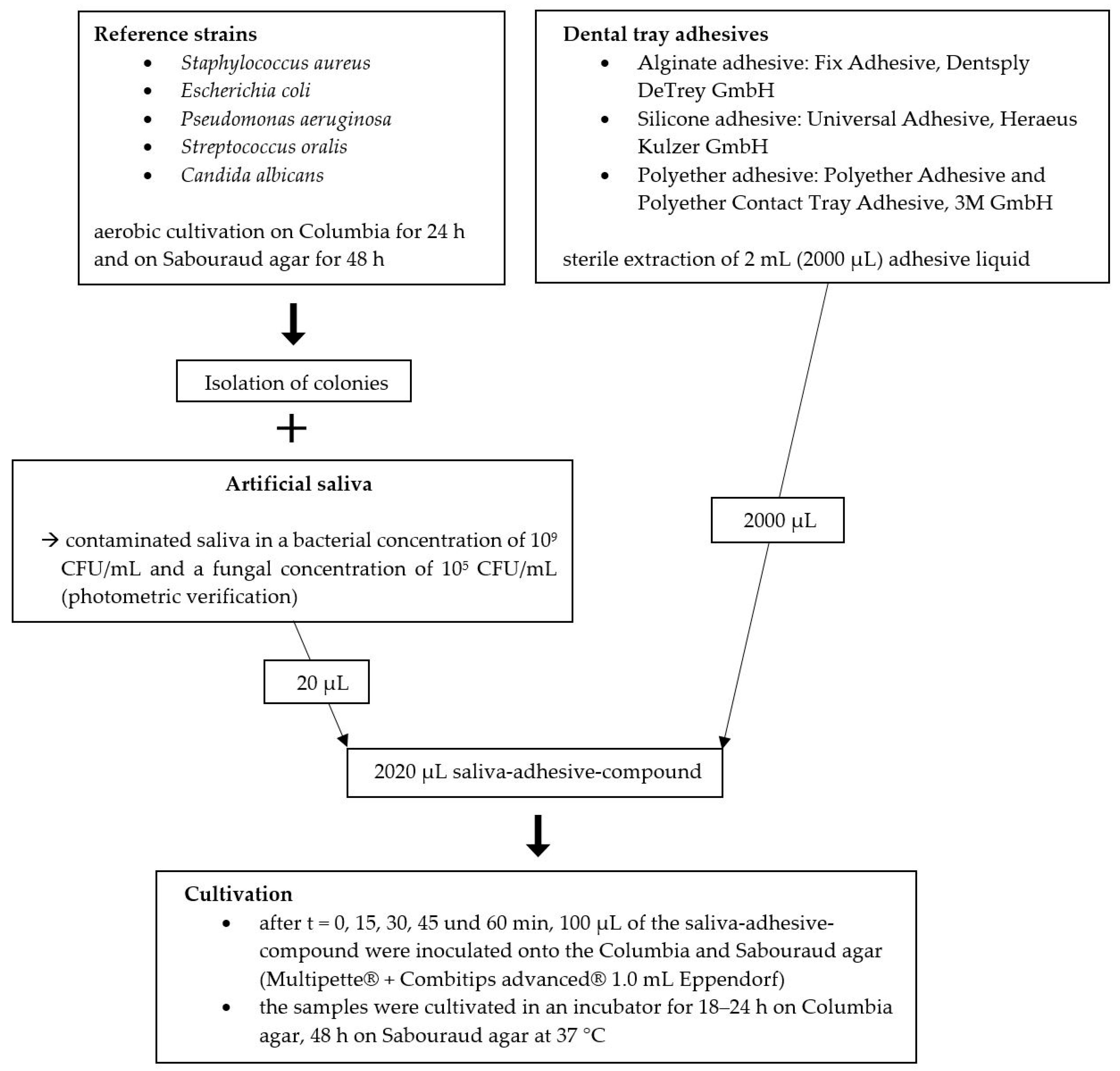
2. Materials and Methods
- Staphylococcus aureus (ATCC 29213);
- Escherichia coli (ATCC 25922);
- Pseudomonas aeruginosa (ATCC 29213);
- Streptococcus oralis (DSM 20627);
- Candida albicans (ATCC 90028).
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Summary of Infection Prevention Practices in Dental Settings: Basic Expectations for Safe Car; Centers for Disease Control and Prevention, US Dept of Health and Human Services: Atlanta, GA, USA, 2021. Available online: https://www.cdc.gov/oralhealth/infectioncontrol/pdf/safe-care2.pdf (accessed on 8 July 2021).
- Centers for Disease Control and Prevention. Guidelines for Infection Control in Dental Health Care Settings; 2003. Available online: https://www.cdc.gov/mmwr/PDF/rr/rr5217.pdf (accessed on 8 July 2021).
- Cristina, M.L.; Spagnolo, A.M.; Sartini, M.; Dallera, M.; Ottria, G.; Perdelli, F.; Orlando, P. Investigation of organizational and hygiene features in dentistry: A pilot study. J. Prev. Med. Hyg. 2009, 50, 175–180. [Google Scholar] [CrossRef]
- Puttaiah, R.; Cederberg, R.; Youngblood, D. A pragmatic approach towards single-use-disposable devices in dentistry. Bull. Group. Int. Rech. Sci. Stomatol. Odontol. 2006, 47, 18–26. [Google Scholar] [PubMed]
- Bundeszahnärztekammer. Statistisches Jahrbuch 2019/2020; Kassenzahnärztliche Bundesvereinigung: Cologne, Germany, 2019. [Google Scholar]
- Ahlholm, P.; Sipilä, K.; Vallittu, P.; Jakonen, M.; Kotiranta, U. Digital Versus Conventional Impressions in Fixed Prosthodontics: A Review. J. Prosthodont. 2018, 27, 35–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sivaramakrishnan, G.; Alsobaiei, M.; Sridharan, K. Patient preference and operating time for digital versus conventional impressions: A network meta-analysis. Aust. Dent. J. 2020, 65, 58–69. [Google Scholar] [CrossRef] [PubMed]
- Herman, D.A. A study of the antimicrobial properties of impression tray adhesives. J. Prosthet. Dent. 1993, 69, 102–105. [Google Scholar] [CrossRef]
- White, J.T.; Jordan, R.D. Infection control during elastomeric impressions. J. Prosthet. Dent. 1987, 58, 711–712. [Google Scholar] [CrossRef]
- Bensel, T.; Pollak, R.; Stimmelmayr, M.; Hey, J. Disinfection effect of dental impression tray adhesives. Clin. Oral Investig. 2013, 17, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Schierz, O.; Müller, H.; Stingu, C.S.; Hahnel, S.; Rauch, A. Dental tray adhesives and their role as potential transmission medium for microorganisms. Clin. Exp. Dent. Res. 2021. [Google Scholar] [CrossRef]
- Nabert-Georgi, C.; Rodloff, A.C.; Jentsch, H.; Reissmann, D.R.; Schaumann, R.; Stingu, C.S. Influence of oral bacteria on adhesion of Streptococcus mutans and Streptococcus sanguinis to dental materials. Clin. Exp. Dent. Res. 2018, 4, 72–77. [Google Scholar] [CrossRef]
- Rosentritt, M.; Behr, M.; Bürgers, R.; Feilzer, A.J.; Hahnel, S. In vitro adherence of oral streptococci to zirconia core and veneering glass-ceramics. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 91, 257–263. [Google Scholar] [CrossRef]
- Zhou, X.; Li, Y. Atlas of Oral Microbiology: From Healthy Microflora to Disease; Elsevier: Amsterdam, The Netherlands; Academic Press: Amsterdam, The Netherlands; New York, NY, USA, 2015; ISBN 978-0-12-802234-4. [Google Scholar]
- Krishnan, K.; Chen, T.; Paster, B.J. A practical guide to the oral microbiome and its relation to health and disease. Oral Dis. 2017, 23, 276–286. [Google Scholar] [CrossRef] [Green Version]
- Rupf, S.; Jentsch, H.; Eschrich, K. Lebensraum Mundhöhle: Mikroorganismen und orale Erkrankungen. Biol. Unserer Zeit 2007, 37, 51–59. [Google Scholar] [CrossRef]
- Rutala, W.; Weber, D.; The Healthcare Infection Control Practices Advisory Committee. Guideline for Disinfection and Sterilization in Healthcare Facilities. Available online: https://www.cdc.gov/infectioncontrol/pdf/guidelines/disinfection-guidelines-H.pdf (accessed on 8 July 2021).
- Renson, A.; Jones, H.E.; Beghini, F.; Segata, N.; Zolnik, C.P.; Usyk, M.; Moody, T.U.; Thorpe, L.; Burk, R.; Waldron, L.; et al. Sociodemographic variation in the oral microbiome. Ann. Epidemiol. 2019, 35, 73–80.e2. [Google Scholar] [CrossRef] [Green Version]
- Hibbing, M.E.; Fuqua, C.; Parsek, M.R.; Peterson, S.B. Bacterial competition: Surviving and thriving in the microbial jungle. Nat. Rev. Microbiol. 2010, 8, 15–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujikawa, H.; Munakata, K.; Sakha, M.Z. Development of a competition model for microbial growth in mixed culture. Biocontrol Sci. 2014, 19, 61–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basson, N.J. Competition for glucose between Candida albicans and oral bacteria grown in mixed culture in a chemostat. J. Med. Microbiol. 2000, 49, 969–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asgeirsson, H.; Thalme, A.; Weiland, O. Staphylococcus aureus bacteraemia and endocarditis—Epidemiology and outcome: A review. Infect. Dis. 2018, 50, 175–192. [Google Scholar] [CrossRef] [PubMed]
- Muthukrishnan, G.; Masters, E.A.; Daiss, J.L.; Schwarz, E.M. Mechanisms of Immune Evasion and Bone Tissue Colonization That Make Staphylococcus aureus the Primary Pathogen in Osteomyelitis. Curr. Osteoporos. Rep. 2019, 17, 395–404. [Google Scholar] [CrossRef]
- Foster, T.J. Antibiotic resistance in Staphylococcus aureus. Current status and future prospects. FEMS Microbiol. Rev. 2017, 41, 430–449. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, D.; Borges, A.; Simões, M. Staphylococcus aureus Toxins and Their Molecular Activity in Infectious Diseases. Toxins 2018, 10, 252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomes, T.A.T.; Elias, W.P.; Scaletsky, I.C.A.; Guth, B.E.C.; Rodrigues, J.F.; Piazza, R.M.F.; Ferreira, L.C.S.; Martinez, M.B. Diarrheagenic Escherichia coli. Braz. J. Microbiol. 2016, 47 (Suppl. 1), 3–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azam, M.W.; Khan, A.U. Updates on the pathogenicity status of Pseudomonas aeruginosa. Drug Discov. Today 2019, 24, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Gow, N.A.R.; Yadav, B. Microbe Profile: Candida albicans: A shape-changing, opportunistic pathogenic fungus of humans. Microbiology 2017, 163, 1145–1147. [Google Scholar] [CrossRef] [PubMed]
- Bertolini, M.; Dongari-Bagtzoglou, A. The Relationship of Candida albicans with the Oral Bacterial Microbiome in Health and Disease. Adv. Exp. Med. Biol. 2019, 1197, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Sabino-Silva, R.; Jardim, A.C.G.; Siqueira, W.L. Coronavirus COVID-19 impacts to dentistry and potential salivary diagnosis. Clin. Oral Investig. 2020, 24, 1619–1621. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Microorganism | t0 | t15 | t30 | t0 vs. t15 | t15 vs. t30 | |||
|---|---|---|---|---|---|---|---|---|
| Median in CFU/mL | Min; Max | Medianin CFU/mL | Min; Max | Median in CFU/mL | Min; Max | p-Value 1 | p-Value 1 | |
| Staphylococcus aureus | ||||||||
| Fix | 0 | 0; 0 | 0 | 0; 0 | 0 | 0; 0 | n.a. | n.a. |
| Universal | 15 | 0; 1887 | 0 | 0; 0 | 0 | 0; 0 | <0.001 | <0.001 |
| Polyether | 328 | 10; 2223 | 0 | 0; 20 | 0 | 0; 0 | <0.001 | <0.001 |
| Polyether Contact Tray | 3000 | 220; 3000 | 0 | 0; 0 | 0 | 0; 10 | <0.001 | <0.001 |
| Candida albicans | ||||||||
| Fix | 0 | 0; 0 | 0 | 0; 0 | 0 | 0; 0 | n.a. | n.a. |
| Universal | 0 | 0; 0 | 0 | 0; 0 | 0 | 0; 0 | n.a. | n.a. |
| Polyether | 0 | 0; 10 | 0 | 0; 0 | 0 | 0; 0 | 0.317 | n.a. |
| Polyether Contact Tray | 0 | 0; 0 | 0 | 0; 0 | 0 | 0; 0 | n.a. | n.a. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paczkowski, I.; Stingu, C.S.; Hahnel, S.; Rauch, A.; Schierz, O. Cross-Contamination Risk of Dental Tray Adhesives: An In Vitro Study. Materials 2021, 14, 6138. https://doi.org/10.3390/ma14206138
Paczkowski I, Stingu CS, Hahnel S, Rauch A, Schierz O. Cross-Contamination Risk of Dental Tray Adhesives: An In Vitro Study. Materials. 2021; 14(20):6138. https://doi.org/10.3390/ma14206138
Chicago/Turabian StylePaczkowski, Isabel, Catalina S. Stingu, Sebastian Hahnel, Angelika Rauch, and Oliver Schierz. 2021. "Cross-Contamination Risk of Dental Tray Adhesives: An In Vitro Study" Materials 14, no. 20: 6138. https://doi.org/10.3390/ma14206138