Survival Benefits of Adjuvant Chemotherapy for Positive Soft Tissue Surgical Margins Following Radical Cystectomy in Bladder Cancer with Extravesical Extension

 , ,
, , 
Abstract
:1. Introduction
2. Methods
Statistical Analysis
3. Results
3.1. Demographic and Clinicopathologic Features
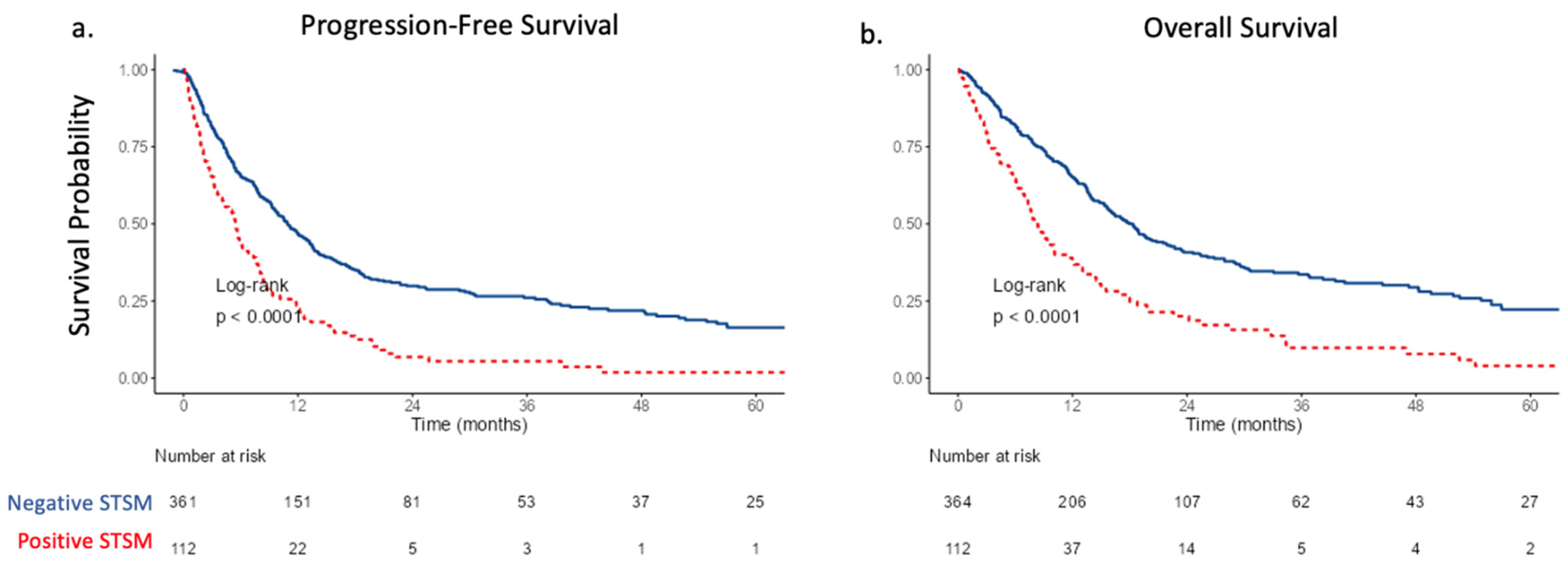
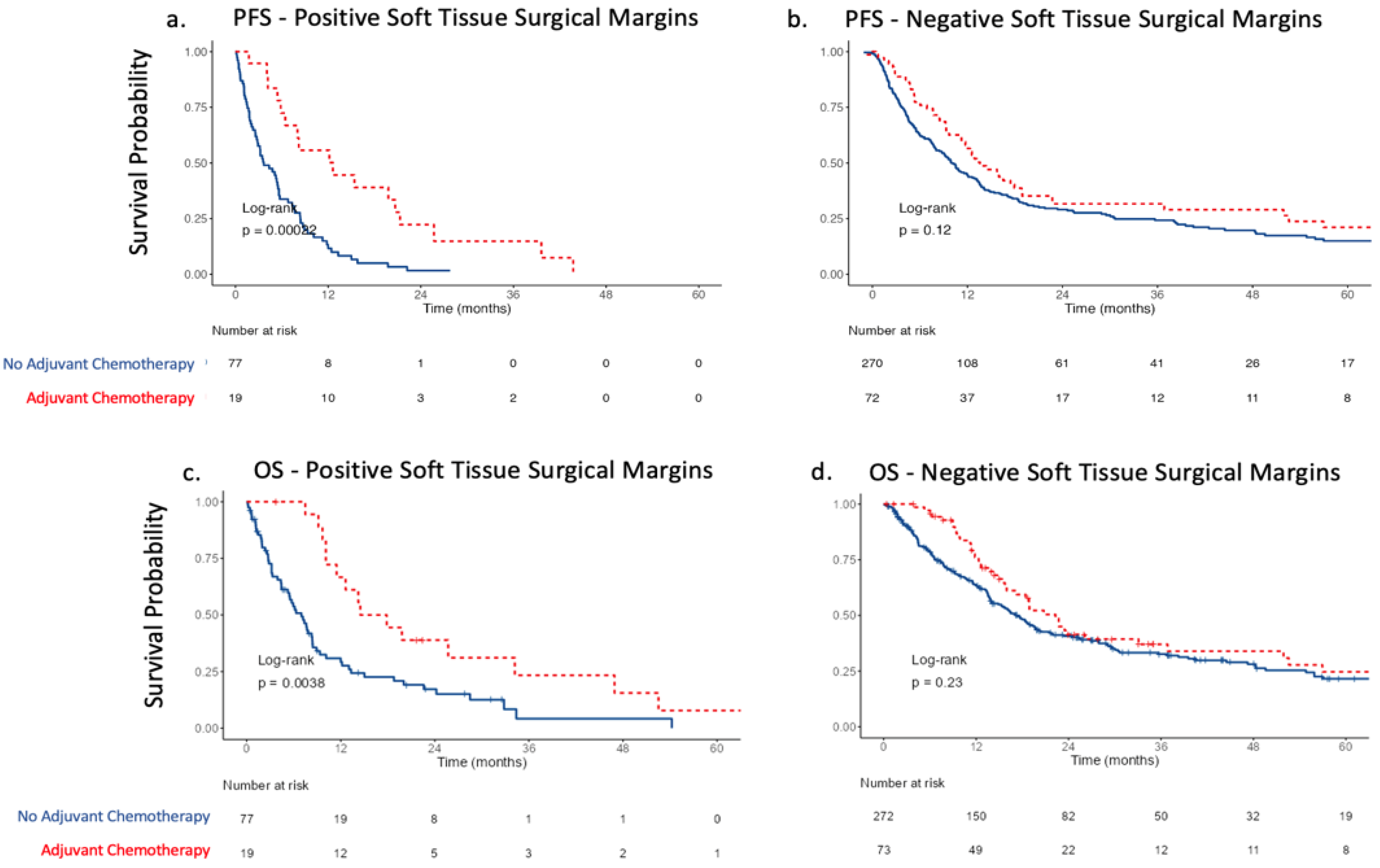
3.2. Survival Estimates
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Burdett, S.; Fisher, D.J.; Vale, C.L.; Sternberg, C.N.; Clarke, N.W.; Parmar, M.K.B.; Bono, A.V.; Cognetti, F.; Collette, L.; Cote, R.J.; et al. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer: A Systematic Review and Meta-Analysis of Individual Participant Data from Randomised Controlled Trials. Eur. Urol. 2022, 81, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, C.N.; Skoneczna, I.; Kerst, J.M.; Albers, P.; Fossa, S.D.; Agerbaek, M.; Dumez, H.; de Santis, M.; Théodore, C.; Leahy, M.G.; et al. Immediate versus Deferred Chemotherapy after Radical Cystectomy in Patients with PT3–PT4 or N+ M0 Urothelial Carcinoma of the Bladder (EORTC 30994): An Intergroup, Open-Label, Randomised Phase 3 Trial. Lancet Oncol. 2015, 16, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Studer, U.E.; Bacchi, M.; Biedermann, C.; Jaeger, P.; Kraft, R.; Mazzucchelli, L.; Markwalder, R.; Senn, E.; Sonntag, R.W. Adjuvant Cisplatin Chemotherapy Following Cystectomy for Bladder Cancer: Results of a Prospective Randomized Trial. J. Urol. 1994, 152, 81–84. [Google Scholar] [CrossRef]
- Stadler, W.M.; Lerner, S.P.; Groshen, S.; Stein, J.P.; Shi, S.-R.; Raghavan, D.; Esrig, D.; Steinberg, G.; Wood, D.; Klotz, L.; et al. Phase III Study of Molecularly Targeted Adjuvant Therapy in Locally Advanced Urothelial Cancer of the Bladder Based on P53 Status. J. Clin. Oncol. 2011, 29, 3443–3449. [Google Scholar] [CrossRef] [PubMed]
- Freiha, F.; Reese, J.; Torti, F.M. A Randomized Trial of Radical Cystectomy versus Radical Cystectomy plus Cisplatin, Vinblastine and Methotrexate Chemotherapy for Muscle Invasive Bladder Cancer. J. Urol. 1996, 155, 495–499; discussion 499–500. [Google Scholar] [CrossRef] [PubMed]
- Bellmunt, J.; Hussain, M.; Gschwend, J.E.; Albers, P.; Oudard, S.; Castellano, D.; Daneshmand, S.; Nishiyama, H.; Majchrowicz, M.; Degaonkar, V.; et al. Adjuvant Atezolizumab versus Observation in Muscle-Invasive Urothelial Carcinoma (IMvigor010): A Multicentre, Open-Label, Randomised, Phase 3 Trial. Lancet Oncol. 2021, 22, 525–537. [Google Scholar] [CrossRef]
- Dotan, Z.A.; Kavanagh, K.; Yossepowitch, O.; Kaag, M.; Olgac, S.; Donat, M.; Herr, H.W. Positive Surgical Margins in Soft Tissue Following Radical Cystectomy for Bladder Cancer and Cancer Specific Survival. J. Urol. 2007, 178, 2308–2312; discussion 2313. [Google Scholar] [CrossRef]
- Novara, G.; Svatek, R.S.; Karakiewicz, P.I.; Skinner, E.; Ficarra, V.; Fradet, Y.; Lotan, Y.; Isbarn, H.; Capitanio, U.; Bastian, P.J.; et al. Soft Tissue Surgical Margin Status Is a Powerful Predictor of Outcomes after Radical Cystectomy: A Multicenter Study of More than 4,400 Patients. J. Urol. 2010, 183, 2165–2170. [Google Scholar] [CrossRef]
- Lehmann, J.; Franzaring, L.; Thüroff, J.; Wellek, S.; Stöckle, M. Complete Long-Term Survival Data from a Trial of Adjuvant Chemotherapy vs Control after Radical Cystectomy for Locally Advanced Bladder Cancer. BJU Int. 2006, 97, 42–47. [Google Scholar] [CrossRef]
- Stöckle, M.; Wellek, S.; Meyenburg, W.; Voges, G.E.; Fischer, U.; Gertenbach, U.; Thüroff, J.W.; Huber, C.; Hohenfellner, R. Radical Cystectomy with or without Adjuvant Polychemotherapy for Non-Organ-Confined Transitional Cell Carcinoma of the Urinary Bladder: Prognostic Impact of Lymph Node Involvement. Urology 1996, 48, 868–875. [Google Scholar] [CrossRef]
- Stein, J.P.; Lieskovsky, G.; Cote, R.; Groshen, S.; Feng, A.-C.; Boyd, S.; Skinner, E.; Bochner, B.; Thangathurai, D.; Mikhail, M.; et al. Radical Cystectomy in the Treatment of Invasive Bladder Cancer: Long-Term Results in 1054 Patients. J. Clin. Oncol. 2001, 19, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Guidelines Detail. Available online: https://www.nccn.org/guidelines/guidelines-detail (accessed on 19 August 2022).
- Zaghloul, M.S.; Christodouleas, J.P.; Smith, A.; Abdallah, A.; William, H.; Khaled, H.M.; Hwang, W.-T.; Baumann, B.C. Adjuvant Sandwich Chemotherapy Plus Radiotherapy vs Adjuvant Chemotherapy Alone for Locally Advanced Bladder Cancer After Radical Cystectomy: A Randomized Phase 2 Trial. JAMA Surg. 2018, 153, e174591. [Google Scholar] [CrossRef] [PubMed]
- Zhegalik, A.G.; Polyakov, S.L.; Rolevich, A.I.; Volkov, A.N.; Minich, A.A.; Vasilevich, V.J.; Mokhort, A.A.; Krasny, S.A.; Sukonko, O.G. Long-Term Results of a Single-Center Prospective Randomized Trial Assessing Efficacy of a Shortened Course of Adjuvant Chemotherapy after Radical Cystectomy in Patients with Locally Advanced Bladder Cancer. Cent. Eur. J. Urol. 2020, 73, 26–32. [Google Scholar] [CrossRef]
- Cognetti, F.; Ruggeri, E.M.; Felici, A.; Gallucci, M.; Muto, G.; Pollera, C.F.; Massidda, B.; Rubagotti, A.; Giannarelli, D.; Boccardo, F.; et al. Adjuvant Chemotherapy with Cisplatin and Gemcitabine versus Chemotherapy at Relapse in Patients with Muscle-Invasive Bladder Cancer Submitted to Radical Cystectomy: An Italian, Multicenter, Randomized Phase III Trial. Ann. Oncol. 2012, 23, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, D.; Raghavan, D.; Carducci, M.; Levine, E.G.; Murphy, B.; Aisner, J.; Kuzel, T.; Nicol, S.; Oh, W.; Stadler, W. Phase II Trial of Gemcitabine plus Cisplatin in Patients with Metastatic Urothelial Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2000, 18, 1921–1927. [Google Scholar] [CrossRef] [PubMed]
- Saxman, S.B.; Propert, K.J.; Einhorn, L.H.; Crawford, E.D.; Tannock, I.; Raghavan, D.; Loehrer, P.J.; Trump, D. Long-Term Follow-up of a Phase III Intergroup Study of Cisplatin Alone or in Combination with Methotrexate, Vinblastine, and Doxorubicin in Patients with Metastatic Urothelial Carcinoma: A Cooperative Group Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1997, 15, 2564–2569. [Google Scholar] [CrossRef]
- Sternberg, C.N.; Yagoda, A.; Scher, H.I.; Watson, R.C.; Geller, N.; Herr, H.W.; Morse, M.J.; Sogani, P.C.; Vaughan, E.D.; Bander, N. Methotrexate, Vinblastine, Doxorubicin, and Cisplatin for Advanced Transitional Cell Carcinoma of the Urothelium. Efficacy and Patterns of Response and Relapse. Cancer 1989, 64, 2448–2458. [Google Scholar] [CrossRef] [PubMed]
- De Santis, M.; Bellmunt, J.; Mead, G.; Kerst, J.M.; Leahy, M.; Maroto, P.; Skoneczna, I.; Marreaud, S.; de Wit, R.; Sylvester, R. Randomized Phase II/III Trial Assessing Gemcitabine/ Carboplatin and Methotrexate/Carboplatin/Vinblastine in Patients with Advanced Urothelial Cancer “Unfit” for Cisplatin-Based Chemotherapy: Phase II—Results of EORTC Study 30986. J. Clin. Oncol. 2009, 27, 5634–5639. [Google Scholar] [CrossRef] [Green Version]
- von der Maase, H.; Sengelov, L.; Roberts, J.T.; Ricci, S.; Dogliotti, L.; Oliver, T.; Moore, M.J.; Zimmermann, A.; Arning, M. Long-Term Survival Results of a Randomized Trial Comparing Gemcitabine plus Cisplatin, with Methotrexate, Vinblastine, Doxorubicin, plus Cisplatin in Patients with Bladder Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 4602–4608. [Google Scholar] [CrossRef]
- Vuky, J.; Balar, A.V.; Castellano, D.; O’Donnell, P.H.; Grivas, P.; Bellmunt, J.; Powles, T.; Bajorin, D.; Hahn, N.M.; Savage, M.J.; et al. Long-Term Outcomes in KEYNOTE-052: Phase II Study Investigating First-Line Pembrolizumab in Cisplatin-Ineligible Patients with Locally Advanced or Metastatic Urothelial Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 2658–2666. [Google Scholar] [CrossRef]
- Balar, A.V.; Galsky, M.D.; Rosenberg, J.E.; Powles, T.; Petrylak, D.P.; Bellmunt, J.; Loriot, Y.; Necchi, A.; Hoffman-Censits, J.; Perez-Gracia, J.L.; et al. Atezolizumab as First-Line Treatment in Cisplatin-Ineligible Patients with Locally Advanced and Metastatic Urothelial Carcinoma: A Single-Arm, Multicentre, Phase 2 Trial. Lancet Lond. Engl. 2017, 389, 67–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powles, T.; Assaf, Z.J.; Davarpanah, N.; Banchereau, R.; Szabados, B.E.; Yuen, K.C.; Grivas, P.; Hussain, M.; Oudard, S.; Gschwend, J.E.; et al. CtDNA Guiding Adjuvant Immunotherapy in Urothelial Carcinoma. Nature 2021, 595, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Neuzillet, Y.; Soulie, M.; Larre, S.; Roupret, M.; Defortescu, G.; Murez, T.; Pignot, G.; Descazeaud, A.; Patard, J.-J.; Bigot, P.; et al. Positive Surgical Margins and Their Locations in Specimens Are Adverse Prognosis Features after Radical Cystectomy in Non-Metastatic Carcinoma Invading Bladder Muscle: Results from a Nationwide Case–Control Study. BJU Int. 2013, 111, 1253–1260. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Negative (N = 364) | Positive (N = 112) | Total (N = 476) | p Value | |
|---|---|---|---|---|
| Age | 0.264 | |||
| Mean (SD) | 70.5 (10.6) | 71.7 (10.0) | 70.8 (10.5) | |
| Range | 36.0–92.0 | 33.0–92.0 | 33.0–92.0 | |
| Sex | 0.783 | |||
| Female | 80 (22.0%) | 26 (23.2%) | 106 (22.3%) | |
| Male | 284 (78.0%) | 86 (76.8%) | 370 (77.7%) | |
| pT Stage | <0.001 | |||
| T3b | 197 (54.1%) | 30 (26.8%) | 227 (47.7%) | |
| T4 | 167 (45.9%) | 82 (73.2%) | 249 (52.3%) | |
| pN Stage | <0.001 | |||
| Nx | 15 (4.1%) | 16 (14.2%) | 31 (6.5%) | |
| N0 | 203 (55.8%) | 48 (42.9%) | 251 (52.7%) | |
| N1–3 | 146 (40.1%) | 48 (42.9%) | 194 (40.8%) | |
| ECOG | 0.086 | |||
| Missing | 1 (0.3%) | 0 (0%) | 1 (0.2%) | |
| 0 | 253 (69.5%) | 66 (58.9%) | 319 (67.0%) | |
| 1 | 84 (23.1%) | 29 (25.9%) | 113 (23.8%) | |
| 2 | 18 (4.9%) | 11 (9.8%) | 29 (6.1%) | |
| 3 | 6 (1.6%) | 5 (4.5%) | 11 (2.3%) | |
| 4 | 2 (0.6%) | 1 (0.9%) | 3 (0.6%) | |
| Neoadjuvant Chemotherapy | 0.505 | |||
| No | 208 (57.1%) | 60 (53.6%) | 268 (56.3%) | |
| Yes | 156 (42.9%) | 52 (46.4%) | 208 (43.7%) | |
| Adjuvant Chemotherapy | 0.771 | |||
| N-Miss | 19 (5.2%) | 16 (14.3%) | 35 (7.4%) | |
| No | 272 (74.8%) | 77 (80.2%) | 349 (73.3%) | |
| Yes | 73 (20.0%) | 19 (19.8%) | 92 (19.3%) | |
| ≥CKD3 | 0.197 | |||
| N-Miss | 54 (14.8%) | 21 (18.7%) | 75 (15.8%) | |
| No | 177 (48.6%) | 45 (40.2%) | 222 (46.6%) | |
| Yes | 133 (36.6%) | 46 (41.1%) | 179 (37.6%) |
| Progression-Free Survival | Overall Survival | |||||
|---|---|---|---|---|---|---|
| N | HR (Univariable) | HR (Multivariable) | HR (Univariable) | HR (Multivariable) | ||
| Age | Mean (SD) | 70.8 (10.5) | 1.01 (1.00–1.02, p = 0.086) | 1.01 (1.00–1.02, p = 0.118) | 1.01 (1.00–1.02, p = 0.140) | 1.01 (0.99–1.02, p = 0.304) |
| ECOG | ||||||
| 0 | 292 (66.4) | - | - | - | - | |
| 1 | 106 (24.1) | 1.15 (0.89–1.47, p = 0.289) | 1.07 (0.83–1.38, p = 0.603) | 1.15 (0.88–1.51, p = 0.297) | 1.10 (0.84–1.44, p = 0.504) | |
| 2 | 29 (6.6) | 1.64 (1.08–2.49, p = 0.020) | 1.54 (1.01–2.34, p = 0.046) | 1.50 (0.97–2.34, p = 0.071) | 1.30 (0.83–2.04, p = 0.252) | |
| 3 | 10 (2.3) | 2.08 (1.07–4.06, p = 0.032) | 1.40 (0.70–2.79, p = 0.340) | 1.58 (0.78–3.21, p = 0.207) | 1.15 (0.56–2.40, p = 0.700) | |
| 4 | 3 (0.7) | 1.70 (0.42–6.84, p = 0.457) | 1.90 (0.47–7.72, p = 0.372) | 2.97 (0.73–11.99, p = 0.127) | 3.52 (0.86–14.44, p = 0.080) | |
| Positive Soft Tissue Margin | ||||||
| No | 344 (78.2) | - | - | - | - | |
| Yes | 96 (21.8) | 2.19 (1.70–2.83, p < 0.001) | 2.04 (1.55–2.68, p < 0.001) | 2.14 (1.65–2.79, p < 0.001) | 1.93 (1.45–2.57, p < 0.001) | |
| pT Stage | ||||||
| T3b | 212 (48.2) | - | - | - | - | |
| T4 | 228 (51.8) | 1.40 (1.13–1.73, p = 0.002) | 1.19 (0.94–1.50, p = 0.145) | 1.43 (1.14–1.79, p = 0.002) | 1.21 (0.95–1.55, p = 0.128) | |
| pN Stage | ||||||
| N0 | 230 (52.3) | - | - | - | - | |
| N1–3 | 184 (41.8) | 2.12 (1.70–2.65, p < 0.001) | 2.16 (1.73–2.72, p < 0.001) | 1.56 (1.23–1.97, p < 0.001) | 1.47 (1.16–1.87, p = 0.002) | |
| Nx | 26 (5.9) | 1.80 (1.15–2.81, p = 0.011) | 1.42 (0.89–2.25, p = 0.137) | 1.90 (1.20–3.01, p = 0.006) | 1.55 (0.96–2.51, p = 0.076) | |
| Neoadjuvant Chemotherapy | ||||||
| No | 245 (55.7) | - | - | - | - | |
| Yes | 195 (44.3) | 1.14 (0.92–1.41, p = 0.219) | 1.12 (0.89–1.40, p = 0.330) | 1.02 (0.81–1.29, p = 0.839) | 0.94 (0.74–1.20, p = 0.626) | |
| Adjuvant Chemotherapy | ||||||
| No | 349 (79.3) | - | - | - | - | |
| Yes | 91 (20.7) | 0.71 (0.55–0.93, p = 0.012) | 0.59 (0.45–0.77, p < 0.001) | 0.76 (0.57–1.00, p = 0.052) | 0.68 (0.51–0.91, p = 0.009) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murthy, P.B.; Naidu, S.; Davaro, F.; Spiess, P.E.; Zemp, L.; Poch, M.; Jain, R.; Vosoughi, A.; Grass, G.D.; Yu, A.; et al. Survival Benefits of Adjuvant Chemotherapy for Positive Soft Tissue Surgical Margins Following Radical Cystectomy in Bladder Cancer with Extravesical Extension. Curr. Oncol. 2023, 30, 3223-3231. https://doi.org/10.3390/curroncol30030245
Murthy PB, Naidu S, Davaro F, Spiess PE, Zemp L, Poch M, Jain R, Vosoughi A, Grass GD, Yu A, et al. Survival Benefits of Adjuvant Chemotherapy for Positive Soft Tissue Surgical Margins Following Radical Cystectomy in Bladder Cancer with Extravesical Extension. Current Oncology. 2023; 30(3):3223-3231. https://doi.org/10.3390/curroncol30030245
Chicago/Turabian StyleMurthy, Prithvi B., Shreyas Naidu, Facundo Davaro, Philippe E. Spiess, Logan Zemp, Michael Poch, Rohit Jain, Aram Vosoughi, G. Daniel Grass, Alice Yu, and et al. 2023. "Survival Benefits of Adjuvant Chemotherapy for Positive Soft Tissue Surgical Margins Following Radical Cystectomy in Bladder Cancer with Extravesical Extension" Current Oncology 30, no. 3: 3223-3231. https://doi.org/10.3390/curroncol30030245