
The Effect of Core Stabilization Training on Improving Gait and Self-Perceived Function in Patients with Knee Osteoarthritis: A Single-Arm Clinical Trial

Abstract
:1. Introduction
Purpose and Hypotheses
2. Materials and Methods
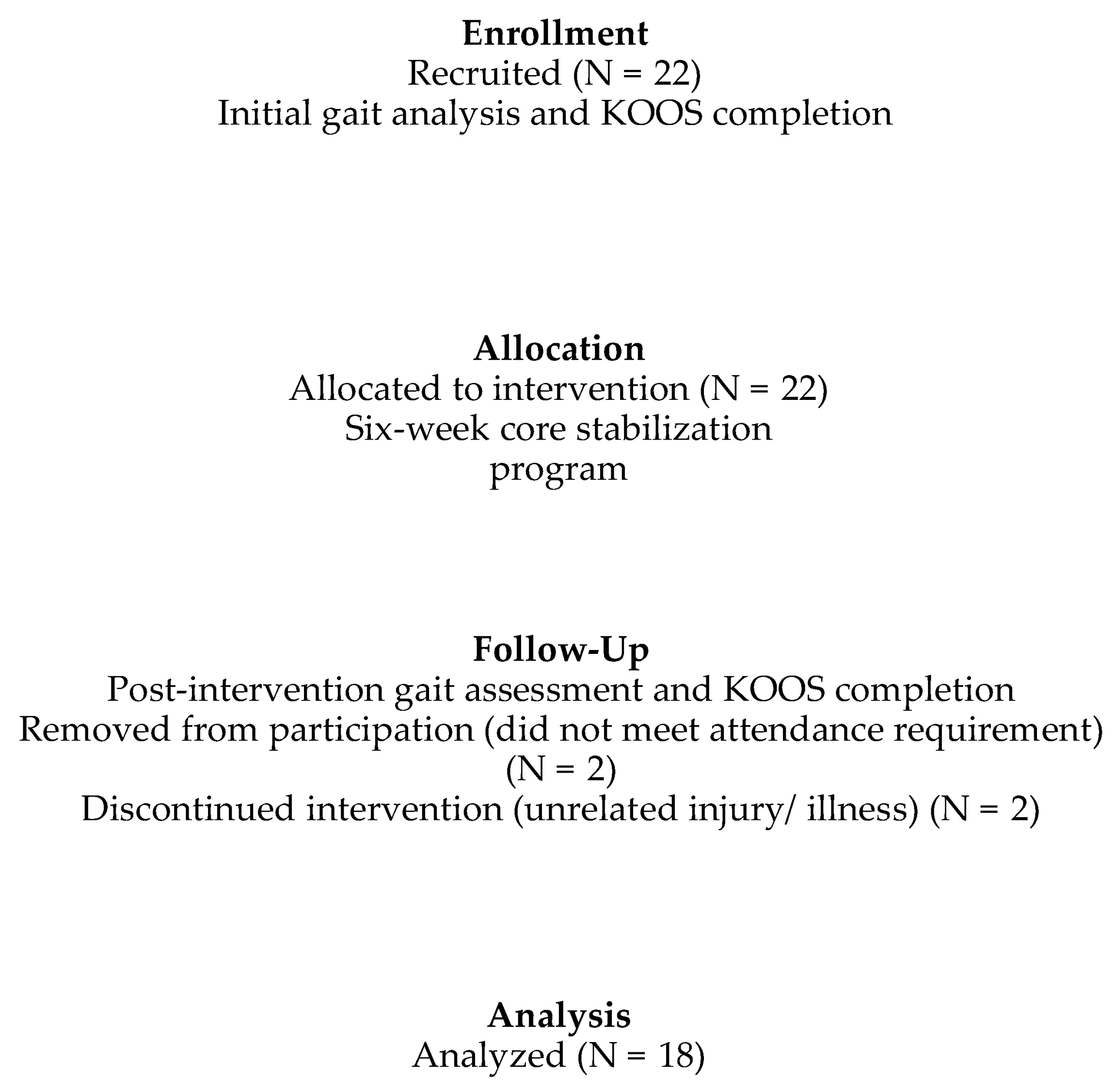
2.1. Participants
2.2. Instrumentation
2.3. Procedures
2.4. Data Processing
2.5. Data Analysis
3. Results
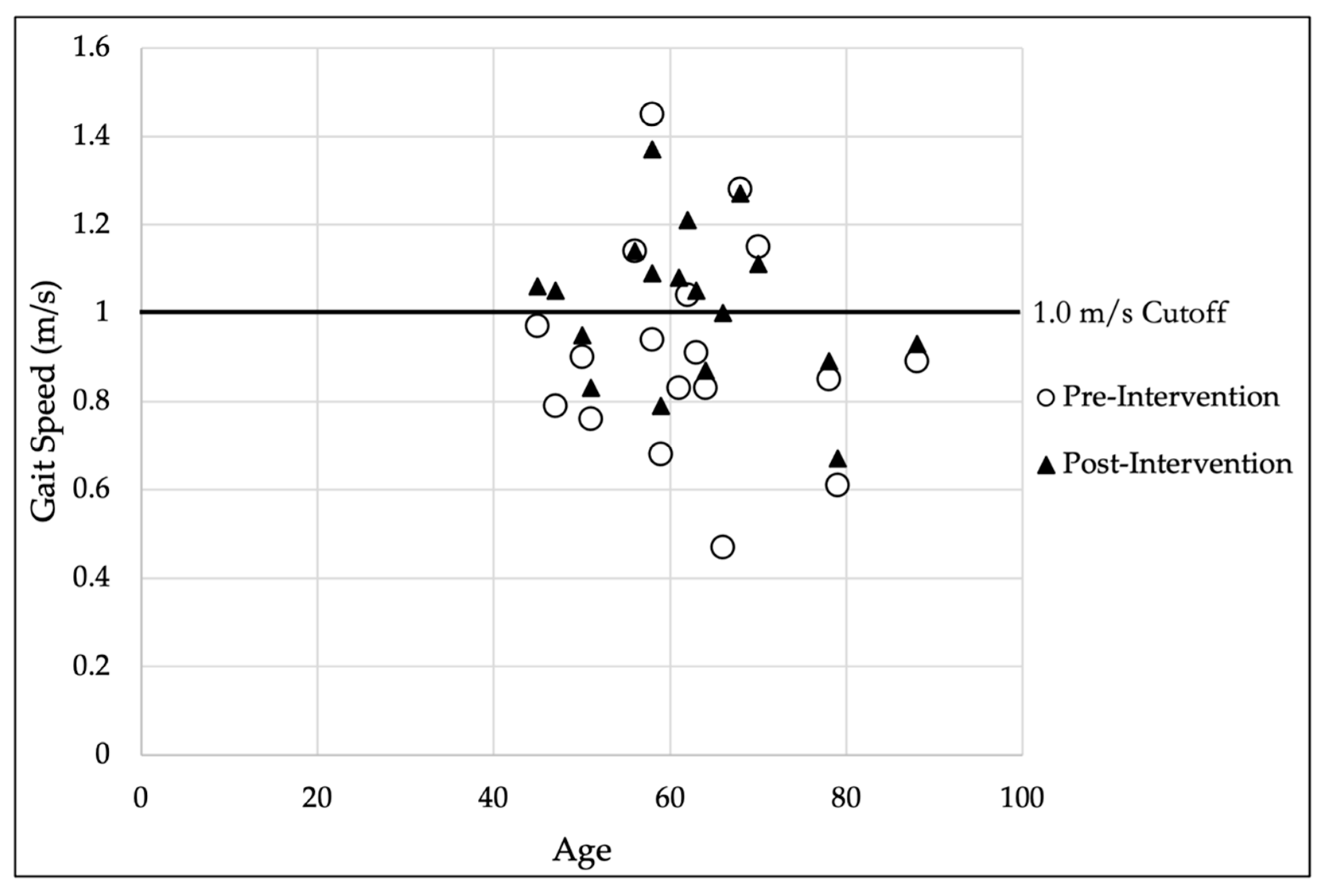
3.1. Gait Analysis
3.2. KOOS Analysis
3.3. Dose–Response Analysis
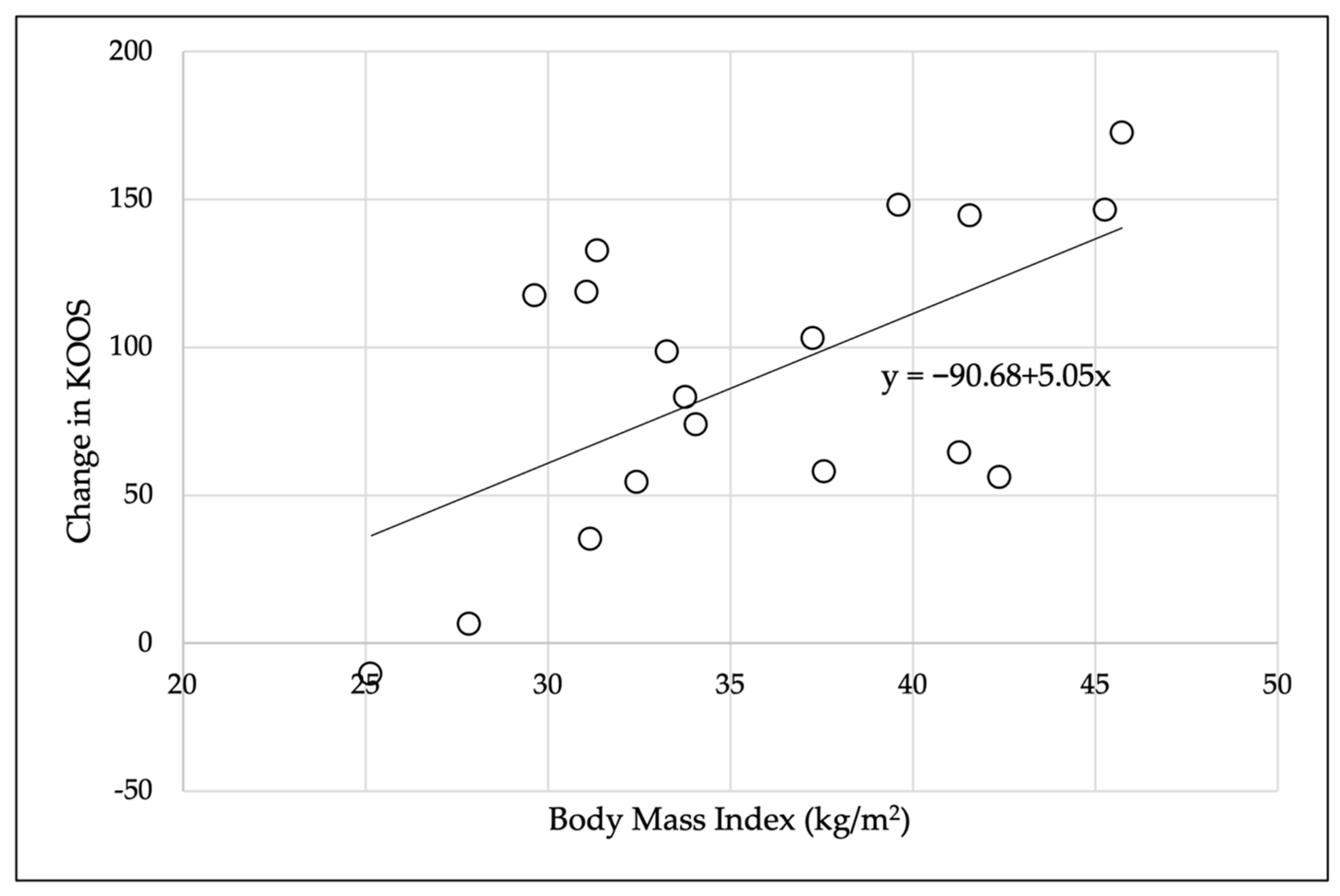
3.4. Correlation Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Long, H.; Liu, Q.; Yin, H.; Wang, K.; Diao, N.; Zhang, Y.; Lin, J.; Guo, A. Prevalence trends of site-specific osteoarthritis from 1990 to 2019: Findings from the Global Burden of Disease Study 2019. Arthritis Rheumatol. 2022, 74, 1172–1183. [Google Scholar] [CrossRef] [PubMed]
- Palazzo, C.; Nguyen, C.; Lefevre-Colau, M.-M.; Rannou, F.; Poiraudeau, S. Risk factors and burden of osteoarthritis. Ann. Phys. Rehabil. Med. 2016, 59, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Bannuru, R.R.; Osani, M.; Vaysbrot, E.; Arden, N.; Bennell, K.; Bierma-Zeinstra, S.; Kraus, V.; Lohmander, L.S.; Abbott, J.; Bhandari, M. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef]
- Thorlund, J.B.; Simic, M.; Pihl, K.; Berthelsen, D.B.; Day, R.; Koes, B.; Juhl, C.B. Similar effects of exercise therapy, nonsteroidal anti-inflammatory drugs, and opioids for knee osteoarthritis pain: A systematic review with network meta-analysis. J. Orthop. Sports Phys. Ther. 2022, 52, 207–216. [Google Scholar] [CrossRef]
- Skou, S.T.; Pedersen, B.K.; Abbott, J.H.; Patterson, B.; Barton, C. Physical activity and exercise therapy benefit more than just symptoms and impairments in people with hip and knee osteoarthritis. J. Orthop. Sports Phys. Ther. 2018, 48, 439–447. [Google Scholar] [CrossRef]
- Weick, J.W.; Bawa, H.S.; Dirschl, D.R. Hyaluronic acid injections for treatment of advanced osteoarthritis of the knee: Utilization and cost in a national population sample. J. Bone Jt. Surg. Am. Vol. 2016, 98, 1429–1435. [Google Scholar] [CrossRef]
- Teo, P.L.; Hinman, R.S.; Egerton, T.; Dziedzic, K.S.; Bennell, K.L. Identifying and prioritizing clinical guideline recommendations most relevant to physical therapy practice for hip and/or knee osteoarthritis. J. Orthop. Sports Phys. Ther. 2019, 49, 501–512. [Google Scholar] [CrossRef]
- Duffell, L.D.; Jordan, S.J.; Cobb, J.P.; McGregor, A.H. Gait adaptations with aging in healthy participants and people with knee-joint osteoarthritis. Gait Posture 2017, 57, 246–251. [Google Scholar] [CrossRef]
- Flowers, D.W.; Brewer, W.; Ellison, J.; Mitchell, K.; Frilot, C. Transversus abdominis activation does not alter gait impairments in patients with and without knee osteoarthritis. Clin. Biomech. 2021, 82, 105270. [Google Scholar] [CrossRef]
- Favre, J.; Erhart-Hledik, J.C.; Andriacchi, T.P. Age-related differences in sagittal-plane knee function at heel-strike of walking are increased in osteoarthritic patients. Osteoarthr. Cartil. 2014, 22, 464–471. [Google Scholar] [CrossRef] [Green Version]
- Kumar, D.; Manal, K.T.; Rudolph, K.S. Knee joint loading during gait in healthy controls and individuals with knee osteoarthritis. Osteoarthr. Cartil. 2013, 21, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Landry, S.C.; McKean, K.A.; Hubley-Kozey, C.L.; Stanish, W.D.; Deluzio, K.J. Knee biomechanics of moderate OA patients measured during gait at a self-selected and fast walking speed. J. Biomech. 2007, 40, 1754–1761. [Google Scholar] [CrossRef]
- Zeni, J.A., Jr.; Higginson, J.S. Differences in gait parameters between healthy subjects and persons with moderate and severe knee osteoarthritis: A result of altered walking speed? Clin. Biomech. 2009, 24, 372–378. [Google Scholar] [CrossRef]
- Flowers, D.W.; Brewer, W.; Mitchell, K.; Ellison, J. Why are we neglecting the core muscles in patients with knee osteoarthritis? A narrative review of the literature. Phys. Ther. Rev. 2021, 26, 276–283. [Google Scholar] [CrossRef]
- Hsieh, R.-L.; Lee, W.-C.; Lo, M.-T.; Liao, W.-C. Postural stability in patients with knee osteoarthritis: Comparison with controls and evaluation of relationships between postural stability scores and international classification of functioning, disability and health components. Arch. Phys. Med. Rehabil. 2013, 94, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Linley, H.S.; Sled, E.A.; Culham, E.G.; Deluzio, K.J. A biomechanical analysis of trunk and pelvis motion during gait in subjects with knee osteoarthritis compared to control subjects. Clin. Biomech. 2010, 25, 1003–1010. [Google Scholar] [CrossRef]
- Daud, D.M.B.A.; Razak, N.R.A.; Lasimbang, H. Core stability deficits in female knee osteoarthritis patients. Acad. J. Sci. 2015, 4, 117–124. [Google Scholar]
- Azuma, K.; Sera, Y.; Shinjo, T.; Takayama, M.; Shiomi, E.; Momoshima, S.; Iwao, Y.; Ishida, H.; Matsumoto, H. Maintenance of the paraspinal muscles may protect against radiographic knee osteoarthritis. Open Access Rheumatol. Res. Rev. 2017, 9, 151–158. [Google Scholar] [CrossRef]
- Tang, S.F.; Chen, C.P.; Chen, M.J.; Pei, Y.-C.; Lau, Y.-C.; Leong, C.-P. Changes in sagittal ground reaction forces after intra-articular hyaluronate injections for knee osteoarthritis. Arch. Phys. Med. Rehabil. 2004, 85, 951–955. [Google Scholar] [CrossRef]
- Roos, E.M.; Lohmander, L.S. The Knee Injury and Osteoarthritis Outcome Score (KOOS): From joint injury to osteoarthritis. Health Qual. Life Outcomes 2003, 1, 64. [Google Scholar] [CrossRef]
- Oishi, K.; Tsuda, E.; Yamamoto, Y.; Maeda, S.; Sasaki, E.; Chiba, D.; Takahashi, I.; Nakaji, S.; Ishibashi, Y. The Knee Injury and Osteoarthritis Outcome Score reflects the severity of knee osteoarthritis better than the revised Knee Society Score in a general Japanese population. Knee 2016, 23, 35–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granacher, U.; Lacroix, A.; Muehlbauer, T.; Roettger, K.; Gollhofer, A. Effects of core instability strength training on trunk muscle strength, spinal mobility, dynamic balance and functional mobility in older adults. Gerontology 2013, 59, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Kisner, C.; Thorp, J. The spine: Exercise and manipulation interventions. In Therapeutic Exercise: Foundations and Techniques, 6th ed.; Kisner, C., Colby, L., Eds.; F.A. Davis: Philadelphia, PA, USA, 2012; pp. 485–538. [Google Scholar]
- Hernandez, D.; Dimaro, M.; Navarro, E.; Dorado, J.; Accoce, M.; Salzberg, S.; Policastro, P.O. Efficacy of core exercises in patients with osteoarthritis of the knee: A randomized controlled clinical trial. J. Bodyw. Mov. Ther. 2019, 23, 881–887. [Google Scholar] [CrossRef]
- Young, J.L.; Rhon, D.I.; Cleland, J.A.; Snodgrass, S.J. The influence of exercise dosing on outcomes in patients with knee disorders: A systematic review. J. Orthop. Sports Phys. Ther. 2018, 48, 146–161. [Google Scholar] [CrossRef] [PubMed]
- Kaushal, S. Missing data in clinical trials: Pitfalls and remedies. Int. J. Appl. Basic Med. Res. 2014, 4, S6–S7. [Google Scholar] [CrossRef]
- Tabachnick, B.; Fidell, L. Using Multivariate Statistics, 4th ed.; Allyn & Bacon: Needham Heights, MA, USA, 2001. [Google Scholar]
- Acock, A.C. Working With Missing Values. J. Marriage Fam. 2005, 67, 1012–1028. [Google Scholar] [CrossRef]
- van Buuren, S. Flexible Imputation of Missing Data; CRC Press LLC: London, UK, 2012. [Google Scholar]
- Goldberg, A.; Schepens, S. Measurement error and minimum detectable change in 4-meter gait speed in older adults. Aging Clin. Exp. Res. 2011, 23, 406–412. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Glenney, S.S. Minimal clinically important difference for change in comfortable gait speed of adults with pathology: A systematic review. J. Eval. Clin. Pract. 2014, 20, 295–300. [Google Scholar] [CrossRef]
- Chui, K.; Hood, E.; Klima, D. Meaningful change in walking speed. Top. Geriatr. Rehabil. 2012, 28, 97–103. [Google Scholar] [CrossRef]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait speed and survival in older adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef]
- Fritz, S.; Lusardi, M. Walking speed: The sixth vital sign. J. Geriatr. Phys. Ther. 2009, 32, 46–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Middleton, A.; Fritz, S.L.; Lusardi, M. Walking speed: The functional vital sign. J. Aging Phys. Act. 2015, 23, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Williams Andrews, A. Normal walking speed: A descriptive meta-analysis. Physiotherapy 2011, 97, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Birmingham, T.B.; Hunt, M.A.; Jones, I.C.; Jenkyn, T.R.; Giffin, J.R. Test-retest reliability of the peak knee adduction moment during walking in patients with medial compartment knee osteoarthritis. Arthritis Rheum. 2007, 57, 1012–1017. [Google Scholar] [CrossRef]
- Huang, S.-C.; Wei, I.P.; Chien, H.-L.; Wang, T.-M.; Liu, Y.-H.; Chen, H.-L.; Lu, T.-W.; Lin, J.-G. Effects of severity of degeneration on gait patterns in patients with medial knee osteoarthritis. Med. Eng. Phys. 2008, 30, 997–1003. [Google Scholar] [CrossRef]
- Kibler, W.B.; Press, J.; Sciascia, A. The role of core stability in athletic function. Sports Med. 2006, 36, 189–198. [Google Scholar] [CrossRef]
- D’Souza, N.; Charlton, J.; Grayson, J.; Kobayashi, S.; Hutchison, L.; Hunt, M.; Simic, M. Are biomechanics during gait associated with the structural disease onset and progression of lower limb osteoarthritis? A systematic review and meta-analysis. Osteoarthr. Cartil. 2021, 30, 381–394. [Google Scholar] [CrossRef]
- Simic, M.; Hinman, R.S.; Wrigley, T.V.; Bennell, K.L.; Hunt, M.A. Gait modification strategies for altering medial knee joint load: A systematic review. Arthritis Care Res. 2011, 63, 405–426. [Google Scholar] [CrossRef]
- Mundermann, A.; Dyrby, C.O.; Hurwitz, D.E.; Sharma, L.; Andriacchi, T.P. Potential strategies to reduce medial compartment loading in patients with knee osteoarthritis of varying severity: Reduced walking speed. Arthritis Rheum. 2004, 50, 1172–1178. [Google Scholar] [CrossRef]
- Andriacchi, T.P.; Mundermann, A.; Smith, R.L.; Alexander, E.J.; Dyrby, C.O.; Koo, S. A framework for the in vivo pathomechanics of osteoarthritis at the knee. Ann. Biomed. Eng. 2004, 32, 447–457. [Google Scholar] [CrossRef]
- Powers, C.M. The influence of abnormal hip mechanics on knee injury: A biomechanical perspective. J. Orthop. Sports Phys. Ther. 2010, 40, 42–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anders, C.; Wagner, H.; Puta, C.; Grassme, R.; Petrovitch, A.; Scholle, H.-C. Trunk muscle activation patterns during walking at different speeds. J. Electromyogr. Kinesiol. Off. J. Int. Soc. Electrophysiol. Kinesiol. 2007, 17, 245–252. [Google Scholar] [CrossRef]
- Collins, N.J.; Misra, D.; Felson, D.T.; Crossley, K.M.; Roos, E.M. Measures of knee function: International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS), Knee Outcome Survey Activities of Daily Living Scale (KOS-ADL), Lysholm Knee Scoring Scale, Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Activity Rating Scale (ARS), and Tegner Activity Score (TAS). Arthritis Care Res. 2011, 63 (Suppl. S11), S208–S228. [Google Scholar] [CrossRef]
- Kuntz, A.B.; Chopp-Hurley, J.N.; Brenneman, E.C.; Karampatos, S.; Wiebenga, E.G.; Adachi, J.D.; Noseworthy, M.D.; Maly, M.R. Efficacy of a biomechanically-based yoga exercise program in knee osteoarthritis: A randomized controlled trial. PLoS ONE 2018, 13, e0195653. [Google Scholar] [CrossRef]
- Whittaker, J.; Truong, L.; Dhiman, K.; Beck, C. Osteoarthritis year in review 2020: Rehabilitation and outcomes. Osteoarthr. Cartil. 2021, 29, 190–207. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Mean (SD) | Minimum | Maximum |
|---|---|---|---|
| Age (years) | 62.39 (11.36) | 45 | 88 |
| Height (m) | 1.65 (0.08) | 1.56 | 1.84 |
| Weight (kg) | 97.20 (19.39) | 61.36 | 127.73 |
| BMI (kg/m2) | 35.58 (6.03) | 25.15 | 45.75 |
| Leg Length (cm) a | 87.14 (5.22) | 78 | 101 |
| Knee Width (cm) a | 11.77 (0.94) | 10.30 | 13.50 |
| Ankle Width (cm) a | 7.18 (0.55) | 6.40 | 8.40 |
| Variable | Pre-Intervention a | Post-Intervention a | Group Differences |
|---|---|---|---|
| T1 (%ST) | 30.45 (6.31) | 27.78 (5.72) | p = 0.051, d = −0.47, 95% CI (−0.01 to 5.36) |
| F2 (%BW) | 99.27 (5.11) | 100.28 (4.03) | p = 0.27, d = 0.25, 95% CI (−2.85 to 0.84) |
| KFA (°) | 30.41 (9.21) | 33.54 (5.50) | p = 0.12, d = 0.34, 95% CI (−7.12 to 0.87) |
| KAM (Nm/kg) | 0.68 (0.35) | 0.50 (0.20) | p = 0.034 b, d = −0.90, 95% CI (0.02 to 0.35) |
| Gait Speed (m/s) | 0.92 (0.24) | 1.02 (0.17) | p = 0.006 b,c, d = 0.59, 95% CI (−0.17 to −0.03) |
| Age (Years) | N | Minimum (m/s) | Maximum (m/s) | Mean (m/s) |
|---|---|---|---|---|
| 40–49 | 2 | 0.1 | 0.25 | 0.18 |
| 50–59 | 6 | −0.08 | 0.15 | 0.05 |
| 60–69 | 6 | −0.02 | 0.53 | 0.19 |
| 70–79 | 3 | −0.04 | 0.06 | 0.02 |
| 80–89 | 1 | NA | NA | 0.04 |
| Variable | Correlation/ Significance | BMI | T1 Change | F2 Change | KFA Change | KAM Change | Gait Speed Change | KOOS Change |
|---|---|---|---|---|---|---|---|---|
| BMI | r | 1 | ||||||
| p | ||||||||
| T1 Change | r | 0.40 | 1 | |||||
| p | 0.10 | |||||||
| F2 Change | r | −0.041 | −0.40 | 1 | ||||
| p | 0.87 | 0.10 | ||||||
| KFA Change | r | −0.22 | 0.18 | 0.12 | 1 | |||
| p | 0.37 | 0.47 | 0.65 | |||||
| KAM Change | r | 0.18 | 0.30 | −0.042 | 0.31 | 1 | ||
| p | 0.46 | 0.23 | 0.87 | 0.21 | ||||
| Gait Speed Change | r | 0.055 | 0.31 | −0.45 | −0.09 | −0.091 | 1 | |
| p | 0.83 | 0.21 | 0.059 | 0.72 | 0.72 | |||
| KOOS Change | r | 0.60 a | 0.17 | −0.14 | −0.001 | 0.085 | 0.38 | 1 |
| p | 0.009 a | 0.50 | 0.58 | 0.10 | 0.74 | 0.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flowers, D.W.; Brewer, W.; Mitchell, K.; Ellison, J.; Frilot, C. The Effect of Core Stabilization Training on Improving Gait and Self-Perceived Function in Patients with Knee Osteoarthritis: A Single-Arm Clinical Trial. Pathophysiology 2022, 29, 495-506. https://doi.org/10.3390/pathophysiology29030040
Flowers DW, Brewer W, Mitchell K, Ellison J, Frilot C. The Effect of Core Stabilization Training on Improving Gait and Self-Perceived Function in Patients with Knee Osteoarthritis: A Single-Arm Clinical Trial. Pathophysiology. 2022; 29(3):495-506. https://doi.org/10.3390/pathophysiology29030040
Chicago/Turabian StyleFlowers, Daniel W., Wayne Brewer, Katy Mitchell, Jennifer Ellison, and Clifton Frilot. 2022. "The Effect of Core Stabilization Training on Improving Gait and Self-Perceived Function in Patients with Knee Osteoarthritis: A Single-Arm Clinical Trial" Pathophysiology 29, no. 3: 495-506. https://doi.org/10.3390/pathophysiology29030040