Assessment of the Ecological Association between Tobacco Smoking Exposure and Bladder Cancer Incidence over the Past Half-Century in the United States

Abstract
:1. Introduction
2. Materials and Methods
2.1. Tobacco Smoking Prevalence
2.2. Age-Adjusted Bladder and Lung Cancer Incidence Rates
2.3. Statistical Analyses
3. Results
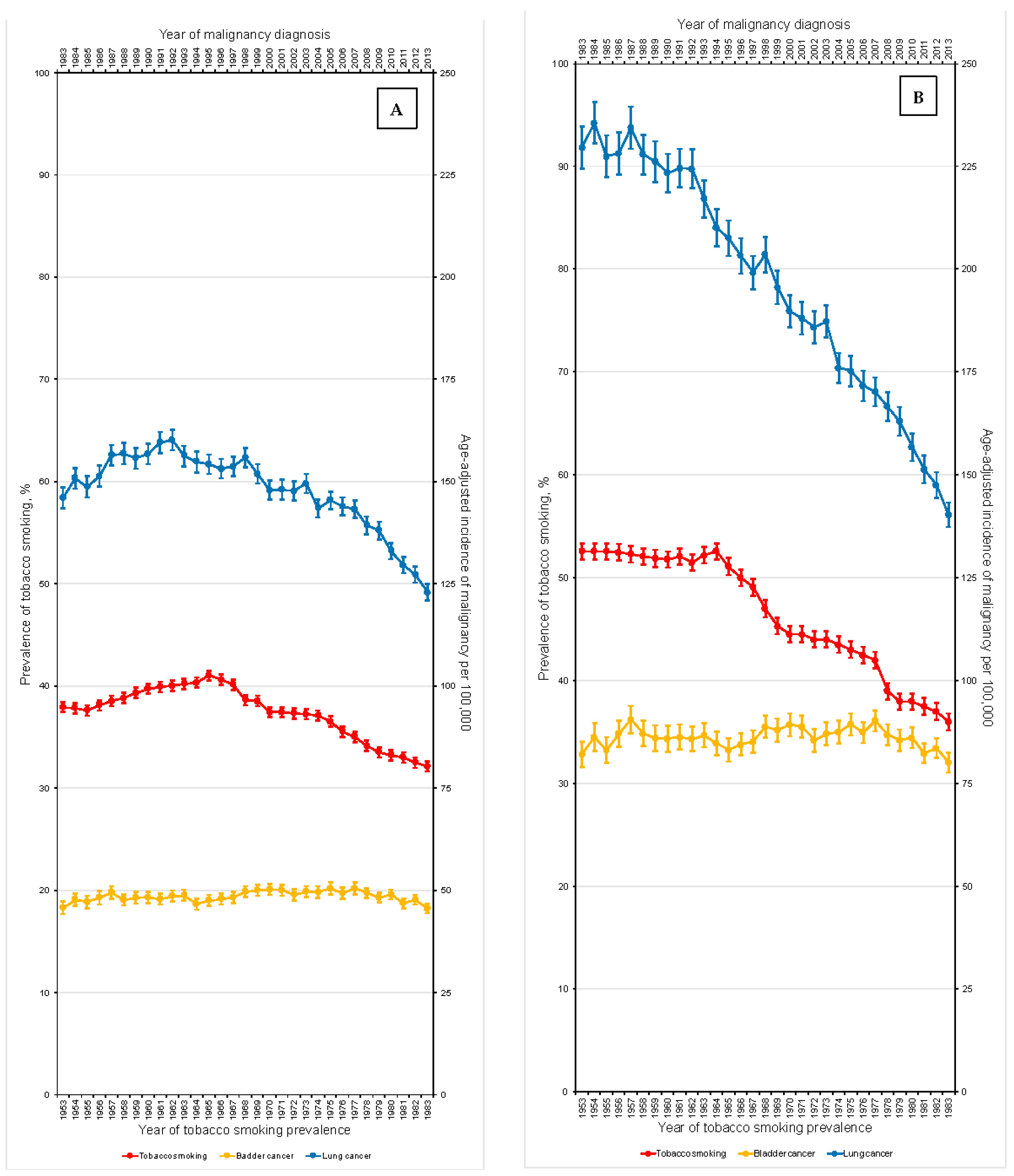
3.1. Overall Population
3.1.1. Annual Percent Changes in Tobacco Smoking Prevalence and Cancer Age-Adjusted Incidence Rates
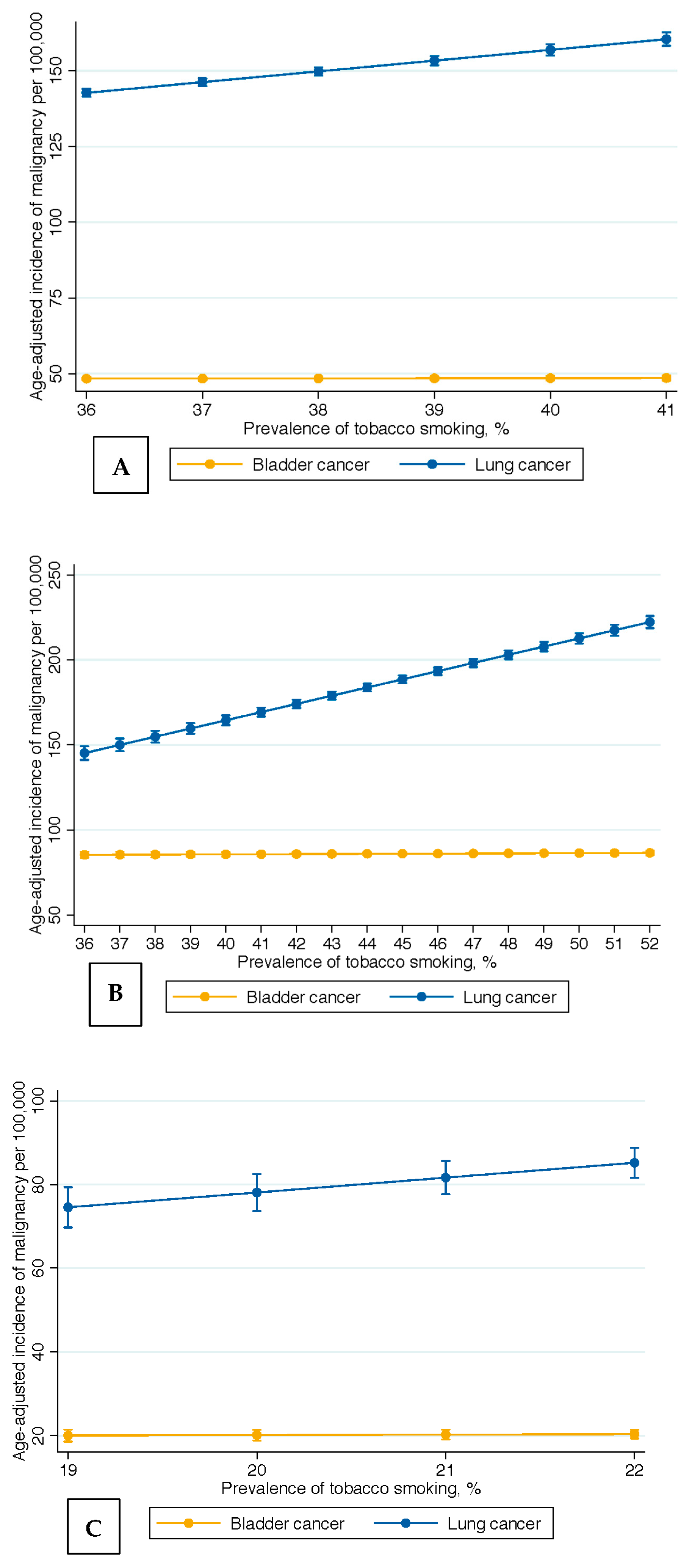
3.1.2. Incidence Rate Differences for Bladder and Lung Cancer
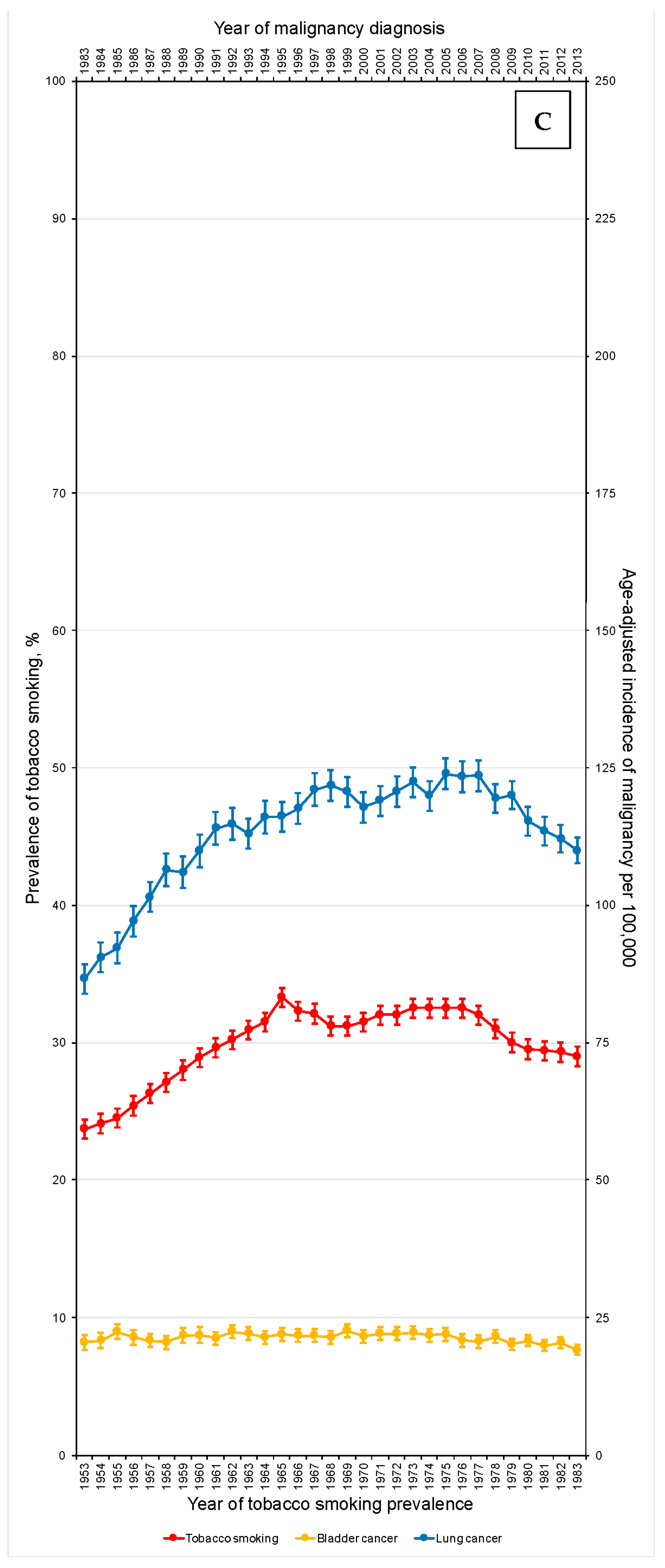
3.2. Gender-Specific
3.2.1. Annual Percent Changes in Tobacco Smoking Prevalence and Cancer Age-Adjusted Incidence Rates
3.2.2. Incidence Rate Differences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Ying, Y.; Xie, H.; Li, J.; Wang, X.; He, L.; Jin, K.; Tang, J.; Xu, X.; Zheng, X. Secondhand smoking increases bladder cancer risk in nonsmoking population: A meta-analysis. Cancer Manag. Res. 2018, 10, 3781–3791. [Google Scholar] [CrossRef]
- American Cancer Society. Bladder Cancer Risk Factors. Available online: https://www.cancer.org/cancer/bladder-cancer/causes-risks-prevention/risk-factors.html#:~:text=People%20who%20smoke%20are%20at,227%2D2345%20for%20more%20information. (accessed on 9 November 2022).
- Svatek, R.S.; Hollenbeck, B.K.; Holmäng, S.; Lee, R.; Kim, S.P.; Stenzl, A.; Lotan, Y. The economics of bladder cancer: Costs and considerations of caring for this disease. Eur. Urol. 2014, 66, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.L. The etiology of bladder cancer. In Urologic Cancers; Barber, N., Ali, A., Eds.; Exon Publications: Brisbane, Australia, 2022. [Google Scholar]
- Baris, D.; Karagas, M.R.; Verrill, C.; Johnson, A.; Andrew, A.S.; Marsit, C.J.; Schwenn, M.; Colt, J.S.; Cherala, S.; Samanic, C.; et al. A case–Control study of smoking and bladder cancer risk: Emergent patterns over time. J. Natl. Cancer Inst. 2009, 101, 1553–1561. [Google Scholar] [CrossRef]
- Besaratinia, A.; Tommasi, S. Genotoxicity of tobacco smoke-derived aromatic amines and bladder cancer: Current state of knowledge and future research directions. FASEB J. 2013, 27, 2090–2100. [Google Scholar] [CrossRef] [PubMed]
- Pezzuto, A.; Citarella, F.; Croghan, I.; Tonini, G. The effects of cigarette smoking extracts on cell cycle and tumor spread: Novel evidence. Futur. Sci. OA 2019, 5, FSO394. [Google Scholar] [CrossRef]
- Tonini, G.; D’Onofrio, L.; Dell’Aquila, E.; Pezzuto, A. New molecular insights in tobacco-induced lung cancer. Futur. Oncol. 2013, 9, 649–655. [Google Scholar] [CrossRef]
- Zhao, X.; Wang, Y.; Liang, C. Cigarette smoking and risk of bladder cancer: A dose–response meta-analysis. Int. Urol. Nephrol. 2022, 54, 1169–1185. [Google Scholar] [CrossRef]
- van Osch, F.H.M.; Vlaanderen, J.; Jochems, S.H.J.; Bosetti, C.; Polesel, J.; Porru, S.; Carta, A.; Golka, K.; Jiang, X.; Stern, M.C.; et al. Modeling the complex exposure history of smoking in predicting bladder cancer: A pooled analysis of 15 case-control studies. Epidemiol. 2019, 30, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Masaoka, H.; Matsuo, K.; Oze, I.; Kimura, T.; Tamakoshi, A.; Sugawara, Y.; Tsuji, I.; Sawada, N.; Tsugane, S.; Ito, H.; et al. Cigarette smoking, smoking cessation and bladder cancer risk: A pooled analysis of ten cohort studies in Japan. J. Epidemiology 2022. [Google Scholar] [CrossRef]
- Ogihara, K.; Kikuchi, E.; Yuge, K.; Ito, Y.; Tanaka, N.; Matsumoto, K.; Miyajima, A.; Asakura, H.; Oya, M. Refraining from smoking for 15 years or more reduced the risk of tumor recurrence in non-muscle invasive bladder cancer patients. Ann. Surg. Oncol. 2015, 23, 1752–1759. [Google Scholar] [CrossRef]
- Fiore, M.C.; Jaén, C.R.; Baker, T.B.; Bailey, W.C.; Benowitz, n.L.; Curry, S.J.; Dorfman, S.F.; Froelicher, E.S.; Goldstein, M.G.; Healton, C.G.; et al. Treating Tobacco Use and Dependence: 2008 Update; U.S. Department of Health and Human Services Public Health Service: Washington, DC, USA, 2008. [Google Scholar]
- Curfman, G.D.; Morrissey, S.; Drazen, J.M. The FDA and tobacco regulation. N. Engl. J. Med. 2008, 359, 1056–1057. [Google Scholar] [CrossRef]
- Garrett, B.E.; Trosclair, A.; Caraballo, R.S.; Pechacek, T.F. Centers for Disease Control and Prevention (CDC). Cigarette smoking—United States, 1965–2008. MMWR Suppl. 2011, 109–113. Available online: https://www.cdc.gov/mmwr/pdf/other/su6001.pdf (accessed on 9 November 2022).
- Islami, F.; Torre, L.A.; Jemal, A. Global trends of lung cancer mortality and smoking prevalence. Transl. Lung Cancer Res. 2015, 4, 327–338. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention: National Center for Health Statistics (US). National Health Interview Survey. Available online: https://www.cdc.gov/nchs/nhis/data-questionnaires-documentation.htm (accessed on 18 January 2023).
- Pinney, J.M. United States. Public Health Service. Office of the Assistant Secretary for Health. Office on Smoking and Health. A Report of the Surgeon General: Appendix: Cigarette Smoking in the United States, 1950–1978. 1979, A-1–A-29. Available online: https://profiles.nlm.nih.gov/101584932X675 (accessed on 19 January 2023).
- Centers for Disease Control and Prevention. Morbidity and Mortality Weekly Reports (MMWR). Available online: https://www.cdc.gov/tobacco/data_statistics/mmwrs/index.htm (accessed on 19 January 2023).
- Cole, A.P.; Friedlander, D.F.; Trinh, Q.-D. Secondary data sources for health services research in urologic oncology. Urol. Oncol. 2018, 36, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Thun, M.; Peto, R.; Boreham, J.; Lopez, A.D. Stages of the cigarette epidemic on entering its second century. Tob. Control 2012, 21, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, D.; Hoffmann, I.; El-Bayoumy, K. The less harmful cigarette: A controversial issue. A tribute to Ernst L. Wynder. Chem. Res. Toxicol. 2001, 14, 767–790. [Google Scholar] [CrossRef]
- Lobo, N.; Afferi, L.; Moschini, M.; Mostafid, H.; Porten, S.; Psutka, S.P.; Gupta, S.; Smith, A.B.; Williams, S.B.; Lotan, Y. Epidemiology, screening, and prevention of bladder cancer. Eur. Urol. Oncol. 2022, 5, 628–639. [Google Scholar] [CrossRef] [PubMed]
- Freedman, N.D.; Silverman, D.T.; Hollenbeck, A.R.; Schatzkin, A.; Abnet, C.C. Association between smoking and risk of bladder cancer among men and women. JAMA 2011, 306, 737–745. [Google Scholar] [CrossRef]
- Bellamri, M.; Walmsley, S.J.; Brown, C.; Brandt, K.; Konorev, D.; Day, A.; Wu, C.-F.; Wu, M.T.; Turesky, R.J. DNA damage and oxidative stress of tobacco smoke condensate in human bladder epithelial cells. Chem. Res. Toxicol. 2022, 35, 1863–1880. [Google Scholar] [CrossRef]
- American Lung Association. State of Tobacco Control. Tobacco Control Milestones. Available online: https://www.lung.org/research/sotc/tobacco-timeline (accessed on 9 November 2022).
- Janisch, F.; Shariat, S.; Schernhammer, E.; Rink, M.; Fajkovic, H. The interaction of gender and smoking on bladder cancer risks. Curr. Opin. Urol. 2019, 29, 249–255. [Google Scholar] [CrossRef]
- Teoh, J.Y.-C.; Huang, J.; Ko, W.Y.-K.; Lok, V.; Choi, P.; Ng, C.-F.; Sengupta, S.; Mostafid, H.; Kamat, A.M.; Black, P.C.; et al. Global trends of bladder cancer incidence and mortality, and their associations with tobacco use and gross domestic product per capita. Eur. Urol. 2020, 78, 893–906. [Google Scholar] [CrossRef]
- Howard, J. Minimum Latency & Types or Categories of Cancer; Centers for Disease Control and Prevention; WTC Health Program: Atlanta, GA, USA, 2013; pp. 1–9. [Google Scholar]
- Castelao, J.E.; Yuan, J.-M.; Skipper, P.L.; Tannenbaum, S.R.; Gago-Dominguez, M.; Crowder, J.S.; Ross, R.K.; Yu, M.C. Gender- and smoking-related bladder cancer risk. Gynecol. Oncol. 2001, 93, 538–545. [Google Scholar] [CrossRef]
- Cumberbatch, M.G.; Rota, M.; Catto, J.W.; La Vecchia, C. The role of tobacco smoke in bladder and kidney carcinogenesis: A comparison of exposures and meta-analysis of incidence and mortality risks. Eur. Urol. 2016, 70, 458–466. [Google Scholar] [CrossRef]
- Division of Cancer Prevention and Control; Centers for Disease Control and Prevention. What Are the Risk Factors for Lung Cancer? Available online: https://www.cdc.gov/cancer/lung/basic_info/risk_factors.htm#:~:text=People%20who%20smoke%20cigarettes%20are,the%20risk%20of%20lung%20cancer (accessed on 22 December 2019).
- Surprising Link’: Smoking and Bladder Cancer. Available online: https://health.clevelandclinic.org/surprising-link-smoking-and-bladder-cancer-2/ (accessed on 18 January 2023).
- Marcus, P.M.; Hayes, R.; Vineis, P.; Garcia-Closas, M.; Caporaso, N.E.; Autrup, H.; Branch, R.A.; Brockmöller, J.; Ishizaki, T.; Karakaya, A.E.; et al. Cigarette smoking, n-acetyltransferase 2 acetylation status, and bladder cancer risk: A case-series meta-analysis of a gene-environment interaction. Cancer Epidemiol. Biomark. Prev. 2000, 9, 461–467. [Google Scholar]
- Burger, M.; Catto, J.W.F.; Dalbagni, G.; Grossman, H.B.; Herr, H.; Karakiewicz, P.; Kassouf, W.; Kiemeney, L.A.; La Vecchia, C.; Shariat, S.; et al. Epidemiology and risk factors of urothelial bladder cancer. Eur. Urol. 2013, 63, 234–241. [Google Scholar] [CrossRef]
- Baris, D.; Waddell, R.; Freeman, L.E.B.; Schwenn, M.; Colt, J.S.; Ayotte, J.D.; Ward, M.H.; Nuckols, J.; Schned, A.; Jackson, B.; et al. Elevated bladder cancer in northern New England: The role of drinking water and arsenic. J. Natl. Cancer Inst. 2016, 108, djw099. [Google Scholar] [CrossRef]
- Michaud, D.S.; Spiegelman, D.; Clinton, S.K.; Rimm, E.B.; Curhan, G.C.; Willett, W.C.; Giovannucci, E.L. Fluid intake and the risk of bladder cancer in men. N. Engl. J. Med. 1999, 340, 1390–1397. [Google Scholar] [CrossRef]
- Mullane, S.A.; Werner, L.; Rosenberg, J.; Signoretti, S.; Callea, M.; Choueiri, T.K.; Freeman, G.J.; Bellmunt, J. Correlation of apobec mrna expression with overall survival and pd-l1 expression in urothelial carcinoma. Sci. Rep. 2016, 6, 27702. [Google Scholar] [CrossRef] [PubMed]
- National Center for Chronic Disease; Health Promotion Office on Health. Reports of the surgeon general. In the Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; Centers for Disease Control and Prevention (US): Atlanta, GA, USA, 2014. [Google Scholar]
- National Cancer Institute. Surveillance, Epidemiology, and End Results Program. Race and Hispanic Ethnicity Changes. Available online: https://seer.cancer.gov/seerstat/variables/seer/race_ethnicity/ (accessed on 24 January 2023).
- Lyratzopoulos, G.; Abel, G.A.; McPhail, S.; Neal, R.D.; Rubin, G.P. Gender inequalities in the promptness of diagnosis of bladder and renal cancer after symptomatic presentation: Evidence from secondary analysis of an English primary care audit survey. BMJ Open 2013, 3, e002861. [Google Scholar] [CrossRef]
- Cohn, J.A.; Vekhter, B.; Lyttle, C.; Steinberg, G.D.; Large, M.C. Sex disparities in diagnosis of bladder cancer after initial presentation with hematuria: A nationwide claims-based investigation. Cancer 2013, 120, 555–561. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | Annual Percent Change | Incidence Rate Difference | R-Squared (%) | ||
|---|---|---|---|---|---|
| %; 95% CI (LB; UB) | p-Value | n, 95% CI (LB; UB) | p-Value | ||
| Overall | |||||
| Tobacco smoking prevalence | −0.22; (−0.29; −0.15) | <0.001 | - | - | - |
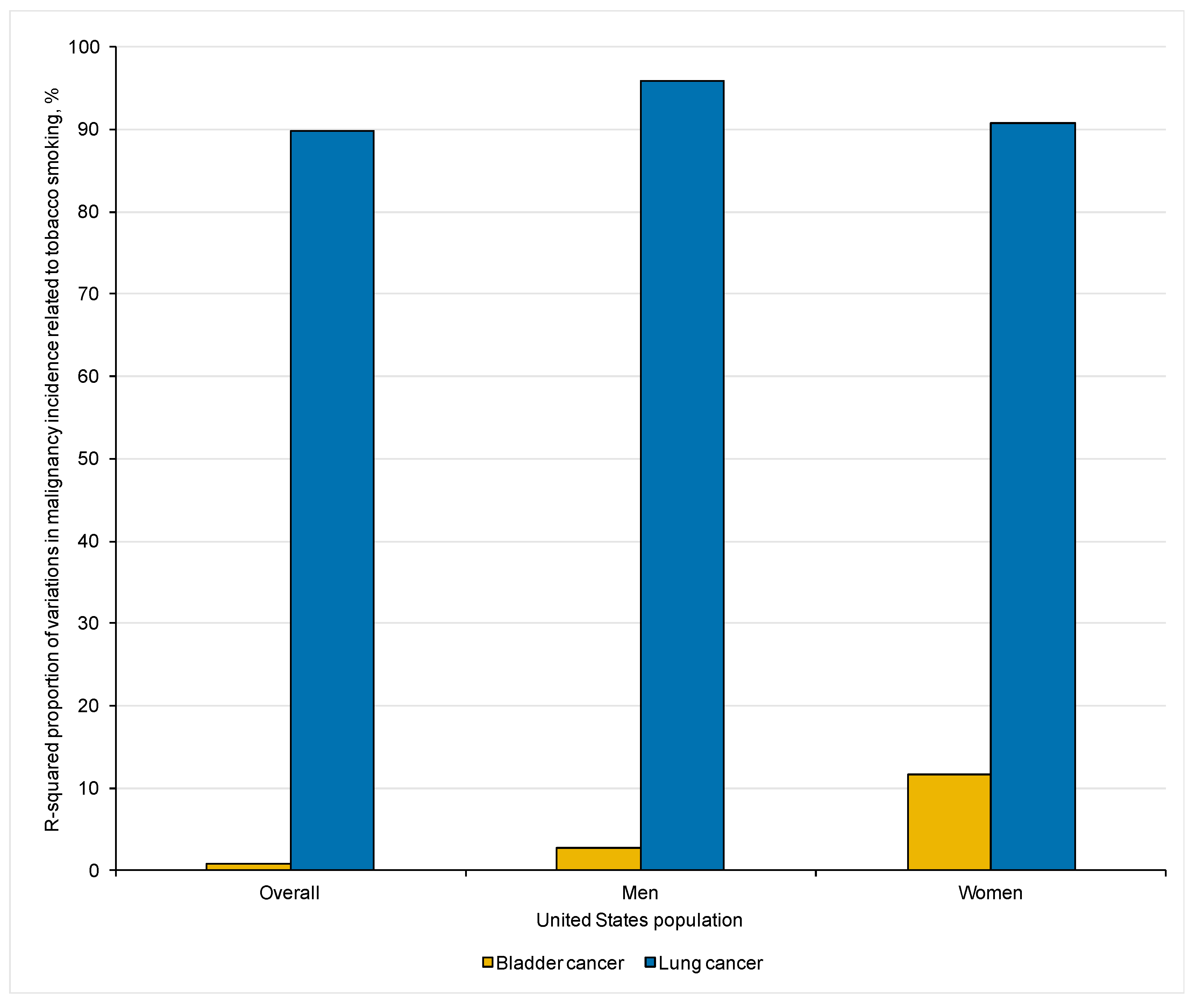
| Bladder cancer incidence | +0.04; (−0.07; +0.16) | 0.43 | +0.04, (−0.14; +0.22) | 0.631 | 0.81 |
| Lung cancer incidence | −0.61; (−0.79; −0.43) | <0.001 | +3.55, (+3.09 +4.00) | <0.001 | 89.72 |
| Men | |||||
| Tobacco smoking prevalence | −0.61; (−0.68; −0.54) | <0.001 | - | - | - |
| Bladder cancer incidence | −0.04; (−0.17; +0.08) | 0.49 | +0.07, (−0.09; +0.23) | 0.374 | 2.74 |
| Lung cancer incidence | −1.62; (−1.76; −1.49) | <0.001 | +4.82, (+4.44; +5.20) | <0.001 | 95.80 |
| Women | |||||
| Tobacco smoking prevalence | +0.18; (+0.09; +0.27) | <0.001 | - | - | - |
| Bladder cancer incidence | −0.18; (−0.33; −0.002) | 0.03 | +0.12, (−0.01; +0.25) | 0.061 | 11.59 |
| Lung cancer incidence | +0.59; (+0.31; +0.88) | <0.001 | +3.55, (+3.12; +3.99) | <0.001 | 90.69 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seisen, T.; Labban, M.; Lipsitz, S.R.; Preston, M.A.; Mossanen, M.; Bellmunt, J.; Rouprêt, M.; Choueiri, T.K.; Kibel, A.S.; Sun, M.; et al. Assessment of the Ecological Association between Tobacco Smoking Exposure and Bladder Cancer Incidence over the Past Half-Century in the United States. Curr. Oncol. 2023, 30, 1986-1998. https://doi.org/10.3390/curroncol30020154
Seisen T, Labban M, Lipsitz SR, Preston MA, Mossanen M, Bellmunt J, Rouprêt M, Choueiri TK, Kibel AS, Sun M, et al. Assessment of the Ecological Association between Tobacco Smoking Exposure and Bladder Cancer Incidence over the Past Half-Century in the United States. Current Oncology. 2023; 30(2):1986-1998. https://doi.org/10.3390/curroncol30020154
Chicago/Turabian StyleSeisen, Thomas, Muhieddine Labban, Stuart R. Lipsitz, Mark A. Preston, Matthew Mossanen, Joaquim Bellmunt, Morgan Rouprêt, Toni K. Choueiri, Adam S. Kibel, Maxine Sun, and et al. 2023. "Assessment of the Ecological Association between Tobacco Smoking Exposure and Bladder Cancer Incidence over the Past Half-Century in the United States" Current Oncology 30, no. 2: 1986-1998. https://doi.org/10.3390/curroncol30020154