
Local Effects of a 1940 nm Thulium-Doped Fiber Laser and a 1470 nm Diode Laser on the Pulmonary Parenchyma: An Experimental Study in a Pig Model

 ,
,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Lasers
2.2. Experimental Animals
2.3. Animal Preparation and Surgery
2.4. Post-Mortem Examination
2.5. Histopathology
2.6. Statistics
3. Results
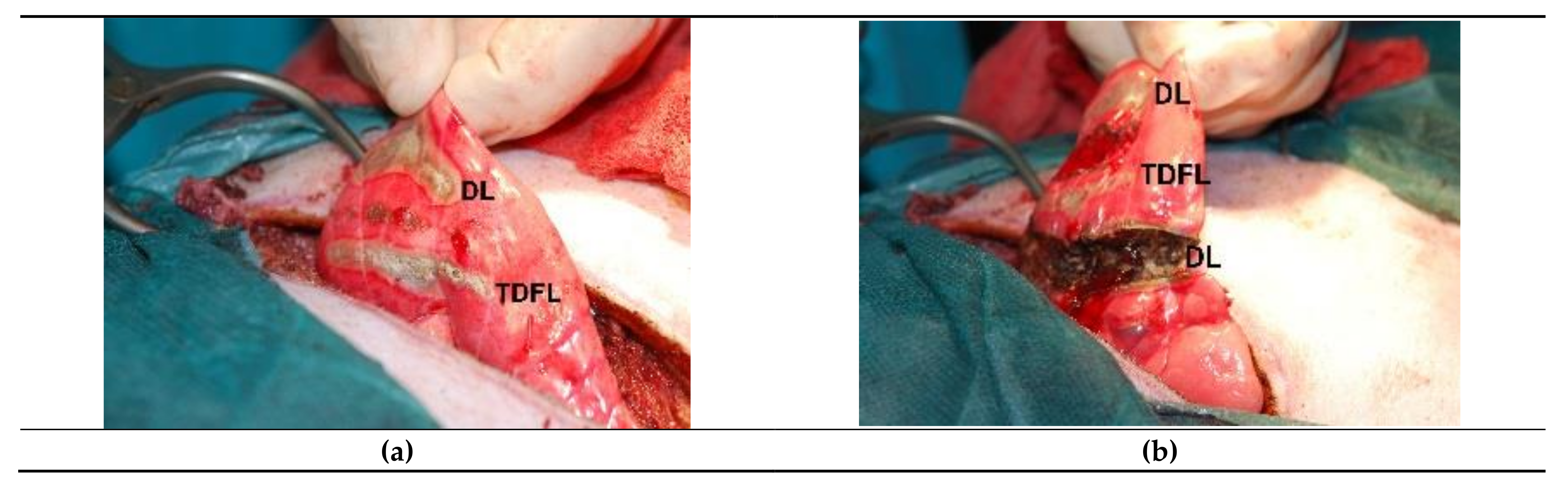
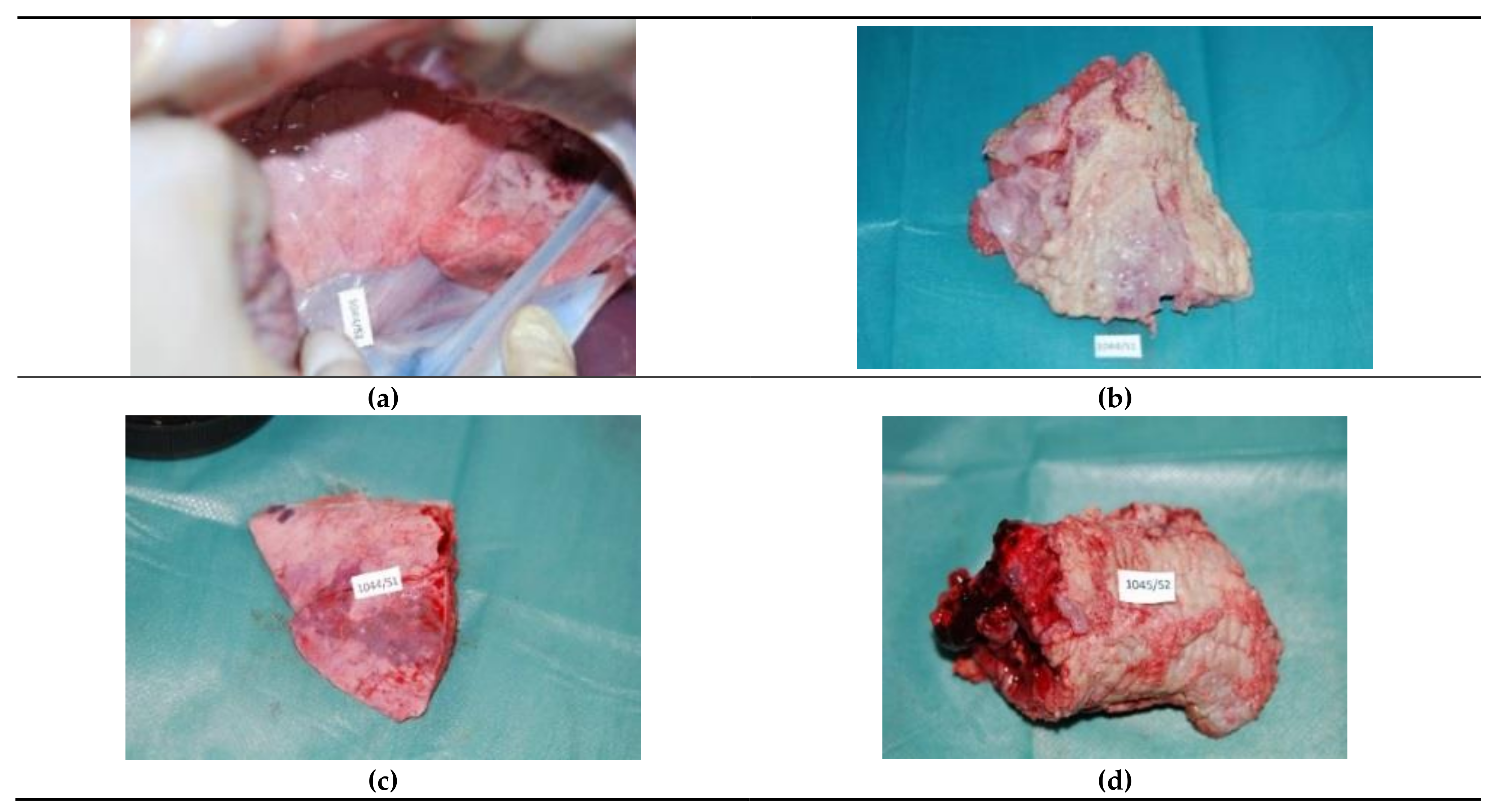
3.1. Intraoperative and Post-Mortem Examination
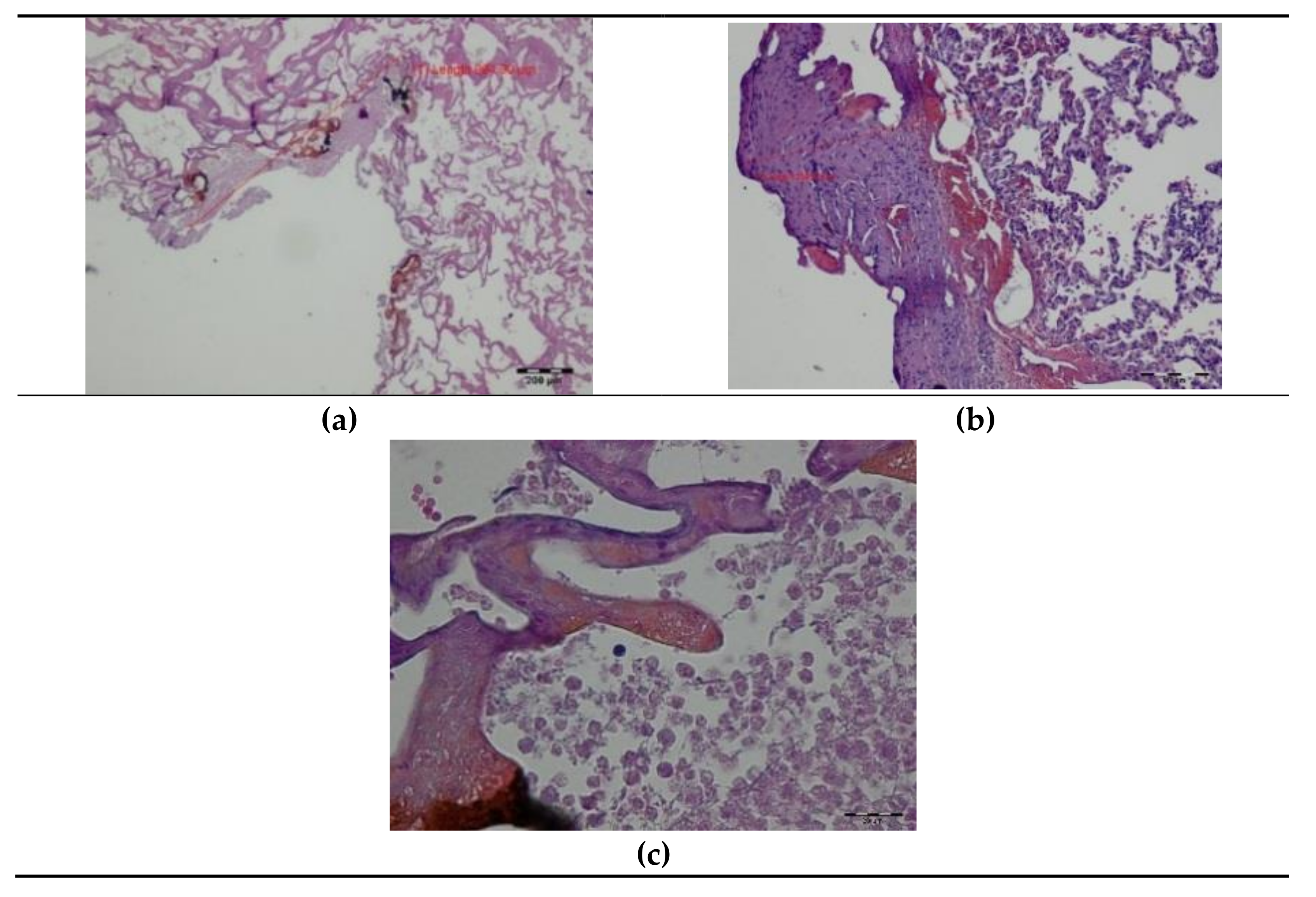
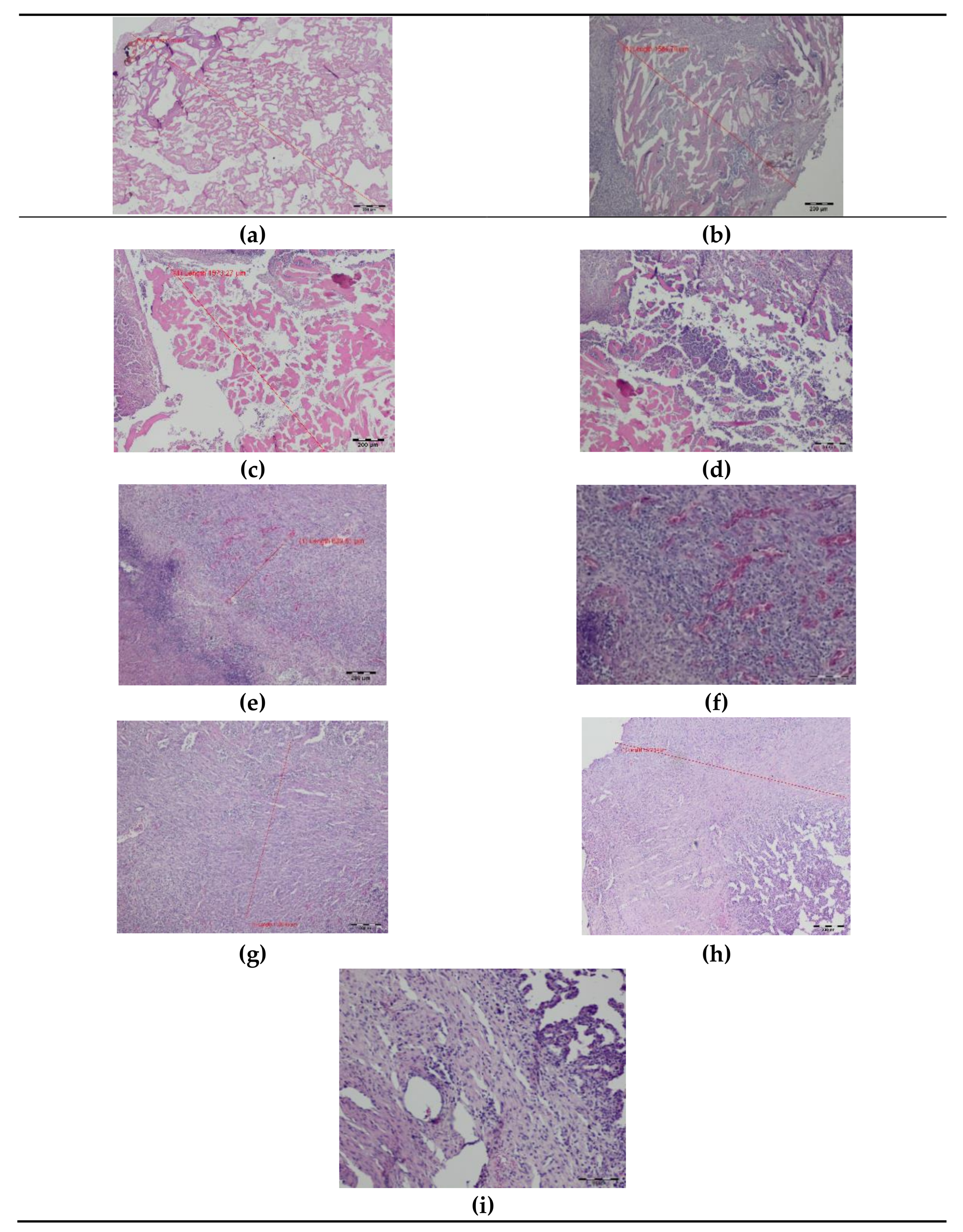
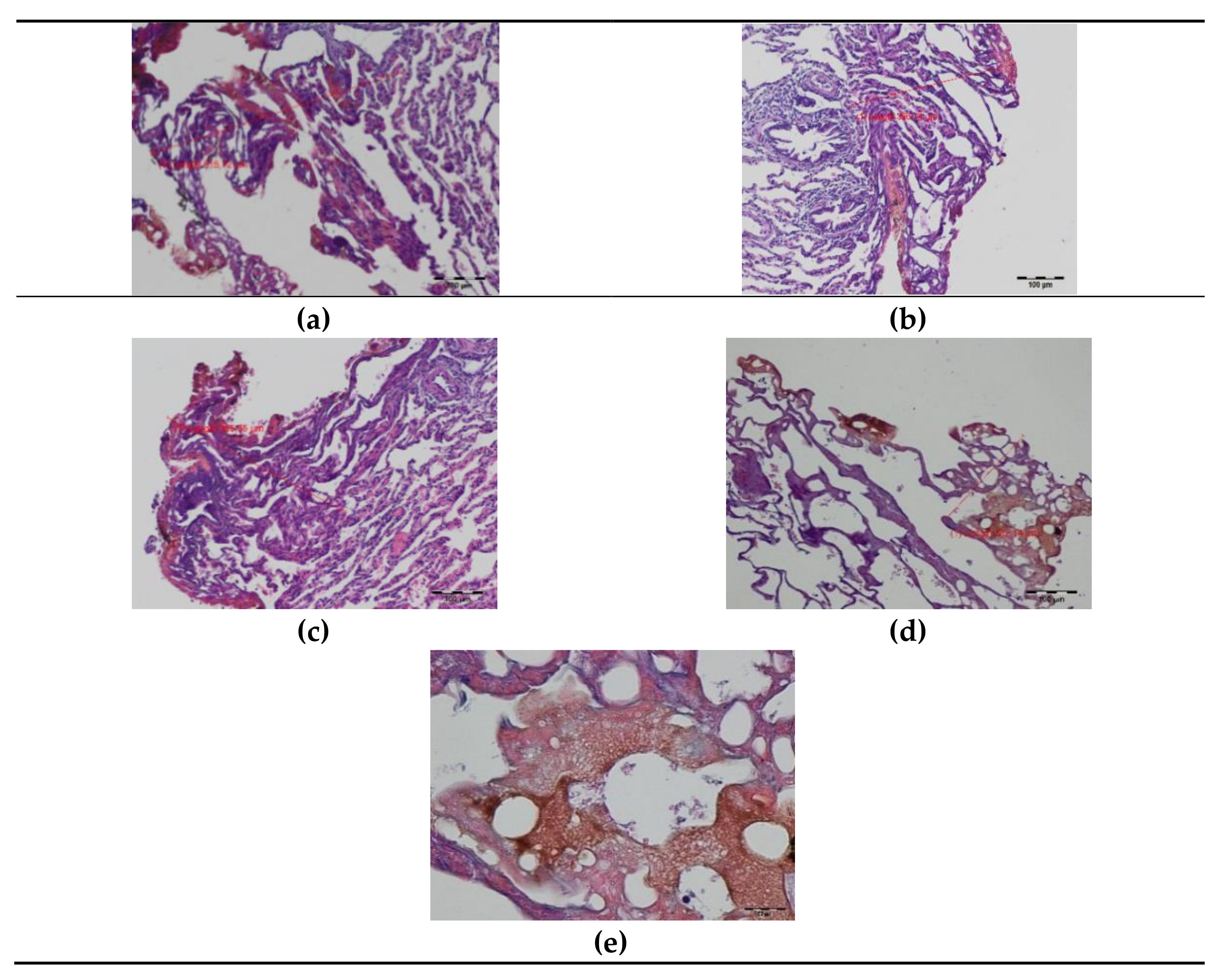
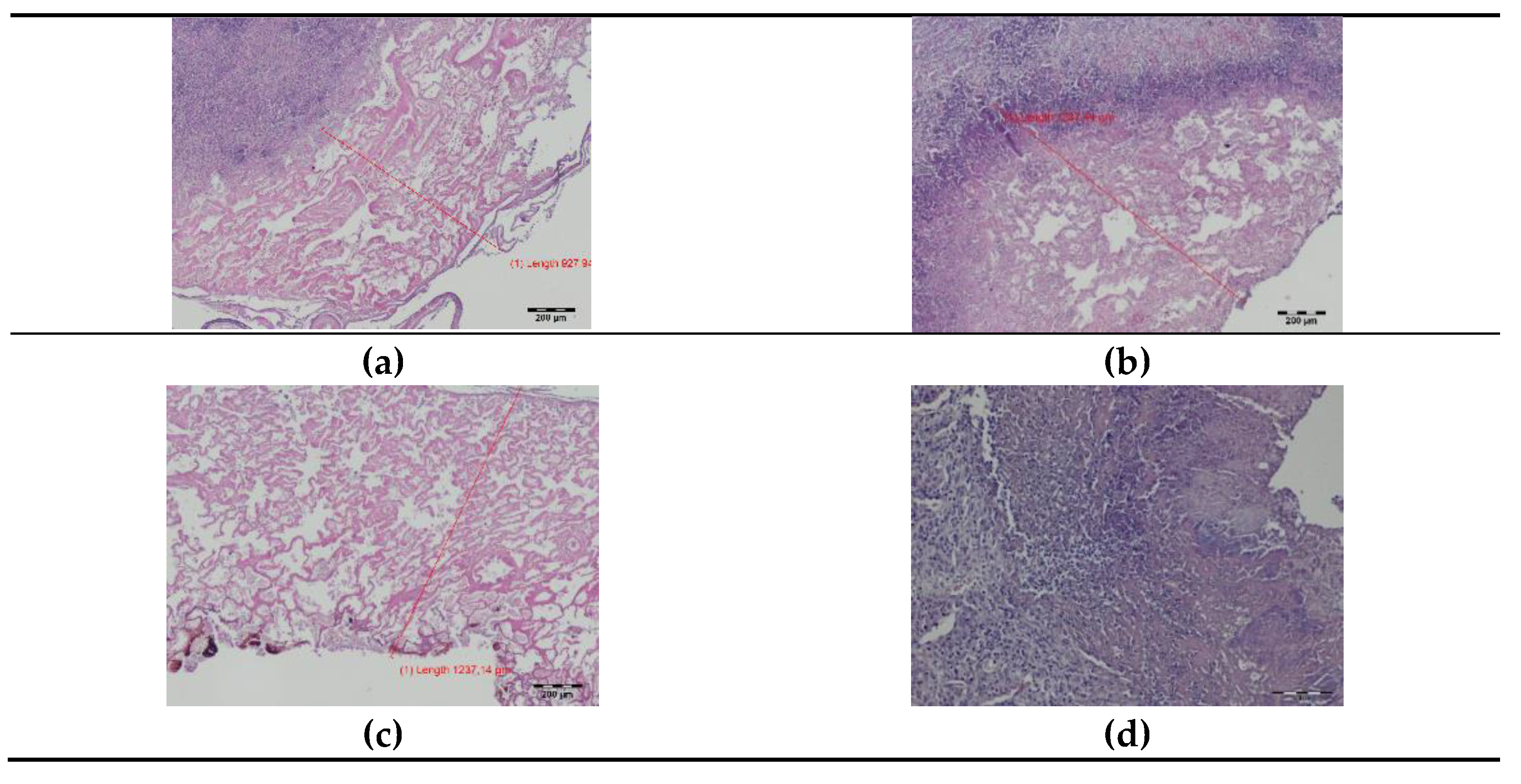
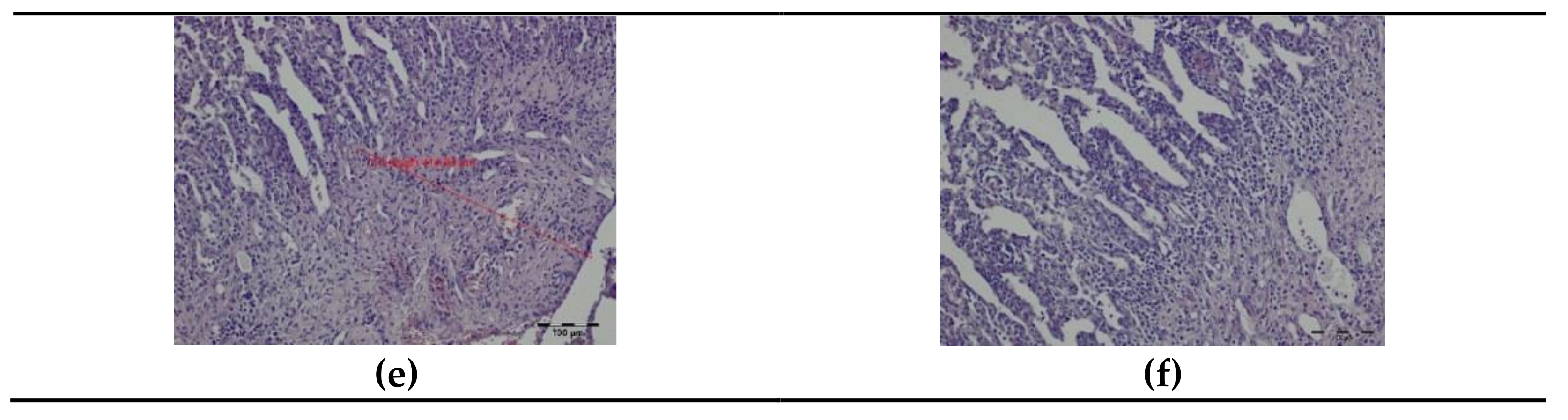
3.2. Histopathology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgements
Conflicts of Interest
References
- Davidson, R.S.; Nwogu, C.E.; Brentjens, M.J.; Anderson, T.M. The surgical management of pulmonary metastasis: Current concepts. Surg. Oncol. 2001, 10, 35–42. [Google Scholar] [CrossRef]
- Pastorino, U.; Buyse, M.; Friedel, G.; Ginsberg, R.J.; Girard, P.; Goldstraw, P.; Johnston, M.; McCormack, P.; Pass, H.; Putnam, J.B., Jr. International Registry of Lung Metastases. Long-term results of lung metastasectomy: Prognostic analyses based on 5206 cases. J. Thorac. Cardiovasc. Surg. 1997, 113, 37–49. [Google Scholar] [CrossRef] [Green Version]
- Panagiotopoulos, N.; Patrini, D.; Lawrence, D.; Scarci, M.; Mitsos, S. Pulmonary metastasectomy and laser-assisted resection. J Thorac. Dis. 2018, 10, S1930–S1933. [Google Scholar] [CrossRef] [PubMed]
- Gossot, D.; Radu, C.; Girard, P.; Le Cesne, A.; Bonvalot, S.; Boudaya, M.S.; Validire, P.; Magdeleinat, P. Resection of pulmonary metastases from sarcoma: Can some patients benefit from a less invasive approach? Ann. Thorac. Surg. 2009, 87, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Dong, S.; Zhang, L.; Li, W.; Du, J.; Liu, X.; Chen, X. Evaluation of video-assisted thoracoscopic surgery for pulmonary metastases: A meta-analysis. PLoS ONE 2014, 9, e85329. [Google Scholar] [CrossRef] [PubMed]
- Wain, J.C.; Kaiser, L.R.; Johnstone, D.W.; Yang, S.C.; Wright, C.D.; Friedberg, J.S.; Feins, R.H.; Heitmiller, R.F.; Mathisen, D.J.; Selwyn, M.R. Trial of a novel synthetic sealant in preventing air leaks after lung resection. Ann. Thorac. Surg. 2001, 71, 1623–1628. [Google Scholar] [CrossRef]
- Kirschbaum, A.; Braun, S.; Rexin, P.; Bartsch, D.K.; Seyfer, P. Comparison of local tissue damage: Monopolar cutter versus Nd:YAG laser for lung parenchyma resection. An experimental study. Interact. Cardiovasc. Thorac. Surg. 2014, 18, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Moghissi, K. Experience in limited lung resection with the use of laser. Lung 1990, 168, 1103–1109. [Google Scholar] [CrossRef]
- McLoughlin, J.B.; O’Sullivan, K.E.; Brown, R.H.; Eaton, D.A. Limax Nd:YAG laser-assisted thoracoscopic resection of pulmonary metastases; a single centre’s initial experience. Ir. J. Med. Sci. 2019, 188, 771–776. [Google Scholar] [CrossRef]
- Weigel, C.; Rosenberg, C.; Langner, S.; Fröhlich, C.P.; Hosten, N. Laser ablation of lung metastases: Results according to diameter and location. Eur. Radiol. 2006, 16, 1769–1778. [Google Scholar] [CrossRef]
- Rolle, A.; Koch, R.; Alpard, S.K.; Zwischenberger, J.B. Lobe-sparing resection of multiple pulmonary metastases with a new 1318-nm Nd:YAG laser--first 100 patients. Ann. Thorac. Surg. 2002, 74, 865–869. [Google Scholar] [CrossRef]
- Kirschbaum, A.; Bartsch, D.K.; Rexin, P. Comparison of the local effects of a 600-μm bare fibre at high laser power on lung parenchyma: Nd:YAG laser 1320 vs. 1064 nm. Lasers Med. Sci. 2017, 32, 557–562. [Google Scholar] [CrossRef]
- Ng, C.S.H.; Capili, F.; Zhao, Z.R.; Yu, P.S.Y.; Ho, J.Y.K.; Lau, R.W.H. Laser resection of pulmonary nodule via uniportal thoracoscopic surgery. J. Thorac. Dis. 2017, 9, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Wang, R.; Qian, K.; Liu, L.; Li, Y.; Hu, M.; Zhao, X.; Hua, L.; Zhi, X. A Retrospective Comparative Study of 2-μm Thulium Laser During Thoracoscopic Resection of Pulmonary Nodules. Indian. J. Surg 2020, 82, 1021–1025. [Google Scholar] [CrossRef]
- Venuta, F.; Rolle, A.; Anile, M.; Martucci, N.; Bis, B.; Rocco, G. Techniques used in lung metastasectomy. J. Thorac. Oncol. 2010, 5, S145–S150. [Google Scholar] [CrossRef] [Green Version]
- Kirschbaum, A.; Ocker, M.; Bartsch, D.K.; Quint, K. Heat dissipation after nonanatomical lung resection using a laser is mainly due to emission to the environment: An experimental ex vivo study. Lasers Med. Sci. 2014, 29, 1037–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolle, A.; Pereszlenyi, A.; Koch, R.; Richard, M.; Baier, B. Is surgery for multiple lung metastases reasonable? A total of 328 consecutive patients with multiple-laser metastasectomies with a new 1318-nm Nd:YAG laser. J. Thorac. Cardiovasc. Surg. 2006, 131, 1236–1242. [Google Scholar] [CrossRef] [Green Version]
- Baier, B.; Kern, A.; Kederali, L.; Bis, B.; Koschel, D.; Rolle, A. Retrospective survival analysis of 237 consecutive patients with multiple pulmonary metastases from advanced renal cell carcinoma exclusively resected by a 1318-nm laser. Interact. Cardiovasc. Thorac. Surg. 2015, 21, 211–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porrello, C.; Gullo, R.; Vaglica, A.; Scerrino, G.; Salamone, G.; Licari, L.; Raspanti, C.; Gulotta, E.; Gulotta, G.; Cocorullo, G. Pulmonary laser metastasectomy by 1318-nm neodymium-doped yttrium-aluminium garnet laser: A retrospective study about laser metastasectomy of the lung. Surg. Innov. 2018, 25, 142–148. [Google Scholar] [CrossRef]
- Meyer, C.; Bartsch, D.; Mirow, N.; Kirschbaum, A. Video-Assisted Laser Resection of Lung Metastases-Feasibility of a New Surgical Technique. Thorac. Cardiovasc. Surg. 2017, 65, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Kirschbaum, A.; Steinfeldt, T.; Gockel, A.; Di Fazio, P.; Quint, K.; Bartsch, D.K. Airtightness of lung parenchyma without a closing suture after atypical resection using the Nd:YAG Laser LIMAX 120. Interact. Cardiovasc. Thorac. Surg. 2014, 18, 92–95. [Google Scholar] [CrossRef] [Green Version]
- Marulli, G.; Droghetti, A.; Di Chiara, F.; Calabrese, F.; Rebusso, A.; Perissinotto, E.; Muriana, G.; Rea, F. A prospective randomized trial comparing stapler and laser techniques for interlobar fissure completion during pulmonary lobectomy. Lasers Med. Sci. 2013, 28, 505–511. [Google Scholar] [CrossRef]
- Kirschbaum, A.; Palade, E.; Kayser, G.; Passlick, B. Local effects of high-powered neodymium-doped yttrium aluminium garnet laser systems on the pulmonary parenchyma: An experimental study on the isolated perfused pig lung lobe. Interact. Cardiovasc. Thorac. Surg. 2012, 15, 191–193. [Google Scholar] [CrossRef] [Green Version]
- Koshelev, V.N.; Chalyk, I. CO2 and YAG lasers in the surgery of traumatic lesions of the liver, spleen and kidney. Vestn. khirurgii Im. II Grek. 1992, 149, 52–56. [Google Scholar]
- Goldenberg, A.; Goldenberg, S.; Guidugli Neto, J.; Chacon, J.P. CO2 laser and suture in splenic parenchyma: An experimental study. Lasers Surg. Med. 1985, 5, 405–413. [Google Scholar] [CrossRef]
- Plapler, H.; Mancini, M.W.; Sella, V.R.; Bomfim, F.R. Evaluation of different laser wavelengths on ablation lesion and residual thermal injury in intervertebral discs of the lumbar spine. Lasers Med. Sci. 2016, 31, 421–428. [Google Scholar] [CrossRef] [PubMed]
- De Araujo, W.J.B.; Timi, J.R.R.; Kotze, L.R.; Vieira da Costa, C.R. Comparison of the effects of endovenous laser ablation at 1470 nm versus 1940 nm and different energy densities. Phlebology 2019, 34, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Źywicka, B.; Rybak, Z.; Janeczek, J.; Czerski, A.; Bujok, J.; Szymonowicz, M.; Dobrzynski, M.; Korczynski, M.; Swiderski, J. Comparison of A 1940 nm Thulium-Doped Fiber Laser and A 1470 nm Diode Laser for Cutting Efficacy and Hemostasis in A Pig Model of Spleen Surgery. Materials 2020, 13, 1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janeczek, M.; Swiderski, J.; Czerski, A.; Zywicka, B.; Bujok, J.; Szymonowicz, M.; Bilewicz, E.; Dobrzyński, M.; Korczyński, M.; Chrószcz, A.; et al. Preliminary evaluation of thulium doped fiber laser in pig model of liver surgery. BioMed. Res. Int. 2018, 2018, 3275284. [Google Scholar] [CrossRef] [PubMed]
- Żywicka, B.; Bujok, J.; Janeczek, M.; Czerski, A.; Szymonowicz, M.; Dobrzyński, M.; Świderski, J.; Rybak, Z. Usefulness of Thulium-Doped Fiber Laser and Diode Laser in Zero Ischemia Kidney Surgery-Comparative Study in Pig Model. Materials 2021, 14, 2000. [Google Scholar] [CrossRef]
- Michalska, M.; Brojek, Z.; Rybak, Z.; Sznelewski, P.; Świderski, M. An all-fiber thulium doped fiber laser for medical application. Elektron. Konstr. Technol. Zastos. 2016, 57, 13–15. [Google Scholar]
- Kirschbaum, A.; Höchsmann, N.; Steinfeldt, T.; Seyfer, P.; Pehl, A.; Bartsch, D.K.; Palade, E. Investigations of initial airtightness after non-anatomic resection of lung parenchyma using a thulium-doped laser with different optical fibres. Lasers Med. Sci. 2016, 31, 1097–1103. [Google Scholar] [CrossRef]
- Scanagatta, P.; Furia, S.; Billè, A.; Duranti, L.; Girelli, L.; Tavecchio, L.D.; Leo, F.; Giovannetti, R.; Pelosi, G.; Porcu, L.; et al. Thulium laser versus staplers for anatomic pulmonary resections with incomplete fissures: Negative results of a randomized trial. Tumori 2014, 100, 259–264. [Google Scholar] [CrossRef]
- Scanagatta, P.; Pelosi, G.; Leo, F.; Furia, S.; Duranti, L.; Fabbri, A.; Manfrini, A.; Villa, A.; Vergani, B.; Pastorino, U. Pulmonary resections: Cytostructural effects of different-wavelength lasers versus electrocautery. Tumori 2012, 98, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Ou, T.W.; Chen, L.; Wang, Q.; Lan, F.; Shen, P.; Li, J.; Xu, J.J. Thulium laser vaporesection versus standard transurethral resection of the prostate: A randomized trial with transpulmonary thermodilution hemodynamic monitoring. Int. J. Urol. 2013, 20, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Bilici, T.; Mutlu, S.; Kalaycioglu, H.; Kurt, A.; Sennaroglu, A.; Gulsoy, M. Development of a thulium (Tm:YAP) laser system for brain tissue ablation. Lasers Med. Sci. 2011, 26, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.A.; Kobler, J.B.; Heaton, J.T.; Lopez-Guerra, G.; Anderson, R.R.; Zeitels, S.M. Thermal damage during thulium laser dissection of laryngeal soft tissue is reduced with air cooling: Ex vivo calf model study. Ann. Otol. Rhinol. Laryngol. 2007, 116, 853–857. [Google Scholar] [CrossRef]
- Kamalski, D.M.; Vincent, R.; Wegner, I.; Bittermann, A.J.; Grolman, W. A nonrandomized comparison of the thulium laser and the CO2 laser in primary stapedotomy for otosclerosis. Otol. Neurotol. 2014, 35, 1715–1719. [Google Scholar] [CrossRef] [PubMed]
- Tendean, M.; Mambu, T.D.B.; Tjandra, F.; Panelewen, J. The use of Thulium-Doped Fiber Laser (TDFL) 1940 nm as an energy device in liver parenchyma resection, a-pilot-study in Indonesia. Ann. Med. Surg. 2020, 60, 491–497. [Google Scholar] [CrossRef]
- Stefani, A.; Oricchio, F.; Cinquepalmi, A.; Aramini, B.; Morandi, U. Is laser-assisted resection preferable to lobectomy for pulmonary metastasectomy? Lasers Med. Sci. 2020, 35, 611–620. [Google Scholar] [CrossRef]
- Franzke, K.; Natanov, R.; Zinne, N.; Rajab, T.K.; Biancosino, C.; Zander, I.; Lodziewski, S.; Ricklefs, M.; Kropivnitskaya, I.; Schmitto, J.D.; et al. Pulmonary metastasectomy: A retrospective comparison of surgical outcomes after laser-assisted and conventional resection. Eur. J. Surg. Oncol. 2017, 43, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Ojanguren, A.; Karenowics, W.; Dackam, S.; Demarchi, M.; Triponez, F. Laser pulmonary metastasectomy by video-assisted thoracic surgery. J. Vis. Surg. 2019, 5, 40. [Google Scholar] [CrossRef]
- Schmid, S.; Le, U.T.; Zeisal, C.; Haager, B.; Passlick, B. Pulmonary metastasectomy in sarcoma - experiences with laser-assisted resection. J. Thorac. Dis. 2018, 10, 314–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mineo, T.C.; Ambrogi, V.; Pompeo, E.; Nofroni, I. The value of the Nd:YAG laser for the surgery of lung metastases in a randomized trial. Chest 1998, 113, 1402–1407. [Google Scholar] [CrossRef] [PubMed]
- Moghissi, K.; Dench, M.; Neville, E. Effect of the non-contact mode of YAG laser on pulmonary tissues and its comparison with electrodiathermy: An anatomic-pathological study. Lasers Med. Sci. 1989, 4, 17–23. [Google Scholar] [CrossRef]
- Welter, S.; Arfanis, E.; Christoph, D.; Hager, T.; Roesel, C.; Aigner, C.; Weinreich, G.; Theegarten, D. Growth patterns of pulmonary metastases: Should we adjust resection techniques to primary histology and size? Eur. J. Cardiothorac. Surg. 2017, 52, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, S.; Toyooka, S.; Iga, N.; Furukawa, M.; Sugimoto, R.; Shien, K.; Nishikawa, H.; Soh, J.; Yamane, M.; Oto, T.; et al. Use of a vessel sealing system versus conventional electrocautery for lung parenchymal resection: A comparison of the clinicopathological outcomes in porcine lungs. Surg. Today 2014, 44, 540–545. [Google Scholar] [CrossRef]
- Rexin, P.; Bartsch, D.; Kirschbaum, A. Local Effects on Lung Parenchyma Using a 600 µm Bare Fiber with the Diode-Pumped Nd:YAG Laser LIMAX® 120. Appl. Sci. 2015, 5, 1560–1569. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time | n | Thulium-Doped Fiber Laser (TDFL) | Diode Laser (DL) |
|---|---|---|---|
| Day 0 | |||
| Superficial zone of thermal damage | 5 | 229.74 ± 34.59 a | 335.29 ± 16.07 b |
| Total zone of thermal damage | 5 | 499.46 ± 61.44 a | 937.39 ± 109.65 b |
| Day 7 | |||
| Superficial zone of thermal damage | 5 | 1256.69 ± 186.44 a | 1800.28 ± 206.41 b |
| Total zone of thermal damage | 5 | 2615.74 ± 487.17 a | 6500.34 ± 1118.02 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janeczek, M.; Rybak, Z.; Lipińska, A.; Bujok, J.; Czerski, A.; Szymonowicz, M.; Dobrzyński, M.; Świderski, J.; Żywicka, B. Local Effects of a 1940 nm Thulium-Doped Fiber Laser and a 1470 nm Diode Laser on the Pulmonary Parenchyma: An Experimental Study in a Pig Model. Materials 2021, 14, 5457. https://doi.org/10.3390/ma14185457
Janeczek M, Rybak Z, Lipińska A, Bujok J, Czerski A, Szymonowicz M, Dobrzyński M, Świderski J, Żywicka B. Local Effects of a 1940 nm Thulium-Doped Fiber Laser and a 1470 nm Diode Laser on the Pulmonary Parenchyma: An Experimental Study in a Pig Model. Materials. 2021; 14(18):5457. https://doi.org/10.3390/ma14185457
Chicago/Turabian StyleJaneczek, Maciej, Zbigniew Rybak, Anna Lipińska, Jolanta Bujok, Albert Czerski, Maria Szymonowicz, Maciej Dobrzyński, Jacek Świderski, and Bogusława Żywicka. 2021. "Local Effects of a 1940 nm Thulium-Doped Fiber Laser and a 1470 nm Diode Laser on the Pulmonary Parenchyma: An Experimental Study in a Pig Model" Materials 14, no. 18: 5457. https://doi.org/10.3390/ma14185457