
A Three-Dimensional Printed Foot Orthosis for Flexible Flatfoot: An Exploratory Biomechanical Study on Arch Support Reinforcement and Undercut


 , ,
, ,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Recruitment
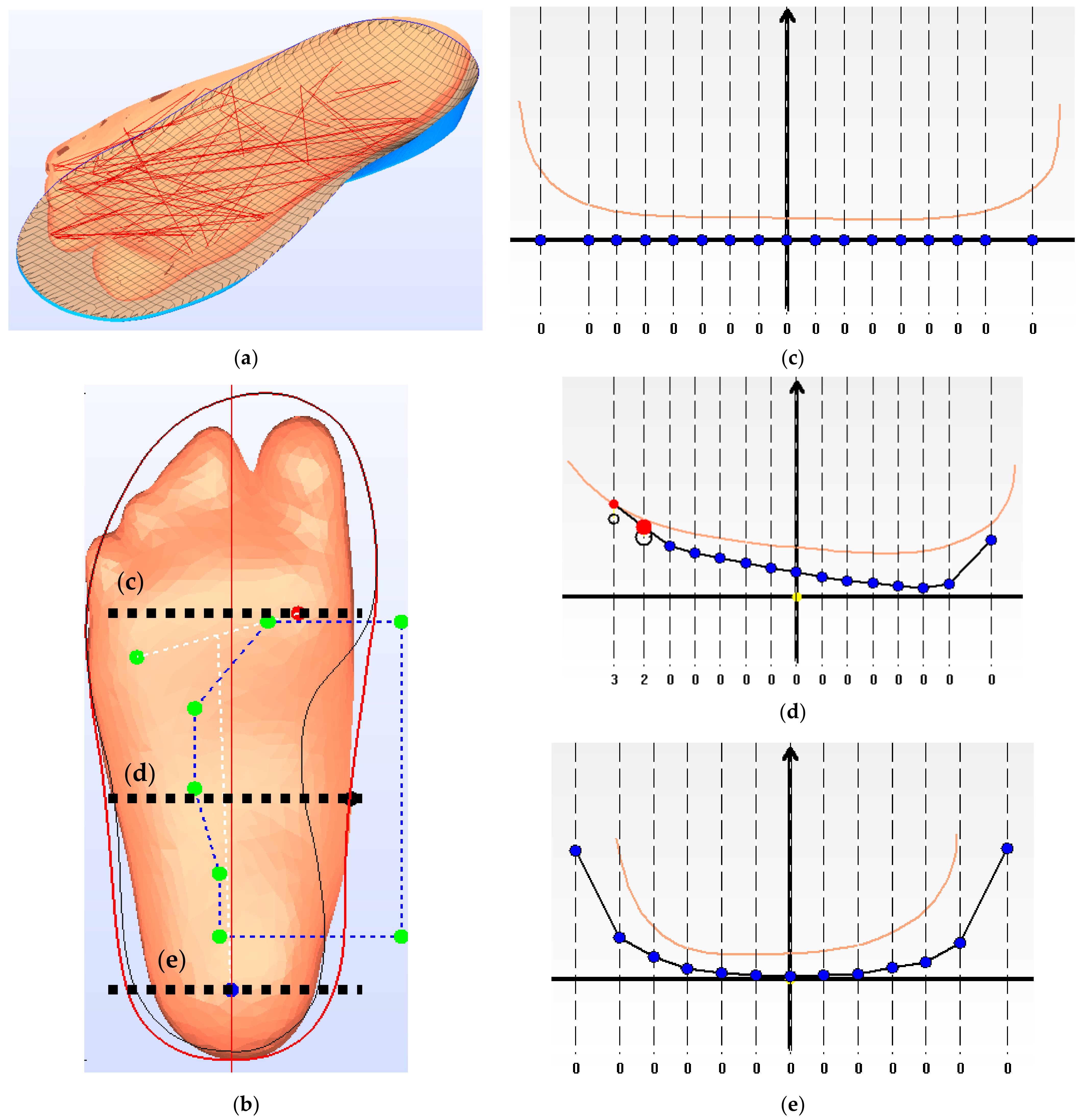
2.2. Foot Shape Acquisition
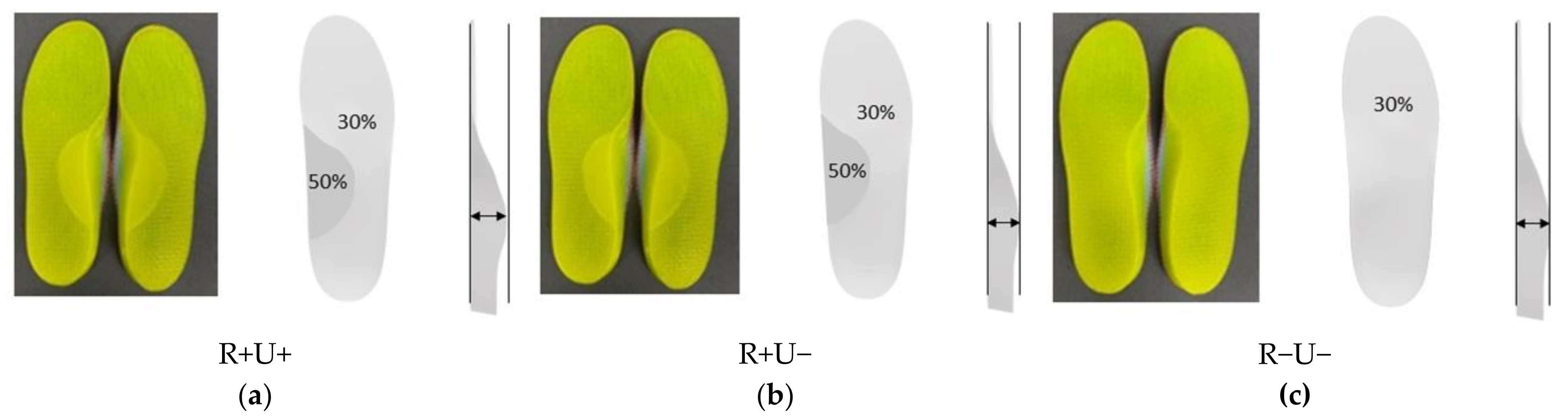
2.3. Generating Orthotic Insole Design
2.4. Fabrication of 3D Printed Insole
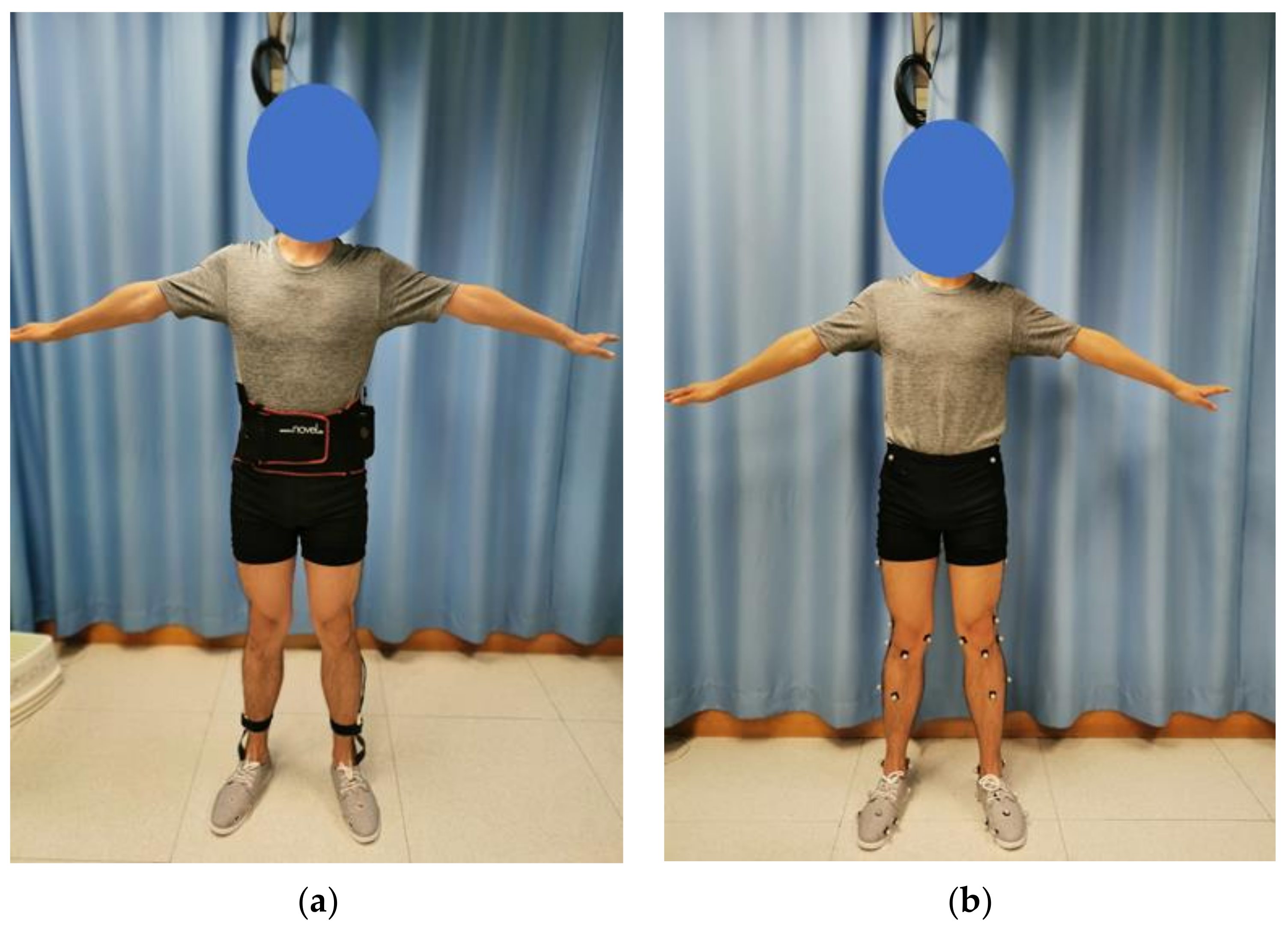
2.5. Experimental Evaluation
2.6. Outcome Measures and Statistical Analyses
3. Results
3.1. Foot Kinematics
3.2. Vertical Ground Reaction Force
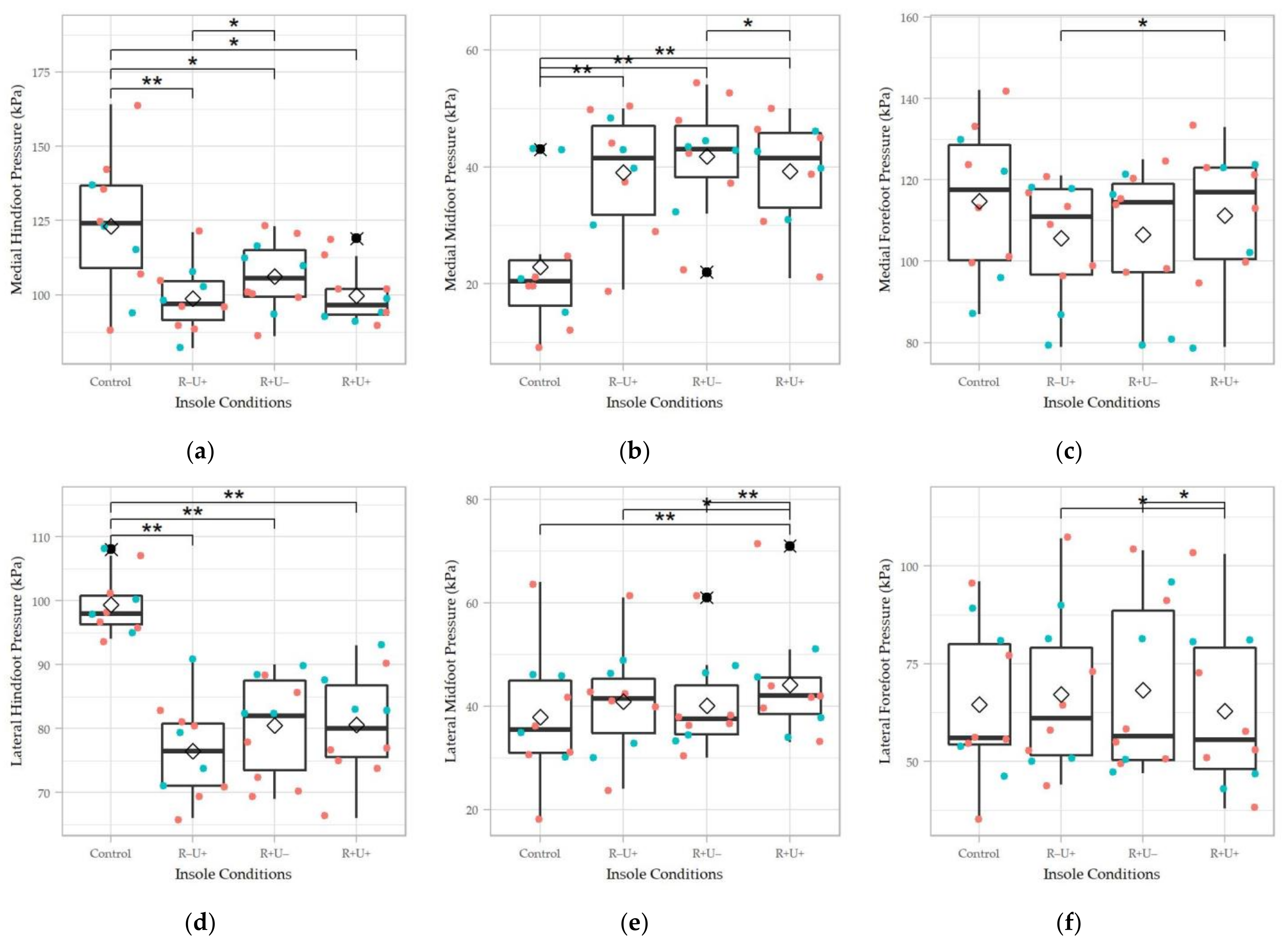
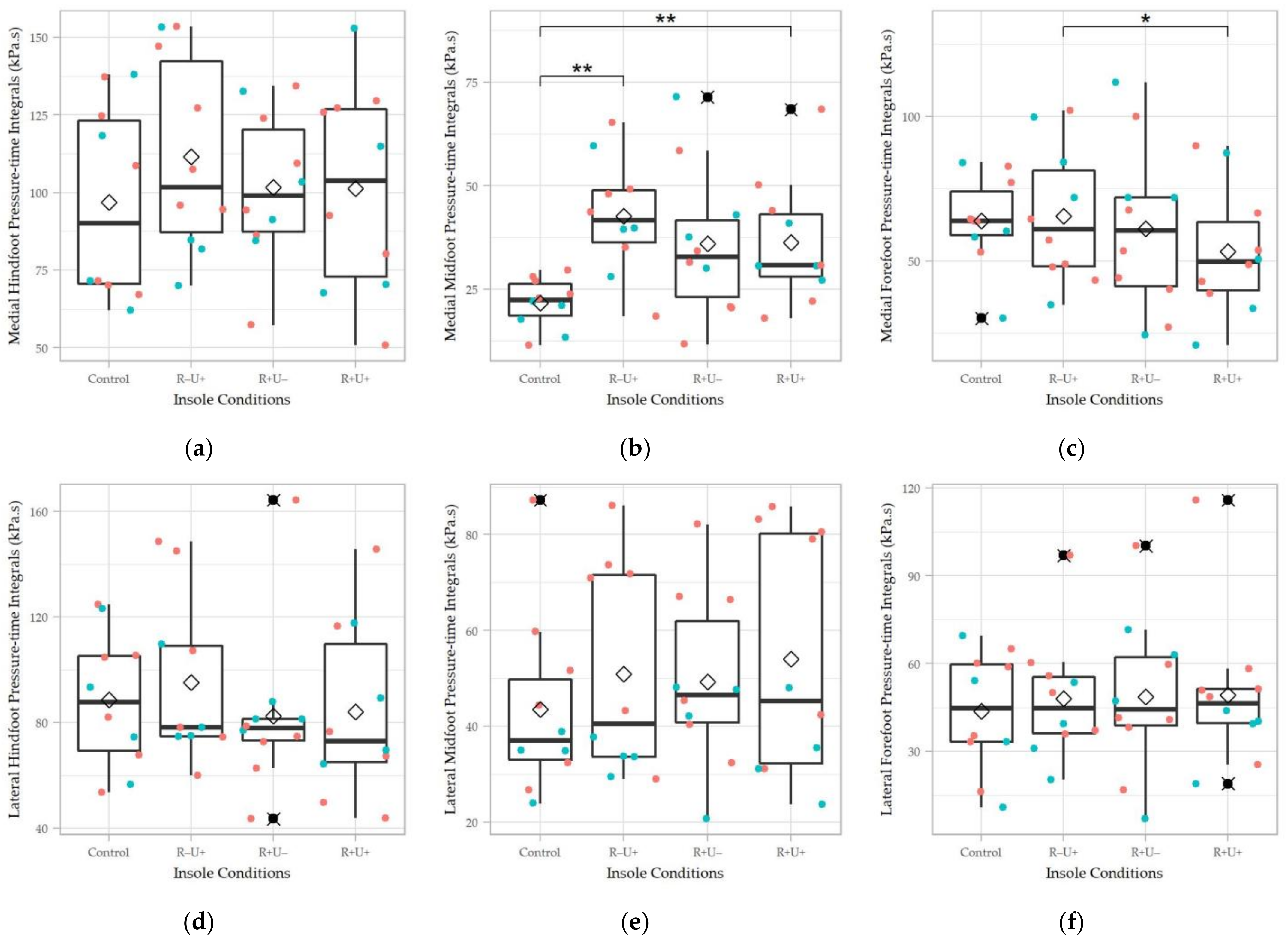
3.3. Plantar Pressure
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pinney, S.J.; Lin, S.S. Current concept review: Acquired adult flatfoot deformity. Foot Ankle Int. 2006, 27, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Aenumulapalli, A.; Kulkarni, M.M.; Gandotra, A.R. Prevalence of flexible flat foot in adults: A cross-sectional study. J. Clin. Diagn. Res. JCDR 2017, 11, AC17. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi-Demneh, E.; Jafarian, F.; Melvin, J.M.; Azadinia, F.; Shamsi, F.; Jafarpishe, M. Flatfoot in school-age children: Prevalence and associated factors. Foot Ankle Spec. 2015, 8, 186–193. [Google Scholar] [CrossRef]
- Harris, E.J.; Vanore, J.V.; Thomas, J.L.; Kravitz, S.R.; Mendelson, S.A.; Mendicino, R.W.; Silvani, S.H.; Gassen, S.C. Diagnosis and treatment of pediatric flatfoot. J. Foot Ankle Surg. 2004, 43, 341–373. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, M.G.; Ceccarelli, F.; Berti, L.; Luciani, D.; Catani, F.; Boschi, M.; Giannini, S. Diagnosis of flexible flatfoot in children: A systematic clinical approach. Orthopedics 2011, 34. [Google Scholar] [CrossRef]
- Cacace, L.A.; Hillstrom, H.J.; Dufour, A.B.; Hannan, M.T. The association between pes planus foot type and the prevalence of foot disorders: The Framingham foot study. Osteoarthr. Cartil. 2013, 21, S166–S167. [Google Scholar] [CrossRef] [Green Version]
- Gross, K.D.; Felson, D.T.; Niu, J.; Hunter, D.J.; Guermazi, A.; Roemer, F.W.; Dufour, A.B.; Gensure, R.H.; Hannan, M.T. Association of flat feet with knee pain and cartilage damage in older adults. Arthritis Care Res. 2011, 63, 937–944. [Google Scholar] [CrossRef] [Green Version]
- Tang, C.Y.K.; Ng, K.H.; Lai, J. Adult flatfoot. BMJ 2020, 368, m295. [Google Scholar] [CrossRef]
- Neville, C.G.; Houck, J.R. Choosing among 3 ankle-foot orthoses for a patient with stage II posterior tibial tendon dysfunction. J. Orthop. Sports Phys. Ther. 2009, 39, 816–824. [Google Scholar] [CrossRef] [Green Version]
- Flemister, A.S.; Neville, C.G.; Houck, J. The Relationship Between Ankle, Hindfoot, and Forefoot Position and Posterior Tibial Muscle Excursion. Foot Ankle Int. 2007, 28, 448–455. [Google Scholar] [CrossRef]
- Chou, L.B.; Wapner, K.L. Conservative Treatment of the Foot. In Mann’s Surgery of the Foot and Ankle; Coughlin, M.J., Saltzman, C.L., Eds.; Elsevier Saunders: Philadelphia, PA, USA, 2014. [Google Scholar]
- Desmyttere, G.; Hajizadeh, M.; Bleau, J.; Begon, M. Effect of foot orthosis design on lower limb joint kinematics and kinetics during walking in flexible pes planovalgus: A systematic review and meta-analysis. Clin. Biomech. 2018, 59, 117–129. [Google Scholar] [CrossRef] [PubMed]
- Dars, S.; Uden, H.; Banwell, H.A.; Kumar, S. The effectiveness of non-surgical intervention (Foot Orthoses) for paediatric flexible pes planus: A systematic review: Update. PLoS ONE 2018, 13, e0193060. [Google Scholar] [CrossRef]
- Tang, S.F.-T.; Chen, C.-H.; Wu, C.-K.; Hong, W.-H.; Chen, K.-J.; Chen, C.-K. The effects of total contact insole with forefoot medial posting on rearfoot movement and foot pressure distributions in patients with flexible flatfoot. Clin. Neurol. Neurosurg. 2015, 129, S8–S11. [Google Scholar] [CrossRef]
- Su, S.; Mo, Z.; Guo, J.; Fan, Y. The effect of arch height and material hardness of personalized insole on correction and tissues of flatfoot. J. Healthc. Eng. 2017, 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrios-Muriel, J.; Romero-Sánchez, F.; Alonso-Sánchez, F.J.; Rodriguez Salgado, D. Advances in orthotic and prosthetic manufacturing: A technology review. Materials 2020, 13, 295. [Google Scholar] [CrossRef] [Green Version]
- Choo, Y.J.; Boudier-Revéret, M.; Chang, M.C. 3D printing technology applied to orthosis manufacturing: Narrative review. Ann. Palliat. Med. 2020, 9, 4262–4270. [Google Scholar] [CrossRef] [PubMed]
- Davia-Aracil, M.; Hinojo-Pérez, J.J.; Jimeno-Morenilla, A.; Mora-Mora, H. 3D printing of functional anatomical insoles. Comput. Ind. 2018, 95, 38–53. [Google Scholar] [CrossRef] [Green Version]
- Staheli, L.T.; Chew, D.E.; Corbett, M. The longitudinal arch. A survey of eight hundred and eighty-two feet in normal children and adults. J. Bone Joint Surg. Am. Vol. 1987, 69, 426–428. [Google Scholar]
- Riccio, I.; Gimigliano, F.; Gimigliano, R.; Porpora, G.; Iolascon, G. Rehabilitative treatment in flexible flatfoot: A perspective cohort study. Musculoskelet. Surg. 2009, 93, 101. [Google Scholar] [CrossRef]
- Telfer, S.; Gibson, K.S.; Hennessy, K.; Steultjens, M.P.; Woodburn, J. Computer-aided design of customized foot orthoses: Reproducibility and effect of method used to obtain foot shape. Arch. Phys. Med. Rehabil. 2012, 93, 863–870. [Google Scholar] [CrossRef] [Green Version]
- Scherer, P.R. Custom Foot Orthoses. In Athletic Footwear and Orthoses in Sports Medicine; Werd, M.B., Knight, E.L., Eds.; Springer: New York, NY, USA, 2010. [Google Scholar]
- Mendes, A.A.M.T.; de Almeida Silva, H.J.; Costa, A.R.A.; Pinheiro, Y.T.; de Almeida Lins, C.A.; de Souza, M.C. Main types of insoles described in the literature and their applicability for musculoskeletal disorders of the lower limbs: A systematic review of clinical studies. J. Bodyw. Mov. Ther. 2020, 24, 29–36. [Google Scholar] [CrossRef]
- Carson, M.; Harrington, M.; Thompson, N.; O’connor, J.; Theologis, T. Kinematic analysis of a multi-segment foot model for research and clinical applications: A repeatability analysis. J. Biomech. 2001, 34, 1299–1307. [Google Scholar] [CrossRef]
- Wong, D.W.-C.; Lam, W.K.; Yeung, L.; Lee, W.C. Does long-distance walking improve or deteriorate walking stability of transtibial amputees? Clin. Biomech. 2015, 30, 867–873. [Google Scholar] [CrossRef]
- Ma, C.Z.-H.; Zheng, Y.-P.; Lee, W.C.-C. Changes in gait and plantar foot loading upon using vibrotactile wearable biofeedback system in patients with stroke. Top. Stroke Rehabil. 2018, 25, 20–27. [Google Scholar] [CrossRef]
- McGill, R.; Tukey, J.W.; Larsen, W.A. Variations of box plots. Am. Stat. 1978, 32, 12–16. [Google Scholar]
- Ahmed, S.; Barwick, A.; Butterworth, P.; Nancarrow, S. Footwear and insole design features that reduce neuropathic plantar forefoot ulcer risk in people with diabetes: A systematic literature review. J. Foot Ankle Res. 2020, 13, 1–13. [Google Scholar] [CrossRef]
- Jiang, Y.; Wang, D.; Ying, J.; Chu, P.; Qian, Y.; Chen, W. Design and Preliminary Validation of Individual Customized Insole for Adults with Flexible Flatfeet Based on the Plantar Pressure Redistribution. Sensors 2021, 21, 1780. [Google Scholar] [CrossRef] [PubMed]
- Levinger, P.; Murley, G.S.; Barton, C.J.; Cotchett, M.P.; McSweeney, S.R.; Menz, H.B. A comparison of foot kinematics in people with normal- and flat-arched feet using the Oxford Foot Model. Gait Posture 2010, 32, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Kido, M.; Ikoma, K.; Hara, Y.; Imai, K.; Maki, M.; Ikeda, T.; Fujiwara, H.; Tokunaga, D.; Inoue, N.; Kubo, T. Effect of therapeutic insoles on the medial longitudinal arch in patients with flatfoot deformity: A three-dimensional loading computed tomography study. Clin. Biomech. 2014, 29, 1095–1098. [Google Scholar] [CrossRef] [Green Version]
- Mo, S.; Leung, S.H.; Chan, Z.Y.; Sze, L.K.; Mok, K.-M.; Yung, P.S.; Ferber, R.; Cheung, R.T. The biomechanical difference between running with traditional and 3D printed orthoses. J. Sports Sci. 2019, 37, 2191–2197. [Google Scholar] [CrossRef]
- Telfer, S.; Abbott, M.; Steultjens, M.P.; Woodburn, J. Dose–response effects of customised foot orthoses on lower limb kinematics and kinetics in pronated foot type. J. Biomech. 2013, 46, 1489–1495. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, M.U.; Brunt, D.; Vander Linden, D. The effect of foot orthotics and gait velocity on lower limb kinematics and temporal events of stance. J. Orthop. Sports Phys. Ther. 1993, 17, 2–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aminian, G.; Safaeepour, Z.; Farhoodi, M.; Pezeshk, A.F.; Saeedi, H.; Majddoleslam, B. The effect of prefabricated and proprioceptive foot orthoses on plantar pressure distribution in patients with flexible flatfoot during walking. Prosthet. Orthot. Int. 2013, 37, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Wahmkow, G.; Cassel, M.; Mayer, F.; Baur, H. Effects of different medial arch support heights on rearfoot kinematics. PLoS ONE 2017, 12, e0172334. [Google Scholar] [CrossRef] [PubMed]
- Needleman, R.L. Current topic review: Subtalar arthroereisis for the correction of flexible flatfoot. Foot Ankle Int. 2005, 26, 336–346. [Google Scholar] [CrossRef]
- Hösl, M.; Böhm, H.; Multerer, C.; Döderlein, L. Does excessive flatfoot deformity affect function? A comparison between symptomatic and asymptomatic flatfeet using the Oxford Foot Model. Gait Posture 2014, 39, 23–28. [Google Scholar] [CrossRef]
- Salles, A.S.; Gyi, D.E. An evaluation of personalised insoles developed using additive manufacturing. J. Sports Sci. 2013, 31, 442–450. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Lou, S.-Z.; Huang, C.-Y.; Su, F.-C. Effects of foot orthoses on gait patterns of flat feet patients. Clin. Biomech. 2010, 25, 265–270. [Google Scholar] [CrossRef]
- Ng, J.W.; Chong, L.J.; Pan, J.W.; Lam, W.-K.; Ho, M.; Kong, P.W. Effects of foot orthosis on ground reaction forces and perception during short sprints in flat-footed athletes. Res. Sports Med. 2021, 29, 43–55. [Google Scholar] [CrossRef]
- Telfer, S.; Woodburn, J.; Collier, A.; Cavanagh, P. Virtually optimized insoles for offloading the diabetic foot: A randomized crossover study. J. Biomech. 2017, 60, 157–161. [Google Scholar] [CrossRef] [Green Version]
- Jin, H.; Xu, R.; Wang, S.; Wang, J. Use of 3D-Printed Heel Support Insoles Based on Arch Lift Improves Foot Pressure Distribution in Healthy People. Med. Sci. Monit. 2019, 25, 7175–7181. [Google Scholar] [CrossRef] [PubMed]
- Tarrade, T.; Doucet, F.; Saint-Lô, N.; Llari, M.; Behr, M. Are custom-made foot orthoses of any interest on the treatment of foot pain for prolonged standing workers? Appl. Ergon. 2019, 80, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-P.; Peng, H.-T.; Wang, X.; Chen, Z.-R.; Song, C.-Y. The arch support insoles show benefits to people with flatfoot on stance time, cadence, plantar pressure and contact area. PLoS ONE 2020, 15, e0237382. [Google Scholar] [CrossRef]
- Laughton, C.; McClay Davis, I.; Williams, D.S. A comparison of four methods of obtaining a negative impression of the foot. J. Am. Podiatr. Med. Assoc. 2002, 92, 261–268. [Google Scholar] [CrossRef]
- Carroll, M.; Annabell, M.-E.; Rome, K. Reliability of capturing foot parameters using digital scanning and the neutral suspension casting technique. J. Foot Ankle Res. 2011, 4, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Jandova, S.; Mendricky, R. Benefits of 3D Printed and Customized Anatomical Footwear Insoles for Plantar Pressure Distribution. 3d Print. Addit. Manuf. 2021, in press. [Google Scholar]
- Ball, K.A.; Afheldt, M.J. Evolution of foot orthotics—Part 1: Coherent theory or coherent practice? J. Manip. Physiol. Ther. 2002, 25, 116–124. [Google Scholar] [CrossRef] [Green Version]
- Barn, R.; Brandon, M.; Rafferty, D.; Sturrock, R.D.; Steultjens, M.; Turner, D.E.; Woodburn, J. Kinematic, kinetic and electromyographic response to customized foot orthoses in patients with tibialis posterior tenosynovitis, pes plano valgus and rheumatoid arthritis. Rheumatology 2014, 53, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Peng, Y.; Wang, Y.; Wong, D.W.-C.; Chen, T.L.-W.; Zhang, G.; Tan, Q.; Zhang, M. Extrinsic foot muscle forces and joint contact forces in flexible flatfoot adult with foot orthosis: A parametric study of tibialis posterior muscle weakness. Gait Posture 2021, 88, 54–59. [Google Scholar] [CrossRef]
- Peng, Y.; Wong, D.W.-C.; Wang, Y.; Chen, T.L.-W.; Tan, Q.; Chen, Z.; Jin, Z.; Zhang, M. Immediate effects of medially posted insoles on lower limb joint contact forces in adult acquired flatfoot: A pilot study. Int. J. Environ. Res. Public Health 2020, 17, 2226. [Google Scholar] [CrossRef] [Green Version]
- Peng, Y.; Wong, D.W.-C.; Wang, Y.; Chen, T.L.-W.; Zhang, G.; Yan, F.; Zhang, M. Computational models of flatfoot with three-dimensional fascia and bulk soft tissue interaction for orthosis design. Med. Nov. Technol. Devices 2021, 9, 100050. [Google Scholar]
- Nozaki, S.; Watanabe, K.; Teramoto, A.; Kamiya, T.; Katayose, M.; Ogihara, N. Sex-and age-related variations in the three-dimensional orientations and curvatures of the articular surfaces of the human talus. Anat. Sci. Int. 2021, 96, 258–264. [Google Scholar] [CrossRef]
- Ross, M.H.; Smith, M.D.; Vicenzino, B. Reported selection criteria for adult acquired flatfoot deformity and posterior tibial tendon dysfunction: Are they one and the same? A systematic review. PLoS ONE 2017, 12, e0187201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, D.W.-C.; Wang, Y.; Leung, A.K.-L.; Yang, M.; Zhang, M. Finite element simulation on posterior tibial tendinopathy: Load transfer alteration and implications to the onset of pes planus. Clin. Biomech. 2018, 51, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Mickle, K.J.; Munro, B.J.; Lord, S.R.; Menz, H.B.; Steele, J.R. Foot shape of older people: Implications for shoe design. Footwear Sci. 2010, 2, 131–139. [Google Scholar] [CrossRef]
- Luo, X.D.; Xue, C.-H.; Li, Y. Study on the foot shape characteristics of the elderly in China. Foot 2017, 33, 68–75. [Google Scholar] [CrossRef]
- Tomassoni, D.; Traini, E.; Amenta, F. Gender and age related differences in foot morphology. Maturitas 2014, 79, 421–427. [Google Scholar] [CrossRef]
- Chiu, M.-C.; Wu, H.-C.; Chang, L.-Y.; Wu, M.-H. Center of pressure progression characteristics under the plantar region for elderly adults. Gait Posture 2013, 37, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Kernozek, T.; LaMott, E. Comparisons of plantar pressures between the elderly and young adults. Gait Posture 1995, 3, 143–148. [Google Scholar] [CrossRef]
- Han, K.-H.; Bae, K.-H.; Jung, H.-G.; Ha, M.-S.; Choi, D.-Y.; Lee, J.-S.; Yang, J.-O. Comparison of plantar pressure and COP parameters in three types of arch support insole during stair descent in elderly with flatfoot. J. Korean Appl. Sci. Technol. 2018, 35, 948–955. [Google Scholar]
- Kerr, C.; Zavatsky, A.; Theologis, T.; Stebbins, J. Kinematic differences between neutral and flat feet with and without symptoms as measured by the Oxford foot model. Gait Posture 2019, 67, 213–218. [Google Scholar] [CrossRef]
- Shin, H.S.; Lee, J.H.; Kim, E.J.; Kyung, M.G.; Yoo, H.J.; Lee, D.Y. Flatfoot deformity affected the kinematics of the foot and ankle in proportion to the severity of deformity. Gait Posture 2019, 72, 123–128. [Google Scholar] [CrossRef]
- Cheung, J.T.-M.; Zhang, M. Parametric design of pressure-relieving foot orthosis using statistics-based finite element method. Med Eng. Phys. 2008, 30, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Lv, M.L.; Yang, J.; Niu, W.; Cheung, J.C.-W.; Sun, W.; Wong, D.W.-C.; Ni, M. Computational modelling of foot orthosis for midfoot arthritis: A Taguchi approach for design optimization. Acta Bioeng. Biomech. 2020, 22, 75–83. [Google Scholar] [CrossRef]
- Peng, Y.; Wong, D.W.-C.; Chen, T.L.-W.; Wang, Y.; Zhang, G.; Yan, F.; Zhang, M. Influence of arch support heights on the internal foot mechanics of flatfoot during walking: A muscle-driven finite element analysis. Comput. Biol. Med. 2021, 132, 104355. [Google Scholar] [CrossRef]
- Yoon, J.-G.; Yoo, K.-T.; Lee, J.-H.; Park, J.-M.; Min, K.-O.; Choi, J.-H. The analysis of Lower Limb Muscle Activity and Motion Analysis according to Normal Foot and Flatfoot during Walking. J. Int. Acad. Phys. Ther. Res. 2012, 3, 364–369. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, K.-W.; Peng, Y.; Chen, T.L.-W.; Zhang, G.; Cheung, J.C.-W.; Lam, W.-K.; Wong, D.W.-C.; Zhang, M. A Three-Dimensional Printed Foot Orthosis for Flexible Flatfoot: An Exploratory Biomechanical Study on Arch Support Reinforcement and Undercut. Materials 2021, 14, 5297. https://doi.org/10.3390/ma14185297
Cheng K-W, Peng Y, Chen TL-W, Zhang G, Cheung JC-W, Lam W-K, Wong DW-C, Zhang M. A Three-Dimensional Printed Foot Orthosis for Flexible Flatfoot: An Exploratory Biomechanical Study on Arch Support Reinforcement and Undercut. Materials. 2021; 14(18):5297. https://doi.org/10.3390/ma14185297
Chicago/Turabian StyleCheng, Ka-Wing, Yinghu Peng, Tony Lin-Wei Chen, Guoxin Zhang, James Chung-Wai Cheung, Wing-Kai Lam, Duo Wai-Chi Wong, and Ming Zhang. 2021. "A Three-Dimensional Printed Foot Orthosis for Flexible Flatfoot: An Exploratory Biomechanical Study on Arch Support Reinforcement and Undercut" Materials 14, no. 18: 5297. https://doi.org/10.3390/ma14185297