Follow-Up Imaging Guidelines for Patients with Stage III Unresectable NSCLC: Recommendations Based on the PACIFIC Trial

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
- (1)
- What timepoint should be used as a reference for initiation of imaging?
- (2)
- What is the recommended frequency of imaging?
- (3)
- What type of imaging should be used and which body regions should be assessed?
- (4)
- Who should follow the patient?
- (5)
- What other assessments or activities should be conducted?
3. Results and Discussion
3.1. Summary of Recommendations
3.2. Detailed Recommendations
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics: A 2020 Special Report on Lung Cancer. Available online: Cancer.ca/Canadian-Cancer-Statistics-2020-EN (accessed on 11 January 2022).
- Seung, S.J.; Hurry, M.; Walton, R.N.; Evans, W.K. Retrospective cohort study of unresectable stage III non-small-cell lung cancer in Canada. Curr. Oncol. 2020, 27, e354–e360. [Google Scholar] [CrossRef] [PubMed]
- Ganti, A.K.; Klein, A.B.; Cotarla, I.; Seal, B.; Chou, E. Update of incidence, prevalence, survival, and initial treatment in patients with non–small cell lung cancer in the US. JAMA Oncol. 2021, 7, 1824–1832. [Google Scholar] [CrossRef] [PubMed]
- Robinson, A.; Vella, E.T.; Ellis, P.M.; Goffin, R.; Hanna, W.; Maziak, D.; Swaminath, A.; Ung, Y.C.; the Lung Cancer Disease Site Group. Ontario Health. Cancer Care Ontario. Recommendations for the Treatment of Patients with Clinical Stage III Non-Small Cell Lung Cancer: Endorsement of the 2019 National Institute for Health and Care Excellence Guidance and the 2018 Society for Immunotherapy of Cancer Guidance. 27 April 2020. Available online: https://www.cancercareontario.ca/en/file/54406/download?token=oMLjCMXY (accessed on 11 January 2022).
- Provincial Health Services Authority. BC Cancer. Treatment of Locally Advanced Non-Small Cell Lung Cancer. Available online: http://www.bccancer.bc.ca/books/lung/management/non-small-cell-lung-cancer-nsclc/combined-modality-therapy-for-unresectable-stage-iii (accessed on 11 January 2022).
- Brade, A.; Jao, K.; Yu, S.; Cheema, P.; Doucette, S.; Christofides, A.; Schellenberg, D. A Canadian perspective on the challenges for delivery of curative-intent therapy in stage III unresectable non-small cell lung cancer. Curr. Oncol. 2021, 28, 1618–1629. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology: Non-Small Cell Lung Cancer. Version 1.2022. Available online: https://www.nccn.org (accessed on 11 January 2022).
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M.; Senan, S.; Waller, D.A.; Vansteenkiste, J.; Escriu, C.; Peters, S.; on behalf of the ESMO Guidelines Committee. ESMO Early and Locally Advanced Non-Small-Cell Lung Cancer (NSCLC) Guideline. Available online: http://interactiveguidelines.esmo.org/esmo-web-app/gl_toc/index.php?GL_id=46 (accessed on 11 January 2022).
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after chemoradiotherapy in stage III non–small-cell lung cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AstraZeneca. Product Monograph: IMFINZI(R) (Durvalumab for Injection). Date of Revision: 21 September 2021. Available online: https://www.astrazeneca.ca/content/dam/az-ca/downloads/productinformation/imfinzi-product-monograph-en.pdf (accessed on 14 January 2022).
- Daly, M.E.; Singh, N.; Ismaila, N.; Antonoff, M.B.; Arenberg, D.A.; Bradley, J.; David, E.; Detterbeck, F.; Früh, M.; Gubens, M.A.; et al. Management of stage III non-small-cell lung cancer: ASCO guideline. J. Clin. Oncol. 2022, 40, 1356–1384. [Google Scholar] [CrossRef] [PubMed]
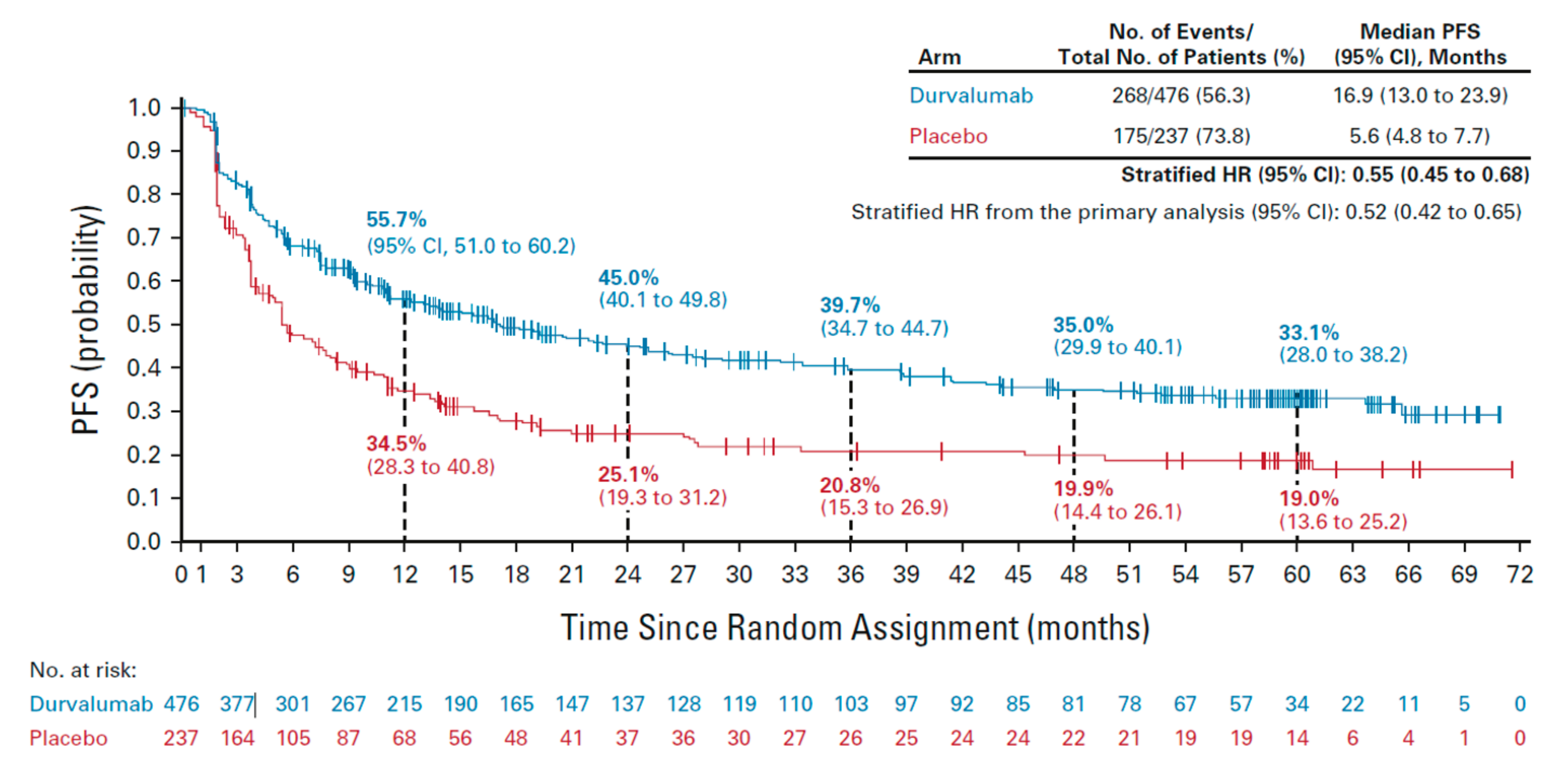
- Spigel, D.R.; Faivre-Finn, C.; Gray, J.E.; Vicente, D.; Planchard, D.; Paz-Ares, L.; Vansteenkiste, J.F.; Garassino, M.C.; Hui, R.; Quantin, X.; et al. Five-year survival outcomes from the PACIFIC trial: Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. J. Clin. Oncol. 2022, 40, 1301–1311. [Google Scholar] [CrossRef]
- Schneider, B.J.; Ismaila, N.; Aerts, J.; Chiles, C.; Daly, M.E.; Detterbeck, F.C.; Hearn, J.W.D.; Katz, S.I.; Leighl, N.B.; Levy, B.; et al. Lung cancer surveillance after definitive curative-intent therapy: ASCO guideline. J. Clin. Oncol. 2020, 38, 753–766. [Google Scholar] [CrossRef]
- Ung, Y.C.; Souter, L.H.; Darling, G.; Dobranowski, J.; Donohue, L.; Leighl, N.; Ellis, P.M.; the Lung Cancer Follow-up Expert Panel. Cancer Care Ontario. Follow-Up and Surveillance of Curatively Treated Lung Cancer Patients. 29 August 2014. Available online: https://www.cancercareontario.ca/sites/ccocancercare/files/guidelines/summary/pebc26-3s.pdf (accessed on 11 January 2022).
- Ho, Q.-A.; Harandi, N.K.; Daly, M.E. Clinical impact of frequent surveillance imaging in the first year following chemoradiation for locally advanced non-small-cell lung cancer. Clin. Lung Cancer 2017, 18, 410–414. [Google Scholar] [CrossRef]
- Grass, G.D.; Naghavi, A.O.; Abuodeh, Y.A.; Perez, B.A.; Dilling, T.J. Analysis of relapse events after definitive chemoradiotherapy in locally advanced non-small-cell lung cancer patients. Clin. Lung Cancer 2019, 20, e1–e7. [Google Scholar] [CrossRef]
- Hall, H.; Tocock, A.; Burdett, S.; Fisher, D.; Ricketts, W.M.; Robson, J.; Round, T.; Gorolay, S.; MacArthur, E.; Chung, D.; et al. Association between time-to-treatment and outcomes in non-small cell lung cancer: A systematic review. Thorax 2021, 77, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): A randomised, phase 2, open-label trial. Lancet 2019, 393, 2051–2058. [Google Scholar] [CrossRef] [PubMed]
- Hearn, J.W.; Videtic, G.M.; Djemil, T.; Stephans, K.L. Salvage stereotactic body radiation therapy (SBRT) for local failure after primary lung SBRT. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 402–406. [Google Scholar] [CrossRef]
- Benamore, R.; Shepherd, F.A.; Leighl, N.; Pintilie, M.; Patel, M.; Feld, R.; Herman, S. Does intensive follow-up alter outcome in patients with advanced lung cancer? J. Thor. Oncol. 2007, 2, 273–281. [Google Scholar] [CrossRef] [Green Version]
- McMurry, T.L.; Stukenborg, G.J.; Kessler, L.G.; Colditz, G.A.; Wong, M.L.; Francescatti, A.B.; Jones, D.R.; Schumacher, J.R.; Greenberg, C.C.; Chang, G.J.; et al. More frequent surveillance following lung cancer resection is not associated with improved survival: A nationally representative cohort study. Ann. Surg. 2018, 268, 632–639. [Google Scholar] [CrossRef] [PubMed]
- Calman, L.; Beaver, K.; Hind, D.; Lorigan, P.; Roberts, C.; Lloyd-Jones, M. Survival benefits from follow-up of patients with lung cancer: A systematic review and meta-analysis. J. Thorac. Oncol. 2011, 6, 1993–2004. [Google Scholar] [CrossRef] [Green Version]
- Dyer, B.A.; Daly, M.E. Surveillance imaging following definitive radiotherapy for non-small cell lung cancer: What is the clinical impact? Semin. Oncol. 2017, 44, 303–309. [Google Scholar] [CrossRef]
- Canadian Association of Thoracic Surgeons. Follow-Up and Surveillance—Curatively-Treated Lung Cancer. Available online: https://www.canadianthoracicsurgeons.ca/2018/08/28/surveillance/ (accessed on 23 March 2022).
- Jazieh, A.R.; Onal, H.C.; Tan, D.S.W.; Soo, R.A.; Prabhash, K.; Kumar, A.; Huggenberger, R.; Robb, S.; Cho, B.-C. Real-world treatment patterns and clinical outcomes in patients with stage III NSCLC: Results of KINDLE, a multicountry observational study. J. Thorac. Oncol. 2021, 16, 1733–1744. [Google Scholar] [CrossRef]
- Pignon, J.P.; Tribodet, H.; Scagliotti, G.V.; Douillard, J.Y.; Shepherd, F.A.; Stephens, R.J.; Dunant, A.; Torri, V.; Rosell, R.; Seymour, L.; et al. Lung adjuvant cisplatin evaluation: A pooled analysis by the LACE Collaborative Group. J. Clin. Oncol. 2008, 26, 3552–3559. [Google Scholar] [CrossRef]
- Ko, J.J.; (BC Cancer, Abbotsford, BC, Canada); Melosky, B.; (BC Cancer, Vancouver, BC, Canada). Personal communication, 2022.
- Kea, B.; Sun, B.C.-A. Consensus development for healthcare professionals. Intern. Emerg. Med. 2015, 10, 373–383. [Google Scholar] [CrossRef]
- Provincial Health Services Authority. BC Cancer. Lung-Management. Available online: http://www.bccancer.bc.ca/health-professionals/clinical-resources/cancer-management-manual/lung/lung#Management (accessed on 15 July 2022).
- Soria, J.-C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in untreated EGFR-mutated advanced non–small-cell lung cancer. N. Engl. J. Med. 2017, 378, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Shields, M.D.; Marin-Acevedo, J.A.; Pellini, B. Immunotherapy for advanced non–small cell lung cancer: A decade of progress. Am. Soc. Clin. Oncol. Educ. Book 2021, 41, e105–e127. [Google Scholar] [CrossRef] [PubMed]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Kurata, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Trial protocol for: Overall survival with durvalumab after chemoradiotherapy in stage III NSCLC. N. Engl. J. Med. 2018, 379, 2342–2350. [Google Scholar] [CrossRef] [PubMed]
- Lou, F.; Sima, C.S.; Rusch, V.W.; Jones, D.R.; Huang, J. Differences in patterns of recurrence in early-stage versus locally advanced non-small cell lung cancer. Ann. Thorac. Surg. 2014, 98, 1755–1760. [Google Scholar] [CrossRef] [Green Version]
- Sugimura, H.; Yang, P. Long-term survivorship in lung cancer: A review. Chest 2006, 129, 1088–1097. [Google Scholar] [CrossRef] [Green Version]
- de Koning, H.J.; van der Aalst, C.M.; de Jong, P.A.; Scholten, E.T.; Nackaerts, K.; Heuvelmans, M.A.; Lammers, J.-W.J.; Weenink, C.; Yousaf-Khan, U.; Horeweg, N.; et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N. Engl. J. Med. 2020, 382, 503–513. [Google Scholar] [CrossRef]
- Tammemägi, M.C.; Ruparel, M.; Tremblay, A.; Myers, R.; Mayo, J.; Yee, J.; Atkar-Khattra, S.; Yuan, R.; Cressman, S.; English, J.; et al. USPSTF2013 versus PLCOm2012 lung cancer screening eligibility criteria (International Lung Screening Trial): Interim analysis of a prospective cohort study. Lancet Oncol. 2022, 23, 138–148. [Google Scholar] [CrossRef]
- National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef] [Green Version]
- Johnson, B.E. Second lung cancers in patients after treatment for an initial lung cancer. J. Natl. Cancer Inst. 1998, 90, 1335–1345. [Google Scholar] [CrossRef]
- Takahashi, M.; Nitta, N.; Takazakura, R.; Nagatani, Y.; Ushio, N.; Murata, K. Detection of mediastinal and hilar lymph nodes by 16-row MDCT: Is contrast material needed? Eur. J. Radiol. 2008, 66, 287–291. [Google Scholar] [CrossRef]
- García-Garrigós, E.; Arenas-Jiménez, J.J.; Sánchez-Payá, J. Best protocol for combined contrast-enhanced thoracic and abdominal CT for lung cancer: A single-institution randomized crossover clinical trial. AJR Am. J. Roentgenol. 2018, 210, 1226–1234. [Google Scholar] [CrossRef] [PubMed]
- Bhalla, A.S.; Das, A.; Naranje, P.; Irodi, A.; Raj, V.; Goyal, A. Imaging protocols for CT chest: A recommendation. Indian J. Radiol. Imaging 2019, 29, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Huynh, K.; Baghdanian, A.H.; Baghdanian, A.A.; Sun, D.S.; Kolli, K.P.; Zagoria, R.J. Updated guidelines for intravenous contrast use for CT and MRI. Emerg. Radiol. 2020, 27, 115–126. [Google Scholar] [CrossRef]
- Caraiani, C.; Petresc, B.; Dong, Y.; Dietrich, C.F. Contraindications and adverse effects in abdominal imaging. Med. Ultrason. 2019, 21, 456–463. [Google Scholar] [CrossRef] [PubMed]
- American College of Radiology. ACR Manual on Contrast Media; ACR Committee on Drugs and Contrast Media, 2021; ISBN 978-1-55903-012-0. [Google Scholar]
- Yokoi, K.; Kamiya, N.; Matsuguma, H.; Machida, S.; Hirose, T.; Mori, K.; Tominaga, K. Detection of brain metastasis in potentially operable non-small cell lung cancer: A comparison of CT and MRI. Chest 1999, 115, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Ellingson, B.M.; Bendszus, M.; Boxerman, J.; Barboriak, D.; Erickson, B.J.; Smits, M.; Nelson, S.J.; Gerstner, E.; Alexander, B.; Goldmacher, G.; et al. Consensus recommendations for a standardized brain tumor imaging protocol in clinical trials. Neuro-Oncology 2015, 17, 1188–1198. [Google Scholar] [CrossRef] [Green Version]
- Kuhn, M.J.; Hammer, G.M.; Swenson, L.C.; Youssef, H.T.; Gleason, T.J. MRI evaluation of “solitary” brain metastases with triple-dose gadoteridol: Comparison with contrast-enhanced CT and conventional-dose gadopentetate dimeglumine MRI studies in the same patients. Comput. Med. Imaging Graph. 1994, 18, 391–399. [Google Scholar] [CrossRef]
- Naidoo, J.; Nishino, M.; Patel, S.P.; Shankar, B.; Rekhtman, N.; Illei, P.; Camus, P. Immune-related pneumonitis after chemoradiotherapy and subsequent immune checkpoint blockade in unresectable stage III non–small-cell lung cancer. Clin. Lung Cancer 2020, 21, e435–e444. [Google Scholar] [CrossRef] [Green Version]
- Vansteenkiste, J.; Naidoo, J.; Faivre-Finn, C.; Özgüroğlu, M.; Villegas, A.; Daniel, D.; Murakami, S.; Hui, R.; Lee, K.; Cho, B.C.; et al. MA05. 02 PACIFIC subgroup analysis: Pneumonitis in stage III, unresectable NSCLC patients treated with durvalumab vs. placebo after CRT. J. Thorac. Oncol. 2018, 13, S370–S371. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Target Population | Patients with curatively treated, stage III, unresectable NSCLC who complete CRT ± consolidation therapy with durvalumab as per the PACIFIC trial and are without clinical suspicion of recurrent disease. | |
| Target Audience | Medical, surgical, and radiation oncologists; oncology nurses and physician assistants; pulmonologists, radiologists; family physician/community primary care team; and patients. | |
| Note | Patient history and physical examination should occur at regular intervals in all years. | |
| Clinical Question | Recommendation | Key Considerations |
| 1. What timepoint should be used as a reference for initiation of imaging? | Recommendation 1.1: For all patients with stage III unresectable NSCLC, imaging should be performed after completion of CRT, regardless of whether durvalumab is received. |
|
| 2. What is the recommended frequency of imaging? | Recommendation 2.1: In Year 1 after CRT, all patients should undergo imaging every 3 months. Recommendation 2.2: In Year 2, all patients should undergo imaging at least every 6 months. Recommendation 2.3: In Years 3, 4, and 5, all patients should undergo imaging at least every 12 months. |
|
| 3. What type of imaging should be used and which body regions should be assessed? | Recommendation 3.1: Contrast CT of the chest and upper abdomen should be used through the end of Year 5 after CRT. Recommendation 3.2: Routine brain imaging is not recommended. |
|
| 4. Who should follow the patient? | Recommendation 4.1: For patients who receive durvalumab, the medical oncologist should follow during Year 1 after CRT; the radiation oncologist should be involved if pneumonitis is suspected. Recommendation 4.2: After Year 1, follow-up can alternate between the medical oncologist and radiation oncologist until transition to the family physician/community primary care team. Recommendation 4.3: For patients who do not receive durvalumab, follow-up can alternate between the medical oncologist and the radiation oncologist post-CRT until transition to the family physician/community primary care team. Recommendation 4.4: Some patients can be transitioned to the family physician/community primary care team after Year 2 following completion of CRT. |
|
| 5. What other assessments or activities should be conducted? | Recommendation 5.1: Throughout Years 1 to 5 after CRT, patients should receive information on smoking cessation, comorbidity management, and relevant vaccinations, as applicable, and be encouraged to receive regular follow-up care for non-cancer conditions and general health concerns. |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ko, J.J.; Banerji, S.; Blais, N.; Brade, A.; Clelland, C.; Schellenberg, D.; Snow, S.; Wheatley-Price, P.; Yuan, R.; Melosky, B. Follow-Up Imaging Guidelines for Patients with Stage III Unresectable NSCLC: Recommendations Based on the PACIFIC Trial. Curr. Oncol. 2023, 30, 3817-3828. https://doi.org/10.3390/curroncol30040289
Ko JJ, Banerji S, Blais N, Brade A, Clelland C, Schellenberg D, Snow S, Wheatley-Price P, Yuan R, Melosky B. Follow-Up Imaging Guidelines for Patients with Stage III Unresectable NSCLC: Recommendations Based on the PACIFIC Trial. Current Oncology. 2023; 30(4):3817-3828. https://doi.org/10.3390/curroncol30040289
Chicago/Turabian StyleKo, Jenny J., Shantanu Banerji, Normand Blais, Anthony Brade, Cathy Clelland, Devin Schellenberg, Stephanie Snow, Paul Wheatley-Price, Ren Yuan, and Barbara Melosky. 2023. "Follow-Up Imaging Guidelines for Patients with Stage III Unresectable NSCLC: Recommendations Based on the PACIFIC Trial" Current Oncology 30, no. 4: 3817-3828. https://doi.org/10.3390/curroncol30040289