Prognosis after Local Recurrence in Patients with Early-Stage Breast Cancer Treated without Chemotherapy


Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gradishar, W.J.; Anderson, B.O.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Blair, S.L.; Burstein, H.J.; Dang, C.; Elias, A.D.; et al. Breast Cancer, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2020, 18, 452–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallerstedt, S.M.; Nilsson Ek, A.; Olofsson Bagge, R.; Kovács, A.; Strandell, A.; Linderholm, B. Personalised medicine and the decision to withhold chemotherapy in early breast cancer with intermediate risk of recurrence-a systematic review and meta-analysis. Eur. J. Clin. Pharmacol. 2020, 76, 1199–1211. [Google Scholar] [CrossRef] [PubMed]
- Geurts, Y.M.; Witteveen, A.; Bretveld, R.; Poortmans, P.M.; Sonke, G.S.; Strobbe, L.J.A.; Siesling, S. Patterns and predictors of first and subsequent recurrence in early breast cancer. Breast Cancer Res. Treat. 2017, 165, 709–720. [Google Scholar] [CrossRef] [PubMed]
- Chia, S.K.; Speers, C.H.; Bryce, C.J.; Hayes, M.M.; Olivotto, I.A. Ten-year outcomes in a population-based cohort of node-negative, lymphatic, and vascular invasion-negative early breast cancers without adjuvant systemic therapies. J. Clin. Oncol. 2004, 22, 1630–1637. [Google Scholar] [CrossRef]
- Jaraj, D.; Höijer, J.; Widman, L.; Ahlgren, J.; Arnesson, L.G.; Einbeigi, Z.; Klintman, M.; Vikhe Patil, E.; Sund, M.; Fredriksson, I.; et al. Long-Term Prognostication for 20 114 Women with Small and Node-Negative Breast Cancer (T1abN0). JNCI. Cancer Spectr. 2020, 5, pkaa084. [Google Scholar] [CrossRef]
- Hassett, M.J.; Hughes, M.E.; Niland, J.C.; Edge, S.B.; Theriault, R.L.; Wong, Y.N.; Wilson, J.; Carter, W.B.; Blayney, D.W.; Weeks, J.C. Chemotherapy use for hormone receptor-positive, lymph node-negative breast cancer. J. Clin. Oncol. 2008, 26, 5553–5560. [Google Scholar] [CrossRef] [Green Version]
- Mariotto, A.; Feuer, E.J.; Harlan, L.C.; Wun, L.M.; Johnson, K.A.; Abrams, J. Trends in use of adjuvant multi-agent chemotherapy and tamoxifen for breast cancer in the United States: 1975–1999. J. Natl. Cancer Inst. 2002, 94, 1626–1634. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: An overview of the randomised trials. Lancet 2005, 365, 1687–1717. [Google Scholar] [CrossRef]
- Narod, S.A.; Iqbal, J.; Miller, A. Why have breast cancer mortality rates declined? J. Cancer Policy 2015, 5, 8–17. [Google Scholar] [CrossRef] [Green Version]
- Sopik, V.; Nofech-Mozes, S.; Sun, P.; Narod, S.A. The relationship between local recurrence and death in early-stage breast cancer. Breast Cancer Res. Treat. 2016, 155, 175–185. [Google Scholar] [CrossRef]
- Anderson, S.J.; Wapnir, I.; Dignam, J.J.; Fisher, B.; Mamounas, E.P.; Jeong, J.H.; Geyer, C.E., Jr.; Wickerham, D.L.; Costantino, J.P.; Wolmark, N. Prognosis after ipsilateral breast tumor recurrence and locoregional recurrences in patients treated by breast-conserving therapy in five National Surgical Adjuvant Breast and Bowel Project protocols of node-negative breast cancer. J. Clin Oncol. 2009, 27, 2466–2473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wapnir, I.L.; Anderson, S.J.; Mamounas, E.P.; Geyer, C.E., Jr.; Jeong, J.H.; Tan-Chiu, E.; Fisher, B.; Wolmark, N. Prognosis after ipsilateral breast tumor recurrence and locoregional recurrences in five National Surgical Adjuvant Breast and Bowel Project node-positive adjuvant breast cancer trials. J. Clin. Oncol. 2006, 24, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- Wapnir, I.L.; Khan, A. Current Strategies for the Management of Locoregional Breast Cancer Recurrence. Oncology 2019, 33, 19–25. [Google Scholar]
- Wapnir, I.L.; Price, K.N.; Anderson, S.J.; Robidoux, A.; Martín, M.; Nortier, J.W.; Paterson, A.H.; Rimawi, M.F.; Láng, I.; Baena-Cañada, J.M.; et al. Efficacy of chemotherapy for ER-negative and ER-positive isolated locoregional recurrence of breast cancer: Final analysis of the CALOR trial. J. Clin. Oncol. 2018, 36, 1073–1079. [Google Scholar] [CrossRef] [PubMed]
- Waeber, M.; Castiglione-Gertsch, M.; Dietrich, D.; Thürlimann, B.; Goldhirsch, A.; Brunner, K.W.; Borner, M.M. Adjuvant therapy after excision and radiation of isolated postmastectomy locoregional breast cancer recurrence: Definitive results of a phase III randomized trial (SAKK 23/82) comparing tamoxifen with observation. Ann. Oncol. 2003, 14, 1215–1221. [Google Scholar] [CrossRef]
- Baek, S.Y.; Kim, J.; Chung, I.Y.; Ko, B.S.; Kim, H.J.; Lee, J.W.; Son, B.H.; Ahn, S.H.; Lee, S.B. Clinical Course and Predictors of Subsequent Recurrence and Survival of Patients with Ipsilateral Breast Tumor Recurrence. Cancer Control. 2022, 29, 10732748221089412. [Google Scholar] [CrossRef]
- Panet-Raymond, V.; Truong, P.T.; Alexander, C.; Lesperance, M.; McDonald, R.E.; Watson, P.H. Clinicopathologic factors of the recurrent tumor predict outcome in patients with ipsilateral breast tumor recurrence. Cancer 2011, 117, 2035–2043. [Google Scholar]
- Fredriksson, I.; Liljegren, G.; Arnesson, L.G.; Emdin, S.O.; Palm-Sjövall, M.; Fornander, T.; Holmqvist, M.; Holmberg, L.; Frisell, J. Local recurrence in the breast after conservative surgery—A study of prognosis and prognostic factors in 391 women. Eur. J. Cancer 2002, 38, 1860–1870. [Google Scholar] [CrossRef]
- Dent, R.; Valentini, A.; Hanna, W.; Rawlinson, E.; Rakovitch, E.; Sun, P.; Narod, S.A. Factors associated with breast cancer mortality after local recurrence. Curr. Oncol. 2014, 21, 418–425. [Google Scholar] [CrossRef] [Green Version]
- Galper, S.; Blood, E.; Gelman, R.; Abner, A.; Recht, A.; Kohli, A.; Wong, J.S.; Smith, D.; Bellon, J.; Connolly, J.; et al. Prognosis after local recurrence after conservative surgery and radiation for early-stage breast cancer. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 348–357. [Google Scholar]
- Voogd, A.C.; Van Oost, F.J.; Rutgers, E.J.T.; Elkhuizen, P.H.M.; Van Geel, A.N.; Scheijmans, L.J.E.E.; Van Der Sangen, M.J.C.; Botke, G.; Hoekstra, C.J.; Jobsen, J.J.; et al. Long-term prognosis of patients with local recurrence after conservative surgery and radiotherapy for early breast cancer. Eur. J. Cancer 2005, 41, 2637–2644. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Tong, Y.; Chen, X.; Shen, K. Prognostic Factors and Surgery for Breast Cancer Patients with Locoregional Recurrence: An Analysis of 5202 Consecutive Patients. Front. Oncol. 2021, 11, 763119. [Google Scholar] [CrossRef] [PubMed]
- Shenouda, M.N.; Sadek, B.T.; Goldberg, S.I.; Keruakous, A.R.; Croft, B.J.; Abi Raad, R.F.; Taghian, A.G. Clinical outcome of isolated locoregional recurrence in patients with breast cancer according to their primary local treatment. Clin. Breast Cancer 2014, 14, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, H.M.; Overgaard, M.; Grau, C.; Jensen, A.R.; Overgaard, J. Loco-regional recurrence after mastectomy in high-risk breast cancer-risk and prognosis. An analysis of patients from the DBCG 82 b&c randomization trials. Radiother Oncol. 2006, 79, 147–155. [Google Scholar] [PubMed]
- Haffty, B.G.; Hauser, A.; Ho Choi, D.; Parisot, N.; Rimm, D.; King, B.; Carter, D. Molecular markers for prognosis after isolated postmastectomy chest wall recurrence. Cancer 2004, 100, 252–263. [Google Scholar] [CrossRef]
- Van Tienhoven, G.; Voogd, A.C.; Peterse, J.L.; Nielsen, M.; Andersen, K.W.; Mignolet, F.; Sylvester, R.; Fentiman, I.V.; Van der Schueren, E.; Van Zijl, K.; et al. Prognosis after treatment for loco-regional recurrence after mastectomy or breast conserving therapy in two randomised trials (EORTC 10801 and DBCG-82TM). Eur. J. Cancer 1999, 35, 32–38. [Google Scholar] [CrossRef]
- Fisher, B.; Anderson, S.; Bryant, J.; Margolese, R.G.; Deutsch, M.; Fisher, E.R.; Jeong, J.H.; Wolmark, N. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N. Engl. J. Med. 2002, 347, 1233–1241. [Google Scholar] [CrossRef] [Green Version]
- Fisher, B.; Anderson, S.; Fisher, E.R.; Redmond, C.; Wickerham, D.L.; Wolmark, N.; Mamounas, E.P.; Deutsch, M.; Margolese, R. Significance of ipsilateral breast tumour recurrence after lumpectomy. Lancet 1991, 338, 327–331. [Google Scholar] [CrossRef]
- Gabriel, L.; Schmidt, M.; Juhasz-Böss, S.; Melchior, P.; von Heesen, A.; Schmidt, G.; Kranzhöfer, N.; Solomayer, E.F.; Juhasz-Böss, I.; Breitbach, G.P. Therapy of isolated locoregional recurrent carcinoma of the breast. Arch. Gynecol. Obstet. 2019, 300, 365–376. [Google Scholar] [CrossRef]
- Wu, H.L.; Lu, Y.J.; Li, J.W.; Wu, S.Y.; Chen, X.S.; Liu, G.Y. Prior Local or Systemic Treatment: A Predictive Model Could Guide Clinical Decision-Making for Locoregional Recurrent Breast Cancer. Front. Oncol. 2022, 11, 791995. [Google Scholar] [CrossRef]
- Lee, K.; Sim, S.H.; Kang, E.J.; Seo, J.H.; Chae, H.; Lee, K.S.; Kim, J.Y.; Ahn, J.S.; Im, Y.H.; Park, S.; et al. The Role of Chemotherapy in Patients with HER2-Negative Isolated Locoregional Recurrence of Breast Cancer: A Multicenter Retrospective Cohort Study. Front. Oncol. 2021, 11, 653243. [Google Scholar] [CrossRef]
- Roberson, M.L.; Nichols, H.B.; Olshan, A.F.; Troester, M.; Robinson, W.R. Premenopausal gynecologic surgery and survival among black and white women with breast cancer. Cancer Causes Control. 2020, 31, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Nichols, H.B.; Trentham-Dietz, A.; Newcomb, P.A.; Egan, K.M.; Titus, L.J.; Hampton, J.M.; Visvanathan, K. Pre-diagnosis oophorectomy, estrogen therapy and mortality in a cohort of women diagnosed with breast cancer. Breast Cancer Res. 2013, 15, R99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obermair, A.; Youlden, D.R.; Baade, P.D.; Janda, M. The impact of risk-reducing hysterectomy and bilateral salpingo-oophorectomy on survival in patients with a history of breast cancer—A population-based data linkage study. Int. J. Cancer 2014, 134, 2211–2222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Maaren, M.C.; de Munck, L.; de Bock, G.H.; Jobsen, J.J.; van Dalen, T.; Linn, S.C.; Poortmans, P.; Strobbe, L.J.; Siesling, S. 10 year survival after breast-conserving surgery plus radiotherapy compared with mastectomy in early breast cancer in the Netherlands: A population-based study. Lancet Oncol. 2016, 17, 1158–1170. [Google Scholar] [CrossRef]
- Wrubel, E.; Natwick, R.; Wright, G.P. Breast-Conserving Therapy is Associated with Improved Survival Compared with Mastectomy for Early-Stage Breast Cancer: A Propensity Score Matched Comparison Using the National Cancer Database. Ann. Surg. Oncol. 2021, 28, 914–919. [Google Scholar] [CrossRef]
- Almahariq, M.F.; Quinn, T.J.; Siddiqui, Z.; Jawad, M.S.; Chen, P.Y.; Gustafson, G.S.; Dilworth, J.T. Breast conserving therapy is associated with improved overall survival compared to mastectomy in early-stage, lymph node-negative breast cancer. Radiother. Oncol. 2020, 142, 186–194. [Google Scholar] [CrossRef]
- Ji, J.; Yuan, S.; He, J.; Liu, H.; Yang, L.; He, X. Breast-conserving therapy is associated with better survival than mastectomy in Early-stage breast cancer: A propensity score analysis. Cancer Med. 2022, 11, 646–1658. [Google Scholar] [CrossRef]
- Amabile, M.I.; Frusone, F.; De Luca, A.; Tripodi, D.; Imbimbo, G.; Lai, S.; D’Andrea, V.; Sorrenti, S.; Molfino, A. Locoregional Surgery in Metastatic Breast Cancer: Do Concomitant Metabolic Aspects Have a Role on the Management and Prognosis in this Setting? J. Pers. Med. 2020, 10, 227. [Google Scholar] [CrossRef]
- Khan, S.A.; Stewart, A.K.; Morrow, M. Does aggressive local therapy improve survival in metastatic breast cancer? Surgery 2002, 132, 620–627. [Google Scholar] [CrossRef]
- Baldini, E.; Lauro, A.; Tripodi, D.; Pironi, D.; Amabile, M.I.; Ferent, I.C.; Lori, E.; Gagliardi, F.; Bellini, M.I.; Forte, F.; et al. Thyroid Diseases and Breast Cancer. J. Pers. Med. 2022, 12, 156. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Number of Patients (N = 135) |
|---|---|
| Year of birth | |
| Mean (range) | 1938.8 (1911–1966) |
| Year of diagnosis | |
| Mean (range) | 1992 (1987–2000) |
| Age at diagnosis (years) | |
| Mean (range) | 53.5 (27.3–77.3) |
| <40 | 13 (9.6%) |
| 40–49 | 46 (34.8%) |
| 50–59 | 34 (25.2%) |
| 60+ | 42 (31.1%) |
| Tumour size (cm) | |
| Mean (range) | 15.0 (0–46) |
| 0–2 | 106 (79.8%) |
| 2–5 | 29 (20.3%) |
| Tumour grade | |
| I | 26 (24.3%) |
| II | 48 (44.9%) |
| III | 33 (30.8%) |
| Missing | 28 |
| ER status | |
| Negative | 43 (35.3%) |
| Positive | 79 (64.8%) |
| Missing | 13 |
| PR status | |
| Negative | 46 (38.7%) |
| Positive | 73 (61.3%) |
| Missing | 16 |
| HER2 status | |
| Negative | 48 (84.2%) |
| Positive | 9 (15.8%) |
| Missing | 78 |
| LVI | |
| No | 92 (79.7%) |
| Yes | 24 (20.3%) |
| Missing | 17 |
| Surgery | |
| Lumpectomy | 130 (96.3%) |
| Mastectomy | 5 (3.7%) |
| Oophorectomy before diagnosis | |
| No | 117 (91.4%) |
| Yes | 11 (8.4%) |
| Missing | 7 |
| Radiotherapy | |
| No | 50 (37.3%) |
| Yes | 84 (62.7%) |
| Missing | 1 |
| Tamoxifen | |
| No | 84 (62.2%) |
| Yes | 51 (37.8%) |
| Missing | 0 |
| Vital status | |
| Dead due to breast cancer | 38 (28.8%) |
| Dead due to other cause/missing | 37 (28.0%) |
| Alive | 57 (43.2%) |
| Missing | 3 |
| Time from diagnosis to local recurrence (years) | |
| Mean (range) | 7.8 (0.3–22.6) |
| 0–1.99 | 19 (14.1%) |
| 2–4.99 | 45 (33.3%) |
| 5+ | 71 (62.2%) |
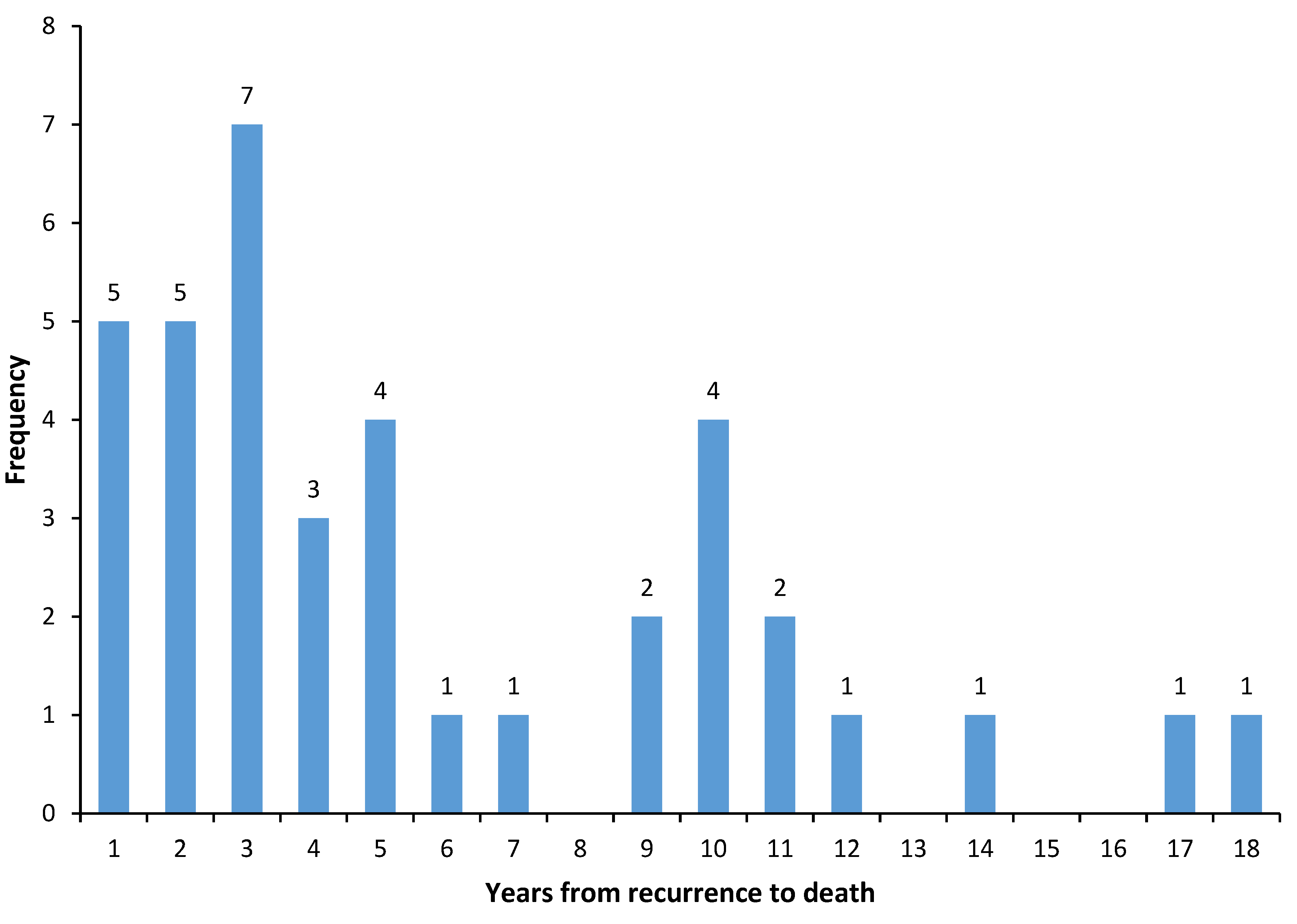
| Time from local recurrence to breast cancer death | |
| Mean (range) | 5.3 (0.3–17) |
| Variable | Univariate HR (95% CI) P | Multivariate HR (95% CI) P |
|---|---|---|
| Age at diagnosis (years) | ||
| <40 | 1 | 1 |
| 40–49 | 0.40 (0.16–1.04) 0.06 | 0.47 (0.18–1.23) 0.12 |
| 50–59 | 0.55 (0.21–1.44) 0.22 | 0.48 (0.18–1.30) 0.15 |
| 60+ | 0.35 (0.13–0.93) 0.03 | 0.23 (0.08–0.66) 0.006 |
| Tumour size | ||
| 0–2 cm | 1 | 1 |
| 2–5 cm | 2.53 (1.18–4.64) 0.02 | 1.79 (0.84–3.82) 0.13 |
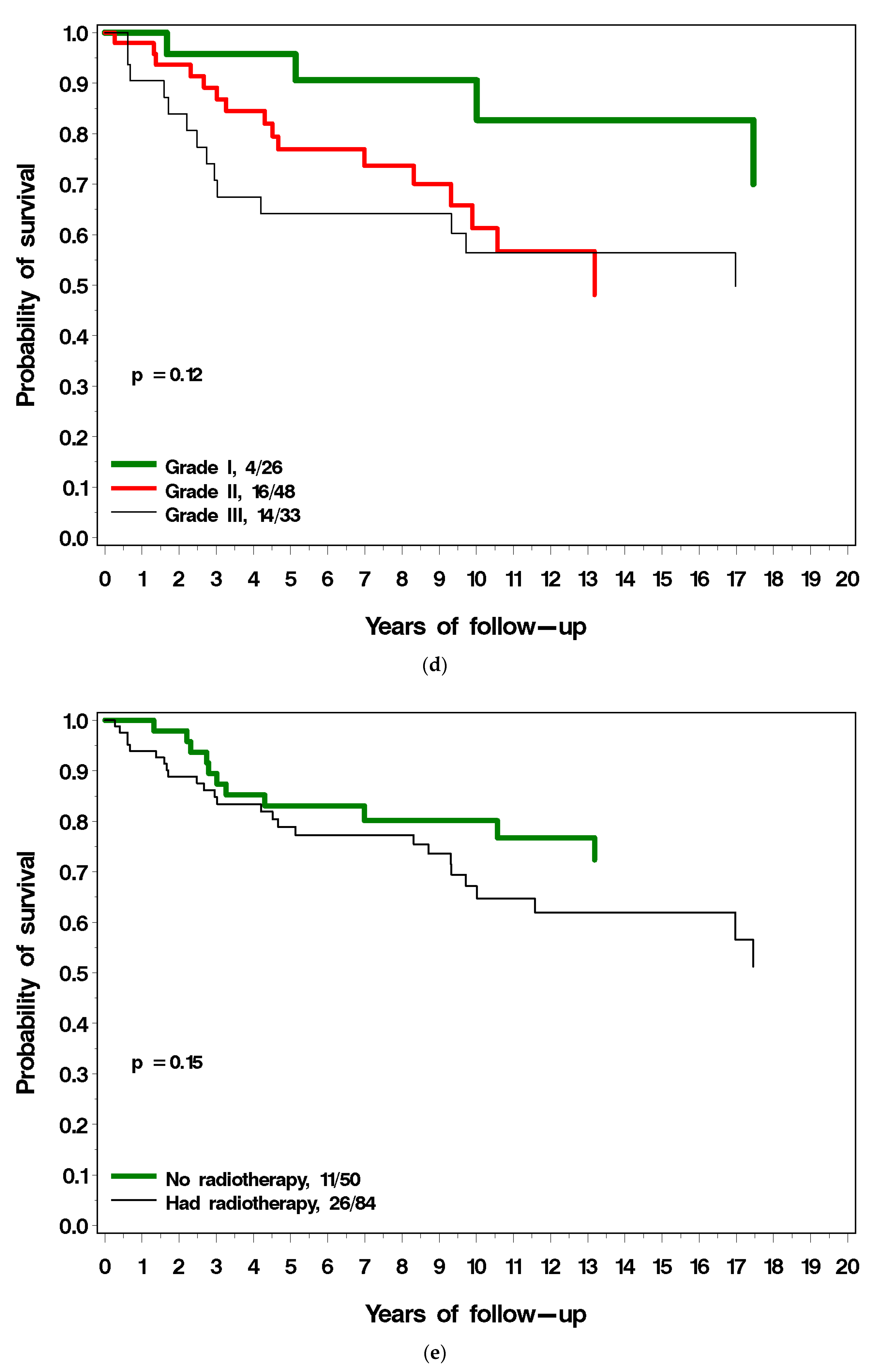
| Grade | ||
| 1 | 1 | |
| 2 | 2.42 (0.87–7.86) 0.09 | |
| 3 | 3.05 (1.00–9.27) 0.05 | Not used |
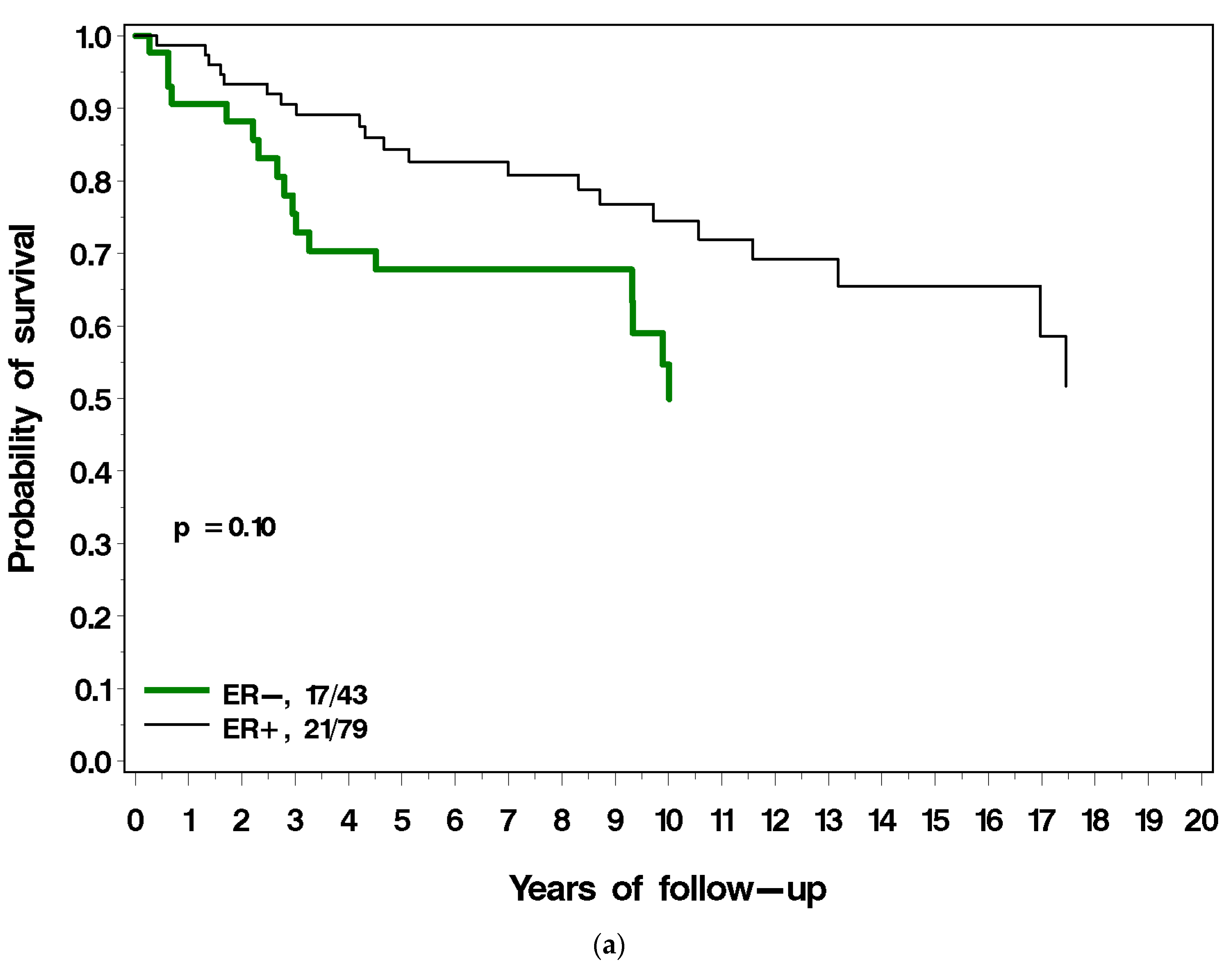
| ER status | ||
| Negative | 1 | 1 |
| Positive | 0.59 (0.31–1.12) 0.10 | 0.81 (0.37–1.79) 0.61 |
| PR status | ||
| Negative | 1 | 1 |
| Positive | 0.33 (0.17–0.64) 0.001 | 0.34 (0.16–0.73) 0.006 |
| LVI | ||
| No | 1 | 1 |
| Yes | 1.86 (0.92–3.79) 0.08 | Not used |
| Oophorectomy | ||
| No | 1 | |
| Yes | 0.47 (0.11–1.94) 0.29 | Not used |
| HER2 status | ||
| Negative | 1 | |
| Positive | 1.19 (0.40–3.53) 0.75 | Not used |
| Radiation at diagnosis | ||
| No | 1 | 1 |
| Yes | 1.70 (0.84–3.44) 0.14 | 1.86 (0.80–4.35) 0.15 |
| Tamoxifen | ||
| No | 1 | 1 |
| Yes | 1.43 (0.74–2.74) 0.29 | 1.06 (0.52–2.19) 0.87 |
| Time diagnosis to local recurrence | ||
| 0–1.99 years | 1 | 1 |
| 2 and + | 0.46 (0.22–0.94) 0.04 | 0.38 (0.17–0.85) 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sopik, V.; Lim, D.; Sun, P.; Narod, S.A. Prognosis after Local Recurrence in Patients with Early-Stage Breast Cancer Treated without Chemotherapy. Curr. Oncol. 2023, 30, 3829-3844. https://doi.org/10.3390/curroncol30040290
Sopik V, Lim D, Sun P, Narod SA. Prognosis after Local Recurrence in Patients with Early-Stage Breast Cancer Treated without Chemotherapy. Current Oncology. 2023; 30(4):3829-3844. https://doi.org/10.3390/curroncol30040290
Chicago/Turabian StyleSopik, Victoria, David Lim, Ping Sun, and Steven A. Narod. 2023. "Prognosis after Local Recurrence in Patients with Early-Stage Breast Cancer Treated without Chemotherapy" Current Oncology 30, no. 4: 3829-3844. https://doi.org/10.3390/curroncol30040290