1. Introduction
Autogenous bone is still the best option for regenerating bone defects because it meets all the indicated requirements of an ideal bone graft material for osteoinduction and osteoconduction [
1,
2,
3]. On the other hand, the use of autografts is limited by the insufficient bone volume, specific surgical complications, postoperative morbidity, and operation cost. Thus, synthetic bone or biomimetic bone materials as alternatives to autogenous bone have been evaluated as artificial bone in orthopedics and dentistry. These alternative materials should provide a variety of shapes and sizes with mechanical strength and biocompatibility suitable for use in the regeneration of bone defect sites. Generally, bioresorbable materials are preferred because they are expected to maintain the bone volume during bone reconstruction and be gradually replaced by newly formed bone [
4]. Numerous physicochemical features of scaffolds, such as surface chemistry, surface roughness, topography, mechanical properties, and interfacial free energy (hydrophobic/hydrophilic balance) are important for cell attachment, proliferation, and differentiation. These factors are also critical to the overall biocompatibility and bioactivity of a particular material [
5,
6,
7].
The resorption of bone substitutes is related to several factors, such as particle size, porosity, chemical and crystallographic properties (composition, Ca/P ratio, phases, and crystallinity), and pH (appropriate for body fluids) [
8,
9]. In general, smaller particle size, higher porosity, lower crystallinity, and higher non-stoichiometric ratio result in faster resorption from bone substitutes [
10]. Hydroxyapatite (HA) and β-tricalcium phosphate (β-TCP) materials are currently used as artificial bone graft materials [
11,
12]. HA produced by sintering is used as a scaffold material because it does not dissolve in bone defects for a long period of time and retains its shape [
13,
14,
15]. In contrast, β-TCP is used as a resorbable bone substitute due to its inherent solubility in a physiological environment [
16]. Biphasic calcium phosphates (BCP), composed of various ratios of HA and β-TCP phases, are mainly applied [
17] to control the rate of resorption. Recent study has shown that the resorption of β-TCP can occur not only by dissolution but also by the phagocytosis of osteoclasts [
18].
Octacalcium phosphate (OCP), which is attracting attention as an alternative calcium phosphate bone graft material, is biodegradable at the bone defect site and has a neutral pH [
19,
20]. The OCP crystal, Ca
8H
2(PO
4)
6 5H
2O, has a water layer between two apatite layers. In a physiological environment, the water layer is removed from the OCP, and the two apatite layers are combined to form HA crystals [
21]. Based on its crystallographic similarity, OCP has been proposed as a precursor of biological apatite crystals in bones and teeth. Histological studies by Suzuki and coworkers found that some calcium phosphate ceramics, such as β-TCP and OCP, were reabsorbed by osteoclasts in addition to dissolution by the physiological pH of OCP [
22,
23,
24]. The superior osteoconductivity of OCP has also been demonstrated in animal-based studies [
4,
25].
To date, a few in vivo and clinical studies using OCP have shown that bone repair is superior to other bone substitutes [
26,
27,
28,
29]. OCP as a bone substitute has many advantages for bone restoration, but the difficulties in mass production limited its practical clinical application. The recent development of OCP mass production technology has opened up the possibility of the clinical applications of OCP. So far, there has been a laboratory-scale study of OCP substances, but this study is the first comparative animal study of a commercialized OCP product. The bone regeneration ability of OCP products was compared with two of the most clinically used materials: heat-treated bovine bone and sintered BCP.
2. Materials and Methods
2.1. Bone Substitute Materials
Three commercially available granular products were used in this study. The bone-forming ability of a newly released OCP bone product was compared with two other types of products that are currently widely used. A xenograft product (Bio-Oss), comprised of an inorganic mineralized trabecular bovine HA matrix, was used as a comparative test group. Bio-Oss (Geistlich Pharma AG, Wolhusen Switzerland), which is produced by deproteination at high temperatures, favors the proliferation of blood vessels and bone cell migration through the interconnecting micropores. Another comparative testing sample was a BCP product (MBCP+) that consists of 20:80% of HA and β-TCP. MBCP+ (Biomatlante SAS, Édouard Belin, France) is a BCP synthetic bone graft substitute with a micro- and macroporous structure closely resembling the architecture of natural human bone.
The OCP test product was a granular synthetic OCP material, Bontree (HudenBio, Gwangju, Korea), consisting mainly of OCP. Bontree is a recently released biodegradable synthetic bone graft substitute with a micro- and macro-pore structure. Unlike the above two products, which are processed at high temperatures, Bontree products are produced at room temperature. In general, bone graft materials prepared at low temperature are known to exhibit high bioactivity, but have low mechanical strength and are easily resorbed. In particular, when the OCP material is subjected to high-temperature treatment, it has a characteristic of changing into a different phase.
2.2. Characterization of Bone Substitute Materials
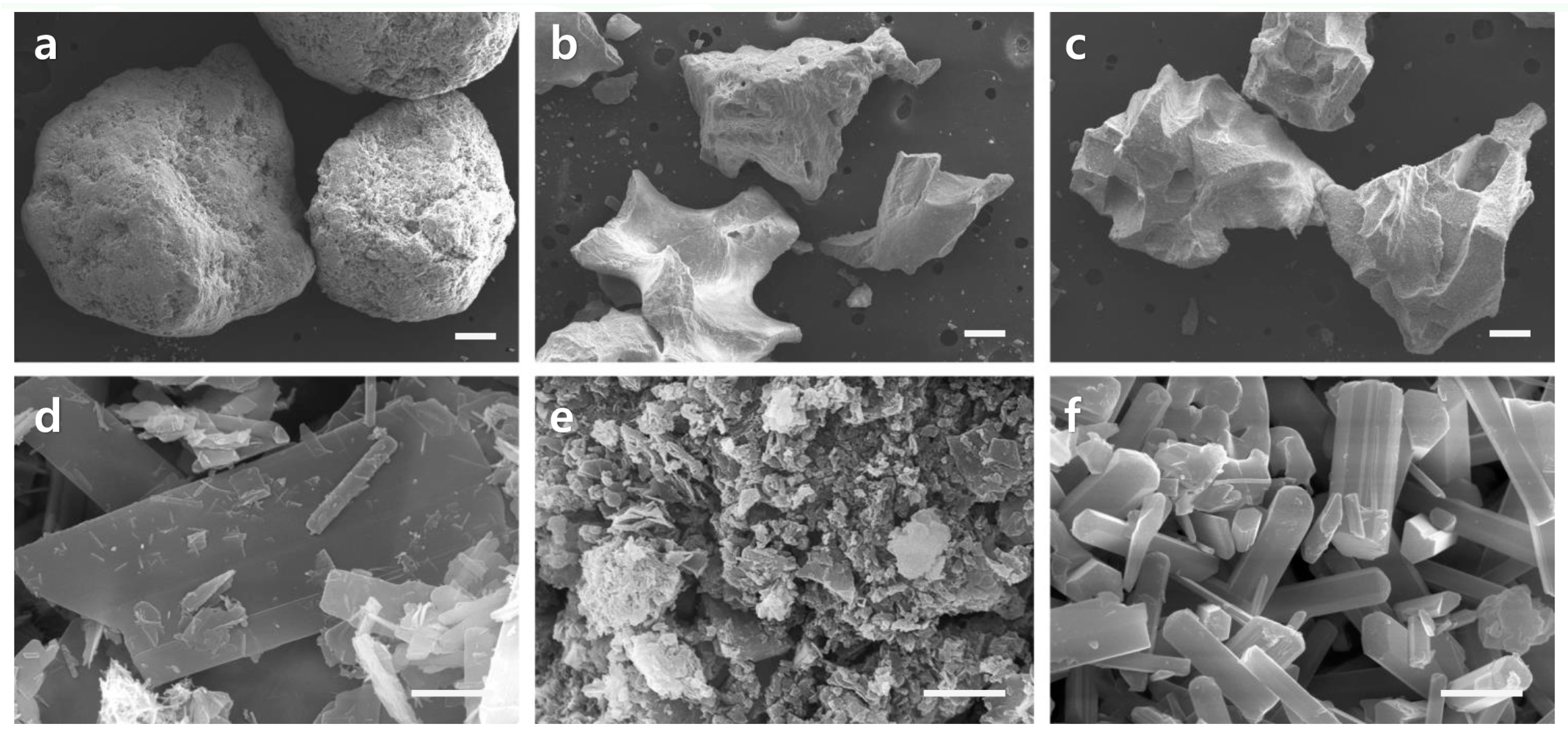
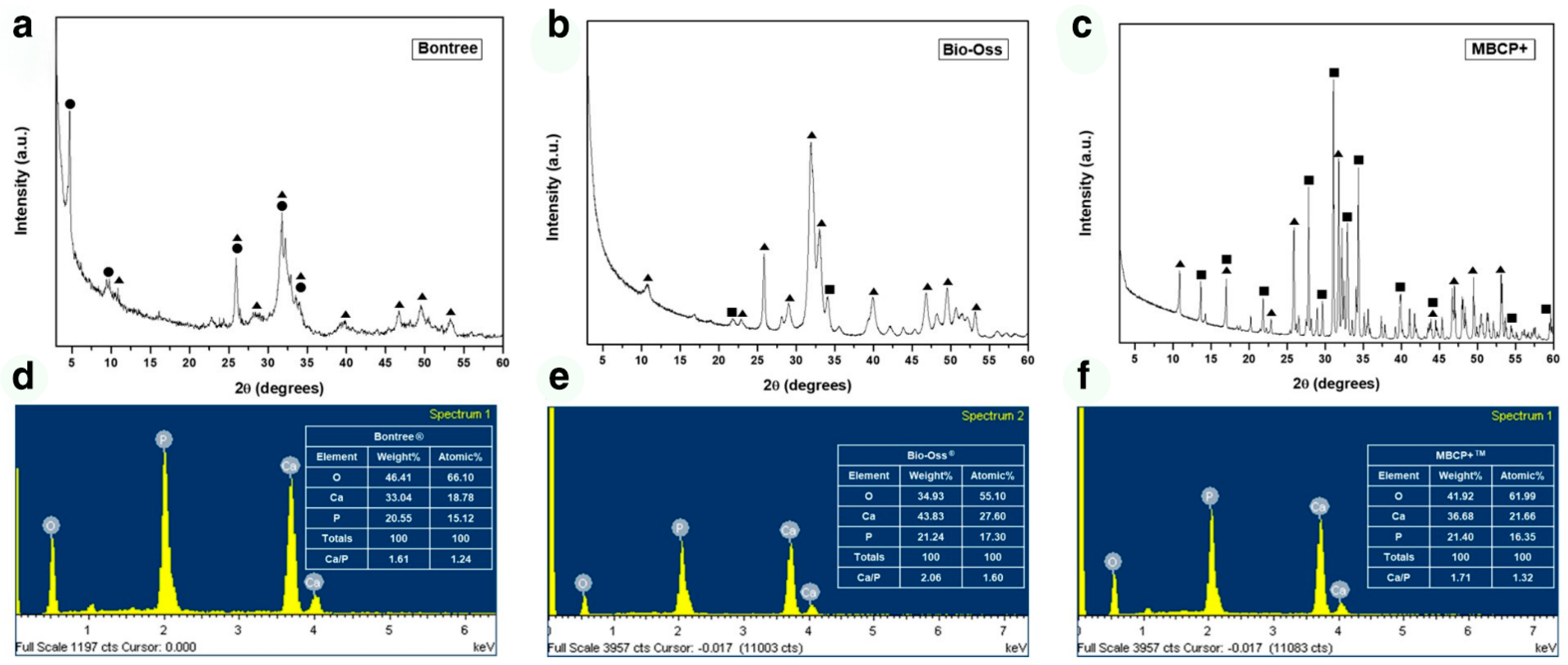
The morphology, size, and pore characteristics of the samples were examined by scanning electron microscopy (SEM, Hitachi S-4300; Hitachi, Tokyo, Japan) at ×50 and ×20,000 magnifications. The phase of the bone graft material and the Ca/P ratio directly affect the rate of bone formation and biodegradation. Therefore, the phases of all samples were investigated by X-ray diffraction (XRD, X’pert MPD-PRO; Panalytical, Almelo, Netherlands). The XRD experiments were performed at 40 kV and 30 mA and using copper Kα radiation. The Ca/P ratio of the samples was measured by energy-dispersive X-ray spectroscopy (EDS. Ultim Max; Oxford Instruments, Abindon, UK).
2.3. Animals
Twelve eleven-week-old male New Zealand White rabbits were obtained from Orientbio (Seongnam, Korea) and maintained under specific pathogen-free conditions. The Institutional Animal Care and Use Committee (CRONEX-IACUC 201908004) of Cronex Co., Ltd. (Seoul, Korea) approved all experimental protocols. The rabbits underwent initial adaptation while being fed a normal diet under temperature, humidity, and light-controlled conditions. After two weeks of acclimatization, healthy animals within the 80th percentile of body weight (3.0–3.5 kg) were numbered with minimal weight variation and underwent surgery.
2.4. Surgical Procedure
The subjects were anaesthetized with an intravenous injection of 5 mg/kg body weight of tiletamine hydrochloride and zolazepam hydrochloride (Zoletil 50; Virbac, Carros, France) and 15 mg/kg body weight of 2% xylazine hydrochloride (Rumpun; Bayer, Seoul, Korea). After a skin incision, both tibias were exposed, and three 3 mm diameter defects were made in each tibia using an implant drill. The defects were filled with Bontree (OCP), Bio-Oss (BHA), or MBCP + (BCP). An additional sham surgery group (CON) was also prepared. After 4 or 12 weeks, the animals were sacrificed, and the tibias were harvested.
2.5. Bone Sample Preparation
Each defect segment was cut using a diamond saw and fixed in 10% formalin for one day. The bone samples were dehydrated in a graded series of ethanol and infiltrated for one day each in a 1:3, 1:1, and 3:1 Technovit 7200 resin (Heraeus Kulzer, Wehrheim, Germany) and ethanol mixture. The sample was polymerized in a UV embedding system (Kulzer Exakt, Wehrheim, Germany) after shaking for one day under vacuum in pure Technovit resin. The hard resin sample obtained was cut and ground to 15 μm thick slides using an EXAKT cutting and grinding machine (Kulzer Exakt 300, 400CS; Wehrheim, Germany). The tissue slides were observed by optical microscopy (6000D; Leica, Germany) after being hematoxylin-eosin (H-E) stained and mounted.
2.6. Histological Observation and Morphometric Analysis
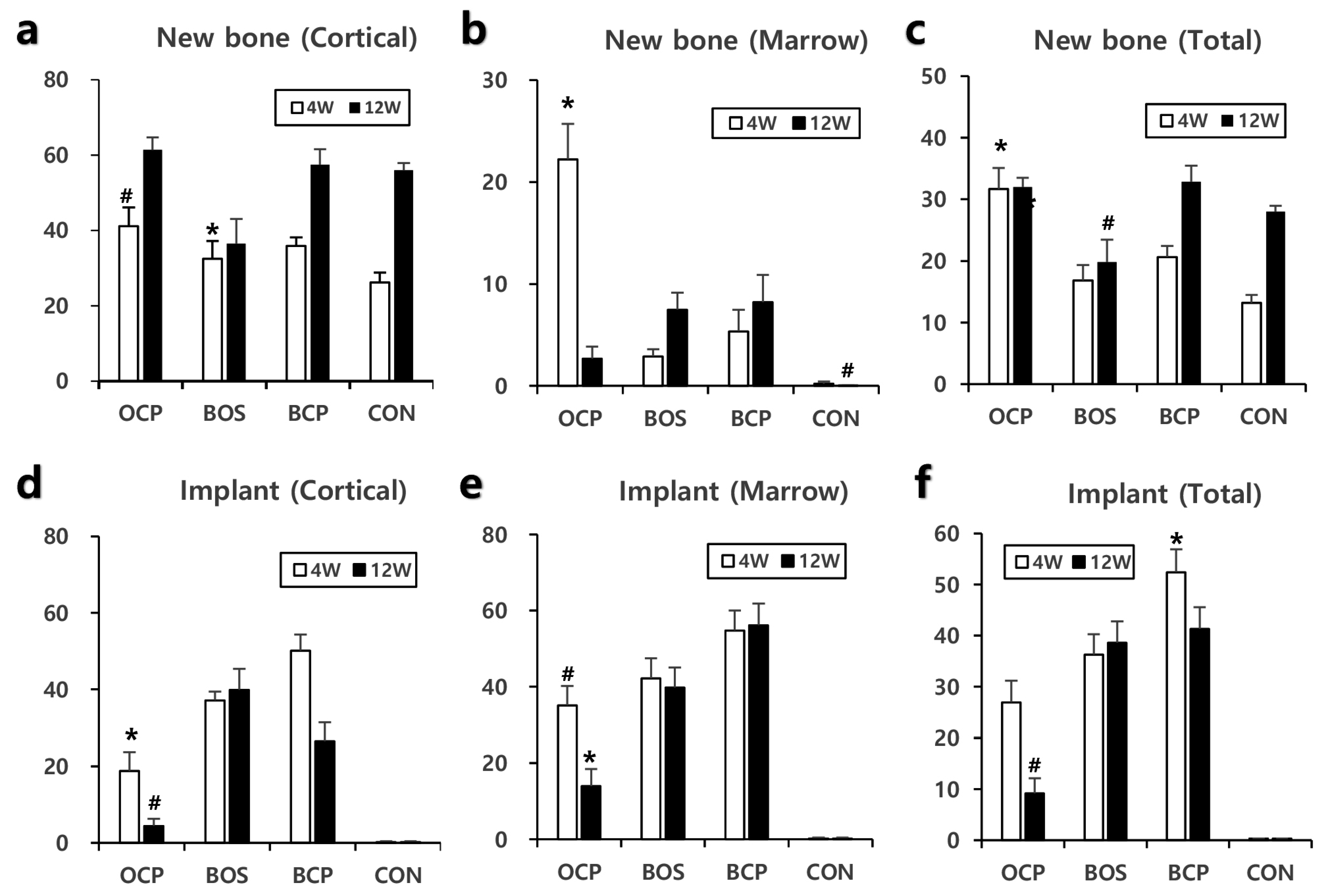
New bone formation and the implant material status were observed, and the bone healing process for each implant material was analyzed (n = 9 each). The new bone formation and the implant material remnant were measured quantitatively using the Image-Pro Plus program (Media Cybernetics, Silver Spring, MD, USA). Two rectangles in a 3 × 1.5 mm size boundary were set on the cortical bone and marrow area in the defect area. An accurate region of regeneration inside a rectangle was gated using the above computer program. The total gated, new bone occupied, and implant material occupied areas were measured based on the color and darkness differences using the Image-Pro program. The percentages of new bone and implant material in the total gated area were calculated.
2.7. Statistical Analysis
The data are presented as graphs representing the mean ± standard error. ANOVA (Scheffe) was performed, and a p value of <0.05 was considered significant. Statistical analysis was performed using IBM SPSS Statistics 23.0 (IBM, Armonk, NY, USA).
4. Discussion
The solubility or biodegradation of calcium phosphate substances is related directly to the Ca/P molar ratio. Various calcium phosphate materials form differently depending on the Ca/P ratio. A calcium phosphate material with a low Ca/P ratio exhibits chemical stability in a low pH environment, whereas a material formed at a high Ca/P ratio has stability under neutral or basic pH conditions. For example, HA exhibits chemical stability at a high pH (i.e., a neutral or basic environment) because its stoichiometric Ca/P ratio is 1.67. In contrast, OCP has a relatively low Ca/P ratio of 1.33 and exhibits stability at a relatively low pH (i.e., acidic environment). Therefore, in animal experiments, the BHA sample composed mainly of HA would exhibit high chemical stability under physiological conditions. This stability would be followed by BCP (composed of HA and β-TCP) and the OCP sample composed mainly of OCP, which show low chemical stability. Therefore, in a neutral in vivo environment, the OCP sample with a relatively low Ca/P ratio had a much faster biodegradation rate than those of the other samples (
Figure 5). These results are consistent with the findings reported elsewhere [
24,
30].
Acidic calcium phosphates, such as OCP and dicalcium phosphate dihydrate (DCPD), are considered soluble ceramics at a neutral pH. In vivo biodegradation is generally associated with the solubility of calcium phosphate at a physiological pH level [
24,
30]. In addition, β-TCP is less acidic than OCP but is the most widely used biodegradable ceramic in vivo [
19,
21], whereas HA is the most chemically stable at physiological pH. In this study, in vivo resorption of the OCP sample, composed mainly of OCP, was approximately two-fold after four weeks and four-fold after 12 weeks, which was notably faster than that of the BCP sample composed of HA and β-TCP and the BHA sample composed of HA. The in vitro resorption rate of OCP was similar to that of β-TCP, but the in vivo resorption of OCP samples was much faster than that of BCP composed of 80% β-TCP. These results show that an additional degradation mechanism is involved in the OCP sample.
In general, the stability of calcium phosphate materials is related to several factors, such as particle size, porosity, Ca/P ratio, phase, and crystallinity [
9,
10]. Even with the same type of calcium phosphate material, the chemical stability in the physiological environment varies with the degree of non-stoichiometry, particle size, porosity, and crystallinity. Non-stoichiometric materials are thermodynamically and chemically unstable compared to stoichiometric materials [
19]. All calcium phosphate bone substitutes examined in this study have non-stoichiometric chemistry: The Ca/P ratio of each tested sample was lower than the stoichiometric ratio. Therefore, all samples used in this experiment are believed to exhibit faster biodegradation than stoichiometric materials.
Micrometer-sized particles take longer to be eliminated than nanometer-sized particles because osteoclasts require a longer time for chemical dissolution and biological absorption. Although the main phase was HA, the BHA samples would have been absorbed quickly because they were comprised of nano-sized particles. SEM (
Figure 1) showed that the particle distribution of the BHA samples was in the tens of nanometers range, with a BCP distribution of several micrometers and OCP from submicron to several micrometer sizes. The crystallinity of a biomaterial also changes its resorption rate. Highly crystalline materials are more resistant to resorption than less crystalline materials because they are thermodynamically more stable. The crystallinity of a material can be deduced from its XRD peak. The XRD (
Figure 2) patterns of the BHA and OCP samples showed broad peaks compared to the BCP sample. This is because BHA and OCP were treated at relatively lower temperatures than BCP, resulting in lower crystallinity.
Several studies have suggested possible in vivo degradation mechanisms of calcium phosphate ceramics [
26,
31]. Many studies have shown that biodegradable calcium phosphate materials are degraded by simple dissolution, fragmentation/disintegration, osteoclastic resorption, or phase conversion [
26]. The predominant degradation mechanism will vary according to the material, and a single mechanism may not be involved. Instead, several mechanisms may be active simultaneously or sequentially. The rapid degradation of the OCP sample, which consists mainly of OCP, is believed to be due to the formation of biological apatite via fast phase conversion of OCP. In addition, OCP exhibits simple dissolution and osteoclastic resorption similar to that observed in other biodegradable calcium phosphate samples. The in vivo resorption of a grafted OCP sample is presumed to be caused by several mechanisms, including dissolution, fragmentation/disintegration, osteoclastic resorption, and phase conversion. The low crystallinity and large porosity of the OCP sample would have improved its resorption rate.
Histomorphometric analysis indicated that the OCP group produced the highest quantity of new bone formation and was the only group to show a significant difference to CON after four weeks (
Figure 3). Interesting results were obtained in the OCP group related to the bone marrow. A significant amount of new bone was generated in the bone marrow after four weeks, but this almost disappeared after 12 weeks. These results suggest that OCP could influence the differentiation of stem cells into osteoblasts in the early stage [
24], and it was presumed that they were resorbed over time. The cortical and medullar areas are under quite different physiological conditions. Cortical bone endures mechanical stress for bearing the body weight and movement forces, whereas the marrow area is a cavity that does not provide support against mechanical stress. Thus, bone remodeling by bone resorption and new bone formation occurs in the cortical bone and leads to the maintenance of a bone structure. On the other hand, there is no active remodeling in the marrow, which leads to the resorption of the bone structure.
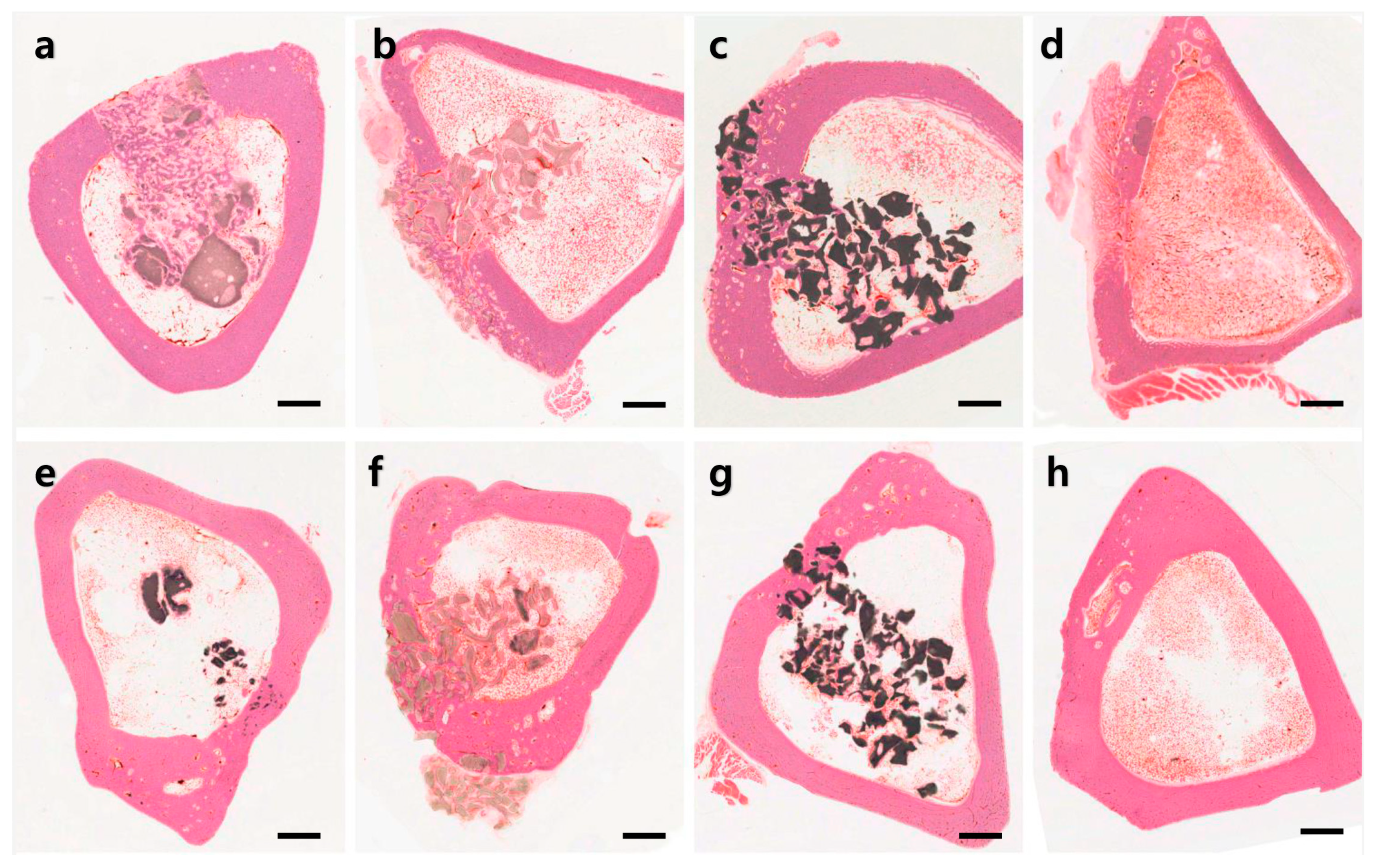
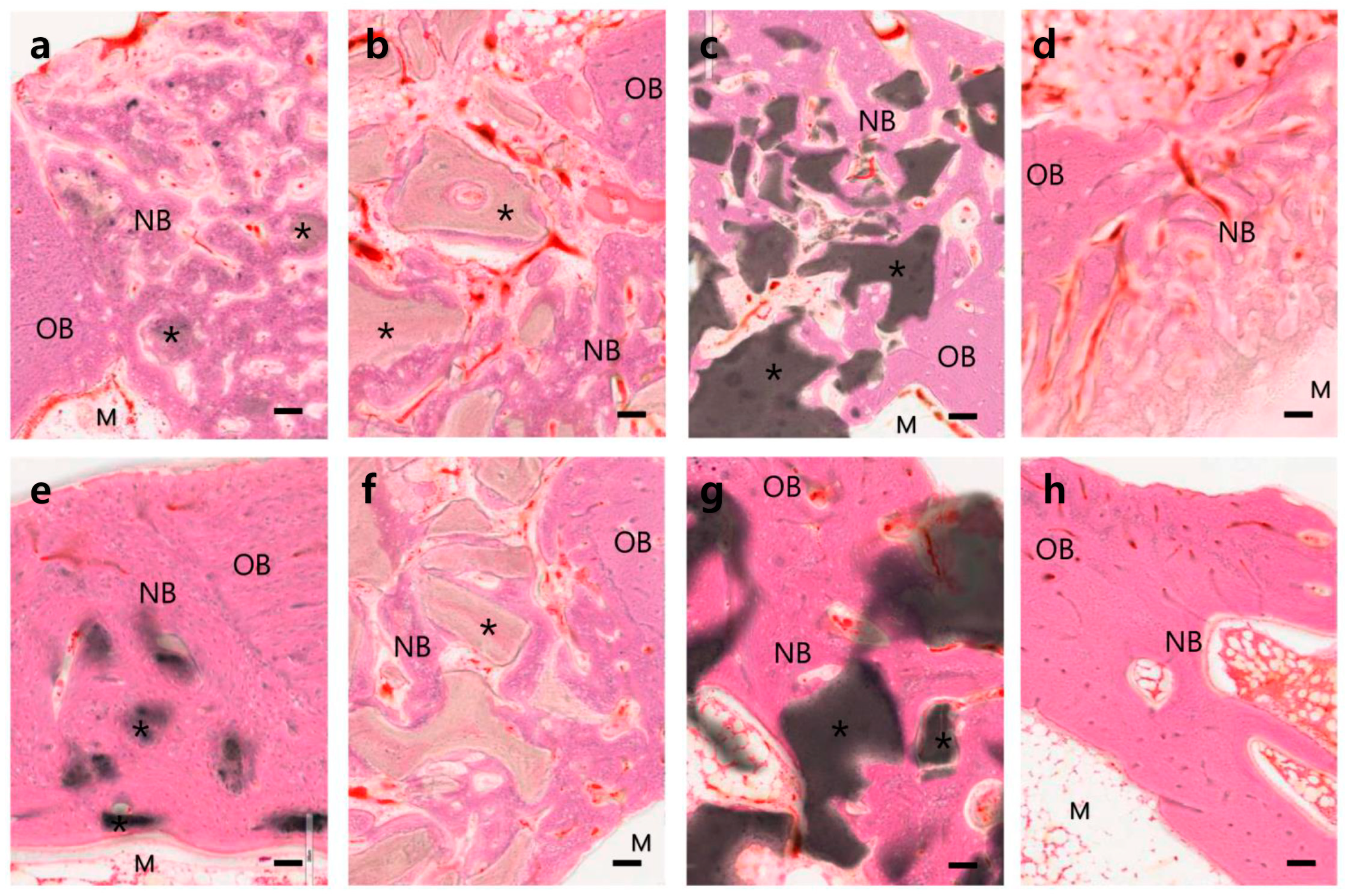
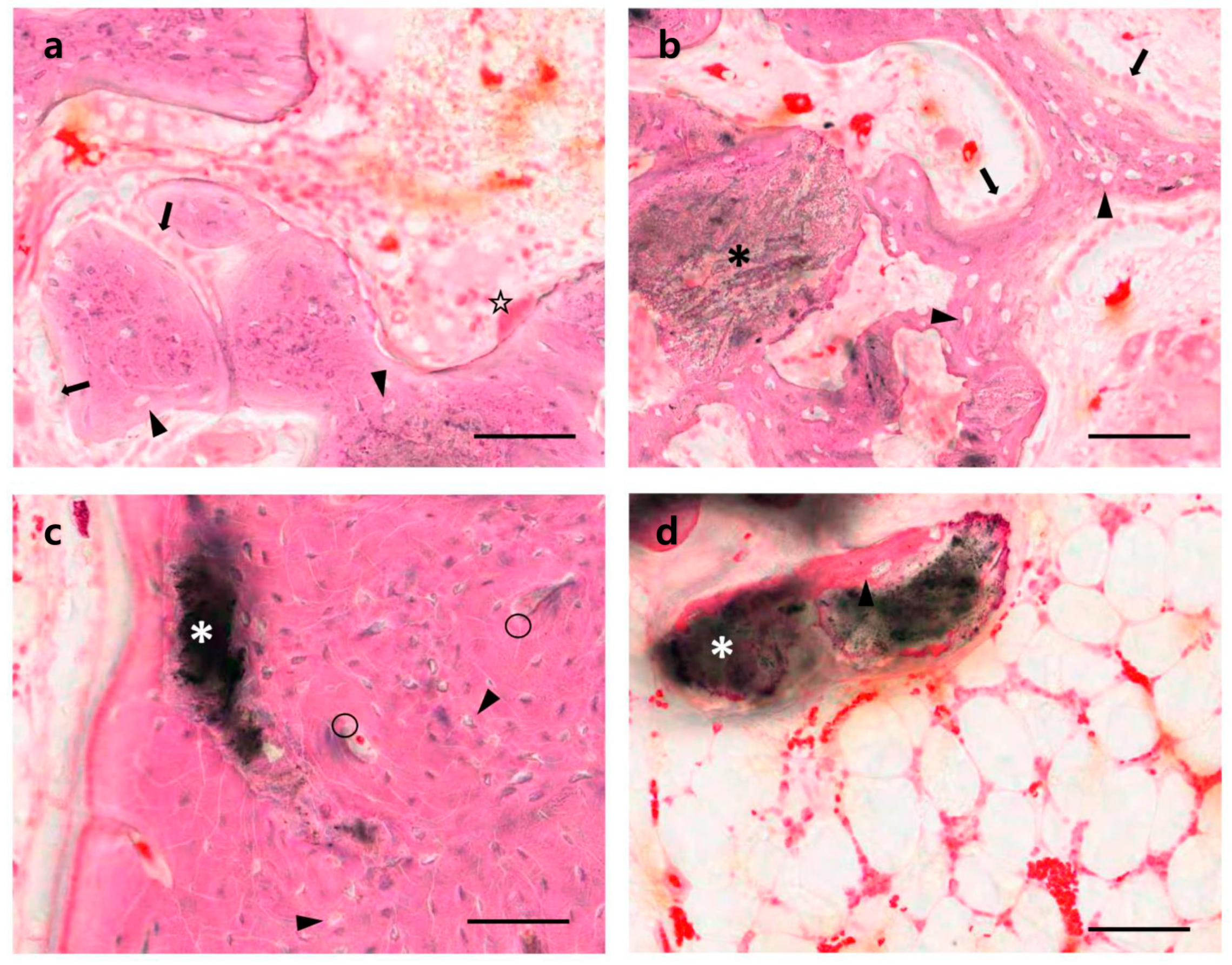
The histological findings showed that the various calcium phosphate samples tested had various dissolution and new bone formation rates (
Figure 5). Most calcium phosphate materials will dissolve with time after being implanted in the body, resulting in the formation of new bone in the dissolved space or on the surface of the implanted materials. The dissolution and new bone formation rates depend on the characteristics of the implanted materials, such as phase composition, porosity, Ca/P molar ratio, crystallinity, particle size, and impurities. Among the samples tested, the fastest bone healing rate was observed at four weeks in the OCP sample group. Well-organized hard callus formation was observed in both the cortical and medullary regions (
Figure 5a). Most of the OCP granules were covered with new bone components, including the osteocytes of the lacuna. At 12 weeks, the bone healing process had progressed to a more mature bone form. The rapid new bone formation and bone remodeling observed in the OCP group were attributed to the rapid mineralization of the OCP crystals caused by phase conversion to biologically active apatite. On the other hand, the relatively slow new bone formation in the other test groups (BHA and OCP) was attributed to the relatively slow resorption and slow mineralization of those substances (
Figure 3,
Figure 4 and
Figure 5). Despite the many advantages of OCP, its acid chemistry may not be a perfect combination for ideal bone substitutes, which will be addressed in a future study.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





