
Effects of Platelet-Rich Osteoconductive–Osteoinductive Allograft Compound on Tunnel Widening of ACL Reconstruction: A Randomized Blind Analysis Study


Abstract
:1. Introduction
2. Materials and Methods
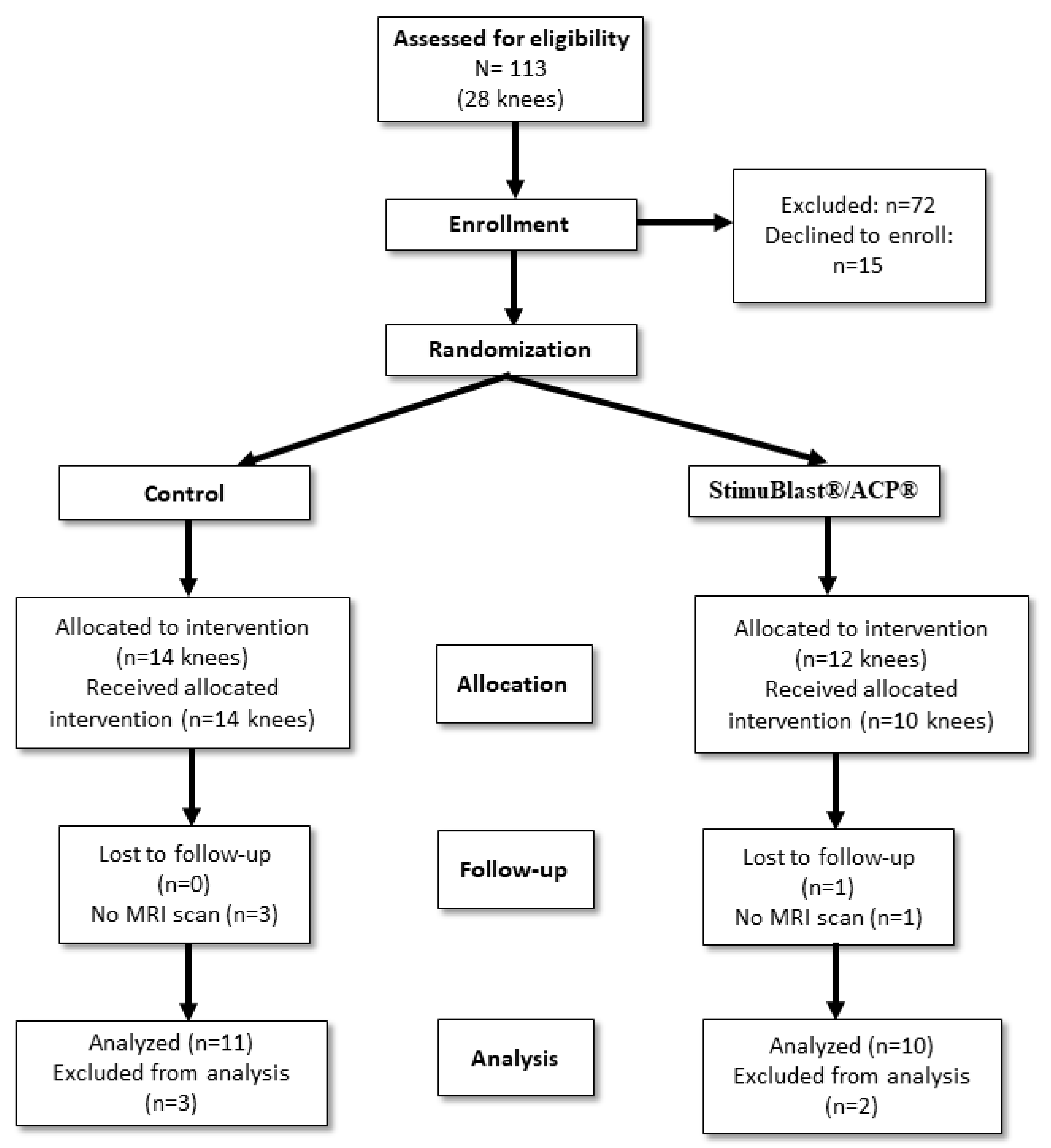
2.1. Patients Allocation
2.2. Inclusion and Exclusion Criteria
2.3. Surgical Procedures
2.4. MRI Scanning Protocol
2.5. Measurement of Tunnel Widening
2.6. Measurement of Graft Maturation
2.7. Tunnel Ganglion Cyst Formation
2.8. Statistical Analysis
3. Results
3.1. Tunnel Widening
3.2. Graft Maturation
3.3. Tunnel Ganglion Cyst Formation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anderson, K.; Seneviratne, A.M.; Izawa, K.; Atkinson, B.L.; Potter, H.G.; Rodeo, S.A. Augmentation of tendon healing in an intraarticular bone tunnel with use of a bone growth factor. Am. J. Sports Med. 2001, 26, 689–698. [Google Scholar] [CrossRef]
- Bach, B.R. Revision anterior cruciate ligament surgery. Arthroscopy 2003, 19, 14–29. [Google Scholar] [CrossRef] [PubMed]
- Buller, L.T.; Best, M.J.; Baraga, M.G.; Kaplan, L.D. Trends in anterior cruciate ligament reconstruction in the United States. Orthop. J. Sports Med. 2014, 3, 2325967114563664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.; Bosque, J.; Meehan, J.P.; Jamali, A.; Marder, R. Increase in outpatient knee arthroscopy in the United States: A comparison of National Surveys of Ambulatory Surgery, 1996 and 2006. J. Bone Jt. Surg. 2011, 93, 994–1000. [Google Scholar] [CrossRef]
- Lyman, S.; Koulouvais, P.; Sherman, S.; Do, H.; Mandl, L.A.; Marx, R.G. Epidemiology of Anterior Cruciate Ligament Reconstruction. J. Bone Jt. Surg. 2009, 91, 2321–2328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sudevan, P.J.; Chandrasekharan, J.; Sambandam, S.N.; Rohinikumar, G.J.; Annamalai, S.; Mounasamy, V. Arthroscopic ACL reconstruction using patellar bone tendon autograft and Rigidfix fixation—A midterm functional outcome. Muscles Ligaments Tendons J. 2017, 7, 247. [Google Scholar] [CrossRef] [PubMed]
- Kruse, L.M.; Gray, B.; Wright, R.W. Rehabilitation After Anterior Cruciate Ligament Reconstruction. A Systematic Review. J. Bone Jt. Surg. 2012, 94, 1737–1748. [Google Scholar] [CrossRef] [Green Version]
- Wiese-Bjornstal, D.M.; Smith, A.M.; Shaffer, S.M.; Morrey, M.A. An Integrated Model of Response to Sport Injury: Psychological and Sociological Dynamics. J. Appl. Sport Psychol. 1998, 10, 46–69. [Google Scholar] [CrossRef] [Green Version]
- Clatworthy, M.G.; Annear, P.; Bulow, J.U.; Bartlett, R.J. Tunnel widening in anterior cruciate ligament reconstruction: A prospective evaluation of hamstring and patella tendon grafts. Knee Surg. Sports Traumatol. Arthrosc. 1999, 7, 138–145. [Google Scholar] [CrossRef]
- Sauer, S.; Lind, M. Bone tunnel enlargement after ACL reconstruction with hamstring autograft is dependent on original bone tunnel diameter. Surg. J. 2017, 3, e96–e100. [Google Scholar] [CrossRef] [Green Version]
- Fules, P.J.; Madhav, R.T.; Goddard, R.K.; Newman-Sanders, A.; Mowbray, M.A. Evaluation of tibial bone tunnel enlargement using MRI scan cross-sectional area measurement after autologous hamstring tendon ACL replacement. Knee 2003, 10, 87–91. [Google Scholar] [CrossRef]
- Jansson, K.A.; Harilainen, A.; Sandelin, J.; Karjalainen, P.T.; Aronen, H.J.; Tallroth, K. Bone tunnel enlargement after anterior cruciate ligament reconstruction with the hamstring autograft and endobutton fixation technique A clinical, radiographic and magnetic resonance imaging study with 2 years follow-up. Knee Surg. Sports Traumatol. Arthrosc. 1999, 7, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Nebelung, W. Bone tunnel enlargement after anterior cruciate ligament reconstruction with semitendinosus tendon using Endobutton fixation on the femoral side. Arthroscopy 1998, 14, 810–815. [Google Scholar] [CrossRef]
- Segawa, H.; Omori, G.; Tomita, S.; Koga, Y. Bone tunnel enlargement after anterior cruciate ligament reconstruction using hamstring tendons. Knee Surg. Sports Traumatol. Arthrosc. 2001, 9, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Foldager, C.; Jakobsen, B.W.; Lund, B.; Christiansen, S.E.; Kashi, L.; Mikkelsen, L.R.; Lind, M. Tibial tunnel widening after bioresorbable poly-lactide calcium carbonate interference screw usage in ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 79–84. [Google Scholar] [CrossRef]
- Maak, T.G.; Voos, J.E.; Wickiewicz, T.L.; Warren, R.F. Tunnel widening in revision anterior cruciate ligament reconstruction. JAAOS-J. Am. Acad. Orthop. Surg. 2010, 18, 695–706. [Google Scholar] [CrossRef]
- Legeros, R.Z. Properties of Osteoconductive Biomaterials: Calcium Phosphates. Clin. Orthop. Relat. Res. 2002, 395, 81–98. [Google Scholar] [CrossRef]
- Yu, T.; Pan, H.; Hu, Y.; Tao, H.; Wang, K.; Zhang, C. Autologous platelet-rich plasma induces bone formation of tissue-engineered bone with bone marrow mesenchymal stem cells on beta-tricalcium phosphate ceramics. J. Orthop. Surg. Res. 2017, 12, 178. [Google Scholar] [CrossRef] [Green Version]
- Drews, B.H.; Merz, C.; Huth, J.; Gulkin, D.; Guelke, J.; Gebhard, F.; Mauch, F. Magnetic resonance imaging in evaluation of tunnel diameters prior to revision ACL reconstruction: A comparison to computed tomography. Skelet. Radiol. 2017, 46, 1361–1366. [Google Scholar] [CrossRef]
- Grassi, A.; Bailey, J.R.; Signorelli, C.; Carbone, G.; Wakam, A.T.; Lucidi, G.A.; Zaffagnini, S. Magnetic resonance imaging after anterior cruciate ligament reconstruction: A practical guide. World J. Orthop. 2016, 7, 638. [Google Scholar] [CrossRef]
- Ma, Y.; Murawski, C.D.; Rahnemai-Azar, A.A.; Maldjian, C.; Lynch, A.D.; Fu, F.H. Graft maturity of the reconstructed anterior cruciate ligament 6 months postoperatively: A magnetic resonance imaging evaluation of quadriceps tendon with bone block and hamstring tendon autografts. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Tashiro, Y.; Gale, T.; Sundaram, V.; Nagai, K.; Irrgang, J.J.; Anderst, W.; Nakashima, Y.; Tashman, S.; Fu, F.H. The graft bending angle can affect early graft healing after anterior cruciate ligament reconstruction: In vivo analysis with 2 years’ follow-up. Am. J. Sports Med. 2017, 45, 1829–1836. [Google Scholar] [CrossRef] [PubMed]
- Weiler, A.; Peters, G.; Mäurer, J.; Unterhauser, F.N.; Südkamp, N.P. Biomechanical properties and vascularity of an anterior cruciate ligament graft can be predicted by contrast-enhanced magnetic resonance imaging: A two-year study in sheep. Am. J. Sports Med. 2001, 29, 751–761. [Google Scholar] [CrossRef] [PubMed]
- Beasley, L.S.; Weiland, D.E.; Vidal, A.F.; Chhabra, A.; Herzka, A.S.; Feng, M.T.; West, R.V. Anterior cruciate ligament reconstruction: A literature review of the anatomy, biomechanics, surgical considerations, and clinical outcomes. Oper. Tech. Orthop. 2005, 15, 5–19. [Google Scholar] [CrossRef]
- Vaisha, R.; Agarwal, A.K.; Ingole, S.; Vijay, V. Current Trends in Anterior Cruciate Ligament Reconstruction: A Review. Cureus 2015, 7, e378. [Google Scholar] [CrossRef] [Green Version]
- Lavender, C.; Singh, V.; Berdis, G.; Fravel, W.; Lamba, C.; Patel, T. Anterior Cruciate Ligament (ACL) Reconstruction Augmented with Bone Marrow Concentrate, Demineralized Bone Matrix, Autograft Bone, and a Suture Tape (The Fertilized ACL). Arthrosc. Sports Med. Rehabil. 2021, 3, e1719–e1722. [Google Scholar] [CrossRef]
- Sundman, E.A.; Cole, B.J.; Fortier, L.A. Growth factor and catabolic cytokine concentrations are influenced by the cellular composition of platelet-rich plasma. Am. J. Sports Med. 2011, 39, 2135–2140. [Google Scholar] [CrossRef]
- El-Hage, Z.M.; Mohammed, A.; Griffiths, D.; Richardson, J.B. Tibial plateau fracture following allograft anterior cruciate ligament (ACL) reconstruction. Injury 1998, 29, 73–74. [Google Scholar] [CrossRef]
- Mithöfer, K.; Gill, T.J.; Vrahas, M.S. Tibial plateau fracture following anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2004, 12, 325–328. [Google Scholar] [CrossRef]
- Sundaram, R.O.; Cohen, D.; Barton-Hanson, N. Tibial plateau fracture following gracilis-semitendinosus anterior cruciate ligament reconstruction: The tibial tunnel stress-riser. Knee 2006, 13, 238–240. [Google Scholar] [CrossRef] [PubMed]
- Rabuck, S.J.; Baraga, M.; Fu, F.H. Anterior Cruciate Ligament Healing and Advances in Imaging. Clin. Sports Med. 2013, 32, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Ghazikhanian, V.; Beltran, J.; Nikac, V.; Feldman, M.; Bencardino, J.T. Tibial tunnel and pretibial cysts following ACL graft reconstruction: MR imaging diagnosis. Skelet. Radiol. 2012, 41, 1375–1379. [Google Scholar] [CrossRef] [PubMed]
- Joshi, Y.V.; Bhaskar, D.; Phaltankar, P.M.; Charalambous, C.P. Tibial Tunnel Cyst Formation after Anterior Cruciate Ligament Reconstruction Using a Non-Bioabsorbable Interference Screw. Knee Surg. Relat. Res. 2015, 27, 269. [Google Scholar] [CrossRef]
- Zysk, S.P.; Fraunberger, P.; Veihelmann, A.; Dörger, M.; Kalteis, T.; Maier, M.; Pellengahr, C.; Refior, H.J. Tunnel enlargement and changes in synovial fluid cytokine profile following anterior cruciate ligament reconstruction with patellar tendon and hamstring tendon autografts. Knee Surg. Sports Traumatol. Arthrosc. 2004, 12, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Hexter, A.T.; Pendegrass, C.; Haddad, F.; Blunn, G. Demineralized bone matrix to augment tendon-bone healing: A systematic review. Orthop. J. Sports Med. 2017, 5, 2325967117734517. [Google Scholar] [CrossRef] [PubMed]
- Porter, M.D.; Shadbolt, B. Femoral aperture fixation improves anterior cruciate ligament graft function when added to cortical suspensory fixation: An in vivo computer navigation study. Orthop. J. Sports Med. 2016, 4, 2325967116665795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muramatsu, K.; Hachiya, Y.; Izawa, H. Serial evaluation of human anterior cruciate ligament grafts by contrast-enhanced magnetic resonance imaging: Comparison of allografts and autografts. J. Arthrosc. Relat. Surg. 2008, 24, 1038–1044. [Google Scholar] [CrossRef]
- Hexter, A.T.; Karali, A.; Kao, A.; Tozzi, G.; Heidari, N.; Petrie, A.; Boyd, A.; Kalaskar, D.M.; Pendegrass, C.; Rodeo, S.; et al. Effect of Demineralized Bone Matrix, Bone Marrow Mesenchymal Stromal Cells, and Platelet-Rich Plasma on Bone Tunnel Healing After Anterior Cruciate Ligament Reconstruction: A Comparative Micro-Computed Tomography Study in a Tendon Allograft Sheep Model. Orthop. J. Sports Med. 2021, 9, 23259671211034166. [Google Scholar] [CrossRef]
- Weimin, P.; Dan, L.; Yiyong, W.; Yunyu, H.; Li, Z. Tendon-to-bone healing using an injectable calcium phosphate cement combined with bone xenograft/BMP composite. Biomaterials 2013, 34, 9926–9936. [Google Scholar] [CrossRef]
- Huangfu, X.; Zhao, J. Tendon-bone healing enhancement using injectable tricalcium phosphate in a dog anterior cruciate ligament reconstruction model. Arthrosc. J. Arthrosc. Relat. Surg. 2007, 23, 455–462. [Google Scholar] [CrossRef]
- Kuang, G.M.; Yau, W.P.; Lu, W.W.; Chiu, K.Y. Local application of strontium in a calcium phosphate cement system accelerates healing of soft tissue tendon grafts in anterior cruciate ligament reconstruction: Experiment using a rabbit model. Am. J. Sports Med. 2014, 42, 2996–3002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, C.Y.; Qin, L.; Lee, K.M.; Chan, K.M. The use of brushite calcium phosphate cement for enhancement of bone-tendon integration in an anterior cruciate ligament reconstruction rabbit model. J. Biomed. Mater. Res. Part B Appl. Biomater. 2009, 89, 466–474. [Google Scholar] [CrossRef]
- Mutsuzaki, H.; Sakane, M. Calcium phosphate-hybridized tendon graft to enhance tendon-bone healing two years after ACL reconstruction in goats. Sports Med. Arthrosc. Rehabil. Ther. Technol. 2011, 3, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, C.B.; Kawamura, S.; Deng, X.H.; Ying, L.; Schneidkraut, J.; Hays, P.; Rodeo, S.A. Bone morphogenetic proteins-signaling plays a role in tendon-to-bone healing: A study of rhBMP-2 and noggin. Am. J. Sports Med. 2007, 35, 597–604. [Google Scholar] [CrossRef]
- Mutsuzaki, H.; Kanamori, A.; Ikeda, K.; Hioki, S.; Kinugasa, T.; Sakane, M. Effect of calcium phosphate–hybridized tendon graft in anterior cruciate ligament reconstruction: A randomized controlled trial. Am. J. Sports Med. 2012, 40, 1772–1780. [Google Scholar] [CrossRef] [PubMed]
- Pan, W.; Wei, Y.; Zhou, L.; Li, D. Comparative in vivo study of injectable biomaterials combined with BMP for enhancing tendon graft osteointegration for anterior cruciate ligament reconstruction. J. Orthop. Res. 2011, 29, 1015–1021. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OIC (StimuBlast®/PRP) | Control | |
|---|---|---|
| Male | 8 | 7 |
| Female | 5 | 7 |
| Age at Time of Surgery | 32.7 ± 10.5 | 32.7 ± 12.7 y.o. |
| Age Range | 16 to 50 y.o. | 15 to 55 y.o. |
| TR/TE/TI (ms) | ETL | Matrix Size | FOV (mm) | Slice Thickness (mm) | |
|---|---|---|---|---|---|
| FSE Sagittal PD | 3200/30 | 10 | 512 × 256 | 140 | 4 |
| FSE Sagittal STIR | 4000/36/130 | 10 | 256 × 192 | 160 | 4 |
| FSE Sagittal (meniscus) | 1500/19 | 10 | 256 × 224 | 140 | 3 |
| FSE Coronal PD | 3200/30 | 10 | 512 × 256 | 120 | 4 |
| FSE Coronal STIR | 4000/36/130 | 10 | 256 × 192 | 140 | 4 |
| FSE Axial PD | 3200/30 | 10 | 512 × 256 | 140 | 4 |
| FSE Axial PD (Additional- perpendicular to graft tunnels) | 3000/34–40 | 10 | 256 × 224 | 140 | 3 |
| OIC (StimuBlast®/ACP®) | Control | |
|---|---|---|
| Minimal Expansion (<1 mm) | 5 | 0 |
| Mild Expansion (<5 mm) | 6 | 11 |
| Moderate Expansion (5–10 mm) | 0 | 1 |
| Large Expansion (10+ mm) | 0 | 0 |
| OIC (StimuBlast®ACP®) | Control | |
|---|---|---|
| Minimal Expansion (<1 mm) | 4 | 0 |
| Mild Expansion (<5 mm) | 8 | 9 |
| Moderate Expansion (5–10 mm) | 0 | 2 |
| Large Expansion (10+ mm) | 0 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solomon, R.; Hommen, J.P.; Travascio, F. Effects of Platelet-Rich Osteoconductive–Osteoinductive Allograft Compound on Tunnel Widening of ACL Reconstruction: A Randomized Blind Analysis Study. Pathophysiology 2022, 29, 394-404. https://doi.org/10.3390/pathophysiology29030031
Solomon R, Hommen JP, Travascio F. Effects of Platelet-Rich Osteoconductive–Osteoinductive Allograft Compound on Tunnel Widening of ACL Reconstruction: A Randomized Blind Analysis Study. Pathophysiology. 2022; 29(3):394-404. https://doi.org/10.3390/pathophysiology29030031
Chicago/Turabian StyleSolomon, Ruth, Jan Pieter Hommen, and Francesco Travascio. 2022. "Effects of Platelet-Rich Osteoconductive–Osteoinductive Allograft Compound on Tunnel Widening of ACL Reconstruction: A Randomized Blind Analysis Study" Pathophysiology 29, no. 3: 394-404. https://doi.org/10.3390/pathophysiology29030031