

Human Health Effects of Oral Exposure to Chromium: A Systematic Review of the Epidemiological Evidence

Abstract
:1. Introduction
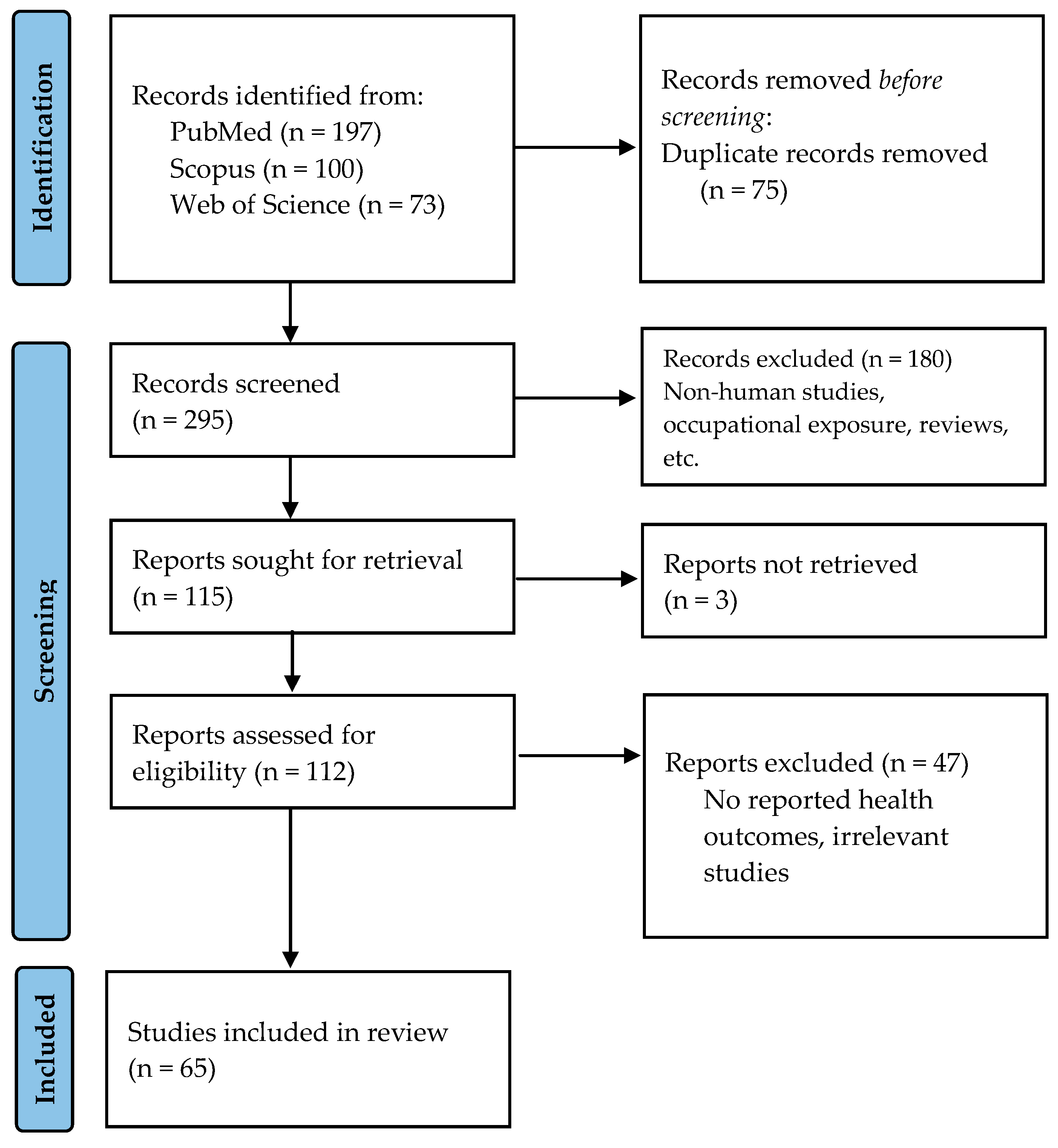
2. Methodology
2.1. Study Eligibility
2.2. Literature Search
3. Results
3.1. Oral Exposure to Chromium and Health Effects on the General Population
3.2. Associations of Cr Biomarkers and Adverse Health Effects during Lifetime
3.2.1. Prenatal Cr Exposure and Fetal Development

{kind=link}
| Study Characteristics (Area, Time, Population) | Study Design | Exposure Levels | Key Findings of Health Outcomes | Ref. |
|---|---|---|---|---|
| China, Jinzhou area, 1970–1978 | Ecological mortality | Drinking water Cr(VI): up to 20,000 μg/L | Malignant tumor mortality rates: 71.89–92.66/100,000 vs. 65.40/100,000 (control) | [22] |
| China, Jinzhou area, 1965–1978 | Ecological mortality | Average Cr(VI) well-water concentration <0.001–20.0 mg/L | All cancer deaths: RR = 1.13, (95% CI: 0.86, 1.46) Stomach cancer deaths: RR = 1.82, (95% CI: 1.11, 2.91) Lung cancer deaths: RR = 1.15, (95% CI: 0.62, 2.07) | [24] |
| China, Jinzhou area, 1965–1978 | Ecological mortality | Average Cr(VI) well-water concentration 0.004–10.5 mg/L | All cancer deaths: RR = 1.10, (95% CI: 0.80, 1.51) Stomach cancer deaths: RR = 1.22, (95% CI: 0.74, 2.01) Lung cancer deaths: RR = 1.76, (95% CI: 0.78, 3.98) | [25] |
| China, Liaoning province, villages of Jinzhou city 2016 626 adults: 319 exposed 307 non-exposed | Cross-sectional | Cr in groundwater: 0.002–2.5 mg/L Cr in soil: 20.1–417.1 mg/kg Cr in air: 5.0–82.9 ng/m3 Exposure surrogate: duration of residence | MDA: β = 0.32, p = 0.0001 CAT: β = 1.60, p < 0.0001/increase with length of residence for age <18 at first exposure SOD: β = −14.73, p < 0.0001 GSH-Px: β = 45.66, p < 0.0001/increase with length of residence for age >18 at first exposure 8-OHdG (log): β = 0.09, p = 0.0075/increase with length of residence for age <18 at first exposure | [27] |
| India, Pradesh Uttar, Kanpur 186 exposed 230 non-exposed | Cross-sectional retrospective | Drinking water Cr(VI): 20,000 μg/L | Gastrointestinal symptoms: OR = 3.1, (95% CI: 1.50, 6.39) (men), OR = 2.44, (95% CI: 1.32, 4.52) (women) Skin symptoms: OR= 3.5 (95% CI 1.41, 8.58) (men), OR = 6.57, (95% CI 2.64, 16.32) (women) Ocular complaints: OR= 3.5 (95% CI 1.22, 9.79) (men) Urinary complaints: OR= 3.1 (95% CI 1.08, 8.87) (women) | [28] |
| India, Pradesh Uttar, Kanpur 143 exposed 70 non-exposed | Cross-sectional retrospective | Drinking water Cr(VI): 20,000 μg/L | RBC count: 5.55 ± 1.39 (exposed men) vs. 4.28 ± 0.69 (control men), p < 0.001 RBC count: 5.67 ± 1.26 (exposed women) vs. 3.89 ± 0.71 (control women), p < 0.001 MCV: 78.56 ± 9.18 (exposed men) vs. 85.38 ± 7.89 (control men), p < 0.001 PLT: 116.2 ± 42.9 (exposed men) vs. 190.3 ± 59.3 (control men), p < 0.001 PLT: 120.2 ± 56.5 (exposed women) vs. 228.4 ± 76.9 (control women), p < 0.001 No association with total leucocyte count | [28] |
| Greece, Voiotia prefecture 2012–2014 122 currently exposed 115 exposed in past 67 non-exposed | Cross-sectional retrospective | Lifetime Cr exposure dose: 3738.0 μg/kg BW (range: 26.1–21,574.7) (currently exposed) Lifetime Cr exposure dose: 1654.6 μg/kg BW (range: 8.6–29,281.1) (exposed in the past) Lifetime Cr exposure dose: 307.1 μg/kg BW (range: 54.0–3736.7) (non-exposed) | Significant associations with Cr exposure dose (ln) Cr-B: β = 0.134, p = 0.023/Cr-H(ln): β = 0.226, p < 0.001 SBP: β = 0.142, p = 0.010/DBP: β = 0.116, p = 0.042 Hb: β = −0.093, p = 0.041/hematocrit: β = −0.094, p = 0.048 TG(ln): β = 0.144, p = 0.009/HDL: β = −0.113, p = 0.034 Sodium: β = −0.145, p = 0.011/Calcium: β = 0.117, p = 0.044 Alkaline phosphatase: β = 0.120, p = 0.035 Amylase: β = 0.159, p = 0.005 Albumin: β = 0.213, p < 0.001/TP: β = 0.144, p = 0.012 IL-12 (ln): β = 0.308, p = 0.012 | [29] |
| Greece, Voiotia, Oinofyta 2010–2011 1181 exposed (1/3 of the total population) | Morbidity Cohort | Exposure surrogate: duration of residence Mean: 17.6 years of residence | Lower urinary tract symptoms: OR = 1.11, p = 0.050 in men Urogenital infections: OR = 1.91, p = 0.049 for >15 years residence | [30] |
| Greece, Voiotia, Oinofyta 1999–2009 5842 exposed | Ecological mortality | Drinking water Cr(VI): range 8–156 μg/L (N = 106) | Primary liver cancer: SMR= 11.04, (95% CI: 4.05, 24.03) Kidney and genitourinary organ cancers: SMR= 3.68, (95% CI: 1.19, 8.58) in women Lung cancer: SMR= 1.45, (95% CI 1.01, 2.03) | [31] |
| USA, California, Kettleman, Hinkley, Topock 1989–1998 No data on persons at risk | Ecological mortality | No data about Cr(VI) concentrations or duration of exposure | Lung cancer deaths: RR = 1.03, (95% CI: 0.90, 1.17) All cancer deaths: RR = 0.93, (95% CI: 0.87, 1.00) All deaths: RR = 0.98, (95% CI: 0.95, 1.02) | [33] |
3.2.2. Cr Exposure during Pregnancy and Health Outcomes in the Mother
3.2.3. Cr Exposure and Health Outcomes in Childhood
| Study Characteristics (Area, Time, Population) | Study Design | Exposure Variables | Biomonitoring Data [(Mean ± SD) or Median] | Key Findings of Health Outcomes | Ref. |
|---|---|---|---|---|---|
| Prenatal exposure | |||||
| China, Hubei province 2012–2014 204 LBW cases 312 controls | Case control | Cr in maternal urine | Cr-U: 4.57 μg/g creatinine (range: 0.02–57.44 μg/g) (cases) Cr-U: 3.33 μg/g creatinine (range: 0.02–87.35 μg/g) (controls) | LBW risk OR = 1.77 (medium tertile), (95% CI: 0.95, 3.29) OR = 2.48 (highest tertile), (95% CI: 1.33, 4.61) | [36] |
| China, Wuhan 2014–2015 734 mother-infant pairs | Birth cohort | 16 metals in umbilical cord serum (U, Cu, Pb, Se, Ba, Tl, Mn, Ni, Sr, As, Zn, Cd, V, Cr, Al, Co) | Cr-S: 10.4 μg/L (P25 6.45 μg/L, P75 16.3 μg/L) | Birth weight: no association Β = −0.02 (95% CI: −0.07, 0.03) per unit increase in lnCr | [37] |
| Israel 2016 975 mother-infant pairs | Cross-sectional | 8 metals in maternal urine (As, Cd, Cr, Hg, Ni, Pb, Se, Tl) | Cr-U: 0.28 μg/g creatinine (P25 0.17 μg/g, P75 0.49 μg/g) | Birth weight: β = −0.120 SD (95% CI: −0.202, −0.037) Birth length: β = −0.133 SD (95% CI: −0.215, −0.05) per one-IQR increase in logCr-U | [38] |
| Canary Islands, Spain 2016 471 mothers | Cross-sectional | 44 metals in cord blood (Ag, As, Au, Ba, Be, Bi, Cd, Ce, Cr, Cu, Dy, Eu, Er, Ga, Gd, Hg, Ho, In, La, Lu, Nb, Nd, Ni, Os, Pb, Pd, Pr, Pt, Ru, Sb, Se, Sm, Sn, Sr, Ta, Tb, Th, Tl, Tm, U, V, Y, Yb, Zn) | Cr-B: 1.10 ± 0.66 μg/L | Birth weight: no significant association When birth weight dichotomized at the P10, the sum of Cr, Ni, and Sb appeared as a risk factor for birth weight (OR = 3.84; 95% CI = 1.42, 10.39) in the multivariate analysis | [39] |
| Spain (5 counties) 2000–2008 327 mother–infant pairs | Birth cohort | 6 metals in placenta (Cd, Pb, Mn, Cr, As, Hg) | Cr-placenta: 80.50 ng/g (P25 46.50 ng/g, P75 111.9 ng/g) | Birth length: β = −0.68 cm, (95% CI: −1.33, −0.04), for Cr in the high vs. low tertile (>99.6 vs. <56.1 ng/g). Gestational age: β = 0.56 weeks, 95% CI: 0.16, 0.97), for Cr in the middle vs. low tertile (56.1–99.6 vs. <56.1 ng/g) | [40] |
| China, Wuhan 2013–2016 3041 pregnant women | Birth cohort | Cr in maternal urine at 1st, 2nd, and 3rd trimesters | Cr-U: 0.98 μg/L (specific gravity-adjusted) (range: 0.61–1.75 μg/L) | 1st trimester: AC: −5.4% (95% CI: −9.6%, −1.2%), EFW: −5.6% (95% CI: −9.8%, −1.4%), ponderal index: −0.11 kg/m3 (95% CI: −0.19, −0.03), per unit increase in lnCr 2nd trimester: AC: −7.0% (95% CI: −12.5%, −1.4%) EFW: −5.0% (95% CI: −10.6%, 0.6%) ponderal index: −0.15 kg/m3 (95% CI: −0.27, −0.03) per unit increase in lnCr | [41] |
| China 2014–2017 1275 mother-infant pairs | Birth cohort | 8 metals in maternal urine (Pb, Cd, Hg, As, Cr, V, Tl, Ba) | Cr-U: 0.75 μg/L (specific gravity-adjusted) (P25 0.43 μg/L, P75 1.24 μg/L) | EFW: β = −0.06 (95% CI: −0.12, 0.00) at 34–36 weeks of gestation Metal mixture: effect on EFW βWQS= −0.05 (95% CI: −0.09, −0.01), mainly driven by Cr (30.41%) at 34–36 weeks of gestation | [42] |
| China 2009–2013 147 SBP cases 381 controls | Nested case control | 5 metals in maternal serum (As, Cd, Cr, Hg, Pb) | Cr-S: 0.275 μg/L (P25 0.196 μg/L, P75 0.417 μg/L) (no difference in cases and controls) | Spontaneous preterm birth (SBP): no association OR = 1.27 (95% CI: 0.84, 1.91) | [43] |
| China, Hubei 2012–2014 7290 pregnant women | Birth cohort | Cr in maternal urine | Cr-U: 1.86 μg/g creatinine (P25 0.86 μg/g, P75 5.65 μg/g) Cr-U: 1.01 μg/L (P25 0.61 μg/L, P75 2.09 μg/L) | Gestational age (days): β = −0.68 (95% CI: −0.88, −0.48) for continuous ln-Cr-U Risk for preterm birth: OR = 1.55 (95% CI: 0.99, 2.42) for the medium tertile vs low tertile of Cr-U OR = 1.89 (95% CI: 1.13, 3.18) for the high vs low tertile of Cr-U | [44] |
| China, Wuhan 2012–2014 5408 pregnant women of which 554 with PROM, 88 with preterm PROM | Birth cohort | Cr in maternal urine | Cr-U: 1.31 μg/g creatinine (P25 0.75 μg/g, P75 3.04 μg/g) (all) Cr-U: 2.39 μg/g creatinine (P25 1.13, P75 6.09) (PROM women) Cr-U: 4.37 μg/g creatinine (P25 1.72, P75 10.45) (preterm PROM women) | OR = 1.47 (95% CI: 1.36, 1.58) for one-unit increase in ln-Cr Risk for PROM: OR = 1.42 (95% CI: 1.09, 1.84) for the medium tertile; OR = 2.77 (95% CI: 2.18, 3.52) for the high vs low tertile of Cr-U Risk for preterm PROM: OR = 2.81 (95% CI: 0.92, 8.60) for the medium tertile vs low tertile of Cr-U OR = 4.54 (95% CI: 1.58, 13.06) for the high vs low tertile of Cr-U Higher associations in boys | [45] |
| Northern China 2003–2016 273 NTD cases 477 controls | Nested case control | 10 metals in maternal blood (Cd, Co, Cr, Cu, Fe, Hg, Mn, Mo, Pb, Zn) | Cr-B: 1.06 μg/L (P25 0.85, P75 1.81) (cases) Cr-B: 1.01 μg/L (P25 0.80, P75 1.38) (controls) | Neural tube defects (NTDs): no association | [46] |
| China 2012–2013 112 infants with CHD 107 controls | Case control | 6 metals in maternal blood (Pb, Cd, Cr, Cu, Hg, Se) | Cr-B: 3.63 μg/L (P25 2.09, P75 4.10) (cases) Cr-B: 3.57 μg/L (P25 3.27, P75 3.99) (controls) p = 0.160 | Congenital heart defects (CHDs): no association OR = 0.24 (95% CI: 0.08, 1.69) for the middle tertile of Cr-B (3.40–3.79 μg/L) vs low tertile (<3.40 μg/L) OR = 0.84 (95% CI: 0.36, 1.96) for the high tertile of Cr-B (>3.79 μg/L) vs low tertile (<3.40 μg/L) (multivariable multi-element logistic regression model) | [47] |
| China 174 children with CS 85 controls | Case control | 6 metals in child’s serum (Cr, Ni, Sn, As, Tl, Pb) | Cr-S: 2.10 μg/L (IQR range 18.10) (cases) Cr-S: 1.17 μg/L (IQR range: 0.53) (controls) | Craniosynostosis (CS): no association OR = 0.24 (95% CI: −0.59, 1.07) for Q2 vs Q1 OR = 0.81 (95% CI: −0.09, 1.72) for Q3 vs Q1 OR = 2.24 (95% CI: −0.13, 4.62) for Q4 vs Q1 | [48] |
| China, Wuhan 2013–2016 628 mother-infant pairs | Birth cohort | 7 metals in maternal urine at 1st, 2nd, 3rd trimesters (V, Cr, Ni, As, Cd, Tl, Pb) | Cr-U: 1.18 μg/g creatinine (P25 0.72 μg/g, P75 2.04 μg/g) | Allergic rhinitis in childhood: OR = 1.41 (95% CI: 1.02, 1.95) with Cr-U at 3rd trimester (logistic regression)/(+) effect in BKMR (+) trend with wheeze and eczema in BKMR | [49] |
| Palestine 2014 502 pregnant women 392 followed up in 6 months | Birth cohort | 5 metals in maternal hair (Cr, Hg, V, Sr, U) | Cr-H: 0.97 ± 0.99 μg/g (range: 0.07–7.52 μg/g) | Child’s positive affectivity: β = −0.13, p = 0.013 Not modified by maternal post-traumatic stress | [50] |
| During pregnancy | |||||
| USA, Boston/New York 2011 380 pregnant women | Cohort | 6 metals in urine (Ba, Cd, Cr, Cs, Pb, Sb) | Cr-U: 0.62 μg/L (P25: 0.47 μg/L, P75: 0.83 μg/L) | Anxiety score during pregnancy: 5.7% (95% CI: 23.9%, 95.7%) increase in the odds of higher anxiety score, per one-quintile increase in the WQS index Top three contributing metals: Cd (61.8%), Cr (14.7%), and Cs (12.7%) | [51] |
| China, Wuhan 2013–2016 305 GDM cases 305 controls | Nested case control | 7 metals in plasma (Mg, Zn, Ca, Fe, Cu, Se, Cr) | Cr-P: 2.65 μg/L (P25: 1.26 μg/L, P75: 5.74 μg/L) (cases) Cr-P: 3.20 μg/L (P25: 1.53 μg/L, P75: 5.80 μg/L) (controls) | Gestational diabetes mellitus: no association OR = 0.93 (95% CI: 0.71, 1.22) per IQR increment | [53] |
| USA, Boston 2006–2008 28 preeclamptic 355 non-preeclamptic | Nested case control | 17 metals in urine (As, Ba, Be, Cd, Cu, Cr, Hg, Mn, Mo, Ni, Pb, Se, Sn, Tl, U, W, Zn) | Cr-U: detected in 7 preeclamptic and in 50 non-preeclamptic | Pre-eclampsia risk: association with detection of Cr-U HR = 3.48, (95% CI: 1.02, 11.8) (limited number of observations) | [54] |
| During childhood | |||||
| China, Hubei 2019 1220 children aged 2–6 years old | Cross-sectional | 23 metals in urine (Al, Ti, V, Cr, Mn, Fe, Co, Ni, Cu, Zn, As, Se, Rb, Sr, Mo, Cd, Sn, Sb, Ba, W, Tl, Pb, U) | Cr-U: 0.59 μg/L (P25 0.35 μg/L, P75 0.94 μg/L) (hypertensive) Cr-U: 0.71 μg/L (P25 0.42 μg/L, P75 1.68 μg/L) (normotensive) | SBP: β = −0.96 (95% CI: −1.87, −0.04) DBP: β = −0.92 (95% CI: −1.83, −0.02) Hypertension risk: β = 0.75 (95% CI: 0.55, 1.02) | [56] |
| West Kazakhstan 632 exposed children aged 7–17 years 621 unexposed children | Cross-sectional | 5 metals in blood (Cr, Mn, Ni, Pb, Cu) | Cr-B: 1.8 μg/L ± 0.36 μg/L (exposed) Cr-B: 0.385 ± 0.18 μg/L (unexposed) | Short stature: OR = 3.578 imbalance of hormones in exposed children: decrease in T3, T4, TSH, gonadotropins (affects sexual development and puberty), STH, IGF-1 in the pre- and pubertal periods | [57] |
| Southern Spain 2010, 2012 393 children, aged 6–11 | Cross-sectional | Cr in urine and hair | Cr-U: median 0.48 μg/L (0.96 μg/g creatinine), max: 21.0 μg/L (21.66 μg/g creatinine) Cr-H: median 0.32 μg/g, max 9.58 μg/g | For Cr-U Full-scale IQ: β = −5.99 (95% CI: −11.9, −0.02) in boys only Percentage of false alarms: β = −0.05 (95% CI: −0.09, −0.01) in boys Percentage of omissions β = 0.03 (95% CI: 0.00, 0.05) in boys Latency in reaction time test: β = 36.90 (95% CI: 3.50, 70.30) in girls Latency in reaction time test: β = 68.35 (95% CI: 6.60, 130.12) in boys For Cr-H Response latency in selective attention test: β = −55.01 (95% CI: −74.04, −35.96) in both sexes | [58] |
| Peru 2016, 2018 78 exposed children, average 10 years old 16 unexposed | Longitudinal | 21 metals in hair (Al, Sb, As, B, Ba, Be, Cd, Co, Cr, Fe, Mn, Hg, Mo, Ni, Pb, Cu, Se, Sn, Tl, V, Zn) | Cr-H: 0.83 μg/g in roots, 1.61 μg/g in tips (exposed) Cr-H: 0.39 μg/g in roots, 0.88 μg/g in tips (unexposed) | White lines on nails: χ2 test, p = 0.002 | [60] |
3.2.4. Cr Exposure and Health Effects during Adulthood
- Chromium and hypertension
- Chromium and cardiovascular system
- Cr and hematological/biochemical parameters (liver function and oxidative stress)
- Cr and obesity
- Cr and renal system
| Study Characteristics (Area, Time, Population) | Study Design | Exposure Variables | Biomonitoring Data [(Mean± SD) or Median] | Key Findings on Health Outcomes | Ref. | |
|---|---|---|---|---|---|---|
| Hypertension | ||||||
| China, 31 provinces 2017–2018 11,037 adults | Cross-sectional | 13 metals in blood and urine (Sb, As, Cd, Pb, Hg, Tl, Cr, Co, Mn, Mo, Ni, Se, Sn) | Cr-B = 0.42 μg/L (P25: 0.16 μg/L, P75: 0.81 μg/L) Cr-U = 0.57 μg/L (P25: 0.28 μg/L, P75: 1.12 μg/L) | No association with hypertension, pre-hypertension, or blood pressure Hypertension: OR = 0.90 (95% CI: 0.63, 1.29) for Cr-B high vs low quartile, OR = 0.98 (95% CI: 0.75, 1.28) for Cr-U high vs low quartile. Pre-hypertension: OR = 0.87 (95% CI: 0.66, 1.17) for Cr-B high vs low quartile, OR = 0.94 (95% CI: 0.74, 1.19) for Cr-U high vs low quartile. | [61] | |
| Cardiovascular disease | ||||||
| China, Guangzhou 2021 69 CHD patients 147 controls | Case control | 10 metals in urine (Cr, Fe, Co, Ni, Cu, As, Se, Cd, Sn, Hg) | Cr-U = 0.50 μg/L (P25: 0.34 μg/L, P75: 0.74 μg/L) (patients) Cr-U = 0.80 μg/L (P25: 0.58 μg/L, P75: 1.18 μg/L) (controls) | CHD: OR= 0.431 (95% CI: 0.151, 1.229) SBP: Spearman’s r = −0.192, p = 0.017 Glycated HbA1c: Spearman’s r = −0.241, p = 0.001 Fasting blood-glucose: Spearman’s r = −0.190, p = 0.022 HDL: Spearman’s r = 0.149, p = 0.032 Total Cholesterol: Spearman’s r = 0.150, p = 0.031 AST: Spearman’s r = 0.164, p = 0.032 | [62] | |
| China, Wuhan 2011 2004 adults, aged 18–80 | Cross-sectional | 23 metals in urine (Al, Ti, V, Cr, Mn, Fe, Co, Ni, Cu, Zn, As, Se, Rb, Sr, Mo, Cd, Sn, Sb, Ba, W, Tl, Pb, U) | Cr-U: 1.46 μg/L (P25: 0.93 μg/L, P75: 2.24 μg/L) | No association with heart rate variability (estimators not mentioned) | [64] | |
| Hematological/biochemical | ||||||
| Greece, Voiotia prefecture 2012–2014 122 currently exposed 115 exposed in past 67 non-exposed | Cross-sectional retrospective | Cr in blood Cr in hair | Cr-B 0.32 μg/L (range: <0.18–0.92 μg/L) (no difference) Cr-H: 0.31 μg/g (P25: 0.21 μg/g, P75: 0.46 μg/g) (currently exposed) Cr-H: 0.12 μg/g (P25: 0.07 μg/g, P75: 0.29 μg/g) (exposed in past) Cr-H: 0.22 μg/g (P25: 0.13 μg/g, P75: 0.32 μg/g) (non-exposed) | Signif. associations with Cr-B Glu(ln): β = 0.248, p < 0.001 Urea: β = −0.143, p = 0.012 Potassium: β = 0.120, p = 0.038 Alkaline phosphatase: β = 0.216, p < 0.001 γ-GT: β = 0.109, p = 0.041 LDH: β = 0.123, p = 0.033 Amylase: β = 0.177, p = 0.002 Albumin: β = 0.232, p < 0.001 TP: β = 0.237, p < 0.001 Calcium: β = 0.219, p < 0.001 | Signif. associations with Cr-H(ln) Hematocrit: β = −0.099, p = 0.041 PLT: β = −0.202, p < 0.001 Platelecrit: β = −0.229, p < 0.001 MCHC: β = −0.191, p = 0.001 RBC-DW: β = −0.191, p = 0.001 Glu(ln): β = 0.193, p = 0.001 TC: β = 0.268, p < 0.001 LDL: β = 0.216, p < 0.001 Alkaline phosphatase: β = 0.131, p = 0.026 LDH: β = 0.175, p = 0.003 Amylase: β = 0.262, p < 0.001 Albumin: β = 0.164, p = 0.005 TP: β = 0.376, p < 0.001 Calcium: β = 0.321, p < 0.001 Phosphate: β = 0.121, p = 0.041 Potassium: β = 0.127, p = 0.033 Sodium: β = −0.142, p = 0.018 | [29] |
| China, Liaoning Province, Jinzhou City 2016–2018 1171 adults: 364 exposed, 807 non-exposed | Cross-sectional | 4 metals in urine (Cr, Cd, Pb, Mn) | Cr-U: 4.67 μg/L (P25: 3.05 μg/L, P75: 6.01 μg/L) (exposed) Cr-U: 4.22 μg/L (P25: 1.74 μg/L, P75: 5.55 μg/L) (non-exposed) | Total protein: β = −0.57 (95% CI: −0.89, −0.26) with GLM/ PIP for Cr = 0.91 with BKMR ALB: β = −0.27, (95% CI: −0.47, −0.07)/PIP for Cr = 1.00 with BKMR ALT: β = 0.63 (95% CI: −0.02, 1.28) with GLM / weight of Cr = 0.38 with quantile g-computation AST: β = 0.24 (95% CI: −0.22, 0.71) with GLM / weight of Cr = −0.83 with quantile g-computation | [65] | |
| China, Liaoning province, Jinzhou city 2017–2019 1121 older adults (mean: 62.4 ± 10.6 years) 433 exposed 688 non-exposed | Cross-sectional | 4 metals in urine (Cr, Cd, Pb, Mn) | Cr-U: 4.02 μg/L (P25: 2.64 μg/L, P75: 5.28 μg/L) (exposed) Cr-U: 3.88 μg/L (P25: 2.74 μg/L, P75: 5.17 μg/L) (non-exposed) | HDL: β = 0.001 (95% CI: −0.03, 0.02) with GLM/(−) association with BKMR LDL: β = 0.02 (95% CI: −0.01, 0.04) with GLM/(+) association with BKMR Triglycerides: β = 0.01 (95% CI: −0.01, 0.03) with GLM Total Cholesterol: β = 0.01 (95% CI: −0.02, 0.03)/(+) association with BKMR | [66] | |
| China, Liaoning province, Jinzhou city 2016 585 adults: 282 exposed 303 non-exposed | Cross-sectional | Cr, Pb, Mn in blood | Cr-B= 0.92 μg/L (P25: 0.83 μg/L, P75: 1.02 μg/L) (exposed) Cr-B= 0.88 μg/L (P25: 0.80 μg/L, P75: 0.99 μg/L) (non-exposed) | RBC: β = 0.16 (95% CI: −0.0004, 0.33) Hb: β = 8.52 (95% CI: 3.10, 13.95) TC: β = −0.08 (95% CI: −0.45, 0.29) LDL: β = −0.08 (95% CI: −0.38, 0.22) SOD: (−) exposure–response relationship, p for trend = 0.017 | [67] | |
| China, rural northwest 2018–2019 785 adults | Cross-sectional | Cr, Co, Cd, Pb in serum | Cr-S: 2.05 μg/L (P25: 0.68 μg/L, P75: 4.98 μg/L) | AST: β = −0.099 (95% CI: −0.035, −0.003) ALT: β = −0.070 (95% CI: −0.043, 0.000) (single-metal model) | [68] | |
| China, Wuhan city and Zhuhai city 2012–2015 3762 adults, 18–80 years old (in 2012, for cross-sectional) Follow-up: 1750 adults for 3 years | Cohort and cross-sectional | Cr in urine | Cr-U: 1.60 µg/L (0.13 μg/mmol creatinine, P25: 0.08, P75: 0.21) | TG: β = −0.25 mmol/L (95% CI: −0.38, −0.11) per 1-unit increase of logCr-U TC: β = −0.05 (95% CI: −0.19, 0.09) per one-unit increase of logCr-U LDL: β = −0.06 (95% CI: −0.16, 0.04) per one-unit increase of logCr-U HDL: β = 0.05 (95% CI: 0.005, 0.10) per one-unit increase of logCr-U | [69] | |
| China, Beijing 2016 275 adults, 68.9 median age | Cross-sectional | 15 metals in urine (Al, Cr, Mn, Fe, Co, Ni, Cu, Zn, As, Se, Sr, Cd, Cs, Ba, Pb). | Cr-U: 0.268 μg/g creatinine (P25: 0.189 μg/g, P75: 0.381 μg/g) | Fasting plasma Glu: β = 0.024 (95% CI: −0.033, 0.081) with GLM Fasting plasma Glu: no association with BKMR | [70] | |
| Pakistan, 4 areas (control, low, medium, high risk of exposure) 48 children and adults: 12 from each area | Cross-sectional | 9 metals in blood, urine, hair, nails (Cd, Cr, Pb, Cu, Ni, Co, Mn, Fe, Zn) | Cr-B: mean values: 0.07 (control area)–0.27 (medium risk) Cr-U: mean values: 0.18 (control area)–0.62 (low risk) Cr-H mean values: 0.25 (control area)–0.59 (medium risk) Cr-Nails mean values: 0.34 (control area)–0.56 (medium risk) | GSH-Px: Spearman’s r = −0.315, p = 0.035 | [71] | |
| India, rural south 2015 847 adults, 715 possibly exposed | Cross-sectional | 8 metals in urine (Cd, As, Pb, Cr, Al, Zn, Cu, Ni) | Diabetes: OD = 1.05 (95% CI: 0.58, 2.02) for Q2 vs. Q1 OD = 1.87 (95% CI: 0.99, 3.51) for Q3 vs. Q1 OD = 2.40 (95% CI: 1.26, 4.56) for Q4 vs. Q1 Glycated HbA1c: Spearman’s r = 0.12, p < 0.01 No correlation with SBP, DBP, BMI, TC, LDL (Spearman’s r) | [72] | ||
| South Korea 2012–2013 500 adults, aged >35 | Cross-sectional | Cr-Toenail: range 0.003–5.76 μg/g | Fasting Glu, SPB, DBP, TG, HDL, waist circumference: No association (ptrend > 0.050) | [55] | ||
| Spain 2013 1440 adults | Cross-sectional | 9 metals in urine (Sb, Ba, Cd, Cr, Co, Cu, Mo, V, Zn) | Cr-U= 3.5 μg/g (P25: 2.2 μg/g, P75: 5.8 μg/g) | GSSG/GSH: Geometric mean ratios = 1.23 (95% CI: 1.04, 1.46) (P80 vs. P20)/non-linear (+) relation of Cr with GSSG/GSH with BKMR MDA and 8-OHdG: No association with Cr-U | [73] | |
| USA 1999–2010 28,539 adults | Cohort | Consumption of Cr-dietary supplement | Risk of diabetes and/or HbA1c ≥ 6.5% OR = 0.81 (95% CI: 0.71, 0.91) for Cr supplement use OR = 0.83 (95% CI: 0.72, 0.96) for ≥ 2000 mg Cr/30 d than no supplement OR = 0.78 (95% CI: 0.66, 0.92) for < 2000 mg Cr/30 d than no supplement | [74] | ||
| USA 1999–2016 1237 women, aged 45–56 | Cohort | 20 metals in urine (As, Ba, Be, Cd, Co, Cr, Cs, Cu, Hg, Mn, Mo, Ni, Pb, Sb, Sn, Tl, U, V, W, Zn) | Cr-U median < 0.4 μg/L Cr > 0.4 μg/L in 24.3% of the population | Incident diabetes: HR = 0.71 (95% CI: 0.50, 1.01) for those with Cr > LOD compared to those with Cr < LOD | [75] | |
| Obesity | ||||||
| China, Liaoning province, Jinzhou City 2017–2019 1187 adults: 349 exposed 838 non-exposed | Cross-sectional | 4 metals in urine (Cr, Cd, Pb, Mn) | Cr-U: 3.48 μg/L (P25: 1.84 μg/L, P75: 4.93 μg/L) | BMI: ptrend = 0.023 (linear regression with quartiles of Cr-U) Positive association below Cr-U median and negative above Cr-U median (with restricted cubic spline) Waist circumference ptrend = 0.018 (linear regression with quartiles of Cr-U) | [77] | |
| Russia 395 adults 20–60 years old 199 lean 196 obese | Cross-sectional | 4 metals in serum, hair and urine (Se, Zn, Cr, V) | Cr-S: 1.664 ng/mL (P25: 1.069, P75: 2.187) (normal weighted) Cr-S: 0.890 ng/mL (P25: 0.618, P75: 1.383) (obese) Cr-H: 0.065 μg/g (P25: 0.037, P75: 0.116) (normal weighted) Cr-H: 0.098 μg/g (P25: 0.059, P75: 0.199) (obese) Cr-U: 0.610 ng/mL (P25: 0.345, P75: 0.964) (normal weighted) Cr-U: 0.670 ng/mL (P25: 0.377, P75: 1.728) (obese) | BMI Cr-S: β = −0.320, p < 0.001 Cr-U: β = −0.054, p = 0.328 Cr-H: β = 0.085, p = 0.117 | [78] | |
| Renal function | ||||||
| Taiwan 2011 1643 adults, >50 years old: 1418 healthy, 225 with impaired eGFR | Cross-sectional | 5 metals in blood (As, Cd, Pb, Ni, Cr) | Cr-B: 0.15 μg/L (IQR: 2.25) | Risk for eGFR < 60 mL/min/1.73 m2 OR= 1.01 (95% CI: 0.97, 1.06) | [79] | |
| Taiwan 2005–2008 360 healthy adults, 19–84 years old | Cross-sectional | Cr, Pb, Cd in urine | Cr-U (geometric mean): 0.83 μg/L (95% CI 0.76 μg/L, 0.92 μg/L) | eGFR: β = −5.99 (95% CI: −9.70, −2.27) with logCr-U [mean eGFR: 100.3 mL/min/1.73 m2 (SD: 20.42) in men, 105.9 mL/min/1.73 m2 (SD: 20.26) in women] | [80] | |
| Taiwan, Changhua County, 2003–2015 2343 CKD patients, 20–90 years old: 533 with progression to end-stage renal disease [ESRD] and 1810 non-ESRD | Cohort of patients | 8 metals in soil (As, Cd, Cr, Hg, Cu, Pb, Ni, Zn) | Cr-Soil: 6.30 ± 11.04 mg/kg (for ESRD patients) Cr-Soil: 5.55 ± 8.89 mg/kg (for non-ESRD patients) | ESDR: HR = 1.072 (95% CI: 0.998, 1.152) for logCr in residential soil [mean eGFRs 17.8 ± 12.3 mL/min per 1.73 m2 (in ESRD patients) vs. 33.7 ± 20.0 (in non-ESRD patients)] | [81] | |
| China, rural areas 2016–2017 3553 adults | Cross-sectional | 23 metals in plasma and urine (Al, Ti, V, Cr, Mn, Fe, Co, Ni, Cu, Zn, As, Se, Rb, Sr, Mo, Cd, Sn, Sb, Ba, W, Tl, Pb, U) | Cr in plasma: app. 10 μg/L Cr-U: app. 2 μg/L | No association with abnormal eGFR (Wilcoxon rank sum test, p > 0.050) abnormal eGFR < 60 mL/min/1.73 m2: 2.5% of the population | [82] | |
| China 2018 1502 men, aged 30–79, of which 357 with nephrolithiasis | Cross-sectional | 5 metals in urine (As, Pb, Cd, Hg, Cr) | Cr-U: 30.20 µg/L (P25: 16.57 μg/L, P75: 45.12 μg/L) | Nephrolithiasis risk: when Cr-U from 17.78 to 25.12 μg/L OR = 1.24 (95% CI: 1.06, 1.45) [eGFR (mL/min/1.73 m2): 73.31 ± 16.64 (in non-nephrolithiasis subjects) vs. 68.97 ± 17.59 (nephrolithiasis subjects)] | [83] | |
| China 2016–2021 160 IgAN patients 480 healthy controls | Case control | 8 metals in plasma (V, Cr, Mn, Co, Cu, Zn, As, Pb) | Cr-U: 1.88 µg/L (P25: 0.95 μg/L, P75: 3.74 μg/L) (patients) Cr-U: 2.63 µg/L (P25: 2.27 μg/L, P75: 3.02 μg/L) (controls) Cr-U lower in patients (p < 0.001) | IgAN risk OR = 0.722 (95% CI: 0.456, 1.14) [eGFR (mL/min/1.73 m2): 71.1 ± 46.2 (cases) vs 104.0 ± 22.2 (controls] | [84] | |
| Other health outcomes | ||||||
| USA, 16 counties 2005–2009 413 reproductive-aged men | Cross-sectional | 20 metals in urine (Co, Cr, Cu, Mn, Mo, Ni, Se, Zn, Sb, As, Ba, Be, Cd, Pb, Pt, Te, Tl, Sn, W, U). | Cr-U: 0.62 μg/L (IQR: 0.66) | Total sperm count: β = 1.87, p = 0.003 DNA fragmentation index β = −5.08, p = 0.0009 [91.3% of the samples within normal range for total sperm count] | [85] | |
| China 2017–2019 210 age-related cataract patients 210 controls | Case control | 14 metals in urine (As, Ba, Cr, Co, Cu, Pb, Li, Mg, Mn, Mo, Fe, Se, Sr, Zn) | Cr-U: 25.02 μg/L (P25: 10.61 μg/L, P75: 36.25 μg/L) | Age-related cataract: OR = 3.71, (95% CI: 1.52, 9.08) (Q4 vs. Q1, in single model) No association in multi-element model | [86] | |
| Spain 2007–2016 458 affected municipalities | Ecological mortality | Distance 20 km or less from emission points 156 Cr-exposed municipalities | Motor neuron disease SMR = 1.12 (95% CI: 1.08, 1.17) for exposed municipalities 15.5% higher risk of MND | [87] | ||
- Cr and other health outcomes
- Cr and cancers
4. Discussion
5. Conclusions and Future Directions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Cardarelli, F. Materials Handbook: A Concise Desktop Reference, 2nd ed.; Springer: London, UK, 2008; p. 368. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. Arsenic, metals, fibres, and dusts. A review of human carcinogens. In IARC Monographs of the Evaluation of Carcinogenic Risks to Humans; International Agency for Research on Cancer (IARC): Lyon, France, 2012; Volume 100C. [Google Scholar]
- Koleli, N.; Demir, A. Chromite. In Environmental Materials and Waste, 1st ed.; Prasad, M.N.V., Shih, K., Eds.; Academic Press: Cambridge, MA, USA, 2016; pp. 245–263. [Google Scholar] [CrossRef]
- Kimbrough, D.E.; Cohen, Y.; Winer, A.M.; Creelman, L.; Mabuni, C. A critical assessment of chromium in the environment. Crit. Rev. Environ. Sci. Technol. 1999, 29, 1–46. [Google Scholar] [CrossRef]
- Fantoni, D.; Brozzo, G.; Canepa, M.; Cipolli, F.; Marini, L.; Ottonello, G.; Zuccolini, M. Natural hexavalent chromium in groundwaters interacting with ophiolitic rocks. Environ. Geol. 2002, 42, 871–882. [Google Scholar] [CrossRef]
- Levy, L.S.; Martin, P.A.; Bidstrup, P.L. Investigation of the potential carcinogenicity of a range of chromium containing materials on rat lung. Br. J. Ind. Med. 1986, 43, 243–256. [Google Scholar] [CrossRef]
- Hathaway, J.A. Role of epidemiologic studies in evaluating the carcinogenicity of chromium compounds. Sci. Total Environ. 1989, 86, 169–179. [Google Scholar] [CrossRef]
- DesMarais, T.L.; Costa, M. Mechanisms of Chromium-Induced Toxicity. Curr. Opin. Toxicol. 2019, 14, 1–7. [Google Scholar] [CrossRef]
- DeFlora, S. Threshold mechanisms and site specificity in chromium (VI) carcinogenesis. Carcinogenesis 2000, 21, 533–541. [Google Scholar] [CrossRef]
- Zhitkovich, A. Chromium in drinking water: Sources, metabolism, and cancer risks. Chem. Res. Toxicol. 2011, 24, 1617–1629. [Google Scholar] [CrossRef]
- Sun, H.; Brocato, J.; Costa, M. Oral Chromium Exposure and Toxicity. Curr. Environ. Health Rep. 2015, 2, 295–303. [Google Scholar] [CrossRef]
- Kerger, B.D.; Paustenbach, D.J.; Corbett, G.E.; Finley, B.L. Absorption and elimination of trivalent and hexavalent chromium in humans following ingestion of a bolus dose in drinking water. Toxicol. Appl. Pharmacol. 1996, 141, 145–158. [Google Scholar] [CrossRef]
- Stern, A.H. A quantitative assessment of the carcinogenicity of hexavalent chromium by the oral route and its relevance to human exposure. Environ. Res. 2010, 110, 798–807. [Google Scholar] [CrossRef]
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies). Scientific Opinion on Dietary Reference Values for chromium. EFSA J. 2014, 12, 3845. [Google Scholar] [CrossRef]
- Vincent, J.B. The biochemistry of chromium. J. Nutr. 2000, 130, 715–718. [Google Scholar] [CrossRef]
- Chen, G.; Liu, P.; Pattar, G.R.; Tackett, L.; Bhonagiri, P.; Strawbridge, A.B.; Elmendorf, J.S. Chromium activates glucose transporter 4 trafficking and enhances insulin-stimulated glucose transport in 3T3-L1 adipocytes via a cholesterol-dependent mechanism. Mol. Endocrinol. 2006, 20, 857–870. [Google Scholar] [CrossRef]
- Verdonck, J.; Duca, R.C.; Galea, K.S.; Iavicoli, I.; Poels, K.; Töreyin, Z.N.; Vanoirbeek, J.; Godderis, L. Systematic review of biomonitoring data on occupational exposure to hexavalent chromium. Int. J. Hyg. Environ. Health 2021, 236, 113799. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality If Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm (accessed on 24 January 2024).
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P.; Agyemang, C.; Remuzzi, G.; Rapi, S.; Perruolo, E.; Parati, G.; ESH Working Group on CV Risk in Low Resource Settings. Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0147601. [Google Scholar] [CrossRef]
- ATSDR (Agency for Toxic Substances and Disease Registry). Toxicological Profile for Chromium. US Department of Health and Human Services, Atlanta. 2012. Available online: https://www.atsdr.cdc.gov/ToxProfiles/tp7.pdf (accessed on 6 September 2023).
- Zhang, J.D.; Li, X.L. Chromium pollution of soil and water in Jinzhou. Zhonghua Yu Fang Yi Xue Za Zhi 1987, 21, 262–264. (In Chinese) [Google Scholar]
- Zhang, J.D.; Li, S. Cancer mortality in a Chinese population exposed to hexavalent chromium in water. J. Occup. Environ. Med. 1997, 39, 315–319, Erratum in J. Occup. Environ. Med. 2006, 48, 749. [Google Scholar] [CrossRef]
- Beaumont, J.J.; Sedman, R.M.; Reynolds, S.D.; Sherman, C.D.; Li, L.H.; Howd, R.A.; Sandy, M.S.; Zeise, L.; Alexeeff, G.V. Cancer mortality in five villages in China with hexavalent chromium-contaminated drinking water. Epidemiology 2008, 19, 12–23. [Google Scholar] [CrossRef]
- Kerger, B.D.; Butler, W.J.; Paustenbach, D.J.; Zhang, J.; Li, S. Cancer mortality in Chinese populations surrounding an alloy plant with chromium smelting operations. J. Toxicol. Environ. Health Pt A 2009, 72, 329–344. [Google Scholar] [CrossRef]
- Smith, A.H. Hexavalent chromium, yellow water, and cancer: A convoluted saga. Epidemiology 2008, 19, 24–26. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Zhao, M.; Pei, L.; Zhang, R.; Liu, X.; Wei, L.; Yang, M.; Xu, Q. Oxidative stress and DNA damage in a long-term hexavalent chromium-exposed population in North China: A cross-sectional study. BMJ Open 2018, 8, e021470. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Bihari, V.; Agarwal, S.K.; Verma, V.; Kesavachandran, C.N.; Pangtey, B.S.; Mathur, N.; Singh, K.P.; Srivastava, M.; Goel, S.K. Groundwater contaminated with hexavalent chromium (Cr(VI)): A health survey and clinical examination of community inhabitants (Kanpur, India). PLoS ONE 2012, 7, e47877. [Google Scholar] [CrossRef]
- Sazakli, E.; Villanueva, C.M.; Kogevinas, M.; Maltezis, K.; Mouzaki, A.; Leotsinidis, M. Chromium in drinking water: Association with biomarkers of exposure and effect. Int. J. Environ. Res. Public Health 2014, 11, 10125–10145. [Google Scholar] [CrossRef] [PubMed]
- Karagiannis, D.; Deliveliotis, C.; Papadimitriou, E.; Riza, E.; Lykou, A.; Petralias, A.; Papatsoris, A.; Linos, A. Oral exposure to hexavalent chromium through drinking water and urologic morbidity in an industrial area of Greece. J. Public Health 2015, 23, 249–255. [Google Scholar] [CrossRef]
- Linos, A.; Petralias, A.; Christophi, C.A.; Christoforidou, E.; Kouroutou, P.; Stoltidis, M.; Veloudaki, A.; Tzala, E.; Makris, K.C.; Karagas, M.R. Oral ingestion of hexavalent chromium through drinking water and cancer mortality in an industrial area of Greece—An ecological study. Environ. Health 2011, 10, 50. [Google Scholar] [CrossRef]
- California EPA Office of Environmental Health Hazard Assessment (OEHHA). Public Health Goal for Hexavalent Chromium (CrVI) in Drinking Water 2011. Available online: https://oehha.ca.gov/media/downloads/water/chemicals/phg/cr6phg072911.pdf (accessed on 24 January 2024).
- Fryzek, J.P.; Mumma, M.T.; McLaughlin, J.K.; Henderson, B.E.; Blot, W.J. Cancer mortality in relation to environmental chromium exposure. J. Occup. Environ. Med. 2001, 43, 635–640. [Google Scholar] [CrossRef]
- Lacagnina, S. The Developmental Origins of Health and Disease (DOHaD). Am. J. Lifestyle Med. 2019, 14, 47–50. [Google Scholar] [CrossRef]
- Darney, S.; Fowler, B.; Grandjean, P.; Heindel, J.; Mattison, D.; Slikker, W., Jr. Prenatal Programming and Toxicity II (PPTOX II): Role of environmental stressors in the developmental origins of disease. Reprod. Toxicol. 2011, 31, 271. [Google Scholar] [CrossRef]
- Xia, W.; Hu, J.; Zhang, B.; Li, Y.; Wise, J.P., Sr.; Bassig, B.A.; Zhou, A.; Savitz, D.A.; Xiong, C.; Zhao, J.; et al. A case-control study of maternal exposure to chromium and infant low birth weight in China. Chemosphere 2016, 144, 1484–1489. [Google Scholar] [CrossRef]
- Yang, X.; Li, Y.; Li, J.; Bao, S.; Zhou, A.; Xu, S.; Xia, W. Associations between exposure to metal mixtures and birth weight. Environ. Pollut. 2020, 263 Pt B, 114537. [Google Scholar] [CrossRef]
- Michael, T.; Kohn, E.; Daniel, S.; Hazan, A.; Berkovitch, M.; Brik, A.; Hochwald, O.; Borenstein-Levin, L.; Betser, M.; Moskovich, M.; et al. Prenatal exposure to heavy metal mixtures and anthropometric birth outcomes: A cross-sectional study. Environ. Health 2022, 21, 139. [Google Scholar] [CrossRef]
- Cabrera-Rodríguez, R.; Luzardo, O.P.; González-Antuña, A.; Boada, L.D.; Almeida-González, M.; Camacho, M.; Zumbado, M.; Acosta-Dacal, A.C.; Rial-Berriel, C.; Henríquez-Hernández, L.A. Occurrence of 44 elements in human cord blood and their association with growth indicators in newborns. Environ. Int. 2018, 116, 43–51. [Google Scholar] [CrossRef]
- Freire, C.; Amaya, E.; Gil, F.; Murcia, M.; LLop, S.; Casas, M.; Vrijheid, M.; Lertxundi, A.; Irizar, A.; Fernández-Tardón, G.; et al. Placental metal concentrations and birth outcomes: The Environment and Childhood (INMA) project. Int. J. Hyg. Environ. Health 2019, 222, 468–478. [Google Scholar] [CrossRef]
- Peng, Y.; Hu, J.; Li, Y.; Zhang, B.; Liu, W.; Li, H.; Zhang, H.; Hu, C.; Chen, X.; Xia, W.; et al. Exposure to chromium during pregnancy and longitudinally assessed fetal growth: Findings from a prospective cohort. Environ. Int. 2018, 121 Pt 1, 375–382. [Google Scholar] [CrossRef]
- Dou, Y.; Yin, Y.; Li, Z.; Du, J.; Jiang, Y.; Jiang, T.; Guo, W.; Qin, R.; Li, M.; Lv, H.; et al. Maternal exposure to metal mixtures during early pregnancy and fetal growth in the Jiangsu Birth Cohort, China. Environ. Res. 2022, 215, 114305. [Google Scholar] [CrossRef]
- Yu, Y.; Gao, M.; Wang, X.; Guo, Y.; Pang, Y.; Yan, H.; Hao, Y.; Zhang, Y.; Zhang, L.; Ye, R.; et al. Recommended acceptable levels of maternal serum typical toxic metals from the perspective of spontaneous preterm birth in Shanxi Province, China. Sci. Total. Environ. 2019, 686, 599–605, Erratum in Sci. Total. Environ. 2020, 725, 138758. [Google Scholar] [CrossRef]
- Pan, X.; Hu, J.; Xia, W.; Zhang, B.; Liu, W.; Zhang, C.; Yang, J.; Hu, C.; Zhou, A.; Chen, Z.; et al. Prenatal chromium exposure and risk of preterm birth: A cohort study in Hubei, China. Sci. Rep. 2017, 7, 3048. [Google Scholar] [CrossRef]
- Huang, S.; Xia, W.; Li, Y.; Zhang, B.; Zhou, A.; Zheng, T.; Qian, Z.; Huang, Z.; Lu, S.; Chen, Z.; et al. Association between maternal urinary chromium and premature rupture of membranes in the Healthy Baby Cohort study in China. Environ. Pollut. 2017, 230, 53–60. [Google Scholar] [CrossRef]
- Tian, T.; Yin, S.; Jin, L.; Liu, J.; Wang, C.; Wei, J.; Liu, M.; Li, Z.; Wang, L.; Yin, C.; et al. Single and mixed effects of metallic elements in maternal serum during pregnancy on risk for fetal neural tube defects: A Bayesian kernel regression approach. Environ. Pollut. 2021, 285, 117203. [Google Scholar] [CrossRef]
- Ou, Y.; Bloom, M.S.; Nie, Z.; Han, F.; Mai, J.; Chen, J.; Lin, S.; Liu, X.; Zhuang, J. Associations between toxic and essential trace elements in maternal blood and fetal congenital heart defects. Environ. Int. 2017, 106, 127–134. [Google Scholar] [CrossRef]
- Xu, C.; Xu, J.; Zhang, X.; Xu, S.; Liu, Q.; Weng, Z.; Gu, A. Serum nickel is associated with craniosynostosis risk: Evidence from humans and mice. Environ. Int. 2021, 146, 106289. [Google Scholar] [CrossRef]
- Ruan, F.; Zhang, J.; Liu, J.; Sun, X.; Li, Y.; Xu, S.; Xia, W. Association between prenatal exposure to metal mixtures and early childhood allergic diseases. Environ. Res. 2022, 206, 112615. [Google Scholar] [CrossRef]
- Vänskä, M.; Diab, S.Y.; Perko, K.; Quota, S.R.; Albarqouni, N.M.A.; Myöhänen, A.; Punamäki, R.L.; Manduca, P. Toxic Environment of war: Maternal prenatal heavy metal load predicts infant emotional development. Infant Behav. Dev. 2019, 55, 1–9. [Google Scholar] [CrossRef]
- Levin-Schwartz, Y.; Cowell, W.; Leon Hsu, H.H.; Enlow, M.B.; Amarasiriwardena, C.; Andra, S.S.; Wright, R.J.; Wright, R.O. Metal mixtures are associated with increased anxiety during pregnancy. Environ. Res. 2022, 204 Pt C, 112276. [Google Scholar] [CrossRef]
- Leal, C.A.; Schetinger, M.R.; Leal, D.B.; Morsch, V.M.; da Silva, A.S.; Rezer, J.F.; de Bairros, A.V.; Jaques, J.A. Oxidative stress and antioxidant defenses in pregnant women. Redox Rep. 2011, 16, 230–236. [Google Scholar] [CrossRef]
- Zhu, G.; Zheng, T.; Xia, C.; Qi, L.; Papandonatos, G.D.; Ming, Y.; Zeng, Z.; Zhang, X.; Zhang, H.; Li, Y. Plasma levels of trace element status in early pregnancy and the risk of gestational diabetes mellitus: A nested case-control study. J. Trace Elem. Med. Biol. 2021, 68, 126829. [Google Scholar] [CrossRef]
- Bommarito, P.A.; Kim, S.S.; Meeker, J.D.; Fry, R.C.; Cantonwine, D.E.; McElrath, T.F.; Ferguson, K.K. Urinary trace metals, maternal circulating angiogenic biomarkers, and preeclampsia: A single-contaminant and mixture-based approach. Environ. Health 2019, 18, 63. [Google Scholar] [CrossRef]
- Wu, L.L.; Gong, W.; Shen, S.P.; Wang, Z.H.; Yao, J.X.; Wang, J.; Yu, J.; Gao, R.; Wu, G. Multiple metal exposures and their correlation with monoamine neurotransmitter metabolism in Chinese electroplating workers. Chemosphere 2017, 182, 745–752. [Google Scholar] [CrossRef]
- Liu, Y.; Yu, L.; Zhu, M.; Lin, W.; Liu, Y.; Li, M.; Zhang, Y.; Ji, H.; Wang, J. Associations of exposure to multiple metals with blood pressure and hypertension: A cross-sectional study in Chinese preschool children. Chemosphere 2022, 307, 135985. [Google Scholar] [CrossRef]
- Zhumalina, A.K.; Bekmukhambetov, E.Z.; Tusupkaliev, B.T.; Zharlikasinova, M.B. Development of scientifically justified proposals on the prevention and treatment of environmentally determined constitutional growth delay in children in the West Kazakhstan region. Environ. Geochem. Health 2019, 41, 1251–1265. [Google Scholar] [CrossRef]
- Caparros-Gonzalez, R.A.; Giménez-Asensio, M.J.; González-Alzaga, B.; Aguilar-Garduño, C.; Lorca-Marín, J.A.; Alguacil, J.; Gómez-Becerra, I.; Gómez-Ariza, J.L.; García-Barrera, T.; Hernandez, A.F.; et al. Childhood chromium exposure and neuropsychological development in children living in two polluted areas in southern Spain. Environ. Pollut. 2019, 252 Pt B, 1550–1560. [Google Scholar] [CrossRef]
- Quinteros, F.A.; Poliandri, A.H.; Machiavelli, L.I.; Cabilla, J.P.; Duvilanski, B.H. In vivo and in vitro effects of chromium VI on anterior pituitary hormone release and cell viability. Toxicol. Appl. Pharmacol. 2007, 218, 79–87. [Google Scholar] [CrossRef]
- Piñeiro, X.F.; Ave, M.T.; Mallah, N.; Caamaño-Isorna, F.; Jiménez, A.N.G.; Vieira, D.N.; Bianchini, F.; Muñoz-Barús, J.I. Heavy metal contamination in Peru: Implications on children’s health. Sci. Rep. 2021, 11, 22729. [Google Scholar] [CrossRef]
- Qu, Y.; Lv, Y.; Ji, S.; Ding, L.; Zhao, F.; Zhu, Y.; Zhang, W.; Hu, X.; Lu, Y.; Li, Y.; et al. Effect of exposures to mixtures of lead and various metals on hypertension, pre-hypertension, and blood pressure: A cross-sectional study from the China National Human Biomonitoring. Environ. Pollut. 2022, 299, 118864. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, D.; Wu, X.; Tu, J.; Gong, C.; Li, Y.; Cui, W.; Chen, J.; Lu, S. Urinary metals as influencing factors of coronary heart disease among a population in Guangzhou, China. Ecotoxicol. Environ. Saf. 2022, 241, 113746. [Google Scholar] [CrossRef]
- Son, J.; Morris, J.S.; Park, K. Toenail Chromium Concentration and Metabolic Syndrome among Korean Adults. Int. J. Environ. Res. Public Health 2018, 15, 682. [Google Scholar] [CrossRef]
- Feng, W.; He, X.; Chen, M.; Deng, S.; Qiu, G.; Li, X.; Liu, C.; Li, J.; Deng, Q.; Huang, S.; et al. Urinary metals and heart rate variability: A cross-sectional study of urban adults in Wuhan, China. Environ. Health Perspect. 2015, 123, 217–222. [Google Scholar] [CrossRef]
- Zhao, M.; Ge, X.; Xu, J.; Li, A.; Mei, Y.; Yin, G.; Wu, J.; Liu, X.; Wei, L.; Xu, Q. Association between urine metals and liver function biomarkers in Northeast China: A cross-sectional study. Ecotoxicol. Environ. Saf. 2022, 231, 113163. [Google Scholar] [CrossRef]
- Zhao, M.; Yin, G.; Xu, J.; Ge, X.; Li, A.; Mei, Y.; Wu, J.; Liu, X.; Wei, L.; Xu, Q. Independent, combine and interactive effects of heavy metal exposure on dyslipidemia biomarkers: A cross-sectional study in northeastern China. Ecotoxicol. Environ. Saf. 2023, 250, 114494. [Google Scholar] [CrossRef]
- Xu, J.; Zhao, M.; Pei, L.; Liu, X.; Wei, L.; Li, A.; Mei, Y.; Xu, Q. Effects of heavy metal mixture exposure on hematological and biomedical parameters mediated by oxidative stress. Sci. Total. Environ. 2020, 705, 134865. [Google Scholar] [CrossRef]
- Chang, Z.; Qiu, J.; Wang, K.; Liu, X.; Fan, L.; Liu, X.; Zhao, Y.; Zhang, Y. The relationship between co-exposure to multiple heavy metals and liver damage. J. Trace Elem. Med. Bio.l 2023, 77, 127128. [Google Scholar] [CrossRef]
- Xiao, L.; Zhou, Y.; Ma, J.; Cao, L.; Wang, B.; Zhu, C.; Yang, S.; Li, W.; Zhang, Z.; Wang, D.; et al. The cross-sectional and longitudinal associations of chromium with dyslipidemia: A prospective cohort study of urban adults in China. Chemosphere 2019, 215, 362–369. [Google Scholar] [CrossRef]
- Liu, L.; Li, A.; Xu, Q.; Wang, Q.; Han, F.; Xu, C.; Liu, Z.; Xu, D.; Xu, D. The association between urine elements and fasting glucose levels in a community-based elderly people in Beijing. Environ. Sci. Pollut. Res. Int. 2022, 29, 30102–30113. [Google Scholar] [CrossRef]
- Bibi, M.; Hashmi, M.Z.; Malik, R.N. The level and distribution of heavy metals and changes in oxidative stress indices in humans from Lahore district, Pakistan. Hum. Exp. Toxicol. 2016, 35, 78–90. [Google Scholar] [CrossRef]
- Velmurugan, G.; Swaminathan, K.; Veerasekar, G.; Purnell, J.Q.; Mohanraj, S.; Dhivakar, M.; Avula, A.K.; Cherian, M.; Palaniswami, N.G.; Alexander, T.; et al. Metals in urine in relation to the prevalence of pre-diabetes, diabetes and atherosclerosis in rural India. Occup. Environ. Med. 2018, 75, 661–667. [Google Scholar] [CrossRef]
- Domingo-Relloso, A.; Grau-Perez, M.; Galan-Chilet, I.; Garrido-Martinez, M.J.; Tormos, C.; Navas-Acien, A.; Gomez-Ariza, J.L.; Monzo-Beltran, L.; Saez-Tormo, G.; Garcia-Barrera, T.; et al. Urinary metals and metal mixtures and oxidative stress biomarkers in an adult population from Spain: The Hortega Study. Environ. Int. 2019, 123, 171–180. [Google Scholar] [CrossRef]
- McIver, D.J.; Grizales, A.M.; Brownstein, J.S.; Goldfine, A.B. Risk of Type 2 Diabetes Is Lower in US Adults Taking Chromium-Containing Supplements. J. Nutr. 2015, 145, 2675–2682. [Google Scholar] [CrossRef]
- Wang, X.; Karvonen-Gutierrez, C.A.; Herman, W.H.; Mukherjee, B.; Harlow, S.D.; Park, S.K. Urinary metals and incident diabetes in midlife women: Study of Women’s Health Across the Nation (SWAN). BMJ Open Diabetes Res. Care 2020, 8, e001233. [Google Scholar] [CrossRef]
- Zhang, R.; Xiang, Y.; Ran, Q.; Deng, X.; Xiao, Y.; Xiang, L.; Li, Z. Involvement of calcium, reactive oxygen species, and ATP in hexavalent chromium-induced damage in red blood cells. Cell. Physiol. Biochem. 2014, 34, 1780–1791. [Google Scholar] [CrossRef]
- Zhao, M.; Ge, X.; Xu, J.; Li, A.; Mei, Y.; Zhao, J.; Zhou, Q.; Liu, X.; Wei, L.; Xu, Q. Negatively interactive effect of chromium and cadmium on obesity: Evidence from adults living near ferrochromium factory. Ecotoxicol. Environ. Saf. 2022, 231, 113196. [Google Scholar] [CrossRef] [PubMed]
- Tinkov, A.A.; Skalnaya, M.G.; Ajsuvakova, O.P.; Serebryansky, E.P.; Chao, J.C.; Aschner, M.; Skalny, A.V. Selenium, Zinc, Chromium, and Vanadium Levels in Serum, Hair, and Urine Samples of Obese Adults Assessed by Inductively Coupled Plasma Mass Spectrometry. Biol. Trace Elem. Res. 2021, 199, 490–499. [Google Scholar] [CrossRef]
- Chung, M.C.; Hsu, H.T.; Mao, Y.C.; Wu, C.C.; Ho, C.T.; Liu, C.S.; Chung, C.J. Association and mediation analyses among multiple metals exposure, plasma folate, and community-based impaired estimated glomerular filtration rate in central Taiwan. Environ. Health 2022, 21, 44. [Google Scholar] [CrossRef] [PubMed]
- Tsai, T.L.; Kuo, C.C.; Pan, W.H.; Chung, Y.T.; Chen, C.Y.; Wu, T.N.; Wang, S.L. The decline in kidney function with chromium exposure is exacerbated with co-exposure to lead and cadmium. Kidney Int. 2017, 92, 710–720. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.C.; Wu, C.L.; Kor, C.T.; Lian, I.B.; Chang, C.H.; Chang, T.H.; Chang, C.C.; Chiu, P.F. Prospective associations between environmental heavy metal exposure and renal outcomes in adults with chronic kidney disease. Nephrology 2018, 23, 830–836. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Yi, X.; Guo, J.; Xu, S.; Xiao, Y.; Huang, X.; Duan, Y.; Luo, D.; Xiao, S.; Huang, Z.; et al. Association of plasma and urine metals levels with kidney function: A population-based cross-sectional study in China. Chemosphere 2019, 226, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, C.; Qin, Z.; Yang, Q.; Lei, J.; Tang, X.; Wang, Q.; Hong, F. Analysis of Threshold Effect of Urinary Heavy Metal Elements on the High Prevalence of Nephrolithiasis in Men. Biol. Trace Elem. Res. 2022, 200, 1078–1088. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zhang, L.; Luo, N.; Wang, M.; Tang, C.; Jing, J.; Chen, H.; Hu, Q.; Tan, L.; Ma, X.; et al. Metal mixture exposure and the risk for immunoglobulin A nephropathy: Evidence from weighted quantile sum regression. Environ. Sci. Pollut. Res. Int. 2023, 30, 87783–87792. [Google Scholar] [CrossRef] [PubMed]
- Branch, F.M.; Perry, M.J.; Chen, Z.; Louis, G.M.B. Metal(loid)s and human semen quality: The LIFE Study. Reprod. Toxicol. 2021, 106, 94–102. [Google Scholar] [CrossRef]
- Li, Y.Q.; Wang, Q.; Liu, R.; Li, G.A.; He, J.L.; Huang, F.; Zhou, Y.F. Associations of exposure to multiple metals with the risk of age-related cataract in Anhui, China: A case-control study. Environ. Sci. Pollut. Res. Int. 2023, 30, 4680–4693. [Google Scholar] [CrossRef]
- Sánchez-Díaz, G.; Escobar, F.; Badland, H.; Arias-Merino, G.; Posada de la Paz, M.; Alonso-Ferreira, V. Geographic Analysis of Motor Neuron Disease Mortality and Heavy Metals Released to Rivers in Spain. Int. J. Environ. Res. Public Health 2018, 15, 2522. [Google Scholar] [CrossRef] [PubMed]
- Mérida-Ortega, Á.; Rothenberg, S.J.; Cebrián, M.E.; López-Carrillo, L. Breast cancer and urinary metal mixtures in Mexican women. Environ. Res. 2022, 210, 112905. [Google Scholar] [CrossRef] [PubMed]
- Caini, S.; Cozzolino, F.; Saieva, C.; Aprea, M.C.; De Bonfioli Cavalcabo’, N.; Ermini, I.; Assedi, M.; Biagiotti, D.; Trane, C.; Facchini, L.; et al. Serum heavy metals and breast cancer risk: A case-control study nested in the Florence cohort of the EPIC (European Prospective Investigation into Cancer and nutrition) study. Sci. Total. Environ. 2023, 861, 160568. [Google Scholar] [CrossRef] [PubMed]
- Matthews, N.H.; Koh, M.; Li, W.Q.; Li, T.; Willett, W.C.; Stampfer, M.J.; Christiani, D.C.; Morris, J.S.; Qureshi, A.A.; Cho, E. A Prospective Study of Toenail Trace Element Levels and Risk of Skin Cancer. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1534–1543. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.H.; Liu, C.S.; Liu, H.J.; Huang, C.P.; Huang, C.Y.; Hsu, H.T.; Liou, S.H.; Chung, C.J. Association between levels of urinary heavy metals and increased risk of urothelial carcinoma. Int. J. Urol. 2016, 23, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.J.; He, J.L.; Tong, X.R.; Yang, W.J.; Zhao, H.H.; Li, G.A.; Huang, F. Associations between essential microelements exposure and the aggressive clinicopathologic characteristics of papillary thyroid cancer. Biometals 2021, 34, 909–921. [Google Scholar] [CrossRef] [PubMed]
- Antwi, S.O.; Eckert, E.C.; Sabaque, C.V.; Leof, E.R.; Hawthorne, K.M.; Bamlet, W.R.; Chaffee, K.G.; Oberg, A.L.; Petersen, G.M. Exposure to environmental chemicals and heavy metals, and risk of pancreatic cancer. Cancer Causes Control 2015, 26, 1583–1591. [Google Scholar] [CrossRef] [PubMed]
- Feki-Tounsi, M.; Olmedo, P.; Gil, F.; Mhiri, M.N.; Rebai, A.; Hamza-Chaffai, A. Trace metal quantification in bladder biopsies from tumoral lesions of Tunisian cancer and controls subjects. Environ. Sci. Pollut. Res. Int. 2014, 21, 11433–11438. [Google Scholar] [CrossRef] [PubMed]
- Núñez, O.; Fernández-Navarro, P.; Martín-Méndez, I.; Bel-Lan, A.; Locutura, J.F.; López-Abente, G. Arsenic and chromium topsoil levels and cancer mortality in Spain. Environ. Sci. Pollut. Res. Int. 2016, 23, 17664–17675. [Google Scholar] [CrossRef]
- Norseth, T. The carcinogenicity of chromium. Environ. Health Perspect. 1981, 40, 121–130. [Google Scholar] [CrossRef]
- Alexander, J.; Aaseth, J. Uptake of chromate in human red blood cells and isolated rat liver cells: The role of the anion carrier. Analyst 1995, 120, 931–933. [Google Scholar] [CrossRef] [PubMed]
- Qu, Q.; Li, X.; An, F.; Jia, G.; Liu, L.; Watanabe-Meserve, H.; Koenig, K.; Cohen, B.; Costa, M.; Roy, N.; et al. CrVI exposure and biomarkers: Cr in erythrocytes in relation to exposure and polymorphisms of genes encoding anion transport proteins. Biomarkers 2008, 13, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Alimonti, A.; Bocca, B.; Mannella, E.; Petrucci, F.; Zennaro, F.; Cotichini, R.; D’Ippolito, C.; Agresti, A.; Caimi, S.; Forte, G. Assessment of reference values for selected elements in a healthy urban population. Ann. Ist. Super Sanità 2005, 41, 181–187. [Google Scholar] [PubMed]
- Minoia, C.; Sabbioni, E.; Apostoli, P.; Pietra, R.; Pozzoli, L.; Gallorini, M.; Nicolaou, G.; Alessio, L.; Capodaglio, E. Trace element reference values in tissues from inhabitants of the European community. I. A study of 46 elements in urine, blood and serum of Italian subjects. Sci. Total. Environ. 1990, 95, 89–105. [Google Scholar] [CrossRef] [PubMed]
- Morton, J.; Tan, E.; Leese, E.; Cocker, J. Determination of 61 elements in urine samples collected from a non-occupationally exposed UK adult population. Toxicol. Lett. 2014, 231, 179–193. [Google Scholar] [CrossRef] [PubMed]
- Santonen, T.; Porras, S.P.; Bocca, B.; Bousoumah, R.; Duca, R.C.; Galea, K.S.; Godderis, L.; Göen, T.; Hardy, E.; Iavicoli, I.; et al. HBM4EU chromates study—Overall results and recommendations for the biomonitoring of occupational exposure to hexavalent chromium. Environ. Res. 2022, 204 Pt A, 111984. [Google Scholar] [CrossRef]
- Skalny, A.V.; Skalnaya, M.G.; Tinkov, A.A.; Serebryansky, E.P.; Demidov, V.A.; Lobanova, Y.N.; Grabeklis, A.R.; Berezkina, E.S.; Gryazeva, I.V.; Skalny, A.A.; et al. Hair concentration of essential trace elements in adult non-exposed Russian population. Environ. Monit. Assess. 2015, 187, 677. [Google Scholar] [CrossRef] [PubMed]
- Rodushkin, I.; Ödman, F.; Branth, S. Multielement analysis of whole blood by high resolution inductively coupled plasma mass spectrometry. Fresen. J. Anal. Chem. 1999, 364, 338–346. [Google Scholar] [CrossRef]
- Chen, Q.Y.; DesMarais, T.; Costa, M. Metals and Mechanisms of Carcinogenesis. Annu. Rev. Pharmacol. Toxicol. 2019, 59, 537–554. [Google Scholar] [CrossRef]

| Study Characteristics (Area, Time, Population) | Study Design | Exposure Variables | Biomonitoring Data [(Mean± SD) or Median] | Key Findings on Health Outcomes | Ref. |
|---|---|---|---|---|---|
| Mexico 2007–2011 452 breast cancer cases 439 controls | Case control | 11 metals in urine (Al, As, Cd, Cr, Ni, Pb, Sb, Co, Mo, Sn, V) | Cr-U: 3.16 μg/g creatinine (P10: 1.27 μg/g, P90: 8.93 μg/g) (cases) Cr-U: 3.00 μg/g creatinine (P10: 1.35 μg/g, P90: 7.97 μg/g) (controls) | No difference of Cr levels in cases and controls (ptrend = 0.709) Breast cancer: mixture of Cr, Ni, Sb, Al, Pb, Sn OR = 1.15 (95% CI: 1.06, 1.25) | [88] |
| Italy 1993–1998 150 breast cancer cases 150 controls | Nested case control | 6 metals in serum (Cd, Co, Cr, Mn, Pb, Tl) | Cr-S: P75: 2.10 μg/L (cases) Cr-S: P75: 2.40 μg/L (controls) | Breast cancer: no difference in Cr levels between cases and controls (p > 0.050) OR = 0.66 (95% CI: 0.26, 1.67) for Cr-S 0.63–2.40 μg/L vs. <0.50 μg/L OR = 0.60 (95% CI: 0.20, 1.82) for Cr-S >2.50 μg/L vs. <0.50 μg/L | [89] |
| USA 1984–2012 10,438 adults 6708 women 3730 men | Prospective cohort | 5 metals in toenails (Cr, Fe, Hg, Se, Zn) | Cr-Toenails: 0.86 ± 2.83 μg/g (women) Cr-Toenails: 0.89 ± 1.82 μg/g (men) | BCC: HR = 1.32 (95% CI: 1.12, 1.56) (only in women) for Q5 (median Cr: 1.78 μg/g) vs. Q1 (median Cr: 0.12 μg/g) SCC: HR = 1.41 (95% CI 0.92, 2.15) (women) for Q4 (median Cr: 0.71 μg/g) vs. Q1 (median Cr: 0.12 μg/g) Melanoma: HR = 1.41 (95% CI: 0.92, 2.15) (women) Melanoma: HR = 0.95 (95% CI: 0.59, 1.54) (men) | [90] |
| Taiwan 2011–2013 205 urothelial carcinoma cases, 406 controls | Case control | 5 metals in urine (Cr, As, Cd, Ni, Pb) | Cr-U: 0.61 ± 0.10 μg/g creatinine (mean ±SE) (controls) Cr-U: 2.38 ± 0.41 μg/g creatinine (mean ±SE) (patients) | Urothelial cancer: OR = 2.01 (95% CI: 1.12, 3.60) (Cr-U: 0.18–0.45 μg/g creatinine) OR = 5.78 (95% CI: 3.37, 9.90) (Cr-U: > 0.45 μg/g creatinine) | [91] |
| China 2017–2019 608 papillary thyroid cancer cases (74.7% females) | Patient study | 10 elements in urine (Co, Cr, Cu, Fe, Mn, Mo, Se, Sr, Zn, and I) | Cr-U: 43.23 μg/g creatinine (P25: 21.61 μg/g, P75: 57.58 μg/g) | Clinicopathologic characteristics of papillary thyroid cancer OR = 1.68, (95% CI 1.02, 2.77) (Q4 vs. Q1) for multifocality, in single -element model No association in multi-element model | [92] |
| USA 2000–2014 2092 patients with pancreatic ductal adenocarcinoma 2353 controls | Case control | Self-reported exposure | Not determined | Pancreatic cancer: OR = 1.42, (95% CI 0.89, 2.26) for self-reported Cr exposure | [93] |
| Tunisia 2007–2010 49 bladder cancer cases 36 controls | Case control | Cr in tissues | Cr: 1.50 ± 3.23 μg/g (mean ± SE) in cancer tissues Cr: 10.09 ± 18.16 μg/g (mean ± SE) in adjacent tissues Cr: 13.48 ± 19.90 μg/g (mean ± SE) in control tissues | Significantly lower Cr level in cancer tissues | [94] |
| Spain 1999–2008 | Ecological mortality | Exposure surrogate: Cr topsoil levels in 21,187 samples | Cr-Soil: 23.2 mg/kg (P25:15.6 mg/kg, P75: 33.8 mg/kg) (range: 0.50–2100 mg/kg) | Cancer of the buccal cavity and pharynx RR = 1.149, (95% CI 1.036, 1.274) (women only) Cancer of esophagus RR = 1.328, (95% CI: 1.146, 1.544) (women) Non-Hodgkin’s lymphoma: RR = 1.092 (95% CI: 1.018, 1.170) (women) Breast cancer: RR = 1.045 (95% CI: 1.009, 1.082) (women) | [95] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sazakli, E. Human Health Effects of Oral Exposure to Chromium: A Systematic Review of the Epidemiological Evidence. Int. J. Environ. Res. Public Health 2024, 21, 406. https://doi.org/10.3390/ijerph21040406
Sazakli E. Human Health Effects of Oral Exposure to Chromium: A Systematic Review of the Epidemiological Evidence. International Journal of Environmental Research and Public Health. 2024; 21(4):406. https://doi.org/10.3390/ijerph21040406
Chicago/Turabian StyleSazakli, Eleni. 2024. "Human Health Effects of Oral Exposure to Chromium: A Systematic Review of the Epidemiological Evidence" International Journal of Environmental Research and Public Health 21, no. 4: 406. https://doi.org/10.3390/ijerph21040406