
A Mixed-Methods Investigation of Facilitators to Accessing and Utilising Mental Health Services amongst Sri Lankan Australians

Abstract
:1. Introduction
The Present Study
2. Method
2.1. Study Design and Procedure
2.2. Participants and Recruitment
2.3. Measures
2.3.1. Demographics
2.3.2. Facilitators to Seeking and Using Mental Health Services
2.3.3. Public Health Interventions
2.4. Statistical Analyses
2.4.1. Quantitative Data
2.4.2. Qualitative Data
3. Results
3.1. Quantitative Findings
3.1.1. Demographics
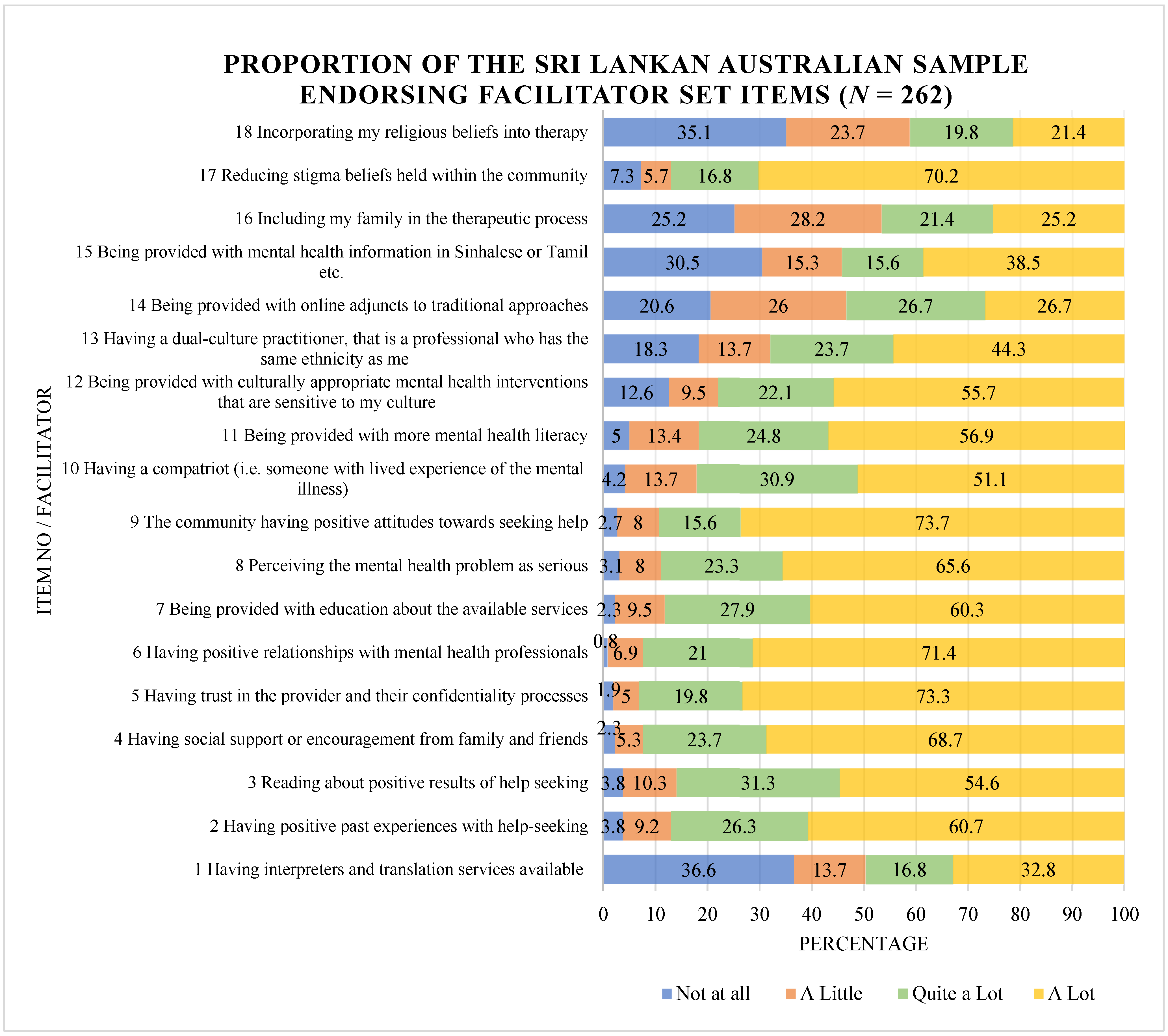
3.1.2. Facilitators to Seeking and Using Mental Health Services
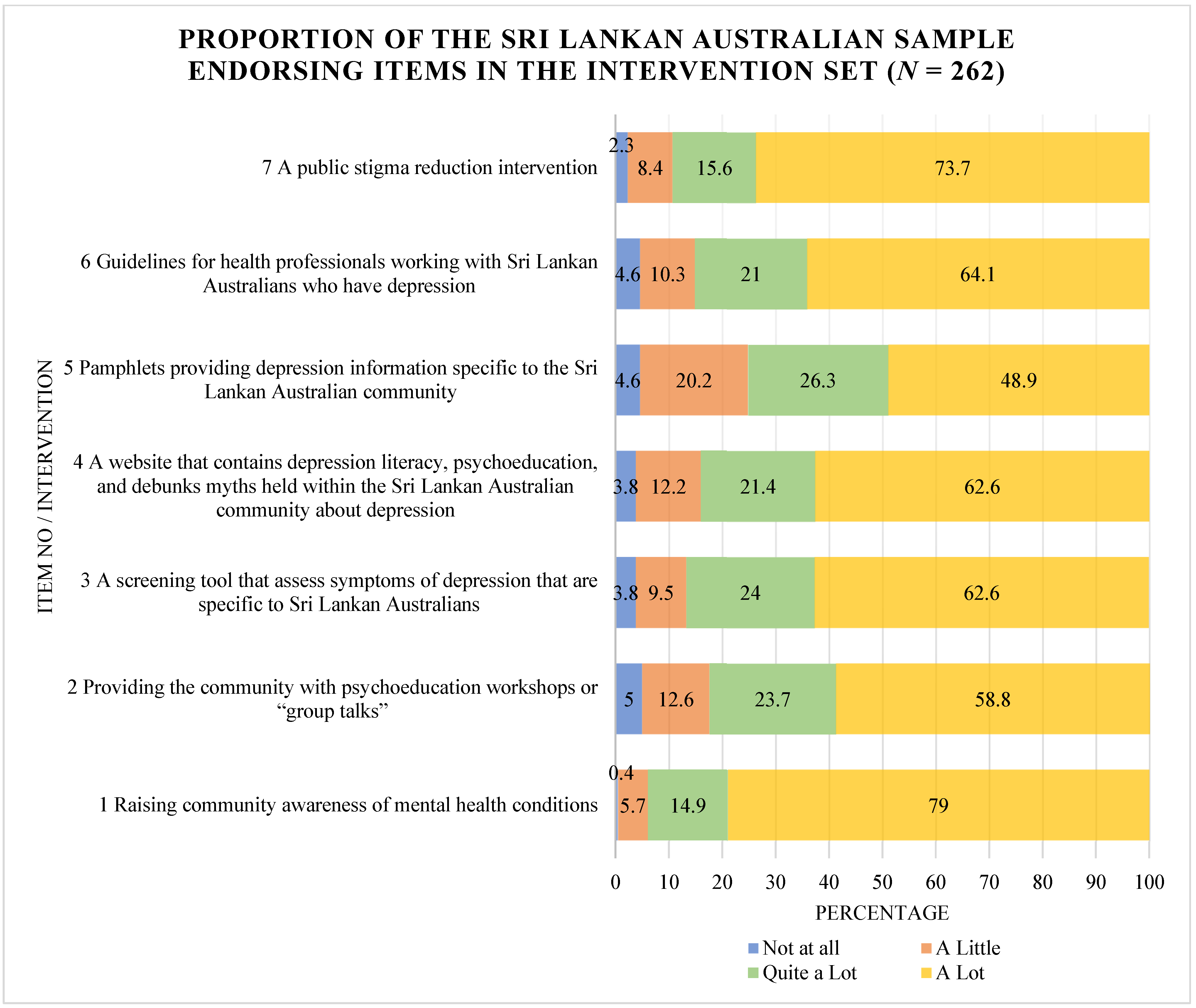
3.1.3. Public Health Interventions
3.2. Qualitative Findings
3.2.1. A Community-Based Approach to Increasing Mental Health Literacy and Addressing Stigma Beliefs
3.2.2. Access to Culturally Responsive Clinicians and Culturally Safe Services
3.2.3. Trust
3.2.4. Accessibility of Services
4. Discussion
4.1. Access to Culturally Safe and Responsive Services and Clinicians
4.2. Addressing Practical Barriers: Confidentiality, Trust, and Affordability
4.3. A Community-Based Approach to Increasing Mental Health Literacy and Addressing Public Stigma Beliefs
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hongo, M.; Oshima, F.; Nishinaka, H.; Seto, M.; Ohtani, T.; Shimizu, E. Reliability and Validity of the Japanese Version of the Barriers to Access to Care Evaluation Scale Version 3 for People With Mental Disorders: An Online Survey Study. Front. Psychol. 2021, 12, 760184. [Google Scholar] [CrossRef] [PubMed]
- Minas, H.; Kakuma, R.; Too, L.S.; Vayani, H.; Orapeleng, S.; Prasad-Ildes, R.; Turner, G.; Procter, N.; Oehm, D. Mental health research and evaluation in multicultural Australia: Developing a Culture of Inclusion. Int. J. Ment. Health Syst. 2013, 7, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logan, S.; Rouen, D.; Wagner, R.; Steel, Z.; Hunt, C. Mental health service use and ethnicity: An analysis of service use and time to access treatment by South East Asian-, Middle Eastern-, and Australian-born patients within Sydney, Australia. Aust. J. Psychol. 2017, 69, 12–19. [Google Scholar] [CrossRef]
- Stolk, Y.; Minas, I.H.; Klimidis, S. Access to Mental Health Services in Victoria: A Focus on Ethnic Communities; Victorian Transcultural Psychiatry Unit: Fitzroy, VIC, Australia, 2008. [Google Scholar]
- Planey, A.M.; Smith, S.M.; Moore, S.; Walker, T.D. Barriers and facilitators to mental health help-seeking among African American youth and their families: A systematic review study. Child. Youth Serv. Rev. 2019, 101, 190–200. [Google Scholar] [CrossRef]
- Basri, T.; Radhakrishnan, K.; Rolin, D. Barriers to and Facilitators of Mental Health Help-Seeking Behaviors among South Asian American College Students. J. Psychosoc. Nurs. Ment. Health Serv. 2022, 60, 32–38. [Google Scholar] [CrossRef]
- Mudunna, C.; Antoniades, J.; Tran, T.; Fisher, J. Factors influencing the attitudes of young Sri Lankan-Australians towards seeking mental healthcare: A national online survey. BMC Public Health 2022, 22, 546. [Google Scholar] [CrossRef]
- Antoniades, J.; Mazza, D.; Brijnath, B. Agency, activation and compatriots: The influence of social networks on health-seeking behaviours among Sri Lankan migrants and Anglo-Australians with depression. Sociol. Health Illn. 2018, 40, 1376–1390. [Google Scholar] [CrossRef]
- Daluwatta, A.; Peiris, D.; Fletcher, K.; Ludlow, C.; Murray, G. Can Sri Lankan Australians Recognise Depression? The Influence of Acculturation, Age and Experiences with Depression on Recognition. Int. J. Environ. Res. Public Health 2022, 19, 14839. [Google Scholar] [CrossRef]
- Wohler, Y.; Dantas, J.A.R. Barriers Accessing Mental Health Services Among Culturally and Linguistically Diverse (CALD) Immigrant Women in Australia: Policy Implications. J. Immigr. Minor. Health 2017, 19, 697–701. [Google Scholar] [CrossRef]
- Fauk, N.K.; Ziersch, A.; Gesesew, H.; Ward, P.; Green, E.; Oudih, E.; Tahir, R.; Mwanri, L. Migrants and Service Providers’ Perspectives of Barriers to Accessing Mental Health Services in South Australia: A Case of African Migrants with a Refugee Background in South Australia. Int. J. Environ. Res. Public Health 2021, 18, 8906. [Google Scholar] [CrossRef]
- Valibhoy, M.C.; Kaplan, I.; Szwarc, J. “It comes down to just how human someone can be”: A qualitative study with young people from refugee backgrounds about their experiences of Australian mental health services. Transcult. Psychiatry 2017, 54, 23–45. [Google Scholar] [CrossRef] [PubMed]
- McCann, T.V.; Mugavin, J.; Renzaho, A.; Lubman, D.I. Sub-Saharan African migrant youths’ help-seeking barriers and facilitators for mental health and substance use problems: A qualitative study. BMC Psychiatry 2016, 16, 275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziguras, S.; Klimidis, S.; Lewis, J.; Stuart, G. Ethnic matching of clients and clinicians and use of mental health services by ethnic minority clients. Psychiatr. Serv. 2003, 54, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Clement, S.; Brohan, E.; Jeffery, D.; Henderson, C.; Hatch, S.L.; Thornicroft, G. Development and psychometric properties the Barriers to Access to Care Evaluation scale (BACE) related to people with mental ill health. BMC Psychiatry 2012, 12, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Thematic Analysis: A Practical Guide; SAGE Publications Ltd.: London, UK, 2022. [Google Scholar]
- Sue DWS, D.; Neville, H.A.; Smith, L. Counseling The Culturally Diverse: Theory and Practice, 9th ed.; Wiley: New York, NY, USA, 2022. [Google Scholar]
- Mianji, F.; Tomaro, J.; Kirmayer, L.J. Linguistic and cultural barriers to access and utilization of mental health care for Farsi-speaking newcomers in Quebec. Int. J. Migr. Health Soc. Care 2020, 16, 495–510. [Google Scholar] [CrossRef]
- Fauk, N.K.; Ziersch, A.; Gesesew, H.; Ward, P.R.; Mwanri, L. Strategies to improve access to mental health services: Perspectives of African migrants and service providers in South Australia. SSM-Ment. Health 2022, 2, 100058. [Google Scholar] [CrossRef]
- Gulliver, A.; Griffiths, K.M.; Christensen, H. Perceived barriers and facilitators to mental health help-seeking in young people: A systematic review. BMC Psychiatry 2010, 10, 113. [Google Scholar] [CrossRef] [Green Version]
- Rastogi, P.; Khushalani, S.; Dhawan, S.; Goga, J.; Hemanth, N.; Kosi, R.; Sharma, R.K.; Black, B.S.; Jayaram, G.; Rao, V. Understanding clinician perception of common presentations in South Asians seeking mental health treatment and determining barriers and facilitators to treatment. Asian J. Psychiatry 2014, 7, 15–21. [Google Scholar] [CrossRef]
- Colucci, E.; Minas, H.; Szwarc, J.; Guerra, C.; Paxton, G. In or out? Barriers and facilitators to refugee-background young people accessing mental health services. Transcult. Psychiatry 2015, 52, 766–790. [Google Scholar] [CrossRef]
- Javanparast, S.; Naqvi, S.K.A.; Mwanri, L. Health service access and utilisation amongst culturally and linguistically diverse populations in regional South Australia: A qualitative study. Rural Remote Health 2020, 20, 5694. [Google Scholar] [CrossRef]
- Cuijpers, P.; Javed, A.; Bhui, K. The WHO World Mental Health Report: A call for action. Br. J. Psychiatry 2023, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, S.; Hickie AM, I. Making better choices about mental health investment: The case for urgent reform of Australia’s Better Access Program. Aust. N. Z. J. Psychiatry 2019, 53, 1052–1058. [Google Scholar] [CrossRef]
- Petrie, K.; Baldwin, P.; Crawford, J.; Harvey, S.B. The voice of mental health practice in Australia: A mixed-method cross-sectional study of gaps and areas of need. Aust. N. Z. J. Public Health 2021, 45, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Parcesepe, A.M.; Cabassa, L.J. Public stigma of mental illness in the United States: A systematic literature review. Adm. Policy Ment. Health Ment. Health Serv. Res. 2013, 40, 384–399. [Google Scholar] [CrossRef] [Green Version]
- Watson, A.C.; Corrigan, P.; Larson, J.E.; Sells, M. Self-Stigma in People with Mental Illness. Schizophr. Bull. 2007, 33, 1312–1318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrigan, P. How stigma interferes with mental health care. Am. Psychol. 2004, 59, 614–625. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Frequency | % |
|---|---|---|
| Gender | ||
| Male | 74 | 28.2 |
| Female | 188 | 71.8 |
| Age group (Mean = 31.7; SD = 11.5) | ||
| 18–29 years | 159 | 60.7 |
| 30–39 years | 53 | 20.2 |
| 40–49 years | 24 | 9.2 |
| 50–59 years | 17 | 6.5 |
| 60–69 years | 8 | 3.0 |
| 70 and over | 1 | 0.4 |
| Highest level of education | ||
| Secondary school or equivalent | 34 | 13.0 |
| TAFE course or equivalent | 20 | 7.6 |
| Undergraduate degree | 118 | 45.0 |
| Postgraduate degree | 90 | 34.4 |
| Country of birth | ||
| Australia | 86 | 32.8 |
| Sri Lanka | 161 | 61.5 |
| Other | 15 | 5.7 |
| Years in Australia (Mean = 19.1; SD = 9.8) | ||
| Under 10 years | 61 | 23.3 |
| 11 to 20 years | 59 | 22.5 |
| 21 to 30 years | 122 | 46.6 |
| Above 31 years | 20 | 7.6 |
| Ethnicity | ||
| Sinhalese | 223 | 85.1 |
| Tamil | 15 | 5.7 |
| Other | 24 | 9.2 |
| Religion | ||
| Buddhist | 158 | 60.3 |
| Christian | 16 | 6.1 |
| Roman Catholic | 31 | 11.8 |
| Atheist or Agnostic | 34 | 13.0 |
| Other | 23 | 8.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daluwatta, A.; Fletcher, K.; Ludlow, C.; Virgona, A.; Murray, G. A Mixed-Methods Investigation of Facilitators to Accessing and Utilising Mental Health Services amongst Sri Lankan Australians. Int. J. Environ. Res. Public Health 2023, 20, 5425. https://doi.org/10.3390/ijerph20075425
Daluwatta A, Fletcher K, Ludlow C, Virgona A, Murray G. A Mixed-Methods Investigation of Facilitators to Accessing and Utilising Mental Health Services amongst Sri Lankan Australians. International Journal of Environmental Research and Public Health. 2023; 20(7):5425. https://doi.org/10.3390/ijerph20075425
Chicago/Turabian StyleDaluwatta, Amanda, Kathryn Fletcher, Chris Ludlow, Ariane Virgona, and Greg Murray. 2023. "A Mixed-Methods Investigation of Facilitators to Accessing and Utilising Mental Health Services amongst Sri Lankan Australians" International Journal of Environmental Research and Public Health 20, no. 7: 5425. https://doi.org/10.3390/ijerph20075425