
Experiences of People with Cardiovascular Disease during COVID-19 in Sweden: A Qualitative Study

{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Recruitment of Participants
2.3. Ethics
2.4. Procedure
2.5. Data Analysis
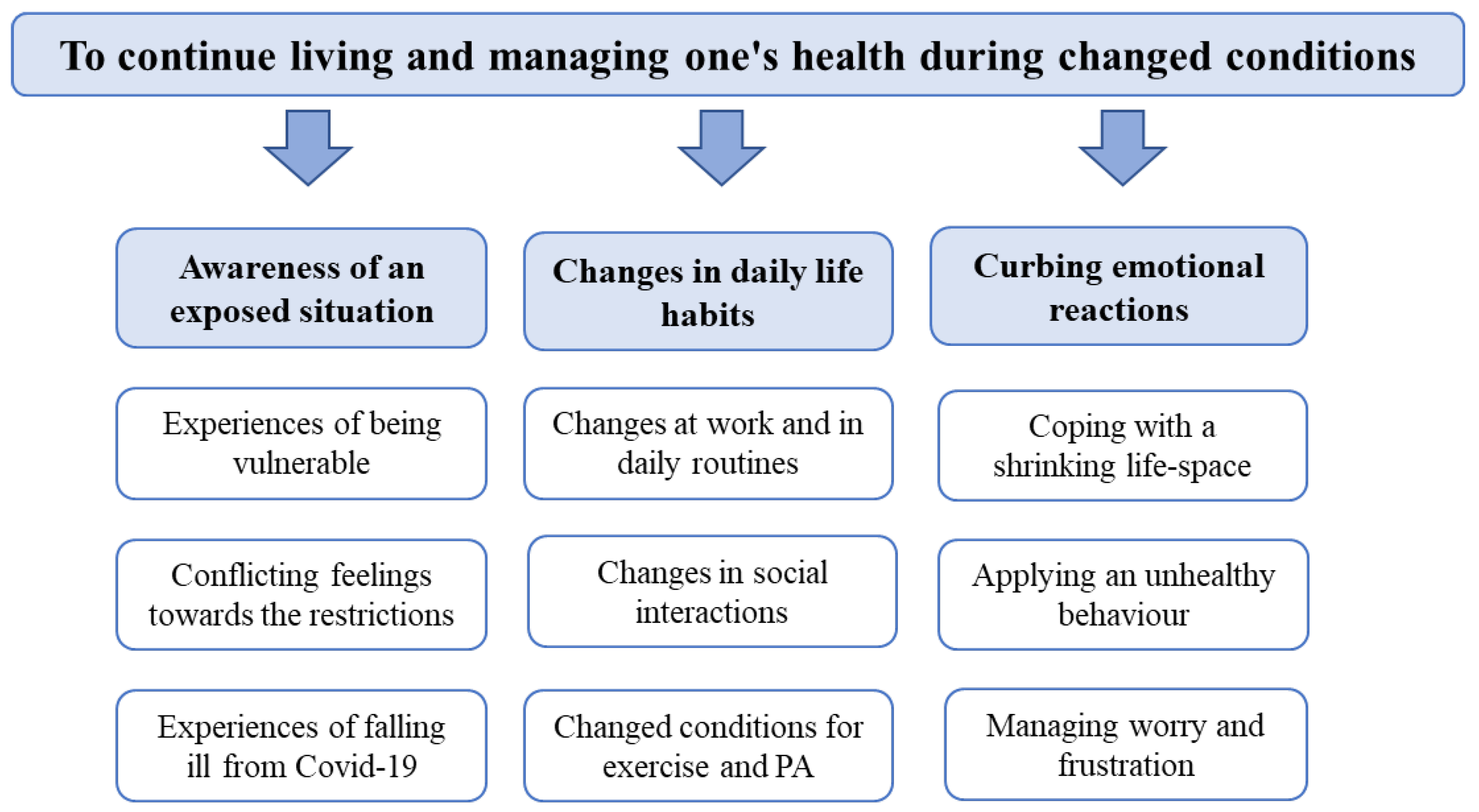
3. Results
3.1. Awareness of An Exposed Situation
3.1.1. Experiences of Being Vulnerable
… If you know you have high blood pressure, um, both my parents suffered a stroke before they passed away, and high blood pressure is definitely a marker. Eh… So that, just knowing that blood pressure is high makes you feel stressed, and then the blood pressure rises even more.P 2
…my doctor does medical check-ups every year, but it [the appointment] was cancelled this year or rather last year, because then [due to the pandemic] they were forced to reallocate resources.P 5
3.1.2. Conflicting Feelings towards the Restrictions
It always feels like you’re doing something wrong, and that’s what will be so nice when it’s over, that you never, that is, you won’t have to feel guilty all the time, for doing something, something that maybe you shouldn’t.P 13
3.1.3. Experiences of Falling Ill from COVID-19
…when I was lying in bed and I took the test on Tuesday, I had a positive result on Wednesday at 3.30 in the afternoon… eh … and I got a bit frightened as I have a condition… lately they say that if you are following your medication you don´t need to be scared, ….but you didn´t know that in the beginning [of the pandemic]….P 12
I was sick for about two weeks. I think I stayed at home for one and a half weeks and then went back to work, and then I was tired and fell ill again… or it could be that I never really had recovered, but I never understood that… It took more than a month and then I felt that I was in a really, very bad shape. … I have a very small slope leading up to the house and it was… I had to take breaks to manage walking up to the house….P 13
3.2. Changes in Daily Life Habits
3.2.1. Changes at Work and in Daily Routines
I feel that lately, there has been some kind of inflation in scheduling digital meetings, now people have realized that these meetings are very easy to arrange, and I think that my co-workers have become less disciplined.P 13
…what’s been positive [during the pandemic] has kind of been that there’s… [pause] the society has sort of gone down to a calmer pace in a way. And that pace kind of fits better with my pace, or my energy, or what to say.P 5
Just being able to keep the routines, that keeps the days containing something, I think it does a lot for your well-being…P 1
3.2.2. Changes in Social Interactions
…I´ve always been comfortable with… being alone…But now, during the pandemic when, when you realise that social life has changed a lot then I have experienced the feeling of loneliness. I´ve felt lonely.P 11
Because I’m the kind of person who likes to hug other people //… to just be able to put a hand on their knee and say “I understand how you feel”, trying to convey my feelings through my hand, I think that’s very important to me… And it’s gone.P 9
3.2.3. Changed Conditions for Exercise and Physical Activity
…so from the first week in November, I think it was about then that we had more restrictions regarding going to gyms…. So I haven´t gone to the gym since then and I haven´t replaced it by doing something else. I´m moving at lot less now, and that´s actually something that, based on my cardiovascular condition, that I´m actually, eh… worried about.P 11
The physiotherapy was also closed. There´s a specialized physiotherapy department for adults suffering from congenital heart diseases. But they had been closed down since March, so that wasn´t an option anymore to go there. //… So that’s a very big difference. So, I notice that I’m weaker in my muscles and stiffer than I was a year ago, I haven’t been able to train that way.P 5
I avoid going to classes with lots of people //…I go during such hours, … when I go late, then I go very late, like half nine or nine o´clock at night. And that sort of makes me exhausted in the morning the next day.P 1
3.3. Curbing Emotional Reactions
3.3.1. Dealing with a Shrinking Life-Space
I´m retired and consequently I don´t have a job… I feel like a housewife with my hands tied behind my back, as I can´t shop, I can´t meet people and children and grandchildren, and so I live a very boring life.P 8
…we were a whole bunch of people that went to the movies together and then we went to a restaurant, and so on, you can´t do that anymore… we liked to go to the opera, but that has also been put to an end. You can´t go to the library, you just read your old books over and over again…P 3
But this is compensation, it’s good that you can do it. Last Sunday the weather was nice, so I invited some friends for coffee on the covered terrace of my cabin. We sat there in the sun, at a proper distance, and drank coffee and, uh, ate something. Sponge cake or something like that. So, I’m like that, I’m constantly trying to find “What can I do to keep my spirits up?”P 6
3.3.2. Applying an Unhealthy Behavior
…I mean, it´s so much easier when you spend so much time at home that you… stuff yourself with all sorts of things. I´ve noticed a big difference there, I haven´t much of a sweet tooth, but I eat more candy now than I´ve done before with chocolate. I feel that there´s often something that slides down my throat when I´ve done my shopping, and I think it´s to comfort myself.P 1
…my behavior has changed. Normally I take a shower every day…. But during the pandemic, the personal hygiene has become worse… I rarely shower, like maybe twice a week, and I´m much more careless with my dental hygiene as well…P 11
3.3.3. Managing Worry and Frustration
… you should be able to manage a situation like this without being depressed. There are others that are in a much worse situation. Think about those who are hit by the pandemic and live in refugee camps, I shouldn´t be complaining.P 8
…well, I can´t go about and worry before something happens, because then I will have a horrible life. So, what will be will be.P 1
It´s been a lot of excuses… blaming something else…eh “Ok, now I can´t make it to the gym, it… it´s better that you respect the recommendations, and…eh… you have a lot to do and it´s bad weather”… eh … lots of excuses to not go out and… and simply take a walk.P 11
4. Discussion
4.1. Awareness of an Exposed Situation
4.2. Changes in Daily Life Habits
4.3. Curbing Emotional Reactions
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anttiroiko, A.-V. Successful government responses to the pandemic: Contextualizing national and urban responses to the COVID-19 outbreak in east and west. Int. J. E-Plan. Res. 2020, 10, 1–25. [Google Scholar] [CrossRef]
- WHO. WHO Announces COVID-19 Outbreak a Pandemic. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020#:~:text=WHO%20has%20been%20assessing%20this,be%20characterized%20as%20a%20pandemic (accessed on 5 November 2020).
- Jeong, I.-K.; Yoon, K.H.; Lee, M.K. Diabetes and COVID-19: Global and regional perspectives. Diabetes Res. Clin. Pract. 2020, 166, 108303. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, I.; Farahnik, J.; Mischley, L.K. Synergy of pandemics—Social isolation is associated with worsened Parkinson severity and quality of life. NPJ Park. Dis. 2020, 6, 28. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Chtourou, H.; Boukhris, O.; Trabelsi, K.; Masmoudi, L.; Brach, M.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. COVID-19 home confinement negatively impacts social participation and life satisfaction: A worldwide multicenter study. Int. J. Environ. Res. Public Health 2020, 27, 6237. [Google Scholar] [CrossRef] [PubMed]
- Irwin, R.E. Misleading media coverage of Sweden’s response to COVID-19. BMJ 2020, 370, m3031. [Google Scholar] [CrossRef]
- Benke, C.; Autenrieth, L.K.; Asselmann, E.; Pané-Farré, C.A. Lockdown, quarantine measures, and social distancing: Associations with depression, anxiety and distress at the beginning of the COVID-19 pandemic among adults from Germany. Psychiatry Res. 2020, 293, 113462. [Google Scholar] [CrossRef]
- Di Corrado, D.; Magnano, P.; Muzii, B.; Coco, M.; Guarnera, M.; De Lucia, S.; Maldonato, N.M. Effects of social distancing on psychological state and physical activity routines during the COVID-19 pandemic. Sport Sci. Health 2020, 25, 619–624. [Google Scholar] [CrossRef]
- Pieh, C.; O′Rourke, T.; Budimir, S.; Probst, T. Relationship quality and mental health during COVID-19 lockdown. PLoS ONE 2020, 15, e0238906. [Google Scholar] [CrossRef]
- Blustein, D.L.; Guarino, P.A. Work and unemployment in the time of COVID-19: The existential experience of loss and fear. J. Hum. Psych. 2020, 60, 702–709. [Google Scholar] [CrossRef]
- Park, C.L.; Russell, B.S.; Fendrich, M.; Finkelstein-Fox, L.; Hutchison, M.; Becker, J. Americans’ COVID-19 stress, coping, and adherence to CDC guidelines. J. Gen. Intern. Med. 2020, 35, 2296–2303. [Google Scholar] [CrossRef]
- Mertens, G.; Gerritsen, L.; Duijndama, S.; Salemink, E.; Engelhard, I.M. Fear of the coronavirus (COVID-19): Predictors in an online study conducted in March 2020. J. Anxiety Disord. 2020, 74, 102258. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F. The first eight months of Sweden’s COVID-19 strategy and the key actions and actors that were involved. Acta Paediatr. 2020, 109, 2459–2471. [Google Scholar] [CrossRef] [PubMed]
- Kivi, M.; Hansson, I.; Bjälkebring, P. Up and about: Older adults’ well-being during the COVID-19 pandemic in a Swedish longitudinal study. J. Gerontol. Soc. Sci. 2020, 76, e4–e9. [Google Scholar] [CrossRef]
- Brandén, M.; Aradhya, S.; Kolk, M.; Härkönen, J.; Drefahl, S.; Malmberg, B.; Rostila, M.; Cederström, A.; Andersson, G.; Mussino, E. Residential context and COVID-19 mortality among adults aged 70 years and older in Stockholm: A population-based, observational study using individual-level data. Lancet Healthy Longev. 2020, 1, e80–e88. [Google Scholar] [CrossRef] [PubMed]
- Orlowski, E.J.W.; Goldsmith, D.J.A. Four months into the COVID-19 pandemic, Sweden’s prized herd immunity is nowhere in sight. J. R. Soc. Med. 2020, 113, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Brogårdh, C.; Hammarlund, C.S.; Eek, F.; Stigmar, K.; Lindgren, I.; Schouenborg, A.T.; Hansson, E.E. Self-perceived life satisfaction during the first wave of the Covid-19 pandemic in Sweden: A cross-sectional study. Int. J. Environ. Res. Public Health 2021, 18, 6234. [Google Scholar] [CrossRef]
- Eek, F.; Larsson, C.; Wisén, A.; Hansson, E.E. Self-perceived changes in physical activity and the relation to life satisfaction and rated physical capacity in swedish adults during the COVID-19 pandemic—A cross sectional study. Int. J. Environ. Res. Public Health 2021, 18, 671. [Google Scholar] [CrossRef]
- Best, L.A.; Law, M.A.; Roach, S.; Wilbiks, J.M.P. The psychological impact of COVID-19 in Canada: Effects of social isolation during the initial response. Can. Psychol. 2020, 62, 143. [Google Scholar] [CrossRef]
- Solomou, I.; Constantinidou, F. Prevalence and Predictors of Anxiety and Depression Symptoms during the COVID-19 Pandemic and Compliance with Precautionary Measures: Age and Sex Matter. Int. J. Environ. Res. Public Health 2020, 17, 4924. [Google Scholar] [CrossRef]
- Liu, F.; Liu, F.; Wang, L. COVID-19 and cardiovascular diseases. J. Mol. Cell. Biol. 2020, 13, 161–167. [Google Scholar] [CrossRef]
- Luo, J.; Zhu, X.; Jian, J.; Chen, X.; Yin, K. Cardiovascular disease in patients with COVID-19: Evidence from cardiovascular pathology to treatment. Acta Biochim. Et Biophys. Sin. 2021, 53, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Malterud, K. Systematic text condensation: A strategy for qualitative analysis. Scand. J. Public Health 2012, 40, 795–805. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.K.; Zidar, D.A.; Bristow, M.R.; Cameron, S.J.; Chan, T.; Harding III, C.V.; Kwon, D.H. COVID-19 and Cardiovascular Disease: From Bench to Bedside. Circ. Res. 2021, 128, 1214–1236. [Google Scholar] [CrossRef] [PubMed]
- Casagrande, M.; Favieri, F.; Tambelli, R.; Forte, G. The enemy who sealed the world: Effects quarantine due to the COVID-19 on sleep quality, anxiety, and psychological distress in the Italian population. Sleep Med. 2020, 75, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Lal, B.; Dwivedi, Y.K.; Haag, M. Working from home during COVID-19: Doing and managing technology-enabled social interaction with colleagues at a distance. Inf. Syst. Front. 2021, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Groarke, J.M.; Berry, E.; Graham-Wisener, L.; McKenna-Plumley, P.E.; McGlinchey, E.; Armou, C. Loneliness in the UK during the COVID-19 pandemic: Cross-sectional results from the COVID-19 Psychological Wellbeing Study. PLoS ONE 2020, 15, e0239698. [Google Scholar] [CrossRef]
- Beery, T.; Olsson, M.R.; Vitestam, M. COVID-19 and outdoor recreation management: Increased participation, connection to nature, and a look to climate adaptation. J. Outdoor Recreat. 2021, 36, 100457. [Google Scholar] [CrossRef]
- Kirwan, R.; Perez de Heredia, F.; McCullough, D.; Davies, I.G.; Butler, T. Impact of COVID-19 lockdown restrictions on cardiac rehabilitation participation and behaviours in the United Kingdom. BMC Sport. Sci. Med. Rehabil. 2022, 14, 67. [Google Scholar] [CrossRef]
- Moons, P.; Goossens, E.; Koen, L.; Kovacs, A.H.; Andresen, B.; Moon, J.R.; Van De Bruaene, A.; Rassart, J.; Van Bulck, L. The COVID-19 pandemic as experienced by adults with congenital heart disease from Belgium, Norway, and South Korea: Impact on life domains, patient-reported outcomes, and experiences with care. Eur. J. Cardiovasc. Nurs. 2022, 21, 620–629. [Google Scholar] [CrossRef]
- Morales-Vives, F.; Dueñas, J.-M.; Vigil-Colet, A.; Camarero-Figuerola, M. Psychological variables related to adaptation to the COVID-19 lockdown in Spain. Front. Psychol. 2020, 11, 565634. [Google Scholar] [CrossRef]
- Sjodahl Hammarlund, C.; Lexell, J.; Brogårdh, C. Growing up with a disability following paralytic poliomyelitis: Experiences from persons with late effects of polio. Disabil. Rehabil. 2019, 6, 960–966. [Google Scholar] [CrossRef] [PubMed]
- Sjödahl Hammarlund, C.; Lexell, J.; Brogårdh, C. Perceived consequences of ageing with late effects of polio and strategies for managing daily life: A qualitative study. BMC Geriatr. 2017, 17, 179. [Google Scholar] [CrossRef] [PubMed]
- Sjödahl Hammarlund, C.; Westergren, A.; Åström, I.; Edberg, A.-K.; Hagell, P. The Impact of Living with Parkinson’s Disease: Balancing within a Web of Needs and Demands. Park. Dis. 2018, 2018, 4598651. [Google Scholar] [CrossRef]
- Kristofferzon, M.L.; Engström, M.; Nilsson, A. Coping mediates the relationship between sense of coherence and mental quality of life in patients with chronic illness: A crosssectional study. Qual. Life Res. 2018, 27, 1855–1863. [Google Scholar] [CrossRef] [PubMed]
- Nygaard Andersen, L.; Kohberg, M.; Gram Herborg, L.; Soegaard, K.; Roessler, K.K. “Here we’re all in the same boat”—A qualitative study of group based rehabilitation for sick-listed citizens with chronic pain. Scand. J. Psychol. 2014, 55, 333–342. [Google Scholar] [CrossRef]
- D’ Addario, M.; Adorni, R.; Steca, P.; Capelli, R.; Zanatta, F.; Fattirolli, F.; Franzelli, C.; Giannattasio, C.; Greco, A. Associations between lifestyle changes and adherence to COVID-19 restrictions in older adults with hypertension. Int. J. Environ. Res. Public Health 2022, 19, 7853. [Google Scholar] [CrossRef]
- Torres, S.J.; Nowson, C.A. Relationship between stress, eating behavior, and obesity. Nutrition 2007, 23, 887–894. [Google Scholar] [CrossRef]
- De Sousa, R.A.L.; Improta-Caria, A.C.; Aras-Júnior, R.; de Oliveira, E.M.; Soci, Ú.P.R.; Cassilhas,, R.C. Physical exercise effects on the brain during COVID-19 pandemic: Links between mental and cardiovascular health. Neurol. Sci. 2021, 42, 1325–1334. [Google Scholar] [CrossRef]
- Sciomer, S.; Moscucci, F.; Maffei, S.; Gallina, S.; Mattioli, A.V. Prevention of cardiovascular risk factors in women: The lifestyle paradox and stereotypes we need to defeat. Eur. J. Prev. Cardiol. 2019, 26, 609–610. [Google Scholar] [CrossRef]
- Malterud, K. Qualitative research: Standards, challenges, and guidelines. Lancet 2001, 358, 483–488. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sjödahl Hammarlund, C.; Norlander, A.; Brogårdh, C. Experiences of People with Cardiovascular Disease during COVID-19 in Sweden: A Qualitative Study. Int. J. Environ. Res. Public Health 2023, 20, 5588. https://doi.org/10.3390/ijerph20085588
Sjödahl Hammarlund C, Norlander A, Brogårdh C. Experiences of People with Cardiovascular Disease during COVID-19 in Sweden: A Qualitative Study. International Journal of Environmental Research and Public Health. 2023; 20(8):5588. https://doi.org/10.3390/ijerph20085588
Chicago/Turabian StyleSjödahl Hammarlund, Catharina, Anna Norlander, and Christina Brogårdh. 2023. "Experiences of People with Cardiovascular Disease during COVID-19 in Sweden: A Qualitative Study" International Journal of Environmental Research and Public Health 20, no. 8: 5588. https://doi.org/10.3390/ijerph20085588